

The Safety and Effectiveness of Pediatric Chiropractic:
A Survey of Chiropractors and Parents in a
Practice-based Research NetworkThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Explore (NY) 2009 (Sep–Oct); 5 (5): 290–295 ~ FULL TEXT
OPEN ACCESS Alcantara J, Ohm J, Kunz D.
International Chiropractic Pediatric Association,
Media, PA, USA
BACKGROUND: With continued popularity of complementary and alternative medicine (CAM) therapies for children, their safety and effectiveness are of high concern for both CAM and conventional therapy providers. Chiropractic is the most popular form of practitioner-based CAM therapies for children.
OBJECTIVE: The objective of this study was to describe the practice of pediatric chiropractic, including its safety and effectiveness. DESIGN: This study used a cross-sectional survey.
SETTING: A practice-based research network was used for this study.
PATIENTS/PARTICIPANTS: Participants were chiropractors and parents of pediatric patients (aged < or =18 years) attending chiropractic visits ranging from one to 12 visits.
INTERVENTION: This is a survey study. No interventions were rendered in the completion of this study.
MAIN OUTCOME MEASURES: Demographics, clinical presentations, treatment-associated aggravations, complications and improvements.
RESULTS: The indicated primary reason for chiropractic care of children was "wellness care." With respect to condition-based presentations, musculoskeletal conditions were the most common, in addition to nonmusculoskeletal conditions of childhood. The most common techniques used were diversified technique, Gonstead technique, Thompson technique, and activator methods. Treatment-associated complications were not indicated by the chiropractic and parent responders. Chiropractor responders indicated three adverse events per 5,438 office visits from the treatment of 577 children. The parent responders indicated two adverse events from 1,735 office visits involving the care of 239 children.
CONCLUSIONS: Both sets of responders indicated a high rate of improvement with respect to the children's presenting complaints, in addition to salutary effects unrelated to the children's initial clinical presentations.
From the FULL TEXT Article:
Introduction
Contemporaneous with the ever-expanding use of complementary and alternative medicine (CAM) by adults is the burgeoning interest in CAM therapies for children. Eisenberg et al [1] determined that CAM utilization by adults increased from 34% in the early 1990s to 42% in the late 1990s. During this same time period, CAM pediatric utilization increased from 11% to 20%. [2] Of the array of CAM therapies available to children, chiropractic is the most popular practitioner-based CAM therapy [3, 4] and is referred to as pediatric chiropractic. [5] Pediatric visits for CAM treatment are for a wide range of disorders, including pain, respiratory and gastrointestinal tract problems, ear infections, enuresis, and hyperactivity, among others. [4, 6] A study by Lee et al [6] characterizing the chiropractic care of children extrapolated that 30 million pediatric patient visits were made to chiropractors in 1997 at a cost of approximately $1 billion, with parents paying some $510 million out of pocket.
Given its continuing popularity, pediatric chiropractic therefore represents a substantial and significant aspect of CAM therapy for children. In a discussion of the evidence for safety and effectiveness of manual therapy for children, Huijbregts [7] pointed out that there is no clear evidence of harm to date. Considering the diversity of approaches in pediatric spinal manipulative therapy (SMT), research on outcome and harm for one treatment approach cannot and should not be applied to all. The safety of chiropractic care in general and the treatment of children in particular continue to generate controversy and debate. [8, 9] The results of this study, and a careful reading of the literature to date, suggest that in general, SMT for children is extremely safe.
METHODS
This study was approved by the Institutional Review Board of Life University, Atlanta, Georgia. The study was approved for implementation for a period of one year beginning September 2007.
