|
|
Chapter 6:
General Causes and Potential Effects of the Subluxation Complex
From R. C. Schafer, DC, PhD, FICC's best-selling book:
“Basic Principles of Chiropractic Neuroscience”
All of Dr. Schafer's books are now available on CDs, with all proceeds being donated |
Spinal Subluxation: Causes and Effects General Causes of Spinal Subluxations Precipitating Factors of Spinal Subluxations Physical Diagnosis Criteria General Effects of Spinal Subluxations Potential Scope of Reactions Functional Alterations Local Pathophysiologic Effects of Subluxation Spondylosis and Related Disorders Spinal Trauma Prevalent Theories of Spinal Pain Subluxation Terminology Fundamental Considerations Clinical Classes of Subluxation The Subluxation Complex as a Disease Entity The Apophyseal Joints Structural Changes in the Subluxation Complex Spinal Joint Locking Articular Neurology Receptor Types Clinical Considerations The Intervertebral Foramen Size and Shape Considerations Contents and Size Alterations Subluxation Effects At the Intervertebral Foramina Distal Neurologic Manifestations of Subluxations The Spinal Nerves Sensory Manifestations The Autonomics Nerve Root Insults Motor Manifestations The Posterior Rami The Vertebral Canal and Related Tissues Cord-Canal Relationships The Meninges The Dentate Ligaments The Spinal Cord Proper Postural and Structural Effects The Effects of Bipedism Pelvic Posture Considerations Structural-Functional Relationships Balance Considerations Postural Analysis Visceroptosis Postural Effects of Pregnancy Segmental Hypermobility Basic Considerations Implications Segmental Hypomobility Basic Considerationn Clinical Studies Implications Structural Adjustment Rationales Terminology The Uniqueness of the Chiropractic Adjustment Motion Barriers During Structural Therapy Specific Chiropractic Adjustments The Articular Snap Thrust Technics Indirect (Functional) Approaches
| Muscular Overload or Weakness | ||
| Abnormal glandular activity Biochemical imbalance Caustic chemical exposure Electric shock | Exposure to drafts Nutritional deficiencies Paralytic effects Postural distortion phenomena Psychomotor responses | Somatospinal reflexes Toxic states (endogenous or exogenous) Trauma, frank/acute Viscerospinal reflexes |
| Structural Imbalance | ||
| Connective-tissue disease IVD pathology Kyphosis Lordosis | Osseous pathology Postural fatigue Scoliosis Short-leg etiologies Sprain | Strain Structural anomalies Trauma, cumulative/repetitive, microtrauma/overuse syndrome |
(1) muscle splinting, especially on the side of greatest stimulation according to Pfluger's law or
(2) from abnormal weight distribution to the facets and other weight-bearing structures of the vertebrae involved.
Pfluger's law states that if a stimulus received by a sensory nerve extends to a motor nerve of the opposite side, contraction occurs only from corresponding muscles; and, if contraction is unequal bilaterally, the stronger contraction always takes place on the side that is stimulated. When affecting one or more vertebrae, this state of decreased mobility of the motion unit encourages nerve dysfunction, leading to pathologic processes in the areas supplied by the affected nerve root or neuromere depending upon the degree and chronicity of involvement.
Physical Diagnosis Criteria
The most commonly used criteria in physical diagnosis of determining the existence of vertebral subluxation-fixation are:
(1) asymmetry such as paraspinal soft-tissue changes (spasticity, contractures, or flaccidness) and palpable osseous malposition (often misleading);
(2) restricted segmental mobility in one or more planes;
(3) dermatomal skin abnormalities such as altered texture or color, bogginess, and vasomotor disorders with resultant temperature, thermographic, and electrical resistance changes; and
(4) possibly altered reflexes. Differential diagnosis by exclusion is frequently applied.
General Effects of Spinal Subluxations
As a primary concept of chiropractic science, spinal subluxations may result in the development of disease states locally within the vertebral motion unit itself or throughout specific areas of the body. These primary and secondary effects of subluxations may be classified into three major categories:
The mechanical effect, motion, and balance of the local segment, or the effect upon the skeleton elsewhere, due to compensatory distortions and alterations as proprioceptive mechanisms attempt to correct the mechanics in the presence of structural imbalance.
The effect of any localized condition occurring within the articulations due to interarticular stress and trauma (often microtrauma) such as irritation, inflammation, swelling, necrosis, and other degenerative changes.
The neurologic scope of subluxation effects may be grossly differentiated as nerve pressure, nerve stretch, nerve torsion, circulatory changes, meningeal irritations, cerebrospinal fluid flow alterations, alterations of proprioceptive responses and reflexes, traumatic insult to the rami communicantes or sympathetic ganglia, among many others. The neurologic effects are undoubtedly the more important of the three from a clinical aspect.
Spinal subluxation syndromes may have more than one immediate cause and effect. Abnormality of development may be complicated by degenerative joint disease, retrograde changes, inflammation, and muscle splinting, for example. The effects may be direct upon nerve roots and their blood vessels, reflex in nature, etc. Therefore, a complicated and far-reaching series of interacting and interdependent changes occur that may be designated as a subluxation syndrome.
Potential Scope of Reactions
When dysfunction manifests clinically, it can be assured that some degree of pathology is present. It also can be appreciated that any point in the complex nervous system can produce changes in the body when stimulated. These changes may manifest not only in adjacent parts but also in areas far remote from the site of irritation. If an irreversible change occurs at any point as a result of local irritation, the effect is some loss of a particular function and the establishment of new pathologic excitations that draw other parts into the process. Pathologist Boyd boldly states, "Disease is function gone wrong."
The neurons are the anatomical and functional units of the nervous system; and localization of effect does not exist in the nervous system. This is not to say that every active means of producing a transformation of the normal nervous state will be reflected in the same manner in the various pathologic progressions because the neurologic element is highly complex in its overt and covert functions. The nerve impulse creates a multitude of cellular reactions and responses besides those of the most intricate, subtle, and variable sensations and motor activities. Once this is recognized, the diagnostician must add the complexities of:
To these can be added those many phenomena that science is only beginning to appreciate or are beyond our present understanding. This underscores the fact that the quality of nerve function relates directly or indirectly to practically every bodily function and contributes significantly to the beginning of physiologic malfunction and the development of pathologic processes.
Functional Alterations
It is a basic premise of chiropractic that a relationship exists between dysfunction of the nervous system and many diseases. It is also fundamental that some aberration within the spinal column produces the nerve dysfunction, or more specifically, that a malpositioned vertebra is at fault. Bergmann reminds us that, besides this malposition, it must be clearly understood that the nerve dysfunction results from more than the structural misalignment. There are neuropathophysiologic, kinesiopathologic, myopathologic, histopathologic, biochemical, and possibly somatopsychic effects involved. Correction of the articular fixation tends to restore normal physiologic processes, and the pathologic processes involved subside to the degree that they are reversible.
It is likely that several overlapping processes are involved in the typical subluxation complex and its reduction by adjustive and manipulative therapy. Individually, the three most popular hypotheses currently being investigated to determine the effects of chiropractic primary therapy are:
The impulse-related theory: eg, improving the transmission or expression of neurologic impulses.
The nonimpulse-related theory: eg, improving the transmission of axonal transport mechanisms.
The biochemical theory: eg, decreasing the local sensitivity of joint afferents and discouraging the production of metabolic debris, including bradykinin, and/or stimulating the production of CNS endorphins.
Local Pathophysiologic Effects of Subluxation
A working hypothesis regarding spinal subluxations states that the vertebral displacement fixation will cause adjacent articulations of the spine to become hypermobile, resulting in stress of these motor units. Frogley believes that neurologic feedback causes the elicitation of ACTH and a resulting increase in the production of corticosteroids as an adaptive mechanism, according to the Hans Selye stress syndrome, and this also may be reflected by possible blood sugar changes.
Irritation at the site of misalignment and hypomobility will cause an inflammatory reaction with edema leading to a disturbance in the normal exchange of nutrients and waste products between capillary and extracellular fluid. Added to this stasis is the probable factor of lactic acid buildup in the area because of the release of the acid from the surrounding hypertonic musculature.
While toxic metabolic end-products (eg, urea, uric acid, creatinine, lactic acid) accumulate in stagnant tissue and congested capillary beds, there is also a corresponding decrease in nutrient and oxygen concentration in these fluids. Thus, the nerves emitting from the involved area will be deficient in necessary nutrients and quite possibly hypoxic as well.
This situation along with the toxicity effects upon the nerve may well result in a disorder in membrane permeability leading to dysfunction and disease. When toxicity occurs in the central and peripheral nervous systems, the formation of acetylcholine at the level of involvement will be interfered with and result in further neural disturbances due to an increased impairment of conduction.
Spondylosis and Related Disorders:
The Phases of Vertebral Unit Degeneration
The degenerative process has been divided by Kirkaldy-Willis into three phases (dysfunction, instability, and stabilization) into which a patient may pass into, out of, and return, depending on various circumstances such as degeneration progression and recurrent trauma (intrinsic or extrinsic).
The phase of dysfunction following trauma exhibits somewhat minor pathologic changes in the involved vertebra's disc and posterior facets, and there are few, if any, residual symptoms following recovery. The phase of instability features segmental hypermobility as the result of lax facet capsules and weakened anular structure. The phase of stabilization is characterized by a return of segmental stability as the result of area fibrosis, apophyseal osteophytes, and centrum osteophytes within the disc and at the disc's periphery.
Table 6.2 outlines a summary of findings, with some modification, described by Kirkaldy-Willis.
| Features | Dysfunction → → | Instability → → | Stabilization |
| History | Strain/sprain | Strain/sprain with likely history of previous injury | Chronic episodes of pain |
| Signs and symptoms | Perivertebral muscle splinting, pain (usually local, unilateral) that is aggravated by certain movements (eg, "catches"), tenderness of hypertonic erectors, lateral flexion unilaterally restricted, painful extension from flexion, antalgic scoliosis with muscle contraction on concave side of lateral bending. | Similar to those of dysfunction except feelings of weakness and periodic tendency toward collapse are usually reported; a segmental shift may be seen during extension from flexion. | Radicular pain, area stiffness, incapacitating attacks after minor trauma, muscle weakness |
| Biomechanics | Rotation or compressive overstress leading to subluxation | Hypermobile joint motion with frequent subluxation, facets likely open and malpositioned | Hypomobile joint motion |
| Pathology | Small anular disc tears, possible disc bulging or herniation, possible nuclear displacement, synovitis leading to facet fixation due to intra-articular adhesion and/or articular cartilage degeneration, probable facet displacement (subluxation) | Lax anulus and posterior joint capsules, coalesced disc tears, degenerated nucleus with probable displacement, circumference bulging of disc at periphery, probable abrupt change in pedicle height, possible A-P shift of unit during flexion and extension, possible tilt of unit on rotation, possible nipping of a synovial fold | Fibrosis, loss of nuclear substance, severe disc-space thinning, apophyseal osteophytes, centrum osteophytes, possible ankylosis, probable root entrapment. |
(1) soft-tissue receptors as the source of pain impulses,
(2) vascular pulsations offering repeated transient mechanical stimuli to tensed or compressed roots, or
(3) inflammatory foci responsible for a sustained neural discharge rather than that of mechanical forces.
Pain perceived in the spine may be the result of either intrinsic or referred causes. Common disorders associated with spinal pain are shown in Table 6.3. Some selected diseases referring pain to the spine are shown in Table 6.4.
| Type | Examples | |
| Degenerative process | Apophyseal osteoarthritis Cauda equina disorders Disc degeneration Hyperostosis Joint instability | Nerve root compression Spinal cord disease Spinal stenosis Spondylolisthesis Spondylosis |
| Developmental deficit | Bastrup's disease Hypermobility Kyphosis Lordosis Scoliosis | Short-leg syndrome Spondylolisthesis Various anomalies (eg, hemivertebrae) | Iatrogenic origin | Ill-advised manipulation Misplaced spinal tap Myelography | Poorly fitted support Postsurgical adhesions Prolonged use of support |
| Infective arthropathy or neuropathy | Actinomycosis Brucellosis Icterohemorrhagica Influenza Leptospirosis Meningitis Osteomyelitis Paratyphoid fever Poliomyelitis | Smallpox Staphylococcal infection Subarachnoid hemorrhage Syphilis Syringomyelia Tetanus Tuberculosis Typhoid fever |
| Inflammatory arthropathy | Ankylosing spondylitis Fibrositis Focal sepsis Muscular rheumatism Osteochondritis Panniculitis Polyarteritis nodosa Polymyalgia arteritica | Psoriasis Regional ileitis Rheumatoid arthritis Reiter's disease Secondary spondylitis System lupus erythematosus Ulcerative colitis |
| Metabolic deficit | Gouty rheumatism Hyperparathyroidism Osteomalacia | Osteoporosis Paget's disease of the spine | Spinal tumors | Aneurysmal bone cysts Hodgkin's sarcoma Myelomatosis | Neurofibroma Secondary carcinoma |
| Trauma | Disc protrusion Dislocation Facet syndrome Fracture Obesity Postural fault Short-leg syndrome | Spondylolisthesis Sprain/strain Subluxation Trauma, cumulative, repetitive microtrauma overuse syndrome |
| Type | Examples | |
| Cervical pain | Malignant lymphadenopathy Pancoast tumor | Subarachnoid hemorrhage Vertebral artery syndrome |
| Thoracic pain | Aortic aneurysm Bronchial carcinoma Cardiac enlargement Coronary artery disease | Gallbladder disease Herpes zoster Hiatus hernia Pulmonary disease |
| Lumbar pain | Aortic obstruction Colon carcinoma Disseminated sclerosis Endometriosis Hip disease Miscellaneous pelvic carcinoma Obstruction of iliac arteries | Pancreatic carcinoma Peptic ulcer Prostatic disease Rectal carcinoma Renal disease Short-leg syndrome Spinal cord tumor |
| Miscellaneous: | Central nervous system diseases such as meningitis, poliomyelitis, syringomyelia, tetanus, spinal subarachnoid hemorrhage. Iatrogenic manifestations Psychogenic causes Visceral diseases causing referred pain to the spine or pressure erosion | |
 |
Abnormal spinal biomechanics clinically relate to subluxations and other spinal malfunctions that result in structural and physiologic inadequacies of the spinal column. This state is the condition of a vertebral motion unit that has lost its normal structural and/or functional integrity and is, therefore, unable to move from its normal resting position, to move properly through its normal range of motion, or to return to its normal resting position after movement.
There are numerous methods of classifying vertebral subluxations. Each has its own rationale and each has certain validity that has been a contribution to our understanding of this complex phenomenon. In chiropractic, the general term vertebral subluxation refers to any alteration of the normal dynamic, anatomical, or physiologic relationships of contiguous articular structures.
There are 115 diarthroses within the spine and pelvis vulnerable to the abnormal movement related to subluxation. Each of these articulations is a site of proprioceptive sensitivity that, when under articular strain, is provoked to express pathophysiologic sensory and motor impulses.
Fundamental Considerations
During the course of the clinical picture of a related pathophysiologic process, an altered vertebral motion unit may be a predisposing factor, a primary factor, a concomitant factor, an attenuating factor, a complicating factor, or a consequential factor. Thus, a complete description of vertebral subluxation syndromes would be voluminous and far beyond the capacities allotted here. Thus, the following should be considered only basic information.
A fixated subluxated vertebral motion unit has lost its normal structural and/or functional integrity and is, therefore, unable to move from its normal resting position, to move properly through its normal range of motion, or to return to its normal resting position after movement. Thus, consideration must be given to a vertebral subluxation's static and dynamic structural position and related functional abnormalities.
The biomechanical element of the vertebral motion unit subluxation is classified by Hildebrandt/Howe according to its static or kinetic aspects and with the number of vertebral motion units involved.
Static Vertebral Motion-Unit Subluxations. Examples are:
For more in-depth information on this topic, please refer to:
Chapter 6: Radiologic Manifestations of Spinal Subluxations
The titles listed in the above list refer to the primary position involved. As a vertebral motion unit has five planes of motion, all movements are biomechanically coupled to some extent.
The common clinical picture is one of segmental fixation during motion relative to the vertebral segments above and below. The commonly associated "off centering" is usually far less in extent than the incomplete dislocation referred to by allopathic orthopedists. In chiropractic semantics, this "off centering" may not even exist in the static spine as seen in the "subluxation" of fixation that produces an abnormal pivot within the normal physiologic range of motion or in the hypermobile segment that returns to a centered position in the neutral position. In addition, an "off centered" vertebra that is not interfering with function is rarely considered a "subluxation" in clinical chiropractic.
Kinetic Vertebral Motion-Unit Subluxations. The three major types are:
(1) aberrant movement subluxations,
(2) hypermobility subluxations, and
(3) hypomobility subluxations.
Clinical Classes of Subluxation
The seven commonly recognized clinical types of subluxation are:
(1) functional subluxation, a functional and slight "off centering" with partial fixation in an otherwise normal articular bed;
(2) pathologic subluxation, an "off centering" derangement in an articular bed that has become deformed as the result of degenerative changes;
(3) traumatic subluxation, in consequence to an extraneous or intrinsic force and the associated muscle spasm;
(4) reflex subluxation, "off centering" induced by asymmetrical muscle contraction from aberrant visceral or somatic reflexes;
(5) defect subluxation, subluxation of an anomalous or developmentally defective spinal or pelvic segment;
(6) fixation subluxation, hypomobile fixation in which a spinal or pelvic segment that is in a neutral position of mobility fails to participate fully in movement;
(7) hypermobile subluxation, pathologic segmental increase in movement consequent to the loss of integrity of the retaining mechanism caused by trauma or degenerative pathology.
The Subluxation Complex as a Disease Entity
In Greenman's opinion, which is shared by many, "Manipulative therapy is not utilized just to treat a specific disease, but rather to maximize the structural-functional integrity of the total human organism to cope with its internal and external environmental stresses which have resulted in the patient's disease." This statement is generally true from a broad viewpoint.
From a more restricted viewpoint, an osseous disrelationship or an abnormal degree of physiologic segmental motion is generally considered a finding and associated soft-tissue aberrations are considered part of the syndrome. It may be either a contributing cause or an effect. Thus, in this context, describing a subluxation would not be a diagnosis. However, some may consider the spine an organ; ie, a part of the body exercising a specific function, and the spine readily meets this definition. In this context, it would be difficult not to consider a specifically defined primary subluxation complex as a diagnosis in that it arrives at the determination of the nature of a disease (ie, a disorder of body function).
A disease entity is characterized usually by at least two of the following criteria:
(1) a recognized etiologic agent (or agents),
(2) an identifiable group of signs and symptoms, or
(3) consistent anatomical alterations (Illustrated Stedman's Medical Dictionary, ed 24, 1982). Rarely does a subluxation-fixation entity have difficulty in meeting these criteria.