Study Sample
An e-mail invitation was sent out to 2,099 chiropractors to participate in the International Chiropractic Pediatric Association (ICPA) practice-based research network (PBRN) program. The purpose of this study was to evaluate the safety and effectiveness of pediatric chiropractic. Inclusion criteria for participation in the PBRN were(a) the chiropractor must be in good standing with the Board of Chiropractic Examiners in his/her state,
(b) they must agree to the terms of participation as an ICPA PBRN participant (ie, PBRN participation must not be used for practice building or marketing, in addition to maintaining patient confidentiality and informed consent), and
(c) that the subject of interest (ie, pediatric patients aged ≤18 years) must have received SMT care ranging from one to 12 visits.Furthermore, the chiropractor was encouraged to invite the parents of pediatric patients to participate in a similar survey examining the chiropractic care rendered to their child.
Survey Content: Chiropractic Survey
The survey instrument was pilot tested with 15 chiropractors and changes made as appropriate prior to implementing the study. Data extracted from the patient file included geographical data such as gender, age, and the number of visits at the time of file review. Furthermore, this study examined the presenting complaints and the approach to patient care (ie, the chiropractic SMT technique applied and the spinal region or regions SMT was rendered). The chiropractors were also asked to document treatment-associated changes such as aggravations, complications, or improvements. Treatment-associated aggravations were defined as worsening of symptoms or complaints following treatment. Treatment-associated complications were operationally defined as cerebrovascular accidents, dislocation, fracture, pneumothorax, sprains and strains, or death as a result of treatment. Treatment-associated improvements were defined as improvement in symptoms or other reported perceived benefits attributed to treatment. The treatment-related aggravations, complications, and improvements were based on subjective reports by the patient or the patient’s parents/ guardians or from the examination findings on the part of the chiropractor.
Survey Content: Parent Survey
The survey instrument was pilot tested with 15 parents/guardians, with changes made as appropriate prior to implementation. Parent/guardian data include age, gender, and level of education. With respect to their child, information extracted includes gender, age, and the number of visits attended. As in the chiropractor survey, this study examined the types of presenting complaints as well as treatment-associated changes such as aggravations, complications, or improvements.
Statistical Analysis
Data was entered in a Portable Document Format (PDF) through Adobe Reader (Adobe Systems, San Jose, CA). From this PDF, an Extensible Markup Language (XML) file was created containing the data entered in the original form. Using Adobe Acrobat, the XML files were converted to a single comma separated value (.csv) file, which was exported to a spreadsheet (Excel, Microsoft Corporation, Redmond, WA) and analyzed using descriptive statistics.
RESULTS
Chiropractor Survey
The data reported herein was derived from a total of 21 chiropractors contributing 577 pediatric clinical cases. All patients received chiropractic SMT at each visit (N = 5,438 office visits).
The cohort of pediatric patients ranged in age from less than a day to 18 years, with an average age of 7.45 years (median age = seven years; mode age = one year). The gender distribution was 273 females and 304 males. The average number of office visits completed during the time of the survey was 9.4 (median = 12; mode = 12). A majority of the patients reported upon were existing patients returning for care with new complaints (n = 476; 82.4% of cohort), whereas 94 (16.2% of cohort) were new patients.
Of the 577 patients, 46% (n = 267) were reported as presenting for “wellness care.” Twenty-five percent of these (n = 67) also indicated a concurrent specific complaint (eg, colic) that was included in the analysis of the various pediatric clinical presentations.
For the 577 patients, the categories for clinical presentation/care werewellness care (46%);
musculoskeletal complaints (26%);
digestion/elimination problems (7%);
ear, nose, and throat problems (6%);
neurological problems (6%);
immune dysfunction (5%); and
other (4%).With respect to the spinal regions addressed, regardless of clinical presentation, 77 patients received full spine SMT care, whereas 500 patients received regional spinal care. Full spine care denotes that SMT was applied to the cervical, thoracic, and lumbosacral spine at each visit. Regional care denotes the patient receiving SMT at one or two spinal regions (ie, cervical and thoracic spine or thoracic and lumbosacral spine). Additionally, 468 patients received some form of cranial care, regardless of full spine or regional spinal care. When examining the specific spinal regions rendered SMT (regardless of whether a patient received full spine or only regional care), 509 patients received SMT to the cervical spine, 550 patients received SMT to the thoracic spine, and 524 received SMT to the lumbosacral region.
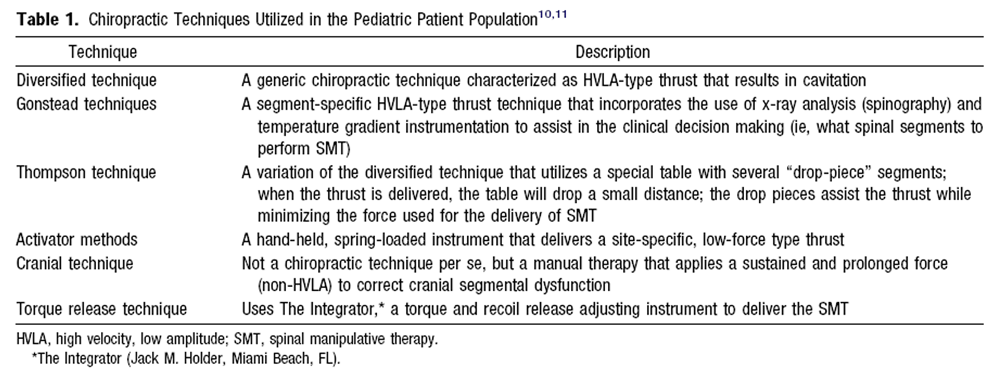
The primary and most common chiropractic SMT technique used by the chiropractors in rendering care werediversified technique (n = 334),
Gonstead technique (n = 58),
Thompson technique (n = 57),
activator methods (n = 43),
cranial technique (n = 23),
torque release technique (n = 6),
and other (n = 55), with n = 1, not indicated.Descriptions of these techniques are provided in Table 1. [10, 11]

Table 1 With respect to treatment-associated aggravations, complications, and improvements, these were not mutually exclusive for each patient. From 5,438 visits where SMT was rendered at each visit, there were three separate reports of treatment-associated aggravations. These were reported as “muscle stiffness,” “spine soreness through the seventh visit,” and “stiff and sore” after SMT to the first cervical vertebrae. The attending chiropractor’s response to the treatment-associated aggravations was to address the complaint by following a course of care consisting of a reexamination and application of a different SMT technique, modification of the SMT technique rendered, or modification of the spinal segment that was rendered the SMT. No treatment-related complications were reported by the patients or their parents/ guardians.
Of the 577 clinical cases, the respondent chiropractors reported 518 patients as experiencing an improvement in their presenting complaint, attributed to the care they received.
Parent/Guardian Survey
The data were provided by 239 parents reporting on a similar number of children. The parents ranged in age from 20 to 51 years, with an average age of 35.58 years (median = 34 years; mode = 33 years). With respect to gender, there were 222 females and 16 males, with one not indicating.
Based on their reported levels of education,7 had PhDs,
29 had Master’s degrees,
73 were baccalaureates,
35 had college certification,
61 had “some college,”
26 were high school graduates,
three had “some high school,” and
five did not indicate level of education.Of the 239 children, 113 were female and 119 were male, with seven genders not indicated. They ranged in age from less than a day to 18 years. Their average age was 6.16 years (median ! 4.67 years; mode = seven years). The patients attended a total of 1,735 visits, with an average of 7.26 visits (median = 11; mode = 12).
With respect to the reasons for seeking chiropractic care, 47% of patients (n = 112) presented for wellness care.
Of those patients indicating a specific complaint, the most common weremusculoskeletal complaints (n = 54);
ear, nose, and throat problems (n = 10);
neurological problems (n = 7);
colic (n = 6);
digestion/elimination problems (eg, constipation and enuresis; n = 9);
immune dysfunction (eg, asthma; n = 3);
birth trauma (n = 7); and
others (n = 26).With respect to treatment-related aggravations, complications, or improvement, these were not mutually exclusive for each patient. Of the 239 clinical cases, 162 parents reported treatment-related improvements, two reported treatment-associated aggravations, and none reported treatment-associated complications. Of the two treatment-associated aggravations, one was a report of soreness of the knee following care to address a knee complaint, and the other was stiffness of the cervical spine following SMT to address cervical spine dysfunction.