Examples for cervical motion-unit dysfunction are shown in Table 6.5.
| Criteria | ||
| Etiologic agent | Abnormal structural support Contractures Unequal muscle balance Paralysis | Poor sleeping postures Somatic or visceral response Sprain Strain |
| Symptoms | Articular grating Headaches Neuralgia Numbness Pain (especially on motion) Possible remote somatic effects | Possible remote visceral effects Stiffness Tenderness Tension Upper extremity pain Weakness |
| Signs | Altered normal reflexes Boggy tissues (focal) Electromyographic signs Fibrosis Hyperemia Hypertonic/flaccid muscles Segmental atrophy | Skin electro-resistance alterations Skin temperature alterations Skin texture alterations Thermographic signs Trigger point development Visual postural imbalance |
| Anatomical alteration | Palpable malalignment Roentgenographic signs | Segmental motion alterations |
The articulating processes of the spine have weak synovial joint capsules that are strengthened by two strong anterior and posterior ligaments, with fibers running perpendicular to the facet plane. They attach just beyond the margin of the facets. They are quite loose and elastic in the cervical region to allow greater mobility without capsule stretch. They are tighter and stronger in the thoracic and lumbar regions.
Wyke points out that, with few exceptions, any type of adjustive or manipulative technique imposes static and dynamic forces across the joint or joints being treated. This is as true for soft-tissue massage as it is for dynamic thrusts. Thus, the general principles of receptor neurology must be recognized if diagnosis and therapy are to be directed in a scientific manner.
Type I receptors are dynamic articular mechanoreceptors that have an extremely low threshold and are slowly adapting. They are found in the superficial fibrous layers of capsules and respond whenever the joint capsule is stretched; thus, they are active almost continuously. These superficial receptors signal the direction, amplitude, and velocity of joint movement. The frequency of discharge is proportional to the forces applied to the capsule.
The surfaces of the articular facets are covered by tough hyaline cartilage and separated by meniscus-like tabs of synovium that originate from the synovial lining. These tabs glide in and out of the joint during motion but are rarely nipped during joint jamming. The tabs appear to allow a degree of extra shock-absorbing and pressure-absorbing protection for the articular cartilage.
The vertebral tilting that is seen in subluxations with disc wedging exhibits an alteration of the relationship of apposing articular surfaces. This produces a change in the direction of compressive forces on these joints. In contrast, severe rotation produces a jamming compression on ipsilateral facets and contralateral facet opening.
When continuous compression is applied to any active and mobile joint, cartilaginous erosion followed by arthritis can be expected. Possible pain-provoking mechanisms at the facet joints include capsular ligament sprain, facet jamming or fixation by subluxation, pinching of a synovial fringe, entrapment of a loose cartilaginous body in the joint, and cervical or lumbar meniscoid entrapment.
The posterior articular facets of the spine possess the histologic capability to account for many of the various phenomena found in the subluxation syndrome. Their proximity to the IVF is of special interest because both structural and functional changes in these facets have been shown to affect the nerve-root sheath and contents.
Structural Changes in the Subluxation Complex
Following experimental research on the apophyseal joints, especially that of normal joint structures and their reaction to injury, Reiter reports an anatomical study of 75 postmortem spines that revealed significant changes, many of which would not be visible on x-ray. Capsular changes included edema, granular ossification, calcification, and adhesion between the capsule and the meningeal covering of the nerve root adjacent to it. Intra-articular changes included hypertrophy of the menisci up to four times their normal size, occasional chondrification and ossification of the menisci, detached bodies, ulcerated areas of denuded hyaline cartilage, cartilage thinning, fibrillation, and osteophytic marginal proliferation.
Spinal Joint Locking
Good defines spinal joint blocking within a subluxation syndrome as an actively maintained, reversible, biomechanical phenomenon in which paravertebral spasm (especially unilateral multifidus and rotator contraction) physiologically locks one or more motion segments, causing a shift of the axes of motion toward an apophyseal joint to the degree that the unsynchronized segment is unable to articulate about the new axis. Thus, any method that helps relocation (normalization) of the axes of movement that releases the nociceptor feedback or relaxes the segmental spasm will be effective in reducing acute joint hypomobility whose initial origin was that of strain.
ARTICULAR NEUROLOGY
Receptor Types
The synovial joints of the body, including the apophyseal joints of the spinal column, are provided with four types of receptor terminals that have variable characteristics. The major features of articular receptor sensory systems are shown in Table 6.6. Types I-III are corpuscular proprioceptive mechanoreceptors that serve as organic transducers. They are stimulated by increased tissue tension such as that induced by any type of active or passive mobilization.
Table 6.6. Characteristics of Joint Receptor Systems
Type I II III IV
Resembles Ruffini corpuscles Pacinian corpuscles Golgi end-organs
Location Outer layers of Sparsely found in Joint ligaments, Joint
joint capsule, deep layers of grape-like clusters (except
grape-like clus- joint capsule and (2-3) or found synovial
ters (3-8) and in fat pads, individually ligaments
grape-like clusters fat pads
(2-4)
Endings Encapsulated Thickly encapsulated Thinly encapsulated Bare
nerve
ending
plexus
Fiber type Myelinated, small Myelinated, medium Myelinated, large Myelin-
and size (6–9 microns) (9–12 microns) (13–17 microns) and
unmyelinated
Threshold Very low Low High High
Conduction Slow Medium Rapid Slow
Adaptation Slow Rapid Very slow Not
adapting
Action Mechanoreceptor Dynamic mecha- Dynamic mecha- Noci-
noreceptor noreceptor ceptor
Function Signals static Signals only rapid Signals direction Signals
position of joint, changes in move- of movement; noxic
speed and direc- ment, acceleration, guards against change
tion of joint deceleration; helps excessive joint
movement; con- initiate momentum, movement by
stantly firing; does not signal regulating muscle
aids in regulat- joint velocity, tone (braking
ing posture and amplitude, or mechanism)
muscle tone dur- direction
ing joint motion
_________________________________________
*Adapted from Kessler/Hertling and Wyke.
Type II receptors are also dynamic articular mechanoreceptors that have a low threshold, but they adapt faster than Type I receptors. They are found in the deep subsynovia of joint capsules. They are normally inactive in resting joints but respond whenever capsule tension is increased. The primary purpose of these deep receptors is merely to signal (by a brief burst of impulses) that joint movement has been initiated.
Type III receptors are commonly found in peripheral joint ligaments, but they are absent in paraspinal ligaments. They have a high threshold and adapt slowly, responding only when capsule tension is greatly increased.
Type IV receptors are widely dispersed pain-conducting nonproprioceptive bare nerve endings within many joint tissues that are normally inactive but become excited when exposed to a high degree of mechanical stress or chemical irritants. They are located in the superficial layers of joint capsules as fine plexuses, in the collateral and intrinsic ligaments of a joint as a fine meshwork, and distributed within articular fat pads and vascular sheaths. Type IV receptors are not found within synovial lining, menisci, or articular cartilage.
Clinical Considerations
Knowledge of the function of the various types of joint receptors is important to any physician directing physical therapy because of the threefold effect produced when these mechanoreceptor impulses enter the spinal cord as the result of active motion, therapeutic mobilization, traction, or vibration.
Reflex Effects
Like the sensory fibers projecting from mechanoreceptors of the skin, the afferent impulses emanating from joint mechanoreceptors take a polysynaptic course. The primary fibers terminate with the fusimotor neurons (but not alpha neurons) in the motor neuron pool within the gray matter of the spinal cord. Thus, they contribute to monitoring muscle spindle activity such as muscle tone and stretch reflex excitability.
In addition, to this primary course, mechanoreceptor afferents also send collaterals that are distributed intersegmentally throughout the neuraxis. Because of this extensive intersegmental system of communication, any motion produced in one joint will tend to inhibit the motor-unit activity and facilitate the tone of the muscles near the joint and often some quite remote (even contralaterally) from the joint stimulated.
Pain Suppression
Unlike the sensory fibers from joint mechanoreceptors, impulses of the primary nociceptor afferents from Type IV receptors course to the alpha neurons in the motor neuron pool within the gray matter of the spinal cord. The effect is abnormal reflex activity in the muscles supplied segmentally.
Like the sensory fibers from joint mechanoreceptors, collaterals are given off in the spinal cord that synapse in the "gateway" of the basal nucleus of the gray matter, ascend via the anterolateral spinal tracts, and ultimately end in the limbic region of the cerebral cortex. However, this flow of pain-provoking impulses can be inhibited presynaptically in the substantia gelatinosa by superimposed impulses from the mechanoreceptors whether they originate from joint mechanoreceptors or cutaneous mechanoreceptors.
It is in this manner that Wyke and others believe joint-pain suppression is achieved by massage, vibration, stretching, traction, TENS, compression, mobilization, rocking, or mild exercise. This theory suggests that the degeneration of peripheral mechanoreceptor pathways commonly associated with the aging process might explain why physical therapy is less effective in relieving pain in the elderly than in the young.
If central input from all joint receptors is blocked, the effect would mimic joint-infiltration anesthesia and feature a diminished joint-pain threshold, absent kinesthetic sensations, postural abnormalities, movement impairments, and gait disturbances.
Conscious Perception
Mechanoreceptor afferents course polysynaptically in their upward ascent, via the posterior and posterolateral columns, to terminate in the paracentral and parietal cerebral cortex. Types I and III (but not Types II or IV) afferents are primarily responsible for initiating kinesthetic perceptions. For this reason, the decrease or loss of kinesthesia is one of the first symptoms to appear when joint disease blocks or destroys Types I and III mechanoreceptor afferents.
Pain may stubbornly persist, however, as long as Type IV impulses can reach the brain stem and cerebral cortex. Degenerative, inflammatory, and traumatic disorders of joints commonly result in a loss of Types I III mechanoreceptor input but not of Type IV nociceptor input.
THE INTERVERTEBRAL FORAMEN
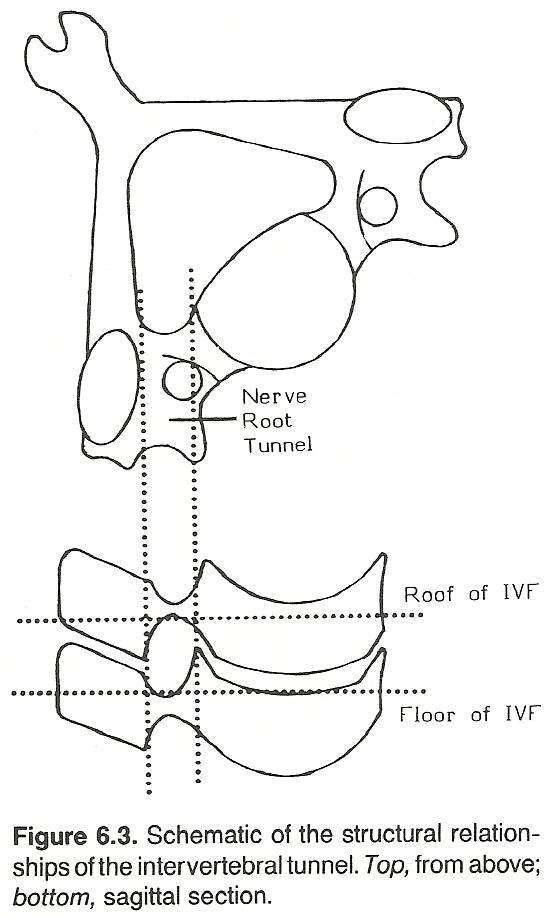 |
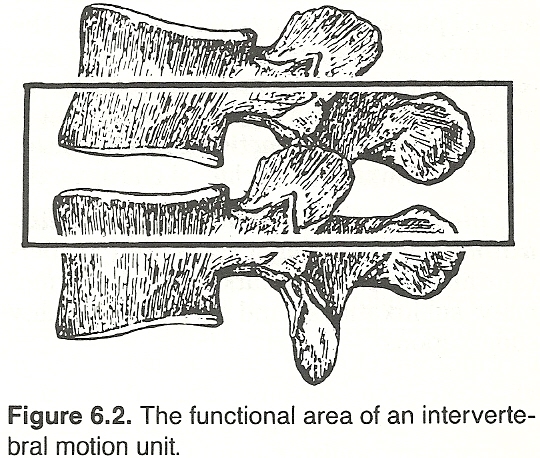
An intervertebral foramen (IVF) is generally bounded above by the inferior pedicle notch of the superior vertebra, below by the superior pedicle notch of the inferior vertebra, anteriorly by the intervertebral disc (IVD) and parts of the two vertebral bodies, and posteriorly by the superior and inferior articular processes.
Vertebral segments normally move in the planes of their articulations (unless the motion is blocked), and it is at the level of the apophyseal facets that most subluxations occur and influence the IVFs far more than any other articulations of the spinal column. Changes in the diameter of normal IVFs result in an abnormal channel between spinal and peripheral levels of the nervous system, which predisposes to malfunction as well as being a direct factor in altering the curves of the spine in which this structural defect is found.
The nerve roots of the cervical spine are located anteriorly and inferiorly to their facets. In the thoracic spine, they lie directly anterior to the facets. In the lumbar spine, the nerve roots are located anteriorly and superiorly to the facets, beneath the pedicles.
Size and Shape Considerations
When viewed laterally, an IVF is generally elliptical in shape, with the diameter of its vertical axis about double its A-P dimension. Because of this, there is usually adequate space for changes in vertical dimension (eg, dynamic axial traction or compression, moderate disc flattening) without injury to the IVF contents as long as there is adequate fat and fluid present. However, reduction of an already short transverse diameter can produce many noxious effects. For this reason, complete disc collapse vertically is often asymptomatic, while a slight posterolateral herniation may protrude upon the IVF and produce severe symptoms.
The Cervical Area
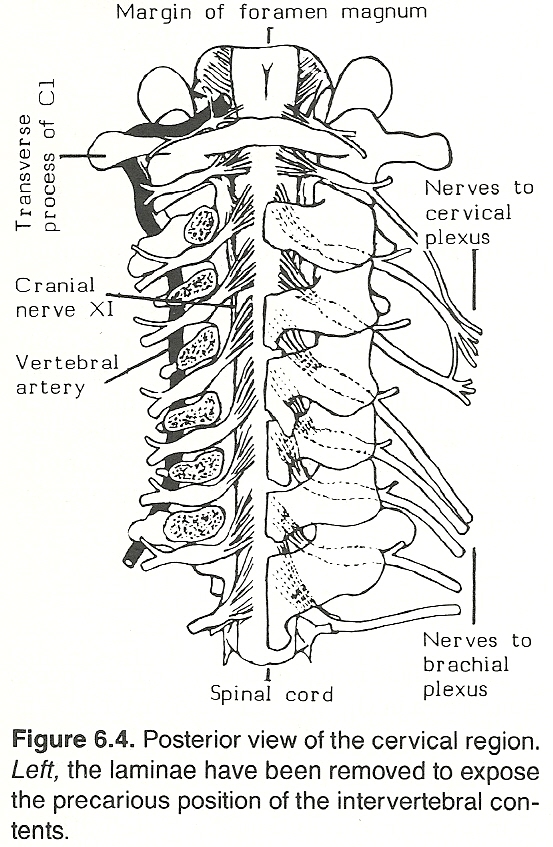 |
The cervical foramina are designed more in the shape of rounded gutters than orifices, averaging 1 cm in length. There is no IVF between the atlas and the occiput or between the atlas and the axis.
The C1 nerve exits over the superior aspect of the posterior arch of the atlas in the vertebral artery sulcus. The C2 nerve exits between the inferior aspect of the posterior arch of the atlas and the superior aspect of pedicle of the axis. It then dangerously transverses the lateral atlantoaxial joint, anterior to the ligamentum flava. The C3--C8 nerves exit through short oval canals, which increase in size as they progress caudally.
Cervical nerves, especially, fill the transverse diameter of their IVFs. Thus, any disorder that reduces this dimension (eg, subluxation, osteophytes, disc herniation, edema) will undoubtedly compromise the integrity of the IVF contents.
The Thoracic Area
The pedicle notch of the vertebra above is quite deep in the thoracic region, while that of the vertebra below is relatively shallow. The result is a pear-shaped canal with sharp bony edges that predispose to fibrotic changes from chronic irritation. The vertebral body and the disc of the superior vertebra form most of the IVFs anterior boundary.
The Lumbar Area
A lumbar IVF is shaped like a kidney bean. It takes considerable posterolateral disc protrusion to encroach the nerve exiting at the same level because the lumbar IVFs are comparatively large. When herniation does cause trouble, it is usually due to pressure on the laterally placed nerve root on the vertebra above.
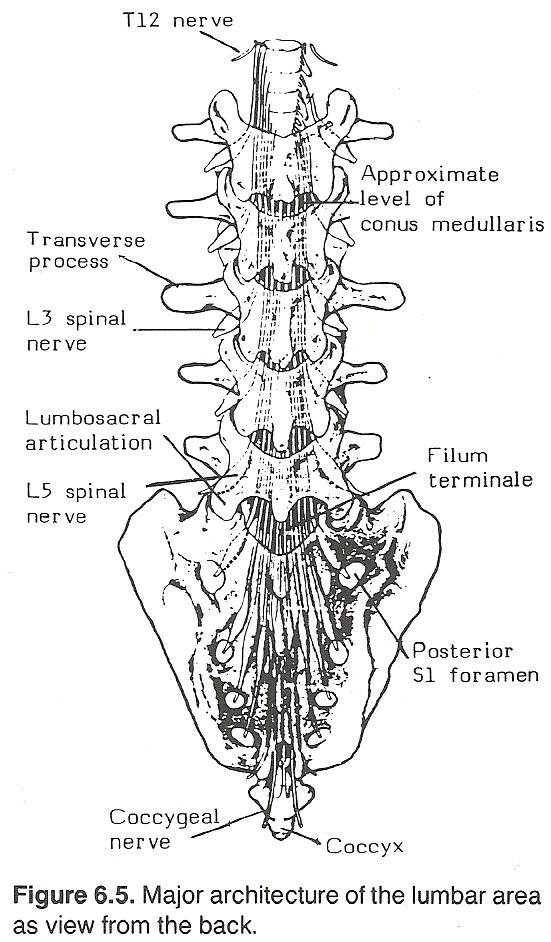 |
Sunderland emphasizes that the passage of the medial branch of the lumbar dorsal ramus and its accompanying vessels through the osseofibrous tunnel and the intimate relationship of the neurovascular bundle to the capsule of the apophyseal joint represents a potential site of fixation and entrapment following pathologic changes involving the joint.
Contents and Size Alterations
Each IVF of the spine is dynamic; widening and expanding with each spinal motion, serving as a channel for nerve and vascular egress and ingress, and allowing compression and stretching of the lipoareolar bed. From one-third to one-half of the foraminal opening is occupied by the spinal nerve root and its sheath, with the remaining portion filled primarily by fat, connective tissue, and the various vessels.
The following structures are found in the IVF:
The anterior nerve root
The posterior nerve root
A portion of the dorsal nerve root ganglion
A bilaminar sleeve of dura and arachnoid membrane, extending to the ganglion
A short continuation of CSF-containing subarachnoid space, which ends just after the ganglion
The recurrent meningeal nerve
The spinal ramus artery
The intervertebral vein
Lymphatic vessels.
Factors That Change IVF Diameter
The typical factors modifying the diameters of the IVFs are:
(1) the disrelationship of facet subluxation,
(2) changes in the normal static curves of the spine,
(3) the presence of induced abnormal curves of the spine,
(4) degenerative thinning, bulging, or extrusion of the related IVD,
(5) swelling and sclerosis of the capsular ligaments and the interbody articulation, and
(6) marginal proliferations of the vertebral bodies and apophyseal articulations.
Consequences of IVF Diameter Alteration
The above factors can insult the viable contents of the IVF and subject its contents to physiologic compromise that results in nerve root pressure, traction, or torque; constriction of the spinal blood vessels; intraforaminal and paraforaminal edema; induration and sclerosis of the periarticular ligaments with incarcerating insult upon the contained receptors; forcing of the foraminal contents into protracted constriction and altered position; and other consequences.
Nerve tissue tolerates slow compression without offering obvious symptoms. Acute phenomena are usually the result of friction, severe or repeated trauma, and encroachment from degenerative thickening or exostosis.
Subluxation Effects At the Intervertebral Foramina
Normally, the cross-sectional area of an IVF leaves ample room for its neural contents during the dynamics of daily life. The IVF narrowing that occurs during spinal extension movements has little if any adverse effects in the normal spine. The channel contents are normally free to adjust to movements throughout the normal range of regional motion.
Pathologic changes in and near the foramen may reduce its dimensions and lead to compression, but, as Sunderland points out, friction over osseofibrous irregularities or traction on a nerve or nerve roots fixed in the foramen by an adhesion is much more likely.
When under constant stress, a vertebral motion unit normally adapts so that changes occur in adjacent IVDs, ligaments, membranes, muscles, and other associated tissues that produce some degree of fixation. Because of this segmental fixation, adjacent IVFs are altered in size. As a rule, two of them become smaller than normal, and the other two become larger than normal. Nerve roots and other contents of the affected IVFs become subjected to insult at the smaller foramina and stretching at the larger foramina.
Possible intervertebral events as a result of a subluxation complex are shown in Table 6.7.
Articular and Para-Articular Changes
Bony foraminal encroachment Minute hemorrhages
Changes resulting from mechanical Minute tearing of dural root sleeve
deformation attachments in or near IVF
Eccentric zygapophyseal cartilage Paravertebral pain and tenderness
compression Pedicle kinking
Joint capsule overstress, resulting in Sclerosis
capsule thickening, reduced mobility Transudation
Trauma to periosteal margins pro-
ducing proliferative changes
Traumatic edema Proprioception and Autonomic Changes
Reflexes to motor components
Abnormal or subnormal somatomotor and
visceromotor reflexes
Circulatory Changes Stimuli interpreted as peripheral
Arteriovenous stagnation sensory stimulation
Cerebrospinal fluid flow alterations Misinterpreted somatosensory reflexes
Changes resulting from ischemia Misinterpreted viscerosensorey
Interference with IVF interstitial fluid reflexes
Interference with nerve root intra- Visceromotor reflexes
cellular fluid Circulatory dysfunction
Sluggish lymphatic flow Smooth muscle dysfunction
Secretory dysfunction
Trophic dysfunction
Musculoskeletal
Visceral
IVD Changes
Anular fiber overstress
Eccentric compression
Nuclear displacement
Protrusion or herniation Toxic Metabolic Products and Effects
of Venous Stagnation from Arterial Backup
Paraforaminal Soft-Tissue Changes Acetylcholine inhibition
Adhesions Cellular malnutrition
Altered nerve root level Creatinine
Encroachment symptoms Hypoxia
Traction symptoms Inflammatory residues
Pedicle kinking Ionic imbalance
Atrophy Lactic acid buildup
Contractures pH changes
Ganglionic compression or irritation Urea
Hyper- or hypo-tonicity Uric acid
Meningeal traction
Effects of Microtrauma
The zygapophyseal articular complex of a subluxated vertebral motion unit is initially subjected to the stress of "off centering" and is attended by the following aspects of microtrauma:
Minute hemorrhage, transudation, and arteriovenous stagnation from the sluggish circulatory flow resulting from the motion unit's decreased mobility and arterial backup.
Para-articular and paraforaminal traumatic edema.
Eccentric compression stress upon the IVD and the apophyseal cartilages.
Possible separation of minute fasciculi of the retaining fibers of the anulus, joint capsule, dural root sleeve, and nerve root sheath.
Stress insult of the proprioceptive bed.
Minute crushing of the periosteal margins with resultant proliferative irritation.
Minute tearing of the attachments of the dural root sleeves if they attach to the lining of the IVF.
The following pathologic changes typically occur:
Extravasation and edema, along with the precipitation of fibrinogen into fibrin, result in interfascicular, foraminal, articular, and capsular thickening and adhesions that restrict fascicular glide, ingress and egress of the foraminal contents, and the competent movement of the vertebral segment within its articular bed. Whenever there is extravasation, mineral salts are precipitated and infiltration and sclerosis commonly result.
Binding adhesions may develop between the dural root sleeves and the nerve roots within the interradicular foramen and between the spinal nerve root sheath and the inner margins of the IVF. When subjected to microtrauma, mesenchymal connective tissue undergoes a relative rapid and extensive degenerative change that is characterized by a loss of functional integrity and substance.
Proprioceptive Responses and Reflexes
The most significant effect is likely that of proprioceptive irritation. The musculoskeletal tissues and particularly the ligaments and paravertebral or intervertebral musculature of the spine are richly endowed with proprioceptive receptors.
First, when overly stimulated by stretching, these neurons interpret the stimuli as somatic sensory stimulation that may be perceived as pain.
Second, they also may send reflexes to their motor components to produce changes within the paravertebral muscles or elsewhere in the soma supplied by the segment.
Third, they may be interpreted as viscerosensory stimuli, whose visceromotor response alters circulatory changes, smooth muscle activity, glandular secretions, or trophic activity in the musculoskeletal tissues or viscera supplied. It is this vast ability of the proprioceptive sensory beds to influence motor changes, both of a somatomotor or visceromotor nature, that is perhaps the most universal effect of vertebral subluxation.
Direct Nerve Pressure
Nerve roots are normally well protected from trauma by the bony border of the IVF and the tough fibrous dura. However, Schaumburg shows that when distorted by degenerative bone and joint disease or a variety of space-occupying lesions, these same protective layers may damage the delicate neural structures.
Direct nerve pressure may come from the misaligned osseous segment itself or from various soft-tissue pathologies causing or affected by the mechanical fault such as contractures, adhesions, inflammatory residues, atrophies, cysts and tumors of related tissues. Direct physical nerve pressure may be responsible for motor alterations and sensory disturbances within this particular nerve and its innervated structures or cause other ramifying reflexes.
Research findings described by Sharpless indicate that the posterior nerve roots are about five times more susceptible to compression block than a peripheral nerve. As little as 10 mm Hg pressure held for 15-30 minutes reduces the compound action potentials of posterior roots to about half their initial value. This effect is thought to be due to mechanical deformation rather than ischemia since the larger fibers are blocked first. It is believed that anoxia affects the small fibers first.
Ganglion Irritation/Compression
Because of its juxtaposition to the IVF, another important factor to be considered is that of irritation/compression of a posterior root ganglion. The ganglion of each spinal nerve generally lies within the upper medial aspect of the IVF, a precarious position. Whenever the transverse diameter of the IVF is modified, the ganglion may be subject to compression and irritation.
This is especially true at the cervical level where it tends to occupy the medial limits of the IVF and is thus vulnerable to and most likely to become involved in any changes in IVF diameter on any event of trauma or the manifold processes of spondylosis. For example, an acute whiplash-like mishap to the cervical spine, especially of the hyperextension type, may force the vagus and the superior cervical sympathetic ganglion against the transverse processes of the atlas and axis, often provoking bizarre autonomic reactions.
Intraneural Effects
It is probable that any interference with or abnormality of the interstitial fluids in which the nerves lie and/or the intracellular fluid of the nerve body itself or the nerve axoplasm will cause a breakdown of the sodium pump mechanism that will prevent the normal flow of impulses along the nerve fibers concerned. These abnormal impulses refer to an overaction or underaction in the rate of impulse frequency along the nerve. Once a threshold stimulus has been reached, a nerve will fire according to the all-or-none law.
Meningeal Irritations
Biomechanical errors in motion and position may place compressive or tractional forces upon the meningeal coverings of the cord or dural root sleeves that may produce mechanical pressure upon the neurons and CSF-flow emanating from the cord itself. These may, therefore, cause the elicitation of abnormal neurologic motor effects or sensory interpretations.
Altered Nerve Root Level
Any induced disrelationship between position level and course direction of nerve root origin (spinal cord) and nerve root exit (IVF) is an important factor to consider. Whenever there is subluxation, changes in normal curves, or the presence of abnormal curves, the relative levels of points of nerve root origin and exit are altered and the nerve root becomes vulnerable to encroachment compression or irritation.
This results whenever the normal curves of the spine are grossly modified (eg, kyphotic deviation of the cervical spine, lordotic exaggeration of the lumbar spine, scoliotic deformity especially at the cervicobrachial area and lumbosacral junction), the nerve root is forced to assume an unusual approximation to one or the other walls of the IVF. Thereafter, the least additional deviation may precipitate a nerve root irritation syndrome.
In addition, a vertebral column affected with partial fixation of several segments when subjected to flexion, extension, and circumduction efforts will suffer marked tension upon the dural root sleeves and the related spinal nerve, especially the cauda equina.
If one or more vertebral segments are functionally embarrassed for any reason by abnormal motor action, added articular and proprioceptive responsibility is imposed upon the segments above and below the involved area. Thus there is an extension of harmful effects that may have noticeable complications. In addition, the phenomenon of bipedism neurologically necessitated the development of an ascending and descending reticular activating mechanism.
It can be assumed that spinal and pelvic interosseous disrelation may overstimulate the ascending portion of the reticular activating mechanism. On the other hand, excessive psychic stress may, by means of the descending portion, provoke overstimulation of the cellular elements in the anterior and lateral horns and provoke abnormal somatic and autonomic reactions.
Paraforaminal Adhesions
Paraforaminal adhesions as the result of stress and traumatic edema often result in a painful restriction of the normal back-and-forth glide (1/4-1/3 inch) of the nerve root within the IVF. Symptoms simulate a low-grade radiculitis: increased pain on movement, straining, and stretching; pain on changing positions and when placing the involved part in extension.
Circulatory Changes
Restricted mobility (eg, vertebral fixation) of a motion unit within its normal physiologic range of movement may cause sluggish lymphatic or vascular circulation that is further influenced by mechanical pressure. This can cause chemical or physical changes within tissues such as anoxia, toxicity, swelling, edema, etc, and the consequent derangement of normal function brought about by these disorders.
Local irritation at the site of misalignment and a decreased ability to move produce an inflammatory reaction with edema leading to a disturbance in the normal exchange of nutrients and waste products between capillary and extracellular fluid. Added to this stasis is the probable factor of lactic acid buildup in the area because of leakage from the surrounding hypertonic muscles.
Local Toxicity Effects
Venous stagnation from arterial backup can produce local toxicity at the spinal level. While toxic metabolic end products (eg, urea, uric acid, creatinine, lactic acid) accumulate in the stagnant tissue and congested capillary beds, there is also a corresponding decrease in nutrient and oxygen concentration in these fluids. Thus, the nerves emanating from the involved area will be deficient in necessary nutrients and quite possibly hypoxic as well.
The buildup of metabolic waste products in the area of the IVF, also may alter the normal pH of local fluids causing a breakdown of the Krebs cycle, due to decreased oxygen and toxicity, which causes a partial breakdown of the sodium pump mechanism, resulting in an ionic imbalance. As the sodium pump can no longer maintain a normal ionic balance, the imbalance can result in a degree of erratic nerve conduction and edema in the tissues of the immediate area. This erratic nerve conduction may be exhibited in all fibers passing through the involved IVF and immediate area.
When toxicity occurs in either the central or peripheral nervous systems, the formation of acetylcholine at the level of involvement will be interfered with and result in further disturbances due to increased nerve conduction impairment. This situation along with the toxicity effects upon the nerve may well result in abnormal membrane permeability leading to dysfunction.
Cerebrospinal Fluid Flow Alterations
This category of disturbances relates to the mechanical effect upon the flow of CSF within the CNS and perhaps within the nerve roots. CSF stagnation possibly occurs in association because of the intimate relationship between spinal fluid and venous blood, contributing to toxicity in the nerve root area.
According to some researchers, minute pressure on meninges alters the flow of CSF and interferes with its ability to remove wastes and provide nutritional substances to the cord and nerve roots. This may be either the effect of direct mechanical pressure or impairment of motion necessary for proper intake and outflow of this nutrient material.
Distal Neurologic Manifestations of Subluxations
Because of the effects of the subluxation's microtrauma and the consequent pathologic changes involved, the neurologic insult may result in:
(1) modification of the basic chronaxie;
(2) alteration of normal impulse amplitude, wave length, and force intensity; and/or
(3) extension of the refractory period.
The neurologic manifestations of a subluxation are not always indicated by the response the nervous system makes to irritation not external to it (ie, discernible in its immediate area), but rather from within the body. Thus, it can be an intrinsic source of neurologic irritation. This altered state of nerve-fiber threshold and the impulse proper leads to dysfunction of the sensory, motor, vasomotor, and spinovisceral responses.
Possible distal manifestations of vertebral subluxations are shown in Table 6.8.
| Acroparesthesia
Angioneurotic edema Cutaneous discolorations Cutaneous flushing or pallor Decreased electrical resistance of skin Dermatographia Fasciculation Formication Gastrointestinal sphincter spasm or inefficiency Hyper- or hypo-esthetic areas Hyper- or hypo-hidrotic areas Hyper- or hypo-peristalsis Hyper- or hypo-reflexia Hyper- or hypo-thermic areas Hyper- or hypo-tonicity Hypertrophy or atrophy Increased flare to scratching Increased or decreased gastrointestinal secretions Increased or decreased glandular secretions Increased or decreased strength Local swelling Malcoordination Mucous membrane congestion or blanching Myocardial spasm or inefficiency | Neuralgia and neurodynia Pain and tenderness Cutaneous and subcutaneous Deep muscular Somatic Visceral Periosteal Postural fatigue Abnormal somatospinal reflexes Abnormal viscerospinal reflexes Diaphragmatic dysfunction Gait disturbances Lymphatic traction or compression Mediastinal displacement Nerve traction or compression Organic displacement Respiratory inhibition Sustained postural stress Vasculature traction or compression Visceral support stretching or shortening Visceral traction or compression Visceroptosis Proliferation or degeneration Sluggish movements Tics Tingling Tremor |
Dysfunctions in the vasomotor field include angioneurotic edema, flushing, mucous membrane congestion, urticaria and dermatographia, vasospasm, and blanching. Minor changes in the circulation of the skin can be crudely measured indirectly by various heat sensitive devices, thermography, or infrared photography. Such changes often parallel circulatory changes in the deeper tissues as they too are affected by similar vasomotor responses.
Changes in the ability of the skin to secrete oils or perspiration can be measured by various electrical resistance instruments. These secretory errors also may be indicative of similar changes in deeper visceral tissues. Hyperhidrosis or dryness, as well as hyperesthesia or hypesthesia, in a local area near the spine implies altered vasomotor activity in the subsequent spinal segment. Hyperesthesia and hyperhidrosis are usually associated with an increased flare (red response) from scratching and a decrease in electrical skin resistance.
Dysfunction in the spinovisceral field may include visceral smooth muscle abnormalities, glandular and mucous membrane secretory malfunctions, and sphincter spasms of the detrusor muscles and myocardium.
Alterations in the quality of tissue may result from trophic disturbances such as atrophies, degeneration, thinning or discoloration of the skin, or other changes that reflect viscerotrophic abnormalities.
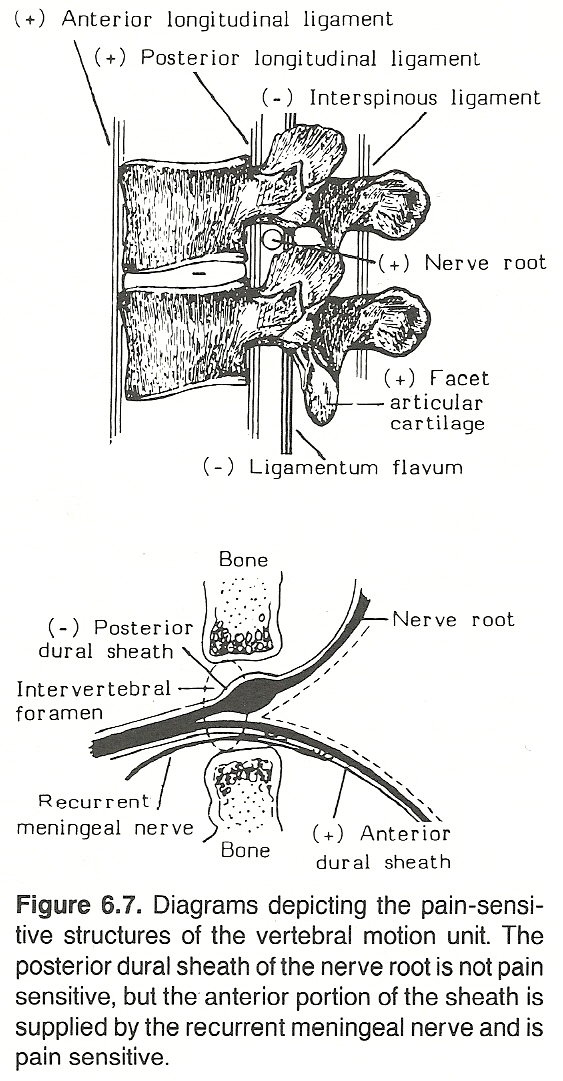 |
Each vertebral motion unit derives high-threshold sensory fibers from:
The usually two fine branches of the recurrent (sinuvertebral) meningeal nerve, running anterior to the spinal nerve in the IVF. An autonomic branch from the paravertebral plexus accompanies the recurrent spinal nerve, usually within the same sheath. These supply the anterior dura, blood vessels of the spinal canal, posterior longitudinal ligament, cortex of the vertebral bodies, and the surface of the posterior anulus. Fibers rarely enter the central IVD. Communicating and linking branches extend across, up, and down at least one segment, and frequently produce radiating or referred symptoms.
The medial branch of the posterior primary ramus. These fibers supply the ligaments and muscles of the posterior aspect of the vertebral unit. As in all synovial joints, the capsules of the articular processes, their fat pads, and their intrinsic and extrinsic ligaments are richly endowed with pain and proprioception receptors. This nerve also sends communicating and linking branches across, up, and down a few segments.
The vertebral joint proper receives innervation from rostral and caudal segments besides those from the local segment. This means that a segmentally arranged nerve supply (with its specific dermatomes, muscles, and reflexes) is not available to evaluate a particular specific vertebral motion unit with certainty.