Of the types of treatment-associated improvements in relation to their indicated presenting complaints, the most common reported improvements were decreased pain (n = 33), improved mood (n = 18), and increased immune function (n = 17).
Interestingly, treatment-associated improvements unrelated to the patients’ initial clinical presentation were reported by many parents. The three most commonly reported improvements wereimmune system–related improvements (eg, sick less often; n = 34),
improved sleep; n = 27), and
improved emotional state or mood (eg, calmer or happier; n = 19).In all, 98 patients were reported as having improvements that were unrelated to their primary reason for seeking chiropractic care.
Discussion
Safety/Adverse Effects
The area of greatest controversy regarding the safety of chiropractic care has been that of SMT of the cervical spine. DiFabio [12] examined 177 cases involving SMT of the cervical spine as reported in 116 articles published between 1925 and 1997. Although the subjects’ age ranged from four months to 87 years, the majority of the cases involved adult patients (average age 39.6 years), and those involving children (ie, aged <18 years) were not well described. The most frequently reported injuries involved arterial dissection or spasm, lesions of the brain stem, and Wallenberg syndrome. The “other” category included visual deficits, hearing loss, balance deficits, and phrenic nerve injury. Ernst [13] described two cases associated with an adverse reaction to SMT. One case involved an infant with congenital torticollis treated with chiropractic spinal manipulation. [14] Within a few hours of receiving care, the child suffered from respiratory distress, quadriplegia, and seizures. A holocord astrocytoma with excessive acute necrosis was found and resected. The second case involved a three-month-old girl treated by a German physiotherapist with forced rotation and retraction of the head. [15] As a result of the care rendered, both vertebral arteries dissected, causing ischemia of the caudal brain stem with subarachnoid hemorrhage. The diagnosis was confirmed with magnetic resonance imaging, and the child died.
Second only to chiropractors in frequency, osteopaths often perform SMT on patients as part of their treatment approach. To address the issue of safety of pediatric osteopathic SMT (OSMT), Hayes and Bezilla [16] performed a retrospective review of medical records of pediatric patients receiving OSMT. Treatment-associated aggravations and complication as previously defined were documented. Of 502 records reviewed, 346 files met their inclusion criteria (ie, patient received two or more office visits) for analysis. No OSMT-related complications were documented. Nine percent (n = 31) of 346 patients reported an OMT-associated aggravation; specific reports included worsening symptoms (n = 7), behavior problems (n = 5), irritability (n = 5), pain (n-4), soreness (n = 4), headache (n = 2), dizziness (n = 1), flulike symptoms (n = 1), treatment reaction (n = 1), and tiredness (n = 1). Based on their findings, Hayes and Bezilla [16] concluded that OSMT appears to be a safe treatment modality for the pediatric population.