Nerve Fiber Proportions
There are about three times more sensory fibers than motor fibers in the cervical area, one and a half more in the thoracic region, and twice as many in the lumbar area. This thought should be kept in mind during palpation.
Pain Distribution
When the anterior root is irritated, pain is felt in the muscles supplied (ie, with myotomal distribution) and often becomes self-perpetuating from the focal spasm produced (eg, a trigger-point syndrome). When the posterior root is irritated, the pain is usually perceived in a dermatomal distribution.
The Autonomics
As the autonomic nerve pathways innervating musculoskeletal tissues are intimately connected with the spinal nerves, it can be recognized that these systems do not operate in isolation. Structural disorders in the spine frequently cause, contribute to, or mimic such "functional" disorders as Meniere's disease, causalgia, shoulder-hand syndrome, asthma, sphincter spasms, cluster headaches, angina, and a large variety of referred pains.
Nerve Root Insults
As described previously, disturbances of nerve function associated with subluxation syndromes can manifest as abnormalities in sensory interpretations and/or motor activities. These disturbances may be through one of two primary mechanisms:
(1) direct nerve or nerve root disorders, or
(2) of a reflex nature.
If direct involvement occurs on the posterior root of a specific neuromere, it manifests as an increase or decrease in awareness over the dermatome; ie, the superficial skin area supplied by this segment. Such manifestation is usually tested with a cotton wisp and pinwheel. Typical examples might include foraminal occlusion or irritating factors exhibited clinically as hyperesthesia. For example, abnormal sensitivity often occurs on the posterior and lateral aspects of the thumb and radial side of the hand, when involvement occurs between C5-C6.
At other times, this root involvement may cause hypertonicity and the sensation of deep pain in the musculature supplied by this neuromere; eg, C7 involvement, with deep pain in the triceps and supinators of the forearm. In addition, direct pressure over the nerve root or its distribution may be particularly painful.
Cyriax gives the cardinal signs of nerve pressure as:
(1) pain on stretching the nerve,
(2) the provocation of paresthesia (eg, pins and needles) on motion,
(3) swelling and tenderness over the nerve sheath,
(4) postural deformity, and
(5) evidence of secondary parenchymatous changes in the nerve (eg, impaired conduction during electrodiagnosis).
Prolonged and/or severe nerve root irritation also may produce evidence of trophic changes in the tissues supplied. This may be characterized by apparent atrophy, but such a sign is particularly objective when the circumference of an involved limb is measured at the greatest girth in the initial stage and this value is compared to measurements taken in a few weeks later. It is for this reason that the circumferences of the thigh, leg, forearm, and upper arm are measured and recorded during many standard examinations.
Motor Manifestations
Nerve root insults from subluxations may also be evident as disturbances in motor reflexes and/or muscular strength. Examples of these reflexes include the tendon reflexes such as seen in the reduced biceps reflex when involvement occurs between C5 and C6, the reduced triceps reflex when involvement occurs between C6 and C7, or the reduced patella and Achilles tendon reflexes when involvement occurs between L4 and L5. These reflexes also must be compared bilaterally to judge whether hyporeflexia is unilateral; unilateral hyperreflexia is pathognomonic of an upper motor neuron lesion.
Muscle strength may be tested in various manners, depending upon which muscles are involved; the primary purpose being to compare the isometric strength of resistance against counterpressure. For example, the strength of the biceps (C6-C7), triceps (C6-C7), anterior tibialis (L4-L5), and gastrocnemius (L5–S1) muscles are commonly tested.
The Posterior Rami
The posterior rami turn sharply backward to supply the spinal muscles and skin of the back. Sunderland emphasizes that the passage of cutaneous branches through the muscles and fascia of the back should not be overlooked as potential sites of entrapment. Such entrapment is most frequent of the greater occipital nerve and the cutaneous branches of the posterior rami of L1–L3 nerves.
A few posterior rami intermix branches, but most remain segmental. The anterior rami run ventrally and laterally, and most enter plexuses or connect with sympathetic fibers via the rami communicantes, whereafter their specific identity is difficult to determine. In the fused sacral region, the anterior and posterior rami, respectively, exit the bony canal through the anterior and posterior foramina.
Tenderness of the rami of the posterior division has particular significance in the palpatory examination of the spine. The sensory distribution runs in a zone extending from the posterior scalp to the coccygeal area and then laterally to the greater trochanter. See Tables 6.9 and 6.10.
| Average Diameter | |
| 1 mm | |
| 2-1/2 mm | |
| 1-1/4 mm | |
| 1-1/2 mm | |
| 2 mm | |
| 1/3 mm | |
| 1 mm | |
| 1/2 mm | |
| 1/4 mm |
| ARami | |
Adjacent muscles, filaments to capsule of atlanto-occipital joint and connections with the anterior branch of C2. | |
The posterior branch supplies and overlying skin, adjacent muscles, and adjacent facet joints. The anterior branch (greater occipital nerve) passes horizontally across the inferior oblique muscle beneath the semispinalis capitis as it transverses vertically and then proceeds within the fascia of the trapezius to the scalp where it divides into numerous twigs that extend as far anterior as the coronal suture. Filaments supply the occipital and superficial temporal arteries. Impulses initiated at the C2 level of the cord in the greater occipital nerve merge with those of the C2 level spinal nucleus of the trigeminal. Thus, this nerve is often involved in suboccipital pain and occipitofrontal headache. | |
| The posterior branch supplies overlying skin and superficial musculature. The anterior branch divides with one branch winding around the facets of C3 and another communicating with the greater occipital nerve. | |
This plexus is formed by the posterior rami of C1–C3 and sensed as cervical a mass of neurovascular tissue lying beneath the semispinalis capitis plexus muscle and as such is quite vulnerable to cervical strains, whiplash-type trauma, and subluxation syndromes. | |
Medial branches essentially supply overlying skin and superficial muscles, and the lateral branches essentially supply the deep muscles of the cervical region. As the nerves cross around the faces of the articular masses between the superior and inferior articular facets, these nerves are quite vulnerable to entrapment. The posterior rami of C8 follows a groove in the superior aspect of the 1st rib and is often involved in a cervical rib or scalenus anticus syndrome. | |
The posterior branches of the upper thoracic nerves are accompanied by the posterior arterial branch of the thoracic aorta as they pass posteriorly via an osseofibrous canal located about 2 cm from the midline. A shorter segment lies transversely between the costotransverse ligaments prior to dividing about 2.5 cm from the midline into terminal branches. The medial branches pass medioinferiorly, send twigs to nerves above and below, and supply adjacent muscles, ligaments, and joint capsules. Cutaneous branches must pierce the trapezius (3–4 cm from the midline) and pass laterally to supply the overlying skin. Thus, numerous areas of possible entrapment occur in the course of these nerves. | |
The posterior divisions of the lower thoracic nerves differ somewhat from those of the upper thoracic nerves. The medial branches are essentially muscular and supply the supraspinous and interspinous ligaments, but they have no cutaneous twigs. The larger lateral branches take an oblique course, emerge from the sacrospinalis, and follow the thoracolumbar fascia. | |
Small, short trunk sinuvertebral nerves enter the canals and are continued distributed to the vertebral arches and posterior facets, veins, sheath surrounding the dura matter, and communicate with the sympathetic chain. Thus, these nerves have two components: one from the spinal nerve and the other from the sympathetic chain. The spinal nerve portion arises just lateral to the posterior root ganglion and is often double. The fine sympathetic twigs arise from the rami communicantes. | |
|
| The relatively small posterior division of lumbar nerves splits from the anterior division at almost a right angle as it projects backward and enters the posterior compartment via an osseofibrous tunnel as it forms partnership with other members of the neurovascular bundle. Some branches quickly course medially (about 5 mm from their origin) and divide into a medial branches and lateral branches:
The lateral branch of the posterior ramus of L5 nerve descends vertically in a groove on the sacral ala just lateral to the S1 articular process to join the lateral branch of S1. The medial branch of L5 curves medially under the lumbosacral apophysis and sends branches medioinferiorly and posterior into the local multifidus muscles and lumbosacral ligaments. |
These nerves form a plexiform arrangement on the back of the sacrum. The lateral branch of S1 joins with that of L5. The lateral branch of S2 projects downward over the sacrum just lateral to the 3rd and 4th foramina and joins the lateral divisions of S3 and S4. All these nerves lie between the interosseous and overlying sacroiliac ligaments, which are supplied by the lateral branches of the L5–S3 posterior rami. The fine medial branches of S1–S4 supply the multifidus muscle. |
Note: Above data adapted from Bradley with modifications.
________________________________________________________________
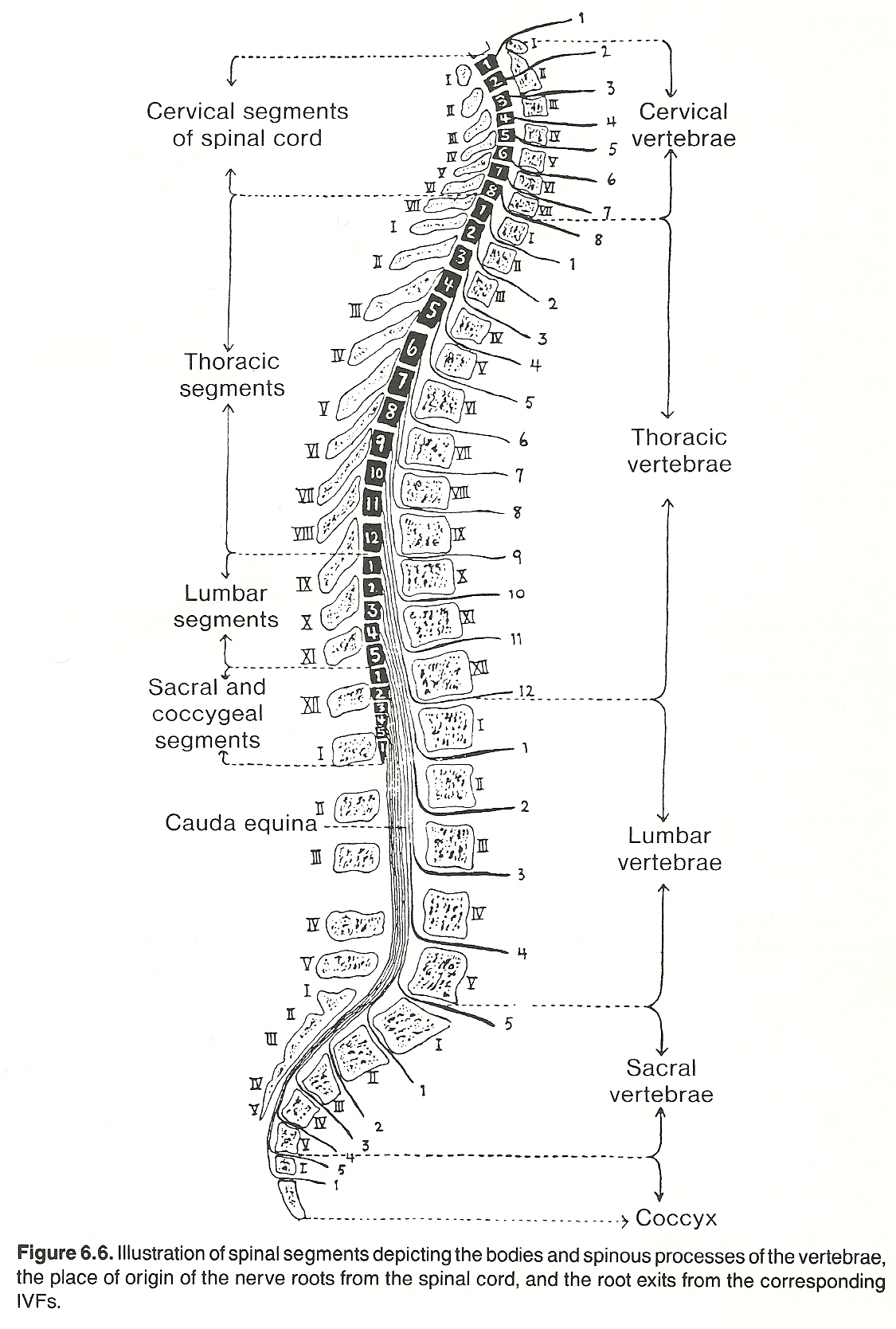
The spinal cord, continuous with the medulla oblongata at the foramen magnum, is protected within the spine anteriorly by the posterior aspect of the vertebral body and IVD, posteriorly by the bony laminae, and laterally by the pedicles. Further protection and stability are provided by the cord's three membranes, the two fluid-filled spaces, the ligamentum flava and dentate ligaments, and the nerve root sheaths.
(1) the cervical segments (C4-T1) to supply the brachial plexus, and
THE VERTEBRAL CANAL AND RELATED TISSUES
To accommodate necessary innervation for the limbs, the spinal cord is enlarged at:
(2) the lumbosacral segments (L2-S3) to supply the lumbar and sacral plexuses. The average sagittal diameter of the adult cervical vertebral canal is 18 mm.
Cord-Canal Relationships
Relative to the origin of the 31 pairs of spinal nerves, a spinal cord "segment" does not necessarily correspond in height or location to its corresponding numbered vertebra and disc, spinal nerve, or the level of the spinous process. The cervical spine contains eight cord segments; the thoracic spine, about 20 segments; and the lumbar spine, probably only a few sacral and coccygeal segments. The adult spinal cord can generally be considered to occupy only the upper two-thirds of the vertebral canal. Exact depth is quite variable.
In the embryo, the spinal cord and vertebral canal are about equal in length until about the 10th week. Because the vertebral column grows faster than the spinal cord, this relationship does not persist. The cord ends near the level of the L3 disc at birth; the L2 disc at age 5; and higher in the adult. This is usually near the level of the L1 disc. Occasionally, it is seen at surgery to terminate in the adult as high as T12 or as low as L3. As the lower third of the vertebral column is approached, the length and obliquity of the nerve roots must progressively increase to reach their respective IVFs.
The vertebral canal increases in length during spinal flexion and lateral bending, and decreases in length during extension. Illi has shown that the amount of linear change is considerably reduced because of the flexion-rotation coupling that occurs. Because of its substantial degree of flexibility, the cord readily adapts to normal lengthening and shortening of the canal during motions.
The Meninges
The spinal cord is sheathed by three cylindrical membranes that extend from the foramen magnum to the midsacral region: the internal pia mater, the middle arachnoid, and the exterior dura mater. These membranes tightly invest the spinal roots and cord, and their extensions surround the cauda equina and fuse at the external terminal filum.
The Dentate Ligaments
The 20 or 21 dentate (saw-toothed) ligaments derive from thickened pia mater. They are inferiorly inclined and extend bilaterally between the anterior and posterior nerve roots from the foramen magnum to the T12-L1 area, penetrate the arachnoid and its fluid-filled spaces, and fix to the inner surface of the dural membrane. They provide a unique pretensed suspension system against sudden jars. It is because of the dentate ligaments that the spinal cord and its roots, but not the rootlets, are put under tension during spinal movements.
The Spinal Cord Proper
Cord Flexibility
Although dentate ligaments help to stabilize the spinal cord in a central position in the canal and help to protect against undue stretch, the cord is still flexible enough (10% of length) under small loads to move as much as 3/8 inch. The cord is quite elastic when deformed axially, but prone to severe damage if a vertebra is displaced horizontally.
A space-occupying sclerotic or fibrotic lesion will restrict the cord's mobility and extensibility and thus increase tensile, torsion, and compression stresses. The symptoms thus produced can be alleviated if the cord can be relaxed.
Grieve proposes that if a biomechanical evaluation could be conducted at the microscopic level routinely in clinical practice, many neurologic disorders in which no mechanical component is suspected would be shown to have their origin in tension of nervous and vascular microtissues that produce a reduction of conduit diameter that interferes with function. We should be reminded here that the founder of chiropractic stated before the turn of the century that "chiropractic as a science is founded on tone."
Cord Folds
In its neutral state, the cord possesses accordion-like folds that flatten on stretch (flexion) and increase on relaxation (extension). This folding and unfolding mechanism is responsible for about three-fourths of the cord's change in length from full flexion to full extension. Once these folds have flattened during flexion, the cord is subjected to direct tensile forces. As a rubber band, the diameter of the cord then reduces on stretch and increases on relaxation.
The Cervical Cord
As maximum cervical movement is at the C5-C6 level and the spinal cord snugly fills the cervical canal, arthritic changes and disc herniations in this area may encroach upon the canal contents. As the cervical cord is at its maximum width at this level, injury may readily lead to neurologic damage.
The Lumbar Cord
The spinal cord ends near the L1 disc. Below this, the elements of the cauda equina are within the vertebral canal of the lumbar spine. The mobility of the cauda equina roots in the relatively large canal provides a safety factor not found in the cervical or thoracic regions. This safety factor, however, is minimized in spinal stenosis.
POSTURAL AND STRUCTURAL EFFECTS
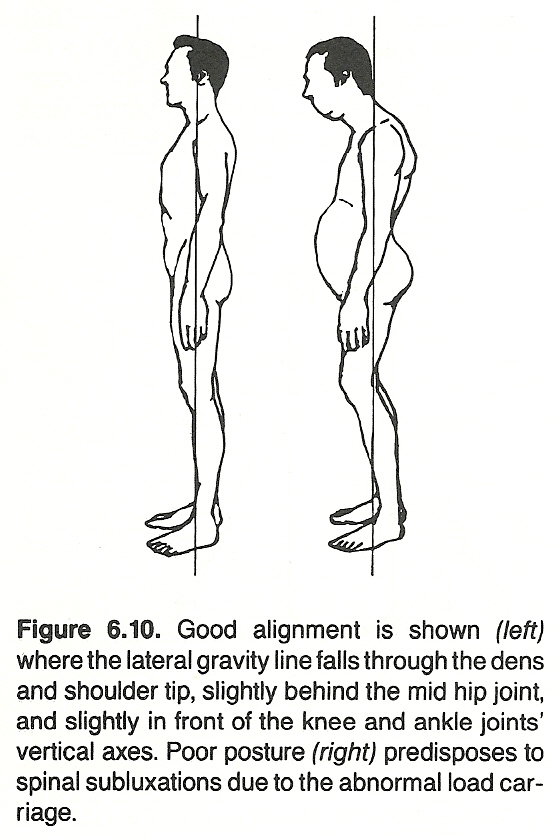 |
An individual's posture can be defined as the relationship of each body structure to the entire structure. Normal posture is that posture which best suits individuals according to their internal and external environmental conditions.
The Effects of Bipedism
An adult spine without discs would resemble that of the newborn. Since animals that walk on four legs and infants prior to assuming the erect position do not have the physiologic curves of the erect adult, it is assumed that these curves are the result of bipedism. In the erect position, the lower lumbar area is especially subjected to considerable shearing stress.