Vohra et al [17] performed a systematic review of the literature documenting adverse events associated with pediatric SMT. Using eight databases and spanning a timeline of 104 years of scientific publications, Vohra et al [17] found only 14 instances of adverse events associated with pediatric SMT. The adverse events include irritability (n = 1), loss of consciousness (n = 1), midback soreness (n = 1), acute lumbar pain (n = 1), headache and stiff neck (n = 1), severe neurological deficits (n = 5), anterior dislocation of the atlas and fracture of the odontoid axis at C2 (n = 1), atlas dislocation (n = 1), and death (n = 2). Ten of the 14 cases were attributed to chiropractic. Controversy remains around the interpretation of the findings of this review. Five of the 10 cases involved adverse events that were minor, self-limiting, and did not require hospitalization or medical attention. In the cases involving severe neurological loss or spine fracture or death, the patients had a preexisting medical condition and/or had a history of neurological trauma, which make it difficult to clearly attribute the adverse event to the SMT
Miller and Benfield [18] recently published a three-year retrospective analysis of adverse events associated with pediatric SMT at the Anglo European College of Chiropractic. Based on 697 children attending 5,242 patient visits, the authors reported that minor adverse reaction is likely to occur at the rate of approximately one per 100 children, or one reaction reported for every 749 treatments in their patient population. Two potential concerns regarding this review are the fact that an adverse event was based solely on parental report of excessive crying, and that the study was performed at a chiropractic teaching clinic with SMT rendered by chiropractic students. Questions remain regarding whether excessive crying on parent report is an adequate way to evaluate adverse effects, and also regarding whether the outcomes of care rendered by students can be generalized to the overall practice of pediatric chiropractic. Our survey of chiropractors reported that 0.51% of the patient population, or one in 1,812 patient visits resulted in a minor adverse events. The results from our parent survey indicate 0.83% of the patient population, or one in 867 clinical encounters, resulted in a minor adverse event. All reported aggravations (from chiropractor and parent survey) were minor, self-limiting, and did not require hospitalization or medical attention. More importantly, the complaints were addressed by the treating chiropractor in subsequent visits and did not dissuade the parent from continuing care for their child.
Based on the National Cancer Institute’s [19] the reported adverse events reported herein were mild (ie, minor, no specific medical intervention, asymptomatic laboratory findings only, radiographic findings only, marginal clinical relevance) in nature. Minor side effects have been reported in 30% to 55% of adults receiving chiropractic SMT, [20-23] whereas in this study, less than 1% of the pediatric population experienced minor adverse events based on chiropractor and parent responders. Several factors may contribute to the low prevalence of adverse events, including possible underreporting of adverse events, limitations in our study design, and selection bias in patients choosing to participate. It is also possible that chiropractors and other clinicians performing SMT in children, aware as they are of the unique biomechanical features of the pediatric spine, [5] are more cautious in their approach than some may be in their approach to SMT in adults. The forces applied during SMT in children are much less than those applied to adults; contact points are altered, patient and chiropractor positions are modified, and low force techniques are compared to high-velocity techniques may be applied less frequently. Also, the malleable and hypermobile nature of the pediatric spine may confer a greater amount of adaptability in the pediatric spine as compared with the typical response seen in adults.
Chiropractic and Wellness Care
According to Jean and Cyr, [24] pediatric patients use CAM approaches for a wide variety of health issues, but principally for chronic conditions involving musculoskeletal, psychological, and infectious problems. Spigelblatt et al [4] found that the three most common presenting conditions/reasons for children seeking chiropractic care were respiratory; ear, nose, and throat problems; and musculoskeletal conditions. Nyiendo and Olsen [25] examined the characteristics of 217 children attending care at a chiropractic college teaching clinic and found that 42% suffered from musculoskeletal complaints, 20% from nonmusculoskeletal complaints, and 33% attended the clinic for general physical examination. Verhoef and Papadopoulos [26] examined the treatment of patients aged less than 18 years by Canadian chiropractors and found that musculoskeletal conditions were the most common presenting complaints, followed by asthma and headaches. The findings of our study support the popularity of musculoskeletal conditions as a presenting complaint in the pediatric population insofar as when there is a specific condition indicated.