The biped stance requires recognition of certain anatomical considerations to recognize that the spine and pelvis are of clinical importance because of their intimate involvement with the nervous system. In the human biped, there is a unique relationship between the musculoskeletal mechanism and the neurologic bed. The neurologic factors that relate to bipedism represent a rationale of clinical chiropractic that is often readily portrayed during dynamic postures.
Human architecture is much like a triad of three superimposed inverted triangles in which strain and stress are greater at certain points than at others. Within the zone of these points of primary function and stress, there is a relatively heavy deposition of sensory nerve endings and motor end plates.
When these areas, heavily populated with neuronal and vascular ramifications, are subject to trauma, occupational stress, the strains of postural fatigue, and abnormal viscerospinal reflexes, the process of transudation, fibrin precipitation, and adhesion formation ensues to establish an intramuscular and myofascial trigger point. To this must be added the principle of neurologic facilitation and spread. Not uncommonly, there is a musculoskeletal syndrome complex that challenges the reserves of the most healthy.
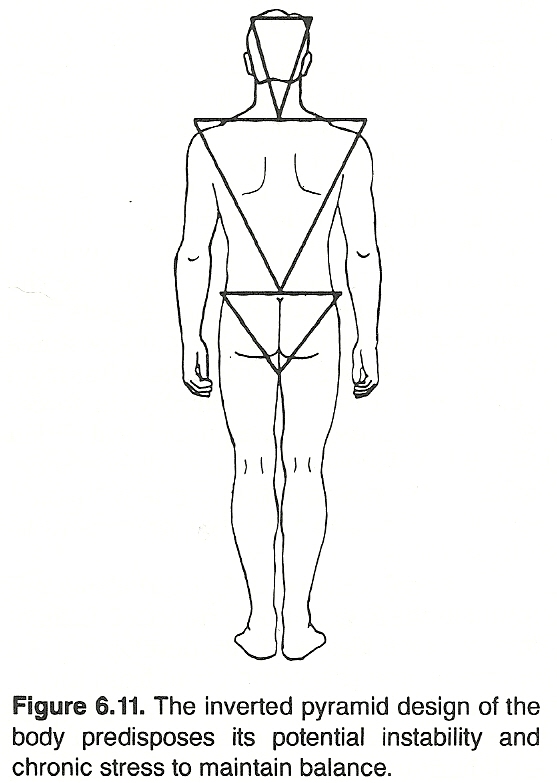 |
Bipedism underlies the clinical concern of gravity and weight bearing, postural faults, strains and stresses of occupation, play, and trauma. Because of such stress, the articular, syndesmotic, and myologic proprioceptive complex is often disturbed. This results in the development of many common spinosomatic and spinovisceral syndromes. A deranged spinal or pelvic segment within its motor bed will invariably result in disturbance of the proprioceptive bed with facilitation of the discomfort/pain phenomenon.
Pelvic Posture Considerations
When erect, body weight and any extrinsic loading of the upper body are transmitted from L5 to the sacral base, the sacroiliac joints, ilia, and ischia. Impact forces from below arise from the foot through the tibia and femur. These axial forces meet at the acetabulum and are primarily dissipated transversely, to be absorbed by the cartilages and ligaments of the hip joints, sacroiliac joints, symphysis pubis, and the spongiosa of pelvic bone.
The gross effect is locking of the involved joints by opposing forces traveling around each side of the pelvis anteriorly and posteriorly from the acetabulum. If these counterdirected axial forces are not equalized, the pelvis would not be in a state of equilibrium according to Newtonian principles. When the force from below is greater, the head of the femur tends to jam within the acetabulum. If the force from above is greater, the L5 and S1 end plates or sacroiliac joints tend to displace.
Structural-Functional Relationships
Research data strongly suggests that sensory afferent impulses may play an important role relative to the maintenance of dynamic equilibrium of the human body to its environment. Overstress of muscles, tendons, and ligaments brings about a change in patterns of afferent nerve impulses that are fired from their nociceptors and mechanoceptors and transmitted to the CNS. It can be hypothesized that, because of these changes, stress develops that affects not only the body's dynamic equilibrium with the forces of gravity but also possible visceral dysfunction, and, in turn, visceral disorders influence the body's dynamic equilibrium.
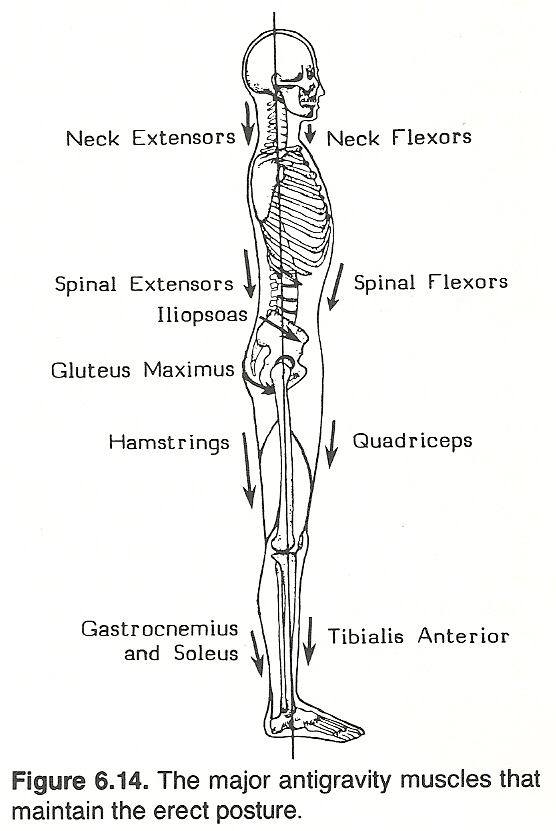 |
Balance Considerations
No two individuals react identically to actual or potential loss of body balance. All vary somewhat in the accommodation process, depending upon one's gross structure and functional capabilities, the momentary potential for redistributing body mass, and the visual efficiency necessary to guide correct accommodations. Irregularities of postural control can be expected to result in deviations from normal standing values.
The symptomatic picture of balance defects is often unclear because individuals vary so much in response to mechanical insult. Some people present with immediate symptoms upon slight deviation, while others offer no symptoms until pathologic changes are in progress. Much of this is determined by how the body is used; eg, occupational and athletic considerations.
Within normal parameters, according to Fernie/Holliday, healthy people have a slightly variable mean speed of postural sway and range of movement in the sagittal and coronal planes. Vision also affects these values significantly, as shown in differences between eyes-open and eyes-closed tests. Studies of normal subjects and amputees show that postural sway increases with age, but the visual dependence for the control of sway is unaffected by age.
Spinal subluxations are often the forerunners of balance defects brought through the effort of the spinal column to compensate for the stress and thus to reduce the more serious effects. Balance defects also may originate from habitual faulty postures in standing, sitting, and lying, as well as from activities that constantly employ the forces of the large muscles in asymmetrical action. When created, such defects serve to lessen the power of the body to withstand shock and are, in turn, the precursors to subluxations.
Additional causes of defects in balance are found in the frequent occurrence of unequal lower extremities, in faulty development of vertebrae and the sacrum, and from the effects of abnormal reflexes. The least common causes of balance defects can be attributed to inheritance and disease. Constitutional stress, visceral malfunction, nutritional status, fatigue and debility, neuromuscular tension, a large variety of psychologic factors, height, weight, and body type all combine to express themselves in one's posture, body balance, and motor ability.
Most balance faults witnessed in practice will be within "physiologic" limits without obvious structural deformity, yet it should be appreciated that abnormal function leads to reduced performance capabilities early and to pathology later if left uncorrected. Isolated muscle weakness should be suspected especially in situations of head or pelvic tilt, trunk imbalance, scoliosis, and uneven gait or limp.
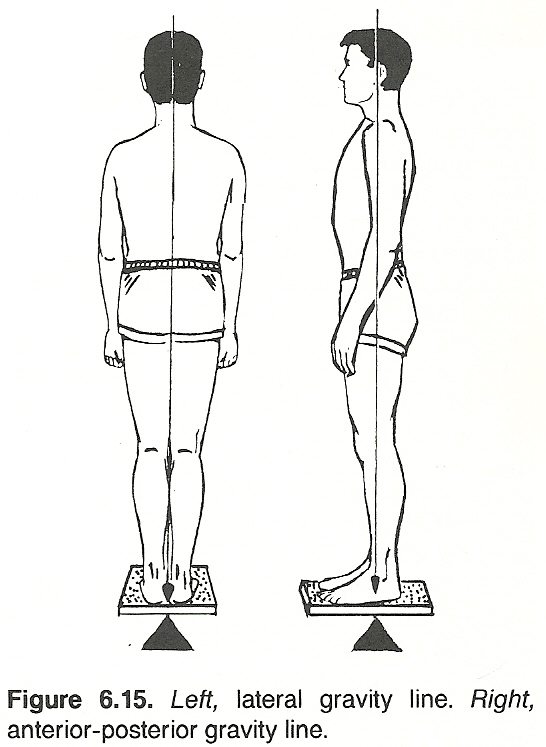
| Conditioned reflexes | Physiologic abnormalities |
| Gravity | Pathology |
| Emotional states | Endocrine disorders |
| Anxiety | Joint disorders |
| Depression | Myopathy |
| Joy | Neuropathy |
| Environment | Structural anomalies |
| Clothing | Lower extremities |
| Occupation | Organs and tissues that attach to or suspended from the spinal column |
| Social customs | Pelvis |
| Weather | Upper extremities |
| Ground angle | Vertebral column |
| Ground surface | Structural malpositions |
| Heat and cold | Dislocations |
| Wind | Fractures |
| Fatigue | Subluxations |
| Pain |
| Aerophagia Albuminuria Anorexia Arthralgia Circulatory impairments Constipation Digestive disturbances Drainage impairments Dysmenorrhea | Fatigue Gait disturbances Increased energy requirements Intolerance to stress Intrafascicular adhesions Irritability Lowered immunity | Myalgia Neuralgia Pseudoemphysema Reduced endurance Resp. inefficiency Trigger points Visceral dysfunctions Visceroptosis |
(1) the structures upon which the strain is imposed, or
(2) the cutaneous branches of the spinal nerve root supplying the strained tissues.
Long-term muscle strain results in adaptive changes in the joints and ligaments to meet the needs of the malaligment. Thus, low-key chronic sprain is a part of the picture. Abnormal fatigue is the result of wasted energy.
The more pronounced an abnormal spinal curvature, the greater becomes the mechanical disadvantage to which the supporting structures are subjected. Thus, the process is a vicious cycle. Along with chronic stress and fatigue, constant pull causes small tears in ligamentous attachments. This results in a series of subperiosteal hemorrhages that may later calcify into exostoses, becoming extremely painful upon further stress. Such a situation may occur in any joint that is subjected to prolonged strain, but it is especially common in the spine and other weight-bearing joints.
Raphael points out that, besides postural stress, the effects of cumulative or repetitive trauma should not be neglected in any discussion of functional stress and fatigue. "Not only is poor posture a predisposing factor to subluxations but also overuse of muscles which lead to myofascial pain syndromes and subluxations."
Neurologic Considerations
There usually is some degree of IVF insult present in spinal malalignment effected by improper balance. Exaggerated cervical or lumbar lordosis, for example, decreases the size of the IVFs and frequently leads to chronic radiculitis. Neuralgic pains in the thorax and legs are common. Less common is intercostal neuralgia.
If originating in the cervical region and associated with hypertrophic changes, pain is often referred about the shoulders and down the arms, frequently being mistaken for angina pectoris. Similar neuralgic pains in the chest wall can be mistaken for pleurisy, pleural adhesions, or pulmonary lesions. Auscultation will serve in differentiation.
Narrowing of the IVF also may cause severe pain that has a segmental distribution perceived in the skin, muscle, or parietal peritoneum. This condition can be misleading as to origin as it mimics the presence of some intra-abdominal disorder.
Trigger Points
Concurrently with postural stress-related neuralgia, myositis, and the development of intrafascicular adhesions, similar events occur in the myofascial planes at points of major tensile stress, leading to the development of "trigger points" and the resulting delta or spread effect.
All muscles have their fascial encasements (epimysium, perimysium, endomysium); and, as muscles lie and move one upon the other, the myofascial planes are described. The amount of fasciculi involved in the all-or-none contraction effort determines the tone or strength of muscle contraction. Furthermore, a muscle usually does more work at one point of its composite than at another.
Circulatory Implications
Disturbances of vascular flow are rarely absent when postural distortions are gross. The low diaphragm results in venous congestion in its failure to assist blood returning to the heart. Sagging viscera stretch mesenteric vessels and narrow their lumen.
Duodenal stasis may be attributed to increased tension on the superior mesenteric vessels. Thus, circulatory symptoms may manifest throughout the body. Researchers have recorded the relief of eye strain and mild myopia in children by postural correction alone. They explain this as a relief of venous congestion in the head.
Such impaired circulatory inefficiency in extreme cases may be sufficient to produce a marked fall in blood pressure and loss of consciousness. This is said to be the result of general muscle relaxation with pooling of blood in the venous reservoirs, especially in the abdomen, thus reducing the practical blood volume. More often, it causes only dyspnea and weakness, sometimes accompanied by palpitation.
Precordial pain resembling angina pectoris is not uncommon. Even when heart disease exists, part of the symptomatic picture may be the result of a postural defect that tends to aggravate the pathologic defect. The marked kyphotic "stoop" of the chronic cardiac case is frequently seen.
Drainage Impairments
Faulty posture mechanics may cause the liver to rotate anteriorly and to the right. Traction is thereby exerted on the common bile duct and in some cases seriously interferes with bile drainage. Ptosis of the kidneys, especially the left kidney, results in traction on the renal veins that may obstruct venous outflow to cause passive congestion and albuminuria.
Respiratory Considerations
Respiratory balance and the maintenance of proper intra-abdominal pressure depend on good body mechanics. In the ideal attitude, the position of the well-poised head with the chest held high is important because the anterior mediastinal ligaments attached to the diaphragm originate in the deep cervical fascia and are attached to the lower cervical vertebrae.
When postural mechanics are poor, a lowered diaphragm is the rule and proper coordination of the muscles of respiration is lost. This abnormal position may decrease vital capacity by more than half. This is commonly recognized. What is not commonly recognized is the importance of the diaphragm in venous and lymphatic circulation.
Venous and lymphatic return is greatly assisted by the rhythmic contractions of the diaphragm. When the diaphragm has been lowered, it has a much shorter range of excursion and is thus much less effective as a circulatory aid. In poor body mechanics, there is always some degree of circulation retardation and improper oxygenation that results in a diminished supply of impoverished blood.
It has been shown that the respiratory difficulty of emphysema is largely due to the low position of the diaphragm (associated with the higher intrathoracic pressure), which limits diaphragmatic excursions. Thus, dyspnea is greatly relieved by a supportive device that increases the extent of diaphragmatic movements.
Because of the depressed rib angles, decreased chest diameters, and low diaphragm associated with poor posture, respiration may be deep and slow. However, it may be shallow and fast in a sitting slumped posture that causes the diaphragm to be raised by viscera pushing upward.
Digestive Disturbances
Mild digestive symptoms may exist in the apparently healthy person. This is sometimes traced to a degree of visceroptosis, which results in dysfunction of the displaced organs. Abdominal dilatation and motility disturbances are not infrequent occurrences. This is most likely the outcome of stretching of the sympathetic nerves.
Pottenger points out that stretched nerves within involuntary or voluntary muscles usually produce a temporary paralysis. In addition, when the abdominal cavity becomes shortened longitudinally, the viscera become crowded as do the glands of internal secretion and the nerve ganglia as well. Thus, orthostatic albuminuria, dysmenorrhea, and constipation may be associated.
Gynecologic Considerations
Slouching while sitting plays a dual role in its effect upon the female pelvic organs. The flattening of the chest walls and the restricted chest motion decrease the thoracic capacity to the extent that active inspiration is only permissible by forcing down the diaphragm. The result is an increase in intra-abdominal pressure that forces the intestines into the pelvis and upon the uterus, tubes, and ovaries. This is partly compensated for by abdominal protrusion; but in time, the supporting ligaments of the uterus lose their elasticity, become elongated, and displacements follow. Pioneer chiropractors were often quite skillful in correcting such prolapses.
Janse describes an article by F. N. Miller that appeared several years ago in the Journal of the American Medical Association. Miller, while professor of gynecology at the School of Medicine of the University of Iowa, showed a correlation between poor posture and such gynecologic disorders as dysmenorrhea, leukorrhea, chronic backache, constipation, amenorrhea, and complaints of pain in the sides.
According to Miller, "The fact that exercise, manipulative therapy, and body development have reduced the frequency of many of the more common female disorders (where traditional methods have failed) would indicate that the cause for these conditions may be found in faulty spinal balance rather than essentially in local lesions."
Goldthwait and other investigators have shown that spinal imbalance definitely distorts the innervation to the reproductive organs and blood vessels within the female pelvis, leaving them prone to congestion, lack of tone, and irregularity of function. In addition, poor posture permits a sagging of the abdominal viscera and their encroachment upon the pelvic contents, which in turn results in a tensile stress upon the nerves and plexuses as well as the blood vessels and organs proper, leading to a large number of functional ailments that are especially common in the female.
Postural Analysis
Gravitational forces create subluxations and spinal distortions by the constant pull of body structures toward the center of the earth. Such distortions are exaggerated by increasing the distance of the vertebrae from the center line of gravity and are decreased by decreasing the distance of the vertebrae from the center line of gravity. Thus, during spinal and pelvic analysis, it is imperative that spinal mechanics and structural deviation are interpreted from the gravitational center line, along with their neuromuscular implications, if the body is to be returned to its normally balanced position.
McDowall offers the hypothesis that primary muscle imbalance leads to vertebral instability and thus subluxation. His findings indicate that studies authorized by B. J. Palmer considered this phenomena before 1934.
Okubo reports that posturography was initiated in 1908 to analyze body motion in cases of cerebellar disease, cerebral disease, and hysteria. Allopathic research during the 1940s was primarily concerned with orthopedics, while the examination of posture through photographic and goniometric means was the trend during the 1950s.
Anatomists and neurologists no longer question the significance of the entire proprioceptive bed disposition in the ligamentous and myologic elements of the spine and pelvis. As a diagnostic aid during the evaluation of postural faults, pioneer chiropractors used a simple plumb line. In more recent years, a number of more sophisticated devices have been invented to measure postural distortions and therapeutic effects. Several types are briefly described below.
The Posturometer
While posture is an ever-changing phenomenon, some reliable baseline of measurement must be devised if postural assessment is to be considered as an integral component of chiropractic spinal analysis. In a study conducted by Vernon, 80 male subjects were assessed with a posturometer. The level of intra- and inter-observer correspondence was calculated to be in the 75% range, indicating that, with minor exceptions, a significant level of reliability was reached to provide a standard of reference for postural assessments.
An earlier posturometer survey of two beginner judo classes was conducted by Homewood. It produced data indicating typical posture. Almost all subjects showed a posterior gravity line. A right-tilted and rotated pelvis and a right low shoulder corroborated earlier studies that showed excessive weight on the right side in most subjects. A recheck after judo instruction and practice showed an improved gravity line but little change in other indicators. It was concluded that judo exercise was inferior to chiropractic in terms of correcting structural distortions.
The Gravity Stress Analyzer
This instrument (GSA) is designed to measure degrees of rotation and lateral flexion of the head, shoulders, and pelvis as they deviate from perfect alignment in the sagittal plane. In addition, deviations of C7 and 15 vertebrae in both the coronal and sagittal planes are recorded. Anderson/Winkler's evaluation of the GSA showed that it was a light-weight, quick to use (5 min or less) instrument. These investigators state that it is essential that studies be carried out to determine:
(1) the accuracy of measures recorded and
(2) the ranges of measurement that characterize normal nonpatient populations.
Photographic Imaging
The development of a static posture analysis instrument with direct application as an objective screening procedure was investigated by Hadden. It allows photographic recording of a patient's static posture and center of gravity vector. The overall accuracy was found to be N4.2 mm on a 360-degree protractor for the center of gravity vector and an overall error of N5.3 mm for measuring spinal distortion as compared to roentgenographic analysis.
Hadden suggests that the device can be used as a pre-x-ray screening instrument to:
(1) determine static biomechanics,
(2) reduce the clinical need for roentgen examination, or
(3) suggest the specific type of films required. It also can be used to evaluate immediately the effect of orthopedic appliances on static posture.
The Four-Quadrant Weight Scale
A unit to analyze posture was developed to evaluate weight-bearing in the sagittal and coronal planes. A report by Vernon/Grice found that the 4QWS instrument may assume a useful role in the chiropractic analysis of the locomotor system.
Integrated Systems
A video-integrated measurement (VIM) system was investigated by Spector and associates that incorporated the use of various noninvasive diagnostic procedures (moiré contourography, electromyography, posturometry, infrared thermography, etc) used individually or in combination for the evaluation of musculoskeletal and other disorders and their management with biofeedback and other therapeutic procedures.
The system provides for measuring individual diagnostic and therapeutic modes on a video monitor, or multiple modes by split-screen superimposition, of real time (actual) images of the patient and idealized (ideal normal) models, along with analog and digital data graphics in color, and other transduced symbolic information. It was concluded that the system:
(1) provided an innovative method by which the therapist and patient could interact within biofeedback training-learning processes and
(2) holds promise for more effective measurement and treatment of a wide variety of physical and behavioral disorders.
The reader should be alerted that specific procedures, techniques, or devices described by the author within this publication do not necessarily imply the approval or the endorsement of the American Chiropractic Association. It is recommended that doctors of chiropractic consult with their respective State Board of Chiropractic Examiners concerning the use of any specific procedure, technique, or device.
Visceroptosis
Nature provides good support for the abdominal organs when the body is normally erect. In the ideal attitude, tissue ledges and shelves exist that partially support the abdominal organs. However, if the lumbar and dorsal curves increase and the abdominal wall relaxes, these vital supports are lost.
Basic Considerations
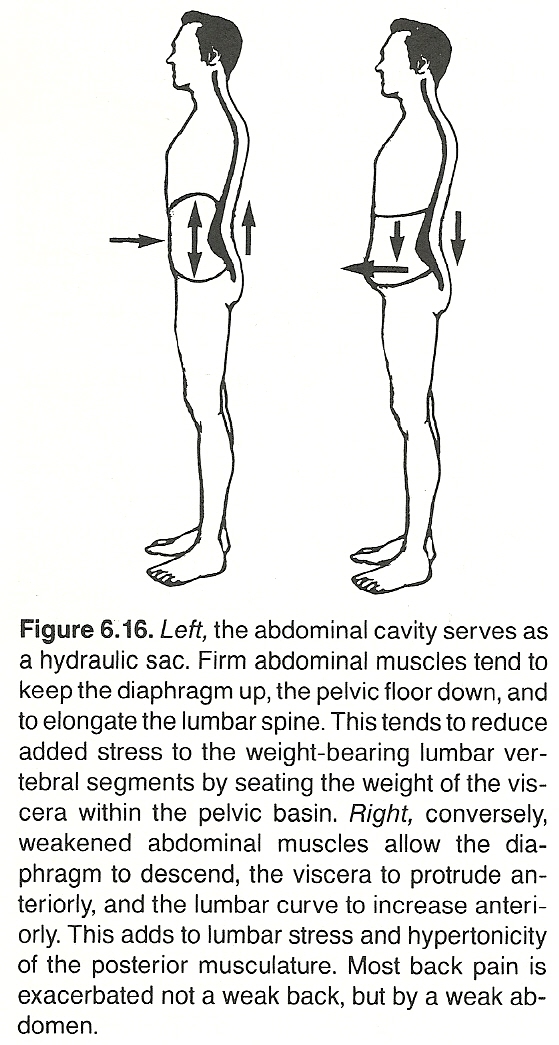 |
Abnormal body mechanics affecting the thoracic and abdominal cavities can interfere with normal function by:
(1) abnormal efferent visceral stimuli reaching organs from the facilitated segment,
(2) abnormal tensions and stretching of visceral supports, nerves, blood and lymph vessels,
(3) venous pooling as the result of inactivity, diaphragm dysfunction, organ displacement, and sustained postural stress, or
(4) abnormal vasomotor impulses to blood vessels. Blocking stress or irritation of blood vessels leads to ischemia or congestion.
There are many general effects to the body as a whole besides these local effects because each abnormal stress results in abnormal discharges of afferent impulses to the CNS, with consequent hormonal reactions that are systemic in character. Also to be considered should be the associated psychic stress that contributes to the clinical picture.
Extreme curvature and malalignment produce physiologic changes and are considered pathologic, but how much deviation is possible without causing severe impairment of health? The effect on function varies in research literature. Most all agree, however, that poor body mechanics predispose to certain visceral disorders; ie, the viscera are held in their optimum position for function in good body mechanics.
Implications
If body mechanics are good, the abdominal cavity is shaped like an inverted pear with adequate space above L4 for the abdominal viscera of an intermediate body type. Anatomical ledges and shelves exist that partially support the abdominal organs. However, if the lumbar and dorsal curves increase and the abdominal wall relaxes, these vital supports are lost.
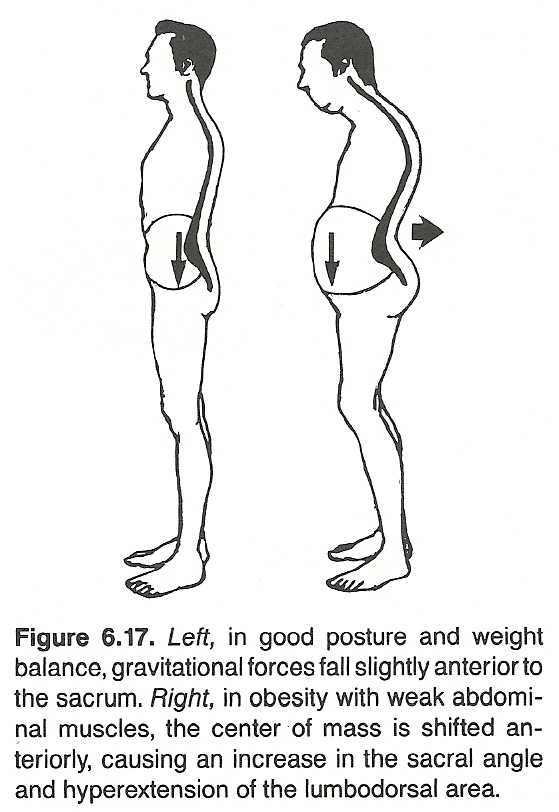 |
With the stomach lying mainly to the left of the spine and supported by a diaphragmatic attachment behind the transverse sagittal plane, there is little tendency for downward displacement of the stomach if there is no rib-cage deformity or abdominal muscle weakness.
The liver is generally posterior to the transverse sagittal plane. It is partly supported by the surrounding organs and its attachments to the diaphragm, but most of its weight is borne by the concave space at the side of the spine and by the curves of the lower ribs.
The spleen is well back and held in place by peritoneal folds, and the pancreas depends chiefly on the surrounding organs for support.
The kidneys normally rest in definite depressions that begin around the level of L4 and are supported by the psoas muscle, quadratus lumborum, and retroperitoneal fat. The attachments of the hepatic and splenic flexures of the colon are external to the kidney and attached to the posterior surface of the abdominal cavity.
About seven-eights of the weight of the abdominal organs is borne by the psoas shelf and the muscles of the abdominal wall. Postural visceroptosis results in dysfunction of the displaced organs. Goldthwait observed that a faulty posture causes the liver to rotate anteriorly and to the right. Traction is thereby exerted on the common bile duct and sometimes seriously interferes with its drainage.
Abdominal dilatation and motility disturbances are also frequent occurrences. This is most likely the outcome of stretching of the sympathetic nerves. Stretched nerves within voluntary muscles usually produce a temporary paralysis.
In addition, when the abdominal cavity becomes shortened longitudinally, the viscera become crowded but so do the glands of internal secretion and the nerve ganglia as well. Thus, orthostatic albuminuria, dysmenorrhea, and constipation may be seen. Visceroptosis also causes an abnormally low pressure in the upper abdomen. If this pressure is sufficiently below atmospheric pressure, air is drawn into the stomach during respiration (aerophagia).
Because of visceroptosis, a compensating lumbar lordosis, and the insult at the IVFs, symptoms can be diffuse and subtle. It has been previously described that duodenal stasis may be attributed to increased tension on the superior mesenteric vessels. One study showed that postural correction relieved 65% of cases exhibiting a picture of duodenal obstruction and 75% of cases presenting with gastric distress, nausea, and abdominal pain associated with visceroptosis.
Postural Effects of Pregnancy
Several years ago, studies by Goldthwait demonstrated the ill effects on spinal posture during pregnancy and visceroptosis. These effects were attributed to the increased tension on nerves and vessels. Browde showed that prolonged experimental increase of intra-abdominal pressure results in neurodegeneration of the end plates and terminal nerve fibers.
A similar picture is seen during pregnancy wherein it has been shown histologically that degeneration of nerve fibers precedes changes in the musculature of the diaphragm and abdominal wall. These degenerative changes in the fibers appeared to be the result of increased intra-abdominal pressure, yet they differed from that of typical Wallerian degeneration.
| Adhesive capsulitis | IVD degeneration |
| Ankylosis | IVD nuclear displacement |
| Apophyseal asymmetry | Ligamentous shortening |
| Articular adhesions | Meniscoid fragments |
| Biomechanical dysequilibrium (eg, short leg, hemivertebra) | Phasic muscular spasm (splinting) |
| Bony encroachment (eg, jammed facet) | Pseudoankylosis |
| Capsular thickening | Somatospinal reflexes |
| Hypertonic postural reflexes | Synovial tabs |
| IVD anular protrusions | Viscerospinal reflexes |
In compensation to a local area of fixation, adjacent joints are forced to assume roles of increased mobility (hyperkinesia), leading to clinical instability. Also, when a unilateral articulation is partially fixated, its contralateral partner is forced to assume the role of both via pivotal hypermobility about an abnormal axis. Invariably, it will be at the site of excessive mobility that is symptomatic rather than the site of the cause of the abnormal movement. Gillet believes that one exception to this is the suboccipital area, which he feels is often involved in a state of muscular fixation.
Total fixation is most frequently found at the occipitoatlantal, lower thoracic, and sacroiliac articulations. In most instances, however, mobility is not restricted in all directions. The earlier a fixation is corrected, the less chance there is for chronic degenerative changes to occur and the greatest change in mobility can be noted after adjustment.
Clinical Studies
Many clinical studies have been conducted to validate partial or complete segmental fixation. Gillet and Liekens, in Europe, have done much to develop a system of dynamic motion palpation. Many of their findings have been collaborated by Faye, Wiles, and several others in North America.
Stress-view roentgenography has also been used extensively to evaluate the existence of segmental fixation in the spine. The first system found in our literature search was developed by Vladef in Detroit during the 1940s and expanded upon by Rich at Lincoln Chiropractic College in the 1950s through cineroentgenology. In more recent years, studies by Illi, Carrick, Giles, Good, Banks, Grice, and Henderson have been highly helpful. Likewise, the works of Vernon, Burnarski, Cox, and Mannen have shed much light on this subject (see chapter bibliography).
Electromyographic studies have also been used to note the somatic changes that occur following adjustive correction of fixations. In this context, the studies of Rebechini-Zasadny, Lewit, and Thabe have greatly added to our knowledge of this concept and its implications.
Implications
When involving one or more vertebrae, a state of decreased mobility of the motion unit encourages neural alterations that can lead to pathologic processes in the areas supplied by the affected nerve root complex, depending upon the degree of fixation and the chronicity of involvement.
An Etiologic Hypothesis. Giles hypothesizes that the main stages evolve as follows:
Decreased mobility or vertebral fixation of a motion unit within its normal physiologic range of movement causes sluggish circulatory flow. Keep in mind that the motion unit is normally dynamic and that the following structures may be found in the IVF: the anterior or motor nerve root, posterior or sensory root, part of the posterior nerve root ganglion, recurrent meningeal nerve, spinal ramus artery, intervertebral vein, lymphatic vessels, nervi nervorum, nervi vasorum, vaso vasorum, and vaso nervorum.
Sluggish circulatory flow in the vertebral veins and arteries causes venous stagnation. Venous stagnation from arterial backup in turn produces a local toxicity. Toxicity, due to the buildup of metabolic waste products in the area of the IVF, alters the normal pH of the local fluids that causes a breakdown of the Krebs cycle.
A breakdown of the Krebs cycle, due to decreased oxygen and toxicity, causes a partial breakdown of the sodium pump mechanism, resulting in an ionic imbalance. Ionic imbalance, as the sodium pump can no longer maintain normal ionic equilibrium, results in some degree of erratic nerve conduction and edema in the tissues of the immediate area. The erratic nerve conduction may be exhibited in all nerves passing through the involved IVF and immediate area. CSF stagnation possibly occurs in association because of the intimate relationship between spinal fluid and venoid blood, contributing to toxicity in the nerve root area.
It should be noted that the hypotheses of several others differ from that of Giles in varying degrees.
Therapeutic Considerations. Segmental hypermobility appears to be the frequent effect of adjacent articular fixation as the result of soft-tissue (muscular and/or ligamentous) contractures. Buerger has shown that there appears to be a lack of stimulation of joint mechanoreceptors that normally inhibit nociceptive afferents. Lack of articular mobility prevents the normal input into the neuronal pool that blocks pain-conducting afferents from conducting impulses to higher CNS levels.
Although nociceptive impulses cannot be measured directly, an accompanying reflex (spontaneous activity of segmental muscles) can be measured by EMG recordings. It has been demonstrated by Thabe that local joint restriction induces abnormal EMG changes and that adjustive therapy normalizes this response concurrently with the correction of joint malfunction.
For many years, it has been realized that the basis of chiropractic therapy cannot rest on empirical results alone. Controlled research studies have been encouraged through such organizations as the Foundation for Chiropractic Education and Research and various chiropractic colleges. The osteopathic profession and more recently the allopathic profession, as well as the scientific community in general, have also increased their investigation of why corrective manipulative therapy, especially that of the spine, exerts its influence on somatic and visceral functions.
Adjustive mobilization of spinal fixations has been demonstrated by an EMG study by Rebechini-Zasadny/Tasharski to show a positive gain in muscle strength, and Vernon has shown a significant but short-term increase in serum beta-endorphins (resembling that following acupuncture) immediately after adjustive therapy. Besides the control of pain, endorphins have far-reaching effects in multiple body systems that are currently undergoing extensive study.
In support of the supposition that fixation is primarily articular in nature, Thabe reports that adjustive techniques could accomplish this correction where local anesthetic injections and mobilization could not. In addition, Mayer and associates found that oral anti-inflammatories do not improve symptoms associated with segmental cervical hypomobility.
STRUCTURAL ADJUSTMENT RATIONALES
Bergmann states that the most specialized and significant therapy employed by the chiropractor involves the adjustment of the articulations of the human body, especially of the spinal column, manually or mechanically, actively or passively, for restoring normal articular relationship and function, restoring neurologic integrity, and influencing physiologic processes.
Terminology
The objective of any therapy must be based upon a rational hypothesis. According to its founder, the objective of chiropractic therapy is to restore normal "tone" to the nervous system. This goal has never varied, while the primary and secondary methods (technics and techniques) used to achieve this goal have undergone and will continue to undergo constant refinement. This is true for the procedures used within all health-care professions.
Although it is recognized that many chiropractic practitioners achieve this by "nonthrust" means (eg, the application of somatosomatic reflexes), objectives are generally achieved by manual articular mobilization unless such a technic is contraindicated in a specific situation.
The terms technique and technic are generally considered synonymous outside the profession of chiropractic. In chiropractic, however, the term technic has been historically restricted to the application of a manually applied adjustive force, while the term technique is used concerning the application of any other procedure (therapeutic or diagnostic).
Chiropractic treatment should be differentiated from chiropractic technic. Case-management treatment includes the application of a primary technique plus all the ancillary procedures incorporated to achieve the clinical objective (eg, physiotherapeutic modalities, nutritional supplementation, diet control, therapeutic exercise, meridian therapy, biofeedback, and psychotherapy or other counseling) in the most efficient manner.
The Uniqueness of the Chiropractic Adjustment
Although the chiropractic "adjustment" is at the foundation of chiropractic therapeutics, few have tried to define it. Sandoz states that it is a passive manual maneuver during which the three-joint complex (IVD and apophyseal joints) is suddenly carried beyond the normal physiologic range of movement without exceeding the boundaries of anatomical integrity.
Swezey, an allopath, refers to a dynamic chiropractic adjustment as the high-velocity short-arc-inducing passive movement of one articulating surface over another. Few would strongly object to either of these attempts to define the purely structural effect induced; ie, if the objective is solely to mobilize a fixation or realign a subluxation. Unfortunately, such purely mechanical concepts are limited; eg, they fail to consider the induced neurologic stimulation upon the cord, root, axoplasmic flow, and mechanoreceptors of the area and the local and remote "spillover" effects of such stimuli.
There is a recent trend by some authors and editors to lump what a chiropractor does during an "adjustment" under the general category of spinal manipulative therapy (SMT). This appears to be a term originated by the allied health professions for it was rarely seen in chiropractic literature prior to the late 1970s.
This author is often uncomfortable with such a generalization because what a chiropractor attempts to do is far removed from the general "mobilization" and gross "manipulation" procedures commonly conducted by physiotherapists and many osteopaths, which typically are passive attempts to increase a restricted range of movement of a joint by stretching contractures. While the term SMT may be appropriate for a large variety of low-velocity extraspinal adjustive techniques or the application of a stretching maneuver to improve a joint's range of motion, it can be argued that its use is a clear misnomer in most instances when applied to the application of scientific chiropractic during spinal therapy.
More than 20 years ago, Levine had the foresight to warn those who defined the chiropractic adjustment solely in structural terms without considering the neurologic overtones involved:
"In discussing chiropractic techniques, it is only proper to note that chiropractic holds no monopoly on manipulation. Manipulation for the purpose of setting and replacing displaced bones and joints, including spinal articulations, is one of the oldest therapeutic methods known. It has been and still is an integral part of the armamentarium of healers of all times and cultures.
”What differentiates chiropractic adjusting from orthopedic manipulations, osteopathic maneuvers, massage, zone therapy, etc? In one sentence, it is the dynamic thrust! The use of the dynamic thrust is singularly chiropractic. And it is the identifying feature of chiropractic techniques.
"However, chiropractic's rationale is hardly based on the fact that its adjustive techniques are applied with a sudden impulse of force. It is the reasons why these techniques are applied, and why they are applied in a certain manner, that distinguish chiropractic from other healing disciplines, manipulative or not. In fact, some chiropractic techniques of recent vintage are not characterized by sudden application. We are thinking of those techniques which have been named 'non-force,' though strictly speaking, the term is a misnomer. What makes them also part of chiropractic is that they are designed to serve the same purpose as the dynamic thrust, though whether they are equally efficient is a moot question."
Motion Barriers During Structural Therapy
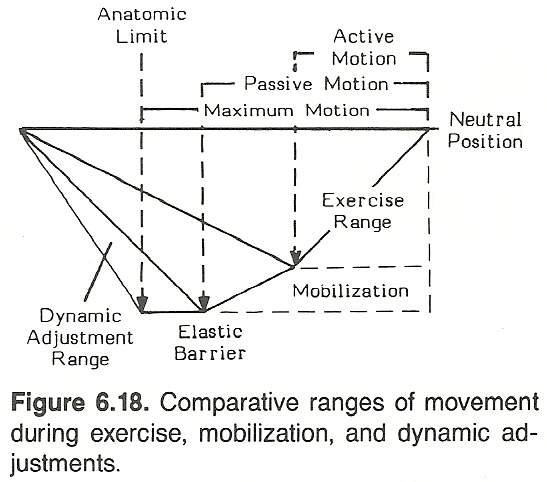 |
Both articular adjustments and manipulation impose static and dynamic forces across joint surfaces. Within its anatomical range of motion, a normal vertebra exhibits:
(1) a voluntary active range,
(2) an involuntary passive range, and a
(3) slight quasi-physiologic motion at the end of the passive range that is determined by ligamentous plasticity and elasticity. To recognize clinical implications, an understanding of the barrier concept is necessary.
When a joint is passively tested for range of motion, the examiner will note increasing resistance to motion referred to as a "bind" or the physiologic motion barrier. When the joint is carried past this point, the added motion becomes painful to the patient. This point is called the anatomical motion barrier (AMB). In evaluating the degrees of passive motion, joints should be moved near but not fully to the AMB.
Thus, joint motion evaluation is accomplished by passively carrying the joint(s) through a range of motion until the AMB is encountered, and then recording the degrees of movement allowed. Active motion usually exists from the neutral position to the point of tissue resistance, while passive motion extends past this to near the elastic barrier.
Grice points out that the usual objective of mobilization techniques is to restore the normal range of passive joint motion from the neutral position to the normal elastic barrier. Thus, it is longer in range than that of active motion and to the maximum point of passive motion. The objective of mobilization (stretching) techniques is to restore motion from the neutral position to the elastic barrier.
Most osteopathic "leverage" techniques are conducted within this range, as are many chiropractic extremity techniques. In contrast, dynamic specific chiropractic spinal adjustments are usually carried a step further into the quasi-physiologic range, often to the anatomical limit, but the duration of the application of force is only a fraction of a second.
Specific Chiropractic Adjustments
It can be generally stated that joints and nerves become painful only when nociceptors are stretched, compressed, or chemically irritated. Analysis consists to a great extent in determining which of these conditions exist to produce the nociceptive input experienced by the patient in pain.
The biomechanical objective in specific chiropractic adjustments is to restore motion throughout the active, passive, and paraphysiologic range of motion. Because of the dynamic forces involved, such techniques should carefully consider the exact geometric plane of articulation (normal or abnormal), asymmetry, the force magnitude to be applied, the direction of force, torque, coupling mechanisms, the state of the holding elements (eg, spastic muscles, articular fixations, stiffness and damping factors), the integrity of the check ligaments (eg, stretched, shortened), and any underlying pathologic processes (eg, infectious, neoplastic, sclerotic, arthrotic, osteoporotic) of the structures directly or indirectly involved.
As local temperature, trabeculae arrangement, density, elasticity, plasticity, flexibility, nutrition, etc, are variables that affect the material properties of tissues, these factors also must be considered. The application of any clinical procedure without consideration of the cause-and-effect forces anticipated is not scientific chiropractic.
The Articular Snap
Skilled spinal adjustments often involve the breaking of the synovial seal of the apophyseal joints, which results in an audible "snap." While some feel that this is insignificant, most authorities believe that breaking the joint seal permits an increase in mobility (particularly that not under voluntary control) from 15 to 20 minutes --allowing the segment to normalize its position. Unsuccessful manipulations resulting in increased pain rarely produce an audible joint release, while successful adjustments usually result in an immediate sense of relief even if some pain and spasm remain, a reduction in palpable hypertonicity, and an improvement in joint motion, and are followed by a gradual reduction in symptoms.
Thrust Technics
Thrust technics applied at an articulation can be divided into two general categories: low-velocity and high-velocity adjustments, and each has various subdivisions depending on the joint being treated, its structural-functional state, and the primary and secondary objectives to be obtained. The term adjustment velocity refers to the speed at which the adjustment is delivered.
In either low-velocity or high-velocity technics:
The force applied may be low, medium, or high.
The duration of the force may be short or sustained.
The amplitude (distance of articular motion) may be short, medium, or long.
The direction of the force may be straight or curving and/or perpendicular, parallel, or oblique to the articular plane.
Overlying soft-tissue tension may be mild, medium, or strong.
Primary or secondary leverage may be applied early, synchronized, or late.
Contralateral stabilization may or may not be necessary.
Thrust onset may be slow, medium, or abrupt.
Fixation (mobility limitations) may be produced by such non-IVF conditions as paravertebral fascial adhesions, ligamentous contractures, IVD dehydration, fibrosed muscle tissue, spondylosis, meningeal sclerosis, or adhesions. A dynamic thrust to these conditions may result in increased mobility by stretching shortened tissues and breaking adhesions, but there is always danger of osseous avulsion or tearing of meninges as scar tissue has a much higher tensile strength than osseous or nerve tissue. In addition, as such states usually involve multiple segments, broadly applied LVTs would be more appropriate.
Low-Velocity Technics (LVTs)
Within the category of low-velocity adjustments fall the many applications that apply slow stretching, pulling, compression, or pushing forces. Sustained or rhythmic manual traction or compression and procedures to obtain proprioceptive neuromuscular facilitation are typical examples. A more specific example would be the application of Spear's double-transverse contact, which is applied to the spine in a deep, low-velocity, alternating, rhythmic fashion to obtain patient relaxation and to stretch paraspinal and intersegmental adhesions and tightened tissues prior to more specific spinal therapy. Many leverage techniques advocated by Cox, Markey-Steffensmeier, and others to reduce IVD protrusions and functional spondylolisthesis can be placed in this category.
High-Velocity Technics (HVTs)
Within the category of high-velocity adjustments fall the many applications of classic dynamic-thrust (direct, rotary, or leverage) chiropractic adjustment technics that are applied to a vertebra's transverse or spinous process or a lamina, with various degrees of counterleverage and/or contralateral stabilization. Contact pressure is usually firm, if the underlying tissues are not acutely painful, when the contact is to be maintained at a specific point and the thrust delivered in a precise direction.
The objective of almost all HVTs is to reposition a subluxated joint and/or release a fixated articulation (increase joint mobility). How this is achieved has not been specifically determined because more is involved than the application of a mechanical force against a resistance. The most common theories are briefly described below:
The mobilization of subluxated articular surfaces. The apophyseal joints can become fixated because of the effects of joint locking (eg, traumatic), muscle spasm, degeneration, an entrapped meniscoid or other loose body, capsular fibrosis, intra-articular "gluing" or adhesions (eg, postsynovitis, chronic rheumatoid conditions), bony ankylosis, facet tropism, etc.
The relaxation of the paravertebral musculature. While a high-velocity force that suddenly stretches muscles spindles in primary muscle spasm increases the spasm, the same force applied to a segment at which its related muscles are in secondary or protective spasm tends to produce relaxation if the thrust succeeds in removing the focal stimulus for the reflex.
The shock-like effect on the CNS. Shock-like forces
(1) are known to frequently have a normalizing effect on self-sustaining CNS reflexes;
(2) are stimulative to the neurons involved, resulting in increased short-term neural and related endocrine activity; and
(3) set up postural and muscle-tone-normalizing cerebellar influences.
Indirect (Functional) Approaches
Manual mobilization and thrust techniques are direct approaches to relieving articular fixations. Indirect functional approaches are often used when the cause for fixation has been determined to be primarily muscular in origin or when any form of manipulation would be contraindicated. Within this category fall many manual light-touch cutaneous reflex techniques, trigger-point therapy, galvanism, transverse massage, therapeutic vibration, isometric and isotonic contraction, etc. It is theorized that these procedures produce their effects because of their influence on the gamma-loop system and/or by the superiority of mechanoreceptor input on nociceptive input.
BIBLIOGRAPHY
American Chiropractic Association:
Chiropractic State of the Art.
Arlington, VA, American Chiropractic Association, 1984, pp 4, 8.
Anderson RT, Winkler M:
The gravity stress analyzer for measuring spinal posture.
Journal of the Canadian Chiropractic Association, 27(2):55-58, 1983.
Arkuszewski Z:
The efficacy of manual treatment in low back pain: A clinical trial.
Manual Medicine, 2:68-71, 1986.
Balduc HA:
Overview of contemporary chiropractic science for the Chiropractic Association of Oklahoma.
Northwestern College of Chiropractic, convention notes, April 24, 1983.
Baltzell LG, Mackey RH (eds):
Firth's Technic Notes.
Publishing data not shown, 1967, pp 2-6, 12-23.
Distributed by National College of Chiropractic.
Banks SD:
Lumbar facet syndrome: Spinographic assessment of treatment by spinal manipulation.
Journal of Manipulative and Physiological Therapeutics, 6:175-180, 1983.
Benner B, Ehni G:
Degenerative lumbar scoliosis.
Spine, 4:548-552, 1979.
Berger PA, et al:
Behavioral acology of the endorphins.
Annual Review of Medicine, 33:397-415, 1982.
Bergmann T:
Integrated chiropractic methods. Compilation of notes presented to the convention of the Oklahoma Chiropractic Association; April 23, 1983; in cooperation with Northwestern College of Chiropractic.
Berthold CH:
Morphology of normal peripheral axons.
In Waxman SG (ed): Physiology and Pathobiology of Axons.
New York, Raven Press, 1978.
Bishop B: Pain:
Its physiology and rationale for management. Part I, neuroanatomical substrate of pain.
Physical Therapy, 60:13-23, 1980; Part II, analgesia systems of the CNS, 60:21-23, 1980.
Black RG:
The chronic pain syndrome.
Surgical Clinics of North America, 55:999-1011, 1975.
Bonica JJ:
Neurophysiologic and pathologic aspects of acute and chronic pain.
Archives of Surgery, 112:750-761, 1977.
Boyd WA:
A Textbook of Pathology.
Philadelphia, Lea & Febiger, 1961.
Bradley KC:
The posterior ramsegmental nerves.
In Glasgow EF, Twomey LT, Scull ER, Kleynhans AM, Idczak RM: Aspects of Manipulative Therapy, ed 2.
New York, Churchill Livingstone, 1985, pp 59-63.
Brena SF, Chapman SL:
Chronic pain: Physiology, diagnosis, management.
In Leek JC, Gershwin ME, Fowler WM Jr: Principles of Physical Medicine and Rehabilitation in the Musculoskeletal Diseases.
Orlando, FL, Grune & Stratton, 1986, pp 189-216.
Brodin H:
Cervical pain and mobilization.
Manual Medicine, 2:18-22, 1985.
Browde AL:
The effect of prolonged pressure on peripheral abdominal nerves.
American Review of Soviet Medicine, 2:213-217, 1944.
Buerger AA:
Experimental neuromuscular models of spinal manual techniques.
Manual Medicine, 1:10-17, 1983.
Burnarski DJ:
Chiropractic biomechanical evaluations: Validity in myofascial low back pain.
Journal of Manipulative and Physiological Therapeutics, 5:155-161, 1982.
Burns L, Chandler LC, Rice RW:
Pathogenesis of Visceral Disease Following Vertebral Lesions.
Chicago, American Osteopathic Association, 1948, pp 3-20.
Burt HA:
Effects of faulty posture.
Proceedings of the Royal Society of Medicine, 43:187, 1950.
Cailliet R:
Disuse syndrome: fibrositic and degenerative changes.
In Brena SF, Chapman SL (eds): Management of Patients with Chronic Pain.
New York, Spectrum Publications, 1983, pp 63-71.
Canadian Memorial Chiropractic College: Segmental Neuropathy.
Toronto, Canadian Memorial Chiropractic College, date of publication not shown. Monograph, pp 6-7, 29-32.
Carrick FR:
Cervical radiculopathy: The diagnosis and treatment of pathomechanics in the cervical spine.
Journal of Manipulative and Physiological Therapeutics, 6:129-137, 1983.
Carrick FR: Treatment of pathomechanics of the lumbar spine by manipulation. Journal of Manipulative and Physiological Therapeutics, 4:173-178, 1981.
Cassidy JD, Kirkaldy-Willis WH, McGregor M:
Spinal manipulation for the treatment of chronic low back and leg pain: an observational study.
In Buerger AA, Greenman PE (eds): Empirical Approaches to the Validation of Spinal Manipulation.
Springfield, MO, Charles C. Thomas, 1985.
Cervero F:
Deep and visceral pain.
In Kosterlitz HW, Terenius LY (eds): Pain and Society.
Weinheim, Verlag Chemic, 1980, pp 263-282.
Coggins WN:
Basic Technique: A System of Body Mechanics.
Creve Coeur, MO, published by author, 1983.
Coote JH, et al:
Reflex discharges into thoracic white rami elicited by somatic and visceral afferent excitation.
Journal of Physiology, 202:141-159, 1969.
Council on Chiropractic Education:
Position/policy paper, adopted January 21, 1978.
Cox JM:
Low Back Pain: Mechanism, Diagnosis and Treatment.
Baltimore, Williams and Wilkins, 1985.
Crue BB, et al:
Neurophysiology of pain peripheral aspects.
Bulletin of the Los Angeles Neurological Society, 41(1):13-42, 1976.
Curtis DR, Eccles JC:
Synaptic action during and after repetitive stimulation.
Journal of Physiology (British), 150:374, 1960.
Cyriax E:
Some common postural deformities and their treatment by exercise and manipulation.
British Journal of Physical Medicine, June 1938.
Cyriax J, Schiotz EH:
Manipulation: Past and Present.
London, Wm. Heineman, 1975.
Cyriax J:
Textbook of Orthopaedic Medicine: Vol One, Diagnosis of Soft Tissue Lesions, ed 8.
London, Bailliere Tindall, 1982, pp 22-42, 65-66.
DeBoer KF, Harmon R, Tuttle CD, Wallace H:
Reliability study of detection of somatic dysfunctions in the cervical spine.
Journal of Manipulative and Physiological Therapeutics, 8:9-15, 1985.
Dee R:
Articular neurology. I
n Sokoloff L (ed): The Joints and Synovial Fluid.
New York, Academic Press, 1978, p 177.
Denslow JS:
An analysis of the variability of spinal reflex thresholds.
Journal of Neurophysiology, 7:207-215, 1944.
Denslow JS, Hassett CC:
The central excitatory state associated with postural abnormalities.
Journal of Neurophysiology, 5:393-402, 1942.
de Reuck AVS, Knight J (eds):
Myotactic, Kinesthetic, and Vestibular Mechanisms.
Ciba Foundation Symposium. Boston, Little, Brown, 1967.
De Rusha JL:
Upper cervical technic correlated with neurodiagnosis.
ACA Journal of Chiropractic, September 1961.
Dowling JJ:
Musculoskeletal Disease: Staged for Rapid Comprehension.
Chicago, Year Book Medical, pp 78-79.
Downing C:
Osteopathic Principles in Disease.
San Francisco, R.J. Orozco, 1923.
Elton D, Burrows GD, Stanley GV:
Clinical measurement of pain.
Medical Journal of Australia, 1:109-111, 1979.
Epstein JA, Epstein BS, Jones MD.
Symptomatic lumbar scoliosis with degenerative changes in the elderly.
Spine, 4:542-547, 1979.
Farfan HF, et al:
The effects of torsion on the lumbar intervertebral joints: The role of torsion in the production of disc degeneration.
Journal of Bone and Joint Surgery, 52A:468, 1970.
Farfan HF:
Mechanical Disorders of the Low Back.
Philadelphia, Lea & Febiger, 1973.
Farfan HF:
The scientific basis of manipulative procedures.
In Graham R (ed): Rheumatic Diseases: Low Back Clinics.
London, W.B. Saunders, April 1980.
Farfan HF:
Symptomatology in terms of the pathomechanics of low-back pain and sciatica.
In Haldeman S (ed): Modern Developments in the Principles and Practice of Chiropractic.
New York, Appleton-Century-Crofts, 1980.
Farfan HF, Sullivan JD:
The relation of facet orientation to intervertebral disc failure.
Canadian Journal of Surgery, 10:179, 1967.
Foundation for Chiropractic Education and Research:
Spinal manipulation current findings on its therapeutic effects and role in treatment.
Spinal Manipulation, 2(3):1-3, October 1986. Anonymous.
Freedman BG:
The biodynamical aspect of cerebrospinal fluid in disease and health.
Journal of Manipulative and Physiological Therapeutics, 2:79-84, 1979.
Frogley R:
Neurological observations of a subluxation.
The Journal of Clinical Chiropractic, 1(3), 1973.
Gainsbury JM:
High-velocity thrust and pathophysiology of segmental dysfunction.
In Glasgow EF, Twomey LT, Scull ER, Kleynhans AM, Idczak RM: Aspects of Manipulative Therapy, ed 2.
New York, Churchill Livingstone, 1985, pp 87-92.
Giles LG:
Spinal fixation and viscera.
Journal of Clinical Chiropractic, 1(3):144-145, 1973.
Gillet H:
The anatomy and physiology of spinal fixation.
Journal of the National Chiropractic Association, December 1963.
Gillet H:
A definition of the subluxation.
The Texas Chiropractor, February 1974.
Gillet H, Liekens M:
Belgian Chiropractic Research Notes.
Huntington Beach, CA, Motion Palpation Institute, 1981.
Gillet H, Liekens M:
A further study of spinal fixations. A
nnals of the Swiss Chiropractic Association, Geneva, IV:41, 1967.
Goldthwait JE, et al:
The Essentials of Body Mechanics in Health and Disease, ed 5.
Philadelphia, J.B. Lippincott, 1952.
Good AB:
Spinal joint blocking.
Journal of Manipulative and Physiological Therapeutics, 6(1):1-7, March 1985.
Goodman CE:
Pathophysiology of pain.
Archives of Internal Medicine, 143:527, 1983.
Greenman PE:
Manipulative therapy in relation to total health care.
In Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy.
New York, Plenum Press, 1978.
Grice AS:
A biomechanical approach to cervical and dorsal adjusting.
In Haldeman S (ed): Modern Developments in the Principles and Practice of Chiropractic.
New York, Appleton-Century-Crofts, 1980, pp 338-339.
Grice AS, Fligg, DB:
Class notes. Department of Biomechanics/Kinesiology, BK101 (Joint Movement and Muscle Testing).
Toronto, Canadian Memorial Chiropractic College, date not shown.
Grice AS, Fligg, DB:
Class notes. Department of Biomechanics/Kinesiology, BK202 (Spinal Dynamics).
Toronto, Canadian Memorial Chiropractic College, date not shown.
Grice AS:
Muscle tonus changes following manipulation.
Journal of the Canadian Chiropractic Association, 19:29-31, 1974.
Grice AS:
Radiographic, biomechanical and clinical factors in lumbar lateral flexion: Part I.
Journal of Manipulative and Physiological Therapeutics, 2:26-34, 1979.
Grieve GP:
Common Vertebral Joint Problems.
London, Churchill Livingstone, 1981, pp 69-73, 161-196.
Grundfest H:
Discussion of excitation and conduction in traumatized nerves.
In Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy.
New York, Plenum Press, 1978.
Gucker T:
Changes in vital capacity in scoliosis: Preliminary report on the effects of treatment.
Journal of Bone and Joint Surgery, 44:469, 1962.
Guillemin R, et al:
The endorphins, novel peptides of brain and hypophyseal origin, with opiate like activity: biochemical and biologic studies.
Annals of the New York Academy of Science, 197:131-157, 1979.
Hadden GR:
The development of a static posture analysis instrument with direct application as an objective pre x-ray screening procedure.
Journal of the Canadian Chiropractic Association, 27(4):139-149, 1983.
Haldeman S:
Referred pain: Extra spinal symptoms of spinal origin.
The Texas Chiropractor, July 1974.
Hartman L:
Classification and application of osteopathic manipulative techniques.
In Glasgow EF, Twomey LT, Scull ER, Kleynhans AM, Idczak RM: Aspects of Manipulative Therapy, ed 2.
New York, Churchill Livingstone, 1985, pp 82-86.
Henderson DJ, Dorman TM:
Functional roentgenometric evaluation of the cervical spine in the sagittal plane.
Journal of Manipulative and Physiological Therapeutics, 8:219-226, 1985.
Henderson DJ:
Significance of vertebral dyskinesia in relation to the cervical syndrome.
Journal of Manipulative and Physiological Therapeutics, 2(1):3-13, March 1979.
Hickey RF, Tregonning GD:
Denervation of spinal facet joints for treatment of chronic low back pain.
New Zealand Journal of Medicine, 86:96-99, 1977.
Hildebrandt RW, Howe JW:
Spinal biomechanics and subluxation classification.
Lombard, IL, National College of Chiropractic, 1974.
Hoag JM, Cole MV, Bradford SG (eds):
Osteopathic Medicine.
New York, McGraw-Hill, 1969.
Homewood AE:
A posturometer survey.
Journal of the Canadian Chiropractic Association, 9(1):9-10, 1965.
Homewood AE:
The Neurodynamics of the Vertebral Subluxation, ed 3.
Place of publication not shown, published by author, 1981, pp 47-66, 69-87, 103-111, 162-167, 265-266.
Illi FW:
The Vertebral Column: Life-Line of the Body.
Chicago, National College of Chiropractic, 1951.
Inman VT, Saunders JB:
Referred pain from skeletal structures.
Journal of Nervous and Mental Disease, 99:660-667, 1944.
Janse J:
A concept: The neurological element as it relates to clinical chiropractic.
The Chirogram, December 1975.
Janse J:
The integrative purpose and function of the nervous system: A review of classical literature.
Journal of Manipulative and Physiological Therapeutics, 1(3), September 1978.
Janse J:
Principles and Practice of Chiropractic.
Lombard, IL, National College of Chiropractic, 1976, pp 43-44, 48-50, 161, 205-221, 243-250.
Jaskoviak PA, Schafer RC:
Chapter 2: Pain suppression in the twentieth century.
In Jaskoviak PA, Schafer RC: Applied Physiotherapy: Practical Applications Within Clinical Chiropractic.
Arlington, VA, American Chiropractic Association, 1986.
Johnson AC:
Postural Correction.
Los Angeles, Chiropractic Educational Extension Bureau, date not listed.
Johnson J:
Manipulative body mechanics therapy.
Journal of the American Osteopathic Association, Vol 60, June 1961.
Judovitch B, Bates W:
Segmental Neuralgia in Painful Syndromes.
Philadelphia, F.A. Davis, 1946.
Kellgren JH:
Observations on referred pain arising from muscle.
Clinical Science, 3:175, 1938.
Kellgren JH, Samuel EP:
The sensitivity and innervation of the articular capsule.
Journal of Bone & Joint Surgery, 32(B):84-92, 1950.
Kendall HO, et al:
Posture and Pain.
Baltimore, Williams & Wilkins, 1952.
Kessler RM, Hertling D (eds):
Management of Common Musculoskeletal Disorders.
Philadelphia, Harper & Row, 1983, pp 27-30, 91-98.
Kfoury PW (ed):
Catalog of Chiropractic Techniques.
Chesterfield, MO, Logan College of Chiropractic, 1977.
Kirkaldy-Willis WH:
Manipulation.
In Kirkaldy-Willis WH (ed): Managing Low Back Pain.
New York, Churchill Livingstone, 1983, pp 175-177.
Kirkaldy-Willis WH:
The three phases of the spectrum of degenerative disease.
In Kirkaldy-Willis WH (ed): Managing Low Back Pain.
New York, Churchill Livingstone, 1983, pp 24-25, 73-89.
Klausen K:
The shape of the spine in young males with and without back complaints.
Clinical Biomechanics, 1:81-84, 1986.
Korr IM (ed):
The Neurobiologic Mechanisms in Manipulative Therapy.
New York, Plenum Press, 1978, pp 45-47, 137-177.
Korr IM: Proprioceptors and the behavior of lesioned segments. In Stark EH (ed): Osteopathic Medicine, Acton, MA, Publication Services Group, 1975, pp 183-199.
Korr IM:
The spinal cord as organizer of disease processes: Some preliminary perspectives.
Journal of the American Osteopathic Association, September 1976.
Kostuik JP, Bentivoglio J:
The incidence of low-back pain in adult scoliosis.
Spine, 6:268-273, 1981.
Kunert W:
Functional disorders of internal organs due to vertebral lesions.
Ciba Symposium, 13(3), 1965.
Lamb DW:
The neurology of spinal pain.
Physical Therapy, 59:971-973, 1979.
Leach RA:
The Chiropractic Theories, ed 2.
Baltimore, Williams & Wilkins, 1986, pp 15-22,28-29, 38-45, 86-105.
Leavitt F, Garron DC, Whisler WW, Sheinkop MB:
Affective and sensory dimensions of back pain.
Pain, 4:273-281, 1978.
Levine M:
The Structural Approach to Chiropractic.
New York, Comet Press, 1964, p 85.
Lewis T:
Suggestions relating to the study of somatic pain.
British Medical Journal, 1:321-327, 1938.
Lewit K:
The contribution of clinical observation to neurobiological mechanisms in manipulative therapy.
In Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy.
New York, Plenum, 1978, pp 43-52.
Loomis RC, Steinbach LJ:
Examination of the Spinal Column for Defects of Balance and Subluxation.
Pittsburgh, Universal Chiropractic College, 1930.
Lynch MK, Kessler RM:
Pain.
In Kessler RM, Hertling D (eds): Management of Common Musculoskeletal Disorders.
Philadelphia, Harper & Row, 1983, pp 51-72.
Macnab I:
Backache.
Baltimore, Williams & Wilkins, 1977.
Mannen EM:
The use of cervical radiographic overlays to assess response to manipulation: A case report.
Journal of the Canadian Chiropractic Association, 24:108-110, 1980.
Markey LP, Steffensmeier LA:
The Markey-Steffensmeier spondylolisthesis maneuver.
The Markey-Lloyd Newsletter, 2(2), February 1987.
Mayer ET, Herrmann G, Pfaffenrath V, Pollmann W, Auberger T:
Functional radiographs of the cervicocranial region and the cervical spine: A new computer-aided technique.
Cephalgia, 5:237-243, 1985.
McAlpine JE:
A discussion of the dentate ligament neural traction mechanism.
International Review of Chiropractic, pp 35-39, October-December 1980.
McDowall DA:
The subluxation specific, the adjustment specific: an early theory of muscle imbalance.
ACA Journal of Chiropractic, 13(1):37-39, 1983.
McKenzie RA:
The Lumbar Spine.
Upper Hutt, New Zealand, Spinal Publications Ltd, 1981, pp 9-14.
Mellin G:
Physical therapy for chronic low back pain: Correlations between spinal mobility and treatment outcome.
Scandinavian Journal of Rehabilitative Medicine, 17:163-166, 1985.
Melzack R, et al:
Neurophysiological foundations of pain.
In Sternbach RA (ed): The Psychology of Pain.
New York, Raven Press, 1978, pp 1-26.
Nachemson A:
Adult scoliosis and back pain.
Spine, 4:513-517, 1979.
Nall SK:
The role of specific manipulation towards alleviating abnormalities in body mechanics and restoration.
Journal of Manipulative and Physiological Therapeutics, 5(1):11-15, 1982.
Neff SD:
The neuroanatomy of vertebral subluxations.
ACA Journal of Chiropractic, 17(4):S55-57, 1980.
Ochs S:
Axoplasmic flow in neurons.
In Gaito J (ed): Macromolecules and Behavior.
New York, Appleton-Century-Crofts, 1966.
Ochs S:
Axoplasmic transport.
In Tower DB (ed): The Basic Neurosciences.
New York, Raven Press, Vol 1, 1975, pp 137-146.
Ochs S:
A brief review of material transport in nerve fibers.
In Goldstein M (ed): The Research Status of Spinal Manipulative Therapy,
NINCDS Monograph No. 15, DHEW Publication No. (NIH) 76-998, Stock No. 017-049-00060-7,
Washington, DC, U.S. Government Printing Office, 1975, pp 189-194.
Okubo J:
The review of posturography in Japan.
Agressologie, 21D:3-24, 1980.
Palmer DD:
The Science, Art, and Philosophy of Chiropractic.
Portland, OR, Portland Printing House, 1910.
Parke WW:
Applied anatomy of the spine.
In Rothman RH, Simeone FA (eds): The Spine.
Philadelphia, W.B. Saunders, 1975, Vol I, pp 33-35.
Perl ER:
Mode of action of nociceptors.
In Hirsch C, et al (eds): Cervical Pain.
Oxford, England, Pergamon, 1972, pp 157-163.
Phillips RB:
The irritable reflex mechanism.
ACA Journal of Chiropractic, January 1974.
Pointon R:
A possible cause of acute osteopathic lesions.
British Osteopathic Journal, 8:10-19, 1976.
Poole PB:
Considerations of neurogenic pain. Ortho-Briefs,
Council on Chiropractic Orthopedics of the American Chiropractic Association, Fall 1982.
Raphael R:
personal correspondence.
Portland, Oregon, 1987.
Rebechini-Zasadny H, Tasharski CC, Heinze WJ:
Electromyographic analysis following chiropractic manipulation of the cervical spine: A model to study manipulation-induced peripheral muscle changes.
Journal of Manipulative and Physiological Therapeutics, 4:61-63, 1984.
Reiter L:
Apophyseal joint functional anatomy and experimental findings: A literature review.
PCC Research Form, 1(2):49-52, Winter 1985.
Roaf R:
The basic anatomy of scoliosis.
Journal of Bone and Joint Surgery, 480: 786, 1966.
Sahlstrand T, Ortengren R, Nachemson A:
Postural equilibrium in adolescent idiopathic scoliosis.
Acta Orthopaedica Scandinavica, 49:354-365, 1978.
Sandoz R:
New trends in the pathogenesis of spinal disorders.
Annals of the Swiss Chiropractic Association, V:93, 1971.
Sandoz R:
Some physical mechanisms and effects of spinal adjustments.
Annals of the Swiss Chiropractors Association, 6:91, 1976.
Sandoz R:
Some reflex phenomena associated with spinal derangements and adjustments.
Annals of the Swiss Chiropractic Association, VII:45, 1981.
Schafer RC:
Symptomatology and Differential Diagnosis. Arlington, VA,
American Chiropractic Association, 1986, pp 226, 290-293, 326-335, 337, 339-340, 841.
Schafer RC:
Clinical Biomechanics: Musculoskeletal Actions and Reactions.
Baltimore, Williams & Wilkins, 1983, pp 121-127, 174-175, 185-187, 194, 199-202, 208-209, 212-215.
Schafer RC (ed):
Basic Chiropractic Procedural Manual, ed 4. Arlington, VA,
American Chiropractic Association, 1984, pp 1-2, 4-9, 15-16.
Schaumberg HH, Spencer PS:
Pathology of spinal root compression.
In Goldstein M (ed): The Research Status of Spinal Manipulative Therapy.
NINCDS Monograph No. 15, DHEW Publication No. (NIH) 76-998, Stock No. 017-049-00060-7.
Washington, DC, U.S. Government Printing Office, 1975.
Sharpless SK:
Susceptibility of spinal roots to compression block.
In Goldstein M (ed): The Research Status of Spinal Manipulative Therapy.
NINCDS Monograph No. 15, DHEW Publication No. (NIH) 76-998, Stock No. 017-049-00060-7.
Washington, DC, U.S. Government Printing Office, 1975.
Simmons EH, Jackson RP:
The management of nerve root entrapment syndromes associated with the collapsing scoliosis of idiopathic lumbar and thoracolumbar curves.
Spine, 4:533-541, 1979.
Sinclair DC, Weddell G, Feindel WH:
Referred pain and associated phenomena.
Brain, 7:184-211, 1948.
Spector B, Eilbert L, Finando S, Fukuda F:
Video integrated measurement system.
Journal of Manipulative and Physiological Therapeutics, 5(2):55-61, 1982.
Speransky AD:
A Basis for the Theory of Medicine; translated by C. P. Dutt.
New York, International Publishers, 1943.
Stephenson RW:
Chiropractic Textbook.
Davenport, IA, published by author, 1927.
Strang VV:
Essential Principles of Chiropractic.
Davenport, IA, Palmer College of Chiropractic, 1984.
Sunderland S:
Anatomical perivertebral influences on the intervertebral foramen.
In Goldstein M (ed): The Research Status of Spinal Manipulative Therapy.
NINCDS Monograph No. 15, DHEW Publication No. (NIH) 76-998, Stock No. 017-049-00060 -7.
Washington, DC, U.S. Government Printing Office, 1975.
Sunderland S:
Traumatized nerves, roots and ganglia: Musculoskeletal factors and neuropathological consequences.
In Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy.
New York, Plenum Press, 1978.
Swezey RL:
The modern thrust of manipulation and traction therapy.
Seminars in Arthritis and Rheumatism, 12(3):326, 1983.
Tehan PJ:
Functional technique: A different perspective in manipulative therapy.
In Glasgow EF, Twomey LT, Scull ER, Kleynhans AM, Idczak RM: Aspects of Manipulative Therapy, ed 2.
New York, Churchill Livingstone, 1985, pp 94-96.
Terrett ACJ, Vernon H:
Manipulation and pain tolerance: A controlled study of the effect of spinal manipulation on paraspinal cutaneous pain tolerance levels.
American Journal of Physical Medicine, 63(5):217-224.
Thabe H:
Electromyography as a tool to document diagnostic findings and therapeutic results associated with somatic dysfunctions in the upper cervical spinal joints and sacroiliac joints.
Manual Medicine, 2:53-58, 1986.
Travell JG, Rinzler SH:
The myofascial genesis of pain.
Postgraduate Medicine, 11:425-434, 1952.
Verner JR:
The Science and Logic of Chiropractic.
Englewood, NJ, published by author, 1941.
Vernon H:
An assessment of the intra- and inter-reliability of the posturometer.
Journal of Manipulative and Physiological Therapeutics, 6(2):57-60, 1983.
Vernon HT, Dhami MSI, Howley TP, Annett R:
Spinal manipulation and beta-endorphin: A controlled study of the effect of a spinal manipulation on plasma beta-endorphin levels in normal males.
Journal of Manipulative and Physiological Therapeutics, 9:115-122, 1986.
Vernon HT, Grice AS:
The four-quadrant weight scale: A technical and procedural review.
Journal of Manipulative and Physiological Therapeutics, 7(3):165-169, 1984.
Vernon HT:
Static and dynamic roentgenography in the diagnosis of degenerative disc disease: A review and comparative assessment.
Journal of Manipulative and Physiological Therapeutics, 5:163-169, 1982.
Vladef T, Hardy M:
The theory of fixation points,
National Chiropractic Journal, June 1945.
Watkins RJ:
Subluxation terminology since 1964.
ACA Journal of Chiropractic, 2(9):S65-70, 1968.
White AA, Hirsch C:
The significance of the vertebral posterior elements in the mechanics of the thoracic spine.
Clinical Orthopaedics, 81:2-41, 1971.
Wiles P:
Postural deformities of the anteroposterior curves of the spine.
The Lancet, April 17, 1937.
Wiles MR:
Reproducibility and interexaminer correlation of motion palpation findings of the sacroiliac joints.
Journal of the Canadian Chiropractic Association, 24:59-68, 1980.
Will TE:
The biochemical basis of manipulative therapeutics: hypothetical considerations.
Journal of Manipulative and Physiological Therapeutics, 1(3):153-156, September 1978.
Will TE:
Hypothetical considerations with regard to the biochemical basis of manipulative therapy.
ACA Journal of Chiropractic, 13:119-123, December 1979.
Wood KW:
Myospasm, myosprain and myalgia.
The Digest of Chiropractic Economics, pp 126-127, May/June 1985.
Wyke BD:
Articular neurology and manipulative therapy.
In Aspects of Manipulative Therapy. Proceedings of Multidisciplinary International Conference on Manipulative Therapy.
Melbourne, Lincoln Institute of Health Sciences, Carlton, Victoria, Australia, August 1979, pp 67-72.
Wyke B:
Neurological mechanisms in the experience of pain.
Acupuncture and Electro-Therapeutical Research International Journal, 4:27-35, 1979.
Yamada K:
The dynamics of experimental posture.
Clinical Orthopaedics, 25:20-31, 1962.
Yamada K, et al: A neurological approach to the etiology and treatment of scoliosis. Journal of Bone and Joint Surgery, 53A:197, 1971.