An important finding of our study, however, is the high frequency with which children were brought to the chiropractor specifically for wellness care. As pointed out by Hawk, [27, 28] chiropractic has at its core a vitalistic and holistic theoretical framework and approach to patient care, which incorporates a number of prevention and health promotion strategies, [27-30] particularly in the training of chiropractors. With the formalization of the model course for public health education in chiropractic colleges [31] and inclusion of public health preventive measures within the scope of chiropractic practice, [32] chiropractic is actively moving toward becoming a “wellness profession.” [27-31] The findings of our study demonstrate that this evolution is being manifested in the clinical practice of pediatric chiropractic. The frequency of wellness care as a motivation for chiropractic care of children was first documented by Rubin. [33] In examining the presenting complaints of new patients to his pediatric clinic, he found that wellness care was a common reason for presentation, along with spinal, respiratory, stomach, and sleep problems. Some studies also show a similar phenomenon in adults; in an international survey of sacro-occipital technique in adult patients, Blum et al [34] found that 42% of 1,316 patients presented for care either for wellness, prevention, or to reduce their risk of illness or injury. Kemper, [35] in addressing the issue of effectiveness of CAM therapies for children, admonished that to answer the question of whether or not CAM therapies work, one of the essential components must be that the families’ goals and expectations of treatment be elicited systematically. The role of wellness care in a family’s choice to pursue chiropractic care should be part of this evaluation Limitations
This study has several limitations. One limitation of our study is the possible underreporting of adverse events by both chiropractors and parents predisposed to view SMT in a positive light. Selection bias (ie, volunteer bias) and measurement bias (ie, attention bias) likely played a role in the results obtained in our study. The PBRN chiropractors were selected mainly from the ICPA membership; members of the ICPA are interested in promoting the chiropractic care of children and wellness care.27,36 Also noteworthy is the bias on the part of the parent population, as they were recruited from the PBRN. Selection bias may exist in that only those parents with positive outcomes of care or lack of adverse events in the care of their child may have been selected. Additionally, studies continue to support the idea that parent CAM users are more likely to use CAM use for their children.24 It is likely that our parent responders were also receiving chiropractic care under the paradigm of wellness care.
CONCLUSION
To the best of our knowledge, this is the first study of its kind addressing the safety and effectiveness of pediatric chiropractic SMT in a practice-based research setting. The results of both our practitioner surveys and our parent surveys demonstrate a highly perceived effectiveness for pediatric chiropractic care as well as a high level of safety. We advocate continued research in this area, with larger prospective cohorts incorporating the covariates of safety and effectiveness of pediatric SMT.
References:
Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Ottolini MC, Hamburger EK, Loprieato JO, et al.
Complementary and alternative medicine use among children in the Washington, DC area.
Ambul Pediatr. 2001;1:122-125.Barnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Spigelblatt L, Laine-Ammara G, Pless IB, Guyver A.
The use of alternative medicine by children.
Pediatrics. 1994;94(6 pt 1):811-814.Alcantara J, Plaugher G, Anrig C.
Pediatric chiropractic.
In: Redwood D, Cleveland C, eds. F
undamentals of Chiropractic.
St. Louis, Mo: Mosby Inc; 2003:349-364.Lee AC, Li DH, Kemper KJ.
Chiropractic care for children.
Arch Pediatr Adolesc Med. 2000;154:401-407.Huijbregts PA.
Manual therapy in children: role of the evidencebased clinician.
J Manual Manipulative Ther. 2006;14:7-9.Fearon J.
Complementary therapies: knowledge and attitudes of health professionals.
Pediatr Nurs. 2003;15:31-5.Kemper KJ, Vohra S, Walls R.
The Use of Complementary and Alternative Medicine in Pediatrics
Pediatrics. 2008 (Dec); 122 (6): 1374-1386Torque release technique.
Holder Research InstituteChiropractic techniques.
American Chiropractic Association Web site.
Accessed March 24, 2009.Di Fabio RP.
Manipulation of the cervical spine: risks and benefits.
Phys Ther. 1999;79:50-65.Ersnt E.
Serious adverse effects of unconventional therapies for children and adolescents: a systematic review of recent evidence.
Eur J Pediatr. 2003;162:72-80.Shafir Y, Kaufman BA.
Quadraplegia after chiropractic manipulation in an infant with congenital torticollis caused by a spinal cord astrocytoma.
J Pediatr. 1992;120:266-268.Jacobi G, Riepert T, Kieslich M, Bohl J.
Fatal outcome during physiotherapy (Vojta’s method) in a 3-month old infant. Case report and comments on manual therapy in children.
Klin Paediatr. 2001;213: 76-85.Hayes NM, Bezilla TA.
Incidence of iatrogenesis associated with osteopathic manipulative treatment of pediatric patients.
J Am Osteopath Assoc. 2006;106:605-608.Vohra S, Johnston BC, Cramer K, Humphreys K.
Adverse Events Associated with Pediatric Spinal Manipulation: A Systematic Review
Pediatrics. 2007 (Jan); 119 (1): e275–e283Miller JE, Benfield K.
Adverse Effects of Spinal Manipulative Therapy in Children Younger Than 3 Years:
A Retrospective Study in a Chiropractic Teaching Clinic
J Manipulative Physiol Ther 2008 (Jul); 31 (6): 419–423National Cancer Institute.
Common Terminology Criteria for Adverse Events v3.0 (CTCAE). Available at:
http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_v40
Accessed February 9, 2009.Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM.
Adverse reactions to chiropractic treatment and their effects on satisfaction and clinical outcomes among patients enrolled in the UCLA Neck Pain Study.
J Manipulative Physiol Ther. 2004;27:16-25.Senstad O, Leboeuf-Yde C, Borchgrevink CF.
Side-effects of chiropractic spinal manipulation: types, frequency, discomfort and course.
Scand J Prim Health Care. 1996;14:50-53.Senstad O, Leboeuf-Yde C, Borchgrevink CF.
Frequency and characteristics of side effects of spinal manipulative therapy.
Spine. 1997; 22:435-441.Leboeuf-Yde C,Hennius B, Rudberg E, Leufvenmark P, ThunmanM.
Side effects of chiropractic treatment: a prospective study.
J Manipulative Physiol Ther. 1997;20:511-515.Jean D, Cyr C.
Use of complementary and alternative medicine in a general pediatric clinic.
Pediatrics. 2007;120:e138-e141.Nyiendo J, Olsen E.
Visit characteristics of 217 children attending a chiropractic college teaching clinic.
J Manipulative Physiol Ther. 1988;11:78-84.Verhoef M, Papadopoulos C.
Survey of Canadian chiropractors’ involvement in the treatment of patients under the age of 18.
J Can Chiropr Assoc. 1999;43:50-57.Hawk C.
The wellness hypothesis.
In: Leach R, ed. The Chiropractic Theories.
Baltimore, Md: Williams & Wilkins; 2003:399-415.Hawk C.
Should chiropractic be a “wellness” profession?
Top Clin Chiropr. 2000;7:23-26.Hawk C, Dusio ME.
Chiropractors’ attitudes toward training in prevention: results of a survey of 492 U.S. chiropractors.
J Manipulative Physiol Ther. 1995;18:135-140.Hawk C, Dusio ME.
A survey of 492 US chiropractors on primary care and prevention-related issues.
J Manipulative Physiol Ther. 1995; 18:57-64.Health Resources and Services Administration.
A Model Course for Public Health Education in Chiropractic Colleges.
Washington, DC: Association of Schools of Public Health; 2002.
ASPH Project #H092-04/04.The Council on Chiropractic Education.
Standards for Doctor of Chiropractic Programs and Requirements for Institutional Status.
Scottsdale, Ariz: The Council on Chiropractic Education; 200: 45-47.Rubin S.
Triage and case presentations in a chiropractic pediatric clinic.
J Chiropr Med. 2007;6:94-98.Blum C, Globe G, Terre L, Mirtz TA, Greene L, Globe D.
Multinational survey of chiropractic patients: reasons for seeking care.
JCCA J Can Chiropr Assoc. 2008;52:175-184.Kemper KJ.
Complementary and alternative medicine for children: does it work?
Arch Dis Child. 2001;84:6-9.Chan E, Rappaport LA, Kemper KJ.
Complementary and alternative therapies in childhood attention and hyperactivity problems.
J Behav Pediatr. 2003;24:4-8.
Return to PEDIATRICS
Since 11-07-2009
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |