|
|
Upper Extremity Pain: Clues Within the History Postural Disorders of the Upper Extremity Spasm Within the Shoulder Girdle Trigger Points of the Shoulder Area Painful Shoulder Syndromes Injuries of the Shoulder Joint Shoulder Sprains and Strains Subluxations of the Shoulder Dislocations of the Shoulder Fractures of the Humerus Injuries of the Scapular Area Injuries of the Clavicle Subluxations of the Clavicleluxation Dislocations of the Clavicle Fractures of the Clavicle The Elbow and Forearm Basic Functional Anatomy Elbow and Radioulnar Movements Trigger Points Selected Clinical Problems of the Elbow and Forearm Roentgenographic Considerations Elbow Strains Elbow Sprains Tennis Elbow Olecranon Bursitis Subluxations of the Elbow Fractures and Dislocations of the Elbow Area Nerve Compression Injuries The Wrist Basic Functional Anatomy Wrist Movements Selected Clinical Problems of the Wrist Area Trauma of the Wrist Area Wrist Sprains and Related Disorders Subluxations of the Wrist Fractures and Dislocations of the Wrist Area Compression Syndromes The Hand and Thumb Thumb Movements Trigger Points Dislocations of the Thumb Selected Clinical Problems of the Hand and Thumb Direct Trauma Sprained Thumb The Fingers Basic Functional Anatomy Finger Movements Trigger Points Structural Fixations in the Hands Selected Clinical Problems of the Fingers Metacarpophalangeal and Interphalangeal Sprains Mallet Finger Trigger Finger Contractures Fractures and Dislocations of the FingersChapter 10:
The Upper Extremity
From R. C. Schafer, DC, PhD, FICC's best-selling book:
“Clinical Biomechanics: Musculoskeletal Actions and Reactions”
Second Edition ~ Wiliams & Wilkins
The following materials are provided as a service to our profession. There is no charge for individuals to copy and file these materials. However, they cannot be sold or used in any group or commercial venture without written permission from ACAPress.
All of Dr. Schafer's books are now available on CDs, with all proceeds being donated
to chiropractic research. Please review the complete list of available books.
The Shoulder Girdle and Arm Basic Functional Anatomy The Shoulder Girdle Shoulder Movements Active and Passive Range of Motion Shoulder Motion Kinesiology of the Shoulder Girdle Goniometry of the Shoulder Selected Clinical Problems of the Shoulder Girdle
| Joint Motion | Prime Movers | Accessories |
| SHOULDER GIRDLE | ||
| Elevation | Trapezius, upper Levator scapulae Rhomboids, major and minor | |
| Depression | Trapezius, lower Latissimus dorsi Pectoralis major, sternal head Pectoralis minor | |
| Abduction | Serratus anterior Pectoralis major and minor | |
| Adduction | Trapezius, upper and lower Rhomboids, major and minor | |
| Upward rotation | Serratus anterior Trapezius, upper and lower | |
| Downward rotation | Levator scapulae Rhomboids, major and minor Pectoralis minor | Latissimus dorsi |
| SHOULDER | ||
| Flexion | Deltoid, anterior Coracobrachialis Pectoralis major, clavicular head | |
| Extension | Deltoid, posterior Teres major Latissimus dorsi Pectoralis major, sternal head | Infraspinatus, lower fibers Teres minor Triceps, long head |
| Abduction | Deltoid, middle Supraspinatus | Deltoid, anterior and posterior |
| Horizontal abduction | Deltoid, posterior | Infraspinatus Teres minor |
| Adduction | Pectoralis major Teres major Latissimus dorsi | Triceps, long head Coracobrachialis Biceps brachii, short head |
| Horizontal adduction | Pectoralis major Deltoid, anterior | Biceps brachii, short head Coracobrachialis |
| External rotation | Infraspinatus Teres minor | Deltoid, posterior |
| Internal rotation | Subscapularis Pectoralis major Latissimus dorsi Teres major | Deltoid, anterior |
Flexion. Shoulder flexion is conducted primarily by the anterior deltoid (C5-C6) and coracobrachialis (C5-C6) with assistance by the clavicular head of the pectoralis major (C5– T1) and biceps (C5-C6). Strength of flexion can be tested from the back of the patient by placing the stabilizing hand on the patient's shoulder so that the anterior deltoid may be palpated during testing. The examiner's active hand grips the patient's anterior lower arm. With the patient's elbow flexed to 90°, resistance is increased as the patient is asked to flex the shoulder. Muscle strength is recorded by grade or in a percentage and compared bilaterally (Fig. 10.4).
Extension. Extension of the shoulder is controlled by the latissimus dorsi (C6– C8), teres major (C5-C6), and posterior part of the deltoid (C5-C6). Assistance is offered by the teres minor (C5-C6) and long head of the triceps (C7-C8). Strength of extension is judged from the back of the patient with the stabilizing hand in nearly the same position so as to palpate the posterior deltoid while the palm of the active hand grips the patient's lower arm at the posterior. The patient's elbow is again flexed, and he or she is asked to slowly extend the shoulder against increasing resistance.
Abduction. When the hand is abducted horizontally, the forces created at the shoulder joint have been calculated to approximate total body weight. Shoulder abduction is conducted by the middle deltoid (C5-C6) and supraspinatus (C5-C6) with assistance by the serratus anterior (C5– C7). Strength of abduction can be tested at the side of the patient by placing the stabilizing hand on the lateral shoulder tip so that the middle of the deltoid may be palpated. The examiner applies increasing resistance laterally above the flexed elbow of the patient as abduction is attempted (Fig. 10.5).
Adduction. Adduction of the shoulder is controlled by the pectoralis major (C5– T1) and latissimus dorsi (C6– C8). Assistance is offered by the teres major (C5-C6) and anterior deltoid (C5-C6). Strength of adduction is measured from behind the patient with the stabilizing hand still on the shoulder tip. The patient's arm is abducted and the elbow is flexed. The examiner then applies increasing resistance medially above the flexed elbow of the patient as the patient attempts adduction.
Internal Rotation. Internal rotation of the shoulder is controlled by four muscles: the subscapularis (C5-C6), pectoralis major (C5– T1), latissimus dorsi (C6– C8), and teres major (C5-C6). The anterior deltoid assists. Strength of the internal rotators is tested with the examiner's stabilizing hand and active hand in the same position. An increasing pulling resistance is applied to the patient's wrist as the patient attempts internal rotation of the arm by moving the hand toward the abdomen (Fig. 10.6).
External Rotation. External rotation of the shoulder is conducted by the infraspinatus (C5-C6) and teres minor (C5), with assistance by the posterior part of the deltoid. Strength of external rotation is judged at the side of the patient by placing the stabilizing hand on the patient's flexed elbow with the examiner's thumb in the angle of the patient's elbow. The active hand, gripping the patient's wrist, applies an increasing pushing resistance to the patient's attempt to externally rotate the arm by moving the hand away from his body (Fig. 10.7).
Scapular Elevation. Shoulder elevation is conducted by the trapezius (XI, C3-C4) and levator scapulae (C3– C5) with assistance from the major and minor rhomboids (C5). Strength is judged by the examiner standing behind the patient and applying increasing resistance with both palms on the patient's shoulders as the patient attempts to shrug his shoulders (Fig. 10.8).
| Muscle | Major Function | Spinal Segment |
| Biceps brachii | Flexion, adduction (short head) | C5-C6 |
| Coracobrachialis | Flexion, adduction | C5-C6 |
| Deltoid | ||
| Anterior fibers | Flexion, internal rotation, abduction, horizontal adduction | C5-C6 |
| Dorsal fibers | Extension, external rotation, horizontal abduction | C5-C6 |
| Middle fibers | Abduction | C5-C6 |
| Infraspinatus | External and lateral rotation, extension (lower fibers), horizontal abduction | C5-C6 |
| Latissimus dorsi | Extension, adduction, medial rotation, depression, downward rotation | C6-C8 |
| Levator scapulae | Elevation, downward rotation | C3-C5 |
| Pectoralis major | Adduction, flexion, depression | C5-T1 |
| Clavicular head | Flexion, medial rotation, adduction | C5-C7 |
| Sternal head | Extension, depression, medial rotation | C6-T1 |
| Pectoralis minor | Adduction, medial/downward rotation, flexion, depression, extension | C7-C8 |
| Rhomboids | Retraction, elevation, adduction, downward rotation | C5 |
| Serratus anterior | Protraction, abduction, upward rotation, depression (lower fibers) | C5-C7 |
| Subscapularis | Medial rotation and adduction | C5-C6 |
| Supraspinatus | Abduction | C5-C6 |
| Teres major | Extension, adduction, medial rotation | C5-C6 |
| Teres minor | External/lateral rotation, extension | C5-C6 |
| horizontal abduction | C5 | |
| Trapezius | Retraction | C3-C4, XI |
| Upper fibers | Elevation, adduction, upward rotation | |
| Lower fibers | Depression, adduction, upward rotation | |
| Triceps | Adduction, extension (long head) | C7-C8 |
Scapular Depression. Shoulder retraction is controlled by the major and minor rhomboids, both of which are usually innervated solely by C5. The trapezius assists. To evaluate the strength of scapular depression, the examiner stands in front of the patient with his hands grasping the patient's shoulder tips over the upper deltoids. The doctor's thumbs are braced under the patient's clavicles, and the fingers are behind the deltoids. The patient is instructed to slowly "throw his shoulders back and down" while the examiner applies increasing resistance; ie, forward toward the thumbs.
Shoulder Protraction. Protraction of the shoulder is conducted by the serratus anterior (C5– C7). In determining strength of protraction, with the examiner behind the patient, the patient is asked to flex the arm so that it is parallel to the floor with the elbow at a right angle to the arm. The examiner's stabilizing hand is placed in the midscapular area to stabilize the patient's spine from rotating, and the active hand is cupped around the patient's flexed elbow. Increasing resistance is applied as the patient attempts to slowly thrust the arm forward as if to touch a forward wall. During this movement, the examiner observes the scapula for possible winging (Fig. 10.9).
"The troublesome fifth cervical area" was discussed in Chapter 7. In this context, note in the above that shoulder girdle flexion, extension, abduction, adduction, internal rotation, external rotation, scapular elevation, scapular depression, and shoulder protraction are all subject to function of the C5 root.
GONIOMETRY OF THE SHOULDER
Restricted Forward Elevation. Place the patient in the neutral position, center the goniometer next to the shoulder, then record the neutral reading with the goniometer arm along the upper arm axis. Have the patient elevate both arms as far as possible, then record the arm readings at the end of the motion.
Restricted Backward Elevation. Place the patient in the neutral prone position, center the goniometer next to the shoulder, and record the neutral reading with the goniometer arm along the axis of the upper arm. Have the patient elevate both arms as far as possible, then record the arm being tested at the end of the motion.
Restricted Abduction or Adduction Motion. Place the patient in the neutral position, center the goniometer over the shoulder. With the goniometer arm along the axis of the arm, record the neutral reading. Have the patient abduct both arms, and record the readings at the end of the motion. Then rotate the goniometer base, have the patient adduct the arm to be tested, and record the reading at end of the motions.
Restricted External or Internal Rotation Motion. Place the patient in the neutral position, center the goniometer next to the elbow, and record the neutral reading (90°) with the goniometer arm along the axis of the forearm. Have the patient attempt to touch the back of the hand and forearm to the top of the examining table. Record the reading for external rotation at the end of the motion. After returning to the neutral position, have the patient attempt to touch the palm and volar surface of the forearm to the table top. Record the reading for internal rotation at the end of the motion.
Ankylosis. When taking the above measurements in ankylosis, measure any deviation from the neutral position.
A general classification of musculoskeletal and related disorders of the upper extremity is offered in Table 10.3.
Trapezius. Increased tone tends to pull the shoulder girdle medial and the occiput posteroinferior and the involved spinous processes lateral (Fig. 10.10).
Many authorities feel that the excessive hypertonicity commonly witnessed is the result of overstress. However, Nelson doubts the muscular "overuse" concept and offer this thought: "The more a muscle is used, the stronger it gets. Certainly, there may be a subluxation, but it would be the result of the muscle spasticity. The cause then must be a nervous or circulatory defect wherein the muscle cannot do sustained work without spasticity. A normal muscle merely tires."
Passive Stretch. Mild passive stretch is an excellent method of reducing spasm in the long muscles, but heavy passive stretch destroys the beneficial reflexes. In rhomboid spasm, for example, the prone patient should place his hand on the involved side behind his back to "wing" the scapula. This slightly stretches the muscle fibers by pulling the scapula from the midline. This may be assisted by the doctor offering a slight tug upward on the scapular angle. The muscle should relax within 2-3 minutes. Thumb pressure, placed on a trigger area, is directed toward the muscle's attachment and held for a few moments until relaxation is complete. Resisting active antagonist contraction is also helpful, especially if the disorder is highly acute.
1. Overuse of poorly conditioned tissues is the common cause. The shoulder tendons are wide bands of collagen fibers. If stress roughens a tendon, its tensile strength decreases. This leads to fibrinoid degeneration in and between the collagen fibers and later fibrosis. With necrosis and the initial inflammatory reparative process, the local tissues become alkaline, which induces precipitation of calcium salts. This deposition may evade an overlying bursa.
Dawbarn's Sign. Still holding pressure, abduct the patient's arm above the horizontal. This should decrease the tenderness. That is, an inflamed subacromial bursa is exposed to palpation when the arm is relaxed, but not when the arm is abducted beyond a right angle.
The shoulder girdle is a common site of minor injury and a not infrequent site of serious disability. It is second only to the knee as a site of chronic prolonged disability. Most shoulder injuries are not single-entity injuries. They are composed of a variety of contusions, strains, and sprains, and possible avulsion and fracture. Fixed dislocations, spontaneously reduced dislocations, and subluxations also complicate the picture. Thus, any painful shoulder syndrome requires careful differentiation.
Selected Clinical Problems of the Shoulder Girdle
Upper Extemity Pain: Clues Within the History
Shoulder pain has a high incidence. Cailliet states that it is second only to low-back and neck pain. Upper extremity pain may be the result of any structural disorder of the limb or a disturbance elsewhere in which the sensory phenomena are referred to the limb. Pain situated in various parts of the extremities will often reveal the point of origin by its peculiar location and quality. The pain may be of mechanical, chemical, thermal, toxic, nutritional, metabolic, or circulatory origin, or a combination of some of these factors depending upon the nature of the pathologic process involved. The most important clues toward determining cause – type of pain, its distribution, and its associated symptoms– are the result of a carefully taken case history.
Peripheral nerve disease frequently indicates a history of entrapment neuropathy. The origin of nerve root lesions may be traced to trauma, a herniated disc, compression, hypertrophic changes in the vertebrae, neoplasms, or inflammation of the nerve root. Differentiation should be made from rare nutritional disorders resulting in a polyneuropathy because of unfavorable metabolic activities within the nerve cells. Peripheral neuritis, less common than peripheral neuropathy, can be classified into one of three types: infectious, allergic, or idiopathic.
Postural Disorders of the Upper Extremity
Shoulder girdle pain and discomfort are often seen in typists, assembly-line workers, and laborers who work overhead with repetitive motions for long durations with little postural change. Most authorities believe the cause can usually be traced to muscular overuse leading to lower cervical or upper thoracic subluxations. Fixated misalignments may be found in the shoulder girdle itself, especially when the scapulae are chronically affected. Acute or chronic fibrositis of the trapezius and rhomboids with trigger points is often superimposed or consequential.
MUSCLE STRENGTHENING
In the therapeutic alignment of the thoracic spine and the shoulder girdle, the common muscles to be strengthened are the scapular adductors and rotators; eg, trapezius, rhomboid major and minor, infraspinatus, and teres minor. Invariably, an associated weakness will be found in the gluteals and abdominals inducing pelvic misalignment.
MUSCLE STRETCHING
The common muscles to be stretched in postural misalignment of the thoracic spine and shoulder girdle are the shoulder adductors and medial rotators; eg, the latissimus dorsi, teres major, subscapularis, and pectoralis major and minor. When these muscle are stretched, the scapula should be firmly stabilized.
Spasm Within the Shoulder Girdle
SELECTED EFFECTS OF HYPERTONICITY IN THE SHOULDER GIRDLE
Excessive hypertonicity of a muscle, confirmed by palpatory tone and soreness, will tend to subluxate its site of osseous attachment. Below is a listing of common problem areas in the upper extremities.
Levator Scapulae. Increased tone tends to pull the scapula medial and superior and the involved transverse processes inferior, lateral, and posterior.
Rhomboid Major. Increased tone tends to pull the scapula medial and superior and the spinous processes lateral and inferior.
Rhomboid Minor. Increased tone tends to pull the scapula medial and superior and the spinouses lateral and inferior.
SPASM MANAGEMENT
Spasm management is usually necessary prior to articular correction and following articular correction to hold the adjustment in alignment.
Therapeutic Exercises. When pain has subsided, two beneficial home progressive exercises are (1) gravity-assisted pendulum exercises holding a weight or iron while prone and (2) holding a broomstick in front with both hands and doing elevations. Isotonic exercises are useful in improving circulation and inducing the stretch reflex when done supine to reduce exteroceptive influences on the central nervous system.
Modalities. Other adjunctive therapies may also be helpful. Peripheral inhibitory afferent impulses can be generated to partially close the presynaptic gate by acupressure, acupuncture, or transcutaneous nerve stimulation. An acidbase imbalance from muscle hypoxia and acidosis may be prevented by supplemental alkalinization. In chronic cases, high-voltage galvanic, relaxation training, and biofeedback therapy are beneficial.
Trigger Points of the Shoulder Area
Various sites of myodysneuria are frequently active in upper extremity intrinsic or extrinsic disorders, or in situations of referred pain. Daily goading of these points by a thumb pad to patient tolerance for 1-2 seconds or steady pressure for 30– 60 seconds can be both diagnostic and therapeutic.
A common source of many shoulder pains sited in the anterolateral shoulder will be found at the insertions of the infraspinatus and supraspinatus muscles at the scapula (Fig. 10.11). In other cases, a localized trigger point may be found in the anterior deltoid, with pain referred to the subdeltoid bursa, or in the sternalis, which refers pain across the chest and down the medial arm (Fig. 10.12).
Other common trigger-point sites in shoulder pain include the lesser tuberosity at the insertion of the subscapularis, the greater tuberosity at the insertion of the supraspinatus tendon, at the glenohumeral joint space, within the bicipital groove, at the acromioclavicular joint, or at the sternoclavicular joint. The levator scapulae, scaleni, pectoralis major and minor, and serratus anterior are less common sites.
Painful Shoulder Syndromes
Tendon inflammation is not as common in the shoulder as it is in the elbow and wrist. However, because tendons are relatively avascular, they are subject to chronic trauma, microtears, slow repair, and aging degeneration in the shoulder.
Most shoulder syndromes involve a degree of either overuse or underuse:
2. Excessive postinjury immobilization leads to muscle atrophy and loss of capsular elasticity, a predisposing factor to capsulitis and periarthrits. Lack of joint movement fosters retention of metabolites, edema, venous stasis, and ischemia leading to fibrous adhesions and trigger-point development.
SUPRASPINATUS TENDINITIS
Inflammation of paratendinous supraspinatus tissues is often a part of subdeltoid or subacromial bursitis. It is also frequently a part of rotator cuff injury and a complication of severe supraspinatus strain. An ache is present on rest which is aggravated by abduction. Pain may be referred as far distal as the deltoid insertion. The distinguishing feature is that pain is restricted to movement only within a certain point of the arc (painful arc syndrome). This is because the acromion process affects the tendon area only during part of its excursion. Point tenderness will be found over the site of inflammation. The patient will complain that it is painful to sleep on the affected side. Treatment is similar to that of bicipital tendinitis.
BICIPITAL TENDINITIS
The synovia of the bicipital groove is a common site of chronic paratendinous inflammation. It is frequently a complication of bicipital rupture (long head) or subluxation of the tendon from the groove. Pain is aggravated on abduction and extension, and tenderness is localized over the inflamed tendon. Most symptoms mimic supraspinatus tendinitis, but the pain is referred distally in the area of the biceps insertion to the radius. Tenderness is found along the anterior shoulder in the bicipital groove, and pain is increased if the patient abducts, flexes, and internally rotates the shoulder. When the patient flexes his arm and supinates his wrist against resistance, a positive sign is pain within the anterior medial upper humerus area. Bicipital tendinitis will greatly affect flexion and extension strength.
SUBDELTOID BURSITIS
Of the 140 bursae of the body, none have more trouble than the subdeltoid bursa (Fig. 10.13). When it becomes inflamed, the patient presents acute, severe, deep-seated local pain. There is weakness with shoulder movement in any plane but especially on abduction. Quite frequently, bursitis will usually limit flexion, extension, and both internal and external rotation. The entire bursa and paratendinous tissues will be swollen and readily palpable. This swelling prevents the greater tuberosity from sliding under the acromion during abduction. Dysfunction of the rotator, bicipital, and subscapularis tendons (which pass through the bursa) will commonly be demonstrated. The initial attacks are localized in the vicinity of the greater tubercle. The chronic stage is characterized by subdeltoid tenderness, restricted motion in abduction and external rotation, and associated capsular contraction and adhesions.
Shoulder bursitis is rarely a primary condition. Degenerative changes in the rotator cuff at the floor of the subdeltoid bursa lead to calcific deposits resulting in acute inflammation of the bursa. When a calcium deposit breaks into the bursa, it absorbs water. This enlarges the bursal space, resulting in increased pressure that exhibits severe pain and some warmth and redness of the overlying skin.
SUBACROMIAL BURSITIS
A painful, faltering abduction arc is also characteristic of subacromial bursitis. To differentiate, palpate the coracoid process under the pectoralis major. It is found by circumducting the humerus, and it is normally tender. Once the process is found, slide your finger slightly lateral and superior until it reaches a portion of the subacromial bursa. If the same palpation pressure here causes greater tenderness than at the process, it is a positive sign of subacromial bursitis.
SUPRASPINATUS CALCIFICATION
Tendon calcification is commonly found in the supraspinatus tendon, near its insertion at the greater tuberosity of the humerus. Symptoms arise suddenly. Pain is usually severe and aggravated by shoulder movement, but the pain is less severe and movements more tolerated than in supraspinatus tendinitis. Tenderness is localized over the bursa. A painful arc syndrome may be noted, similar to that seen in supraspinatus tendinitis. Associated bursitis may be present, which is responsible for much of the acute symptoms.
Deposits may appear in shoulder tendons, ligaments, or aponeuroses, and especially within the rotator cuff. They may be chronic, silent, or extremely acute. Spontaneous absorption may occur relatively fast. The calcification is viewed in roentgenography as a large dense opacity above the outer head of the humerus. It is most frequently related to middle age with no definite history of trauma, but it is only occasionally seen in the young. In the well-developed person, symptoms from calcification may not appear for many months after injury.
TRICEPS BRACHII CALCIFICATION
Repetitive stretching of the posterior elements of the shoulder from throwing frequently causes an inflammation of the posterior capsule tissues of the shoulder. This may result in an osteotendinous calcification at the infraglenoid area where the long head of the triceps originates. Once calcification forms, the follow through in throwing is quite painful.
CAPSULITIS
Capsulitis of the shoulder is often the result of a sprain attended by a spontaneously reduced subluxation or of prolonged overuse. Joint pain is aggravated by movement. Tenderness and other symptoms are generalized within the whole joint area rather than being localized. Motion limitation may be considerable in adhesive capsulitis (frozen shoulder) where the head of the humerus is "glued" to the glenoid cavity.
PERIARTHRITIS
Periarthritis of the shoulder – commonly called "frozen shoulder" or Duplay's syndrome– is often a challenge because it is usually near the terminal stage when the patient is first seen. A combination of several chronic, diffuse, degenerative shoulder disorders are usually involved. Loss of scapulohumeral rhythm is a characteristic feature. This is readily noted when viewed from the posterior. During the early stage, shoulder motion stiffens at the extreme ranges of abduction and internal rotation.
Differentiation must be made from the early stage of capsulitis. Humeral motion restriction is exhibited in all planes in periarthritis, but adduction and rotation are especially affected. Scapulothoracic motion, however, will be normal. Atrophy is readily noted and proportionate to the chronicity of the condition. Tenderness is diffuse throughout the upper arm with the possible exception of the posterior and medial aspects. The capsule becomes thick and contracted, which contributes to motion limitation. The rotator cuff also becomes thick and inelastic, and the tendon becomes cemented within the groove.
In time, the adhesions and soft tissues thicken and become tightly fixed, binding capsule to bone. As the joint cavity "dries", the head of the humerus is pulled tightly against the glenoid fossa. Arm use aggravates the condition, and symptoms are more acute at night after a day's activity. Rest offers relief, thus improvement is seen in the morning. The accessory muscles overwork in an attempt to compensate for primary shoulder muscle deficiency, causing aching posterior shoulder and neck muscles. A superiorly subluxated 1st rib or a lower cervical subluxation is usually a common and important contributing factor. Roentgenography is often negative with the exception of an obliterated joint space.
TRAUMATIC ARTHRITIS
Osteoarthritis of the shoulder is seen more in literature than in actual practice. Usually, the case is a periarthritis where degenerative changes have occurred within the soft tissues. The characteristic picture is one of pain, tenderness on pressure, and rarely some swelling. Passive motion is comparatively painless, but active motion induces severe pain. Differentiation must be made from supraspinatus rupture, subdeltoid bursitis, and inflammation of other bursae about the shoulder.
OTHER SYNDROMES
Cervical pathology and subluxation syndromes, traumatic brachial plexus traction, cervical ribs, and neurovascular compression syndromes frequently involve or refer pain to the upper extremity. These disorders have been discussed previously in Chapter 7. Upper rib and upper thoracic syndromes may also involve or refer pain to the upper extremity, and these have been discussed in Chapter 8.
The examiner should also keep in mind that both referred pain and tenderness may be of a visceral nature, especially from the liver, gallbladder, and right diaphragm to the right shoulder and from the stomach, left diaphragm, and heart to the left shoulder. Referred pain and tenderness, however, are not always predictable. It is not true that visceral reflexes do not affect local joint function. They may or may not produce musculoskeletal symptoms and signs.
Injuries of the Shoulder Joint
Shoulder Sprains and Strains
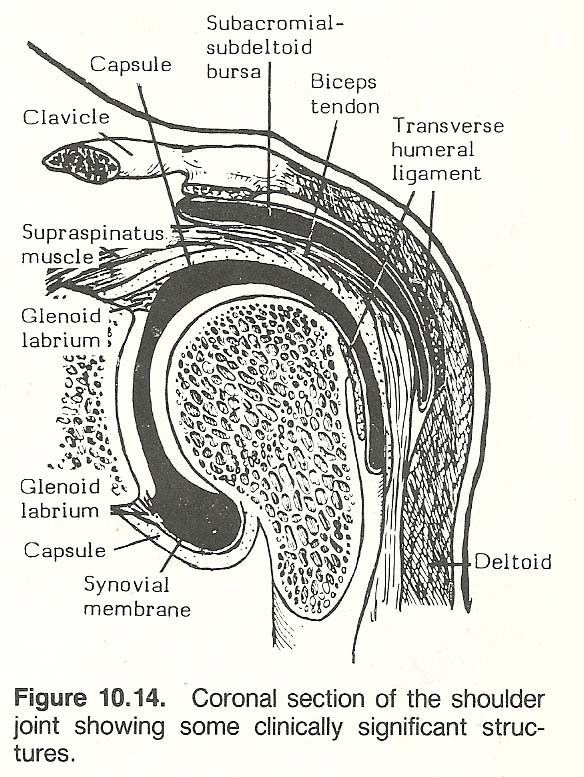 |
The shoulder is at the forefront of high-incidence injuries. Tears of the rotator cuff, usually without humeral displacement, are common. Most are the result of throwing injuries, falls on the shoulder point, and vertical forces directed along the humerus. Careful evaluation of the soft tissues is necessary (Fig. 10.14). Subclavian and axillary vessel injury may be the result of direct trauma or a sudden and violent shoulder movement. Rarely, just muscular hypertrophy may produce venous insufficiency or thrombosis. Brachial plexus and coracoid injuries are sometimes related in anterior blows. Epiphyseal injuries of the proximal humerus are rare, heal well, and are usually treated conservatively (closed).
GENERAL SHOULDER SPRAINS
The major symptoms and signs of shoulder sprain are pain, tenderness on pressure, and, rarely, swelling. Passive motion is comparatively painless, but active motion induces severe pain. Differentiation must always be made from rupture of the supraspinatus tendon, subdeltoid bursitis, fracture, and inflammation of other bursae about the shoulder.
THE LAX SHOULDER JOINT
Repeated subluxations without clinical dislocation often produce a loose joint. The history will reveal frequent episodes of mild trauma, each incorporating a period of pain and limited motion, followed by an audible "click" as the head of the humerus slips painfully back into the fossa. After reduction, examination reveals few signs except residual tenderness and a lax capsule.
Shoulder Stability. Stability in the shoulder is mainly dependent upon muscle tone and not ligament strength. This becomes readily apparent in paralysis. The weakest part of the shoulder joint is at the anterolateral aspect of the capsule, thus the greatest stress is applied to the joint when the arm is abducted to the horizontal and the humerus is externally rotated. The strongest position of the joint is when the arm is held downward and rotated internally. Note that this is the position instinctively used both in active shoulder "blocking" and when the arm is placed in a sling for rest.
The Lax Capsule Test. To determine a lax capsule, have the patient clasp his fingers behind his head and laterally abduct his elbows. Palpate high in the axilla over the glenohumeral capsule while applying posterior force on the patient's flexed elbow. While laxity of the anterior capsule can always be demonstrated by this maneuver, care must be taken not to dislocate the humerus within a loose capsule. If episodes of pain from the instability are frequent, some form of external support should be provided, and the patient should be advised of the risks involved in repeated subluxation.
THE BICIPITAL SYNDROME
In shoulder injury, after possible dislocation and fracture have been eliminated, special attention should be given to the bicipital muscle (Fig. 10.15). The biceps is the most powerful flexor of the elbow and a strong supinator. Within the shoulder area, proximal strains and tears along the long head's course within the bicipital groove to the glenoid rim are frequently seen.
Acute rupture of the biceps tendon occurs as a result of forceful contraction of the biceps muscle or forceful movement of the arm with the biceps contracted. The injury may be avulsion of the tendon from the muscle belly anywhere along its course or be pulled free from its glenoid attachment. It is often a crippling problem and usually accompanied by tenosynovitis.
Signs and Symptoms. An acute tendon tear is often felt by the patient as a "snap", followed by swelling, tenderness, and ecchymosis over the bicipital groove and bulging of the biceps near the antecubital fossa at the lower half of the humerus. Pain is usually felt on the anterior shoulder about 2 inches below the humeral head at the site of the thecal tunnel. If the long head is torn, the contracted muscle belly moves distally and bulges even if the short head is intact. This is an important sign in differentiating a proximal biceps problem from other shoulder problems. A hollow in the upper humeral area can usually be both seen and felt. Flexion and supination, especially against resistance, increases the bulging at the lower half of the upper arm. Strength of forearm supination is decreased.
Yergason's Stability Test. The seated patient flexes the elbow, pronates the forearm, and attempts elbow flexion, forearm supination, and humeral external rotation against the resistance of the examiner. The doctor stabilizes the patient's elbow with one hand while offering resistance to the patient's distal forearm with his other hand during the maneuver (Fig. 10.16). Severe pain in the shoulder during this test is usually a positive indication of a bicipital tendon lesion, a tear of the transverse humeral ligament, or bicipital tendinitis.
Loose-Tendon Syndrome. In some chronic bicipital disorders, the tendon may appear slack and actually glide from side to side on palpation during repeated adduction and external rotation. To further evaluate, place the patient's affected forearm on your knee. Palpate the bicipital groove with one hand while the other hand moves the patient's elbow laterally and anterior while the patient resists the movement. If the tendon is slack, it will be felt to "jump" during the motion. Injury to the transverse humeral ligament is often involved.
BICIPITAL TENDON DISLOCATION
A bicipital tendon may be found to be dislocated or at least partially subluxated from its groove and express symptoms. This is due to rupture or loosening of the transverse ligament which holds the tendon of the long head within the bicipital groove. The mechanism of injury is usually heavy lifting, "Indian" arm wrestling, or a slip while carrying a heavy object. Injury occurs, especially in young adults, when the contracted biceps meets an overload.
Signs and Symptoms. A subluxated tendon will be felt and/or heard to snap as the patient forward flexes and abducts his arm, then returns it to its natural position. The patient is unable to place the ipsilateral hand on the sacrum. As time passes, motion restrictions indicate cuff degeneration. Yergason's and Abbott-Saunders' tests are positive. Extreme tenderness will be found at the superior aspect of the bicipital groove, with some tenderness along the groove distally. A slack tendon will be found on palpation of the upper groove as the humerus is abducted and internally rotated. A "jumping" sensation from the tendon is felt if the transverse ligament is partially torn. A gliding sensation is felt if the ligament is completely torn.
Abbott-Saunders Test. This is a modification of Yergason's test that forces the biceps tendon against the lesser tuberosity which will stress an instable tendon. Bring the arm of the seated patient into full abduction, rotate it externally, and then lower the arm to the patient's side. A "click" felt or heard, frequently accompanied by pain and a reproduction of symptoms, is a positive sign of subluxation or dislocation of the biceps tendon.
ROTATOR CUFF STRAINS
Five deep muscles lying around the glenohumeral joint comprise the rotator cuff. The infraspinatus and teres minor work as external rotators of the humerus. The subscapularis and teres major rotate the humerus medially. The supraspinatus pulls the humerus into the glenoid fossa and abducts the humerus initially (10– 15°) before the deltoid becomes effective. In further abduction, the supraspinatus stabilizes the humerus as the deltoid, during full abduction, tends to displace the humerus from the glenoid. The mechanism of injury may be a fall on an outstretched hand, a blow on the shoulder, throwing, or heavy lifting.
The Role of the Rotator Cuff. The intrinsic rotators of the shoulder are active during abduction and external rotation. When the horizontal arm is loaded to produce anterior dislocation of the humerus, the subscapularis has proved to be the primary muscle responsible for preventing displacement. The supraspinatus, infraspinatus, and teres minor contract to stabilize the head of the humerus in the glenoid fossa. If the horizontal arm is also extended backward about 30° and loaded so that the complete rotator cuff is at full contraction, the anterior shear force is about quadrupled. Because the shallow glenoid fossa offers almost no protection, this force must be counteracted by the capsule and associated ligaments to prevent anterior displacement.
Force Couples. The upward pull on the humerus by the supraspinatus and deltoid must be counterbalanced by the weight of the arm and the oblique, somewhat downward, pull of the subscapularis and teres minor. If these forces are not balanced, the humerus will not be stabilized in the glenoid fossa. These force couples explain why rotator cuff tears seriously impair the initial 20– 30° of humeral abduction, when the supraspinatus tendon is active but the deltoid has yet to become fully active.
When the arm is hanging loosely at the side, the slope of the glenoid fossa, the horizontal pull of the supraspinatus, and the tightening of the superior aspect of the joint capsule prevent downward subluxation of the humerus even without the aid of the deltoid. The plane of the glenoid fossa and the weight of the individual's arm (plus added weight) determine the necessary force of the supraspinatus and joint capsule to prevent inferior subluxation of the humeral head.
Signs and Symptoms. On examination, the patient's arm is held to the side and cannot be abducted and externally rotated actively without pain; however, nearly a full range of passive movement can be obtained with care. The arc of pain is generally located between 45°and 90° as the tuberosity of the humerus passes under the acromion process. Pain may also be noticed during adduction from 120° to 170° with subacromial crepitus, varying amounts of weakness, and recurrent "bursitis" episodes. When the patient is asked to raise his arm, the shoulder hunches in support, a short motion may be made, but the arm quickly collapses to the side in pain. While passive motions of the shoulder are unrestricted, pain may be felt when the humeral head presses under the acromial arch. When the shoulder is extended, the front and back of the humerus will be tender but not as acute as at the greater tubercle. Extreme tenderness is found where the cuff inserts into the tuberosities. A superior subluxation of the humerus is often associated. Pain is increased when active internal rotation is resisted.
Arm Drop Test. Hold the patient's arm horizontally at 90° abduction and then ask him to hold that position without assistance. If this cannot be done actively for a few moments without pain, it is a positive indication of a torn rotator cuff. In lesser tears, the patient may be able to hold the abduction (a slight tap on the forearm will make it drop) and slowly lower it to his side, but the motion will not be smooth.
Subacute Cases. Tenderness will be found over the lesser tuberosity. An important sign in 1-2 weeks after injury is an area of thinning or depression at the fossae of the supraspinatous and infraspinatus (especially) muscles. If this is the site of rupture, a "catch" and clicking sound may be felt and heard at the site during passive movements if swelling is minimal.
Stages. Three stages of trauma are commonly recognized and can often be related to age:(1) Edema and hemorrhage resulting from overuse, characteristically seen in the young before 25 years but may be seen at any age.
(2) With repeated episodes, the subacromial bursa becomes fibrotic and thickened. The patient is usually 25– 40 years old.
(3) This stage is characterized by wearing of bone and rupture of the tendon in individuals over 40 years, associated with anterior acromial erosion and spurs. However, as Nelson points out, these stages fail to recognize the effect of a reflex-produced ischemia so often seen in practice.Supraspinatus Ruptures. A supraspinatus tear is characterized by a dull ache on rest which is aggravated by initial abduction. It is usually sited in the rotator cuff or common tendinous insertion rather than within the tendon itself. Complete ruptures are rare in comparison to partial tears. The tendon of the supraspinatus may be the site of paratendinitis or ectopic calcification.
The degree of injury is determined by the degree of pain or weakness on passive motion or active motion against resistance. Differentiation must be made from bicipital tenosynovitis by a positive Yergason's sign and severe pain on palpation. Roentgenographs are usually negative; but in chronic cases, the anterior edge of the acromion may show spur formation or a displaced fracture of the tuberosity.
DELTOID STRAINS
This powerful abductor is a frequent site of acute and chronic disability. Injury may be from intrinsic forces; eg, powerful contraction of the deltoid has been known to fracture its attachment from the clavicle or humerus. Anterior, middle, or posterior deltoid strain can be associated with acute subdeltoid bursitis, but the clinical picture is quite different.
Anterior Deltoid Strain. This strain is often seen following a posteriorly directed force on a horizontally extended arm. Symptoms arise slowly, often peaking 6– 8 hours after injury. Pain and weakness increase on forward abduction. Evidence of swelling and tenderness appear in the anterior third of the muscle.
Middle Deltoid Strain. This strain follows forceful abduction against resistance in the lateral plane. Symptoms arise slowly. Pain and weakness increase on lateral abduction. Evidence of swelling and tenderness appear in the middle third of the muscle.
Posterior Deltoid Strain. This strain is the result of a posteriorly directed strain. Symptoms arise slowly. Pain and weakness increase on posterior abduction. Evidence of swelling and tenderness appear in the posterior third of the muscle.
BRACHIALIS STRAIN
In sprain of the proximal radioulnar joint, there is often a related injury to the brachialis anticus muscle with contracture, or, especially in children, a strip of periosteum may be torn from the anterior aspect of the humerus, followed by callus formation and blocked joint motion. The athlete or manual laborer may present a highly developed muscle belly on the anterolateral aspect of the upper arm which is easily found between the deltoid and the lateral head of the triceps.
Subluxations of the Shoulder
Most shoulder subluxations are not acute, exhibit little or no swelling, but they usually present chronic (often episodic) pain, movement stiffness or "blocks," and other signs of local tissue fibrosis and joint "gluing." Mild to moderate local muscle weakness and possible atrophy are characteristic. Postural distortions of the lower cervical and upper dorsal spine and musculoskeletal abnormalities of some aspect of the shoulder girdle are invariably related.
Shoulder subluxations may be primary conditions after injury, or they may occur weeks or months after reduction of a primary dislocation. Thus, in cases of chronic shoulder pain, the history should be probed for possible shoulder dislocation with spontaneous reduction.
During articular correction of a shoulder subluxation, dynamic thrusts should be reserved for nonacute, fixated situations. When subluxation accompanies an acute sprain, attempts at correction should be more in line with gentle traction pressures after the musculature has been relaxed. Obviously, the probability of fracture fragments, osteoporosis, abscess, etc, must be eliminated prior to any form of manipulation.
ORTHOPEDIC SUBLUXATION OF THE HUMERAL HEAD
This acute condition is probably a dislocation that has partially reduced itself spontaneously. It usually occurs when the greater tuberosity has been displaced upward as a whole to lie between the humeral head and the glenoid. The capital part is rotated to a degree but has not completely escaped from its capsular envelope. The outer border of the shaft is impacted firmly into the cancellous tissue of the head of the humerus.
SUPERIOR HUMERUS SUBLUXATION
Because of its bony arch, the humerus cannot dislocate much superiorly unless there is severe traction involved. However, several authorities believe that superior subluxation can often be demonstrated on bilateral roentgenography. Schultz feels this is the most common shoulder subluxation seen. This writer, however, believes the term to be a misnomer as the suprahumeral joint is not an articulation in the true sense of the word but is solely a structure that serves as a protective and supportive mechanism. Most likely what is referred to as a superior humeral subluxation is the result of contractures within the superior humeral area that prevent the greater tuberosity from gliding smoothly under the coracoacromial ligament during abduction. The result is chronic compression and irritation of the enclosed tissues. Keep in mind that the acromioclavicular meniscus progressively thins with age. It is quite thick in the young but may be completely gone by the 5th or 6th decade.
ANTERIOR HUMERUS SUBLUXATION
This is a frequent type of shoulder subluxation where the mechanism of injury is that similar to anterior humeral dislocation. There is difficulty in raising the arm overhead. Fullness will be noted on the upper anterior arm that will be tender on palpation. The deltoid will feel taut and stringy. A sensitive coracoid process will be found higher than the head of the humerus. Signs of acute or chronic sprain will be found depending upon the history. Check the infraspinatus, teres minor, and rhomboid major muscles for possible strain.
POSTERIOR HUMERUS SUBLUXATION
The physical signs of this infrequently seen disorder are usually negative, and bilateral roentgenography is required for confirmation. In a few cases, the posterior area may feel fuller than the unaffected side. An unusually prominent coracoid process may be felt, and a slight hollow may be felt above the humerus. Signs of taut tissues on the posterior aspect of the humeral head and lax tissues on the anterior aspect are often found. Evaluate the integrity of the pectoralis major muscle.
INFERIOR HUMERUS SUBLUXATION
A slight hollowness may be found at the joint space, indicating that the humeral head has dropped from its normal position. The deltoid will often feel firm and stringy, indicating a chronic disorder. Evaluate the integrity of the supraspinatus, long head of the triceps, deltoid, coracobrachialis, and clavicular division of the pectoralis major. Signs are often vague and should be confirmed by bilateral roentgenography.
Dislocations of the Shoulder
Most dislocations are anterior dislocations of the glenohumeral joint (85%), followed by acromioclavicular dislocations (10%), sternoclavicular dislocations (3%), and posterior dislocations (2%). True dislocations must be differentiated from pseudo-subluxations where the humerus is displaced inferiorly by hemarthrosis. Poor muscle tone is usually related. The typical mechanism is an extension force against an abducted arm that is externally rotated.
The glenoid cavity covers only a small part of the head of the humerus. In extreme degrees of abduction, extension, and flexion, any force transmitted through the humeral shaft is applied obliquely to the body surface and directly on the capsule of the joint, through which the head of the bone is then forced. In fracture dislocations, the humeral fracture is invariably displaced with the articular surface outside the joint.
The primary stabilizers of the shoulder under passive loading are the abductors, the glenohumeral capsule, and ligament complex of the shoulder joint. The subscapularis and capsule provide the major dynamic stability anteriorly during external rotation. Once these tissues are torn, stretched, or weakened, less force is necessary for subsequent dislocations. If this is the case, surgical shortening of the subscapularis may be necessary.
CLINICAL TESTS
Apprehension Test. If chronic shoulder dislocation is suspected, slowly and gently abduct and externally rotate the patient's arm with the elbow flexed toward a point where the shoulder might easily dislocate. If shoulder dislocation exists, the patient will become quite apprehensive, symptoms may be reproduced, and the maneuver is resisted as further motion is attempted.
Dugas' Test. The patient places his hand on his opposite shoulder and attempts to touch his chest wall with his elbow and then raise his elbow to chin level. If it is impossible to touch the chest with the elbow or to raise the elbow to chin level, it is a positive sign of a dislocated shoulder (Fig. 10.17).
VARIETIES
Symptoms may be severe in primary dislocation, even if the soft tissues and capsule are not greatly damaged. Heroic reductions from misguided compassion should be avoided.
Four types of dislocations may be classified according to the direction in which the humeral head leaves the socket, and these can be subclassed according to the point at which the head of the humerus comes to rest or according to limb position: anterior, inferior, posterior, or superior displacement.
Anterior Dislocations. Subcoracoid (common), intracoracoid, and subclavicular types may be found. The typical mechanism involves a combination of abduction, extension, and external rotation of the shoulder. The common means are: (1) A fall on the outstretched arm where the trauma drives the humeral head forward against the anterior capsule. (2) Abduction with the humerus in internal rotation or forward flexion where the humerus in external rotation becomes limited by the acromial arch. If forceful elevation is applied when this point of impingement is reached, the arch is used as a fulcrum to dislocate the proximal head anterior and inferior. (3) A fall or blow to the lateral shoulder from the rear.
In subcoracoid luxation, the head of the humerus lies under the coracoid process – either in contact with it or at a finger's breadth distance at most below it. The humeral head may be displaced inward until three-fourths of its diameter lies to the medial side of the process or be simply balanced on the anterior edge of the glenoid fossa. The humeral axis passes to the medial side of the fossa. The elbow hangs away from the side, the lateral deltoid bulge is flat, the acromion is prominent, and the glenoid cavity is empty. Palpation reveals the absence of the usual bony resistance below the lateral aspect of the acromion and the presence of abnormal resistance below the coracoid process or in the axilla. Active movement is lost, and passive abduction is strongly resisted by the patient. Dugas' test is positive. The arm can be passively adducted but not to the degree that the elbow can touch the chest with the fingers resting on the opposite shoulder. Measurement in abduction shows shortening.
In intracoracoid dislocations, the humeral head is displaced further medially. The symptoms and signs are those of the subcoracoid type except that the head of the humerus is felt further displaced and the shoulder is more flattened. The arm may be fixed in horizontal abduction. Severe capsule laceration is usually involved which allows for the greater displacement.
Complications of Anterior Dislocations. When the humerus dislocates anteriorly, its posterolateral margin is often forced against the rim of the glenoid to produce a compression fracture (Hill-Sachs deformity). The malpositioned humerus frequently tears the cartilaginous labrum and capsule from the glenoid rim (Bankhart's lesion) with an avulsed fragment of bone. If the anatomical neck has fractured, the humeral head will not participate in passive movement of the shaft. Crepitus can usually be felt. Fracture of the greater tuberosity, tears of the rotator cuff, and recurrent dislocation are common complications. Anterior fracture dislocations are usually related with displacement of the greater tuberosity, but the capsule is not displaced. Any anterior luxation can do great harm to the brachial artery, vein, or nerves. Circulation must always be checked before reduction is attempted.
Inferior Dislocations. Subglenoid and luxatio erecta types are infrequently seen in which the humeral head lies below the glenoid fossa. The common cause is forcible abduction followed by rotation or impulsion. The mechanism of injury is usually a leverage force on an abducted arm such as in an arm tackle. There is severe pain and disability. The arm is fixed at about 45° in abduction. A hollowness will be found at the joint space, with the humeral head inferior to its normal position and often palpable within the axilla. The deltoid is flattened and extremely spastic. In subglenoid luxation, the symptoms are those of subcoracoid flattening, but abduction and flattening of the shoulder are more marked. The upper part of the greater tuberosity is usually torn. In the rare instances of luxatio erecta, forcible elevation of the arm causes the head of the humerus to be displaced far downward so that the arm becomes locked in a vertically erect position.
Posterior Dislocations. This is often a diagnostic challenge in the young well-muscled individual because all joint motions may be unrestricted, yet disability is acute. Two types are seen which differ only in the extent of displacement; ie, subacromial and subspinous types. The cause is direct pressure lateral and posterior, or pressure has been exerted in the same direction along a flexed, adducted, and internally rotated humerus. It is sometimes produced during a convulsive attack. The patient's arm is abducted and rotated internally, and the elbow is directed slightly forward. The shoulder is flat in front and full behind, where the head of the humerus may be felt. The coracoid is prominent. The head of the humerus lies on the outer edge of the glenoid fossa or further posterior under the scapular spine or on the infraspinatus. These features are not as obvious as those of anterior dislocation. Passive abduction and external rotation motions are restricted. In severe cases, the lateral side of the capsule is usually torn. There may be an associated cuff tear or an avulsion fracture of the greater tuberosity resulting in persistent pain. The internal and external scapular muscles are usually lacerated or contain fragments of the torn tuberosities.
Superior Dislocations. A supraglenoid luxation is very rare except in rough sports or accidents with unusual force mechanisms. A routine A-P x-ray view may show narrowing of the space between the head of the humerus and the acromion, indicating a tear. Referral for arthrography may be necessary. Take care not to confuse the growth plate of the proximal humerus with that of a fracture line.
ROENTGENOGRAPHIC CONSIDERATIONS
Careful evaluation of the glenohumeral articulation is necessary to judge alignment congruity. In approximately 20% of cases of shoulder dislocation, fractures of the glenoid are associated. Lesser tuberosity fractures are often related to a posterior dislocation of the shoulder. Vigorous contractions of the triceps muscle, as seen in throwing excesses, may produce avulsion injuries to the inferior aspect of the glenoid.
Fractures of the Humerus
Fractures of the proximal humerus are not common. They are usually seen in mature women with a degree of osteoporosis. The mechanism is often a fall on the outstretched pronated upper extremity. About 85% of these fractures are of the simple type, usually involving the surgical neck and greater tuberosity of the humerus. A scapula fracture may be associated. In most cases, early mobilization, without compromising long-term effects, is beneficial.
Roentgenographic Considerations. Fragments are usually displaced less than 1 cm, are angulated less than 45°, and are held in place by an intact rotator cuff and periosteum. Displacement of the greater tuberosity of more than 1 cm indicates a torn rotator cuff. Fractures through the surgical neck, frequently associated with brachial plexus injuries, are usually displaced anteriorly and medially due to the pull of the pectoralis major. Fractures through the head or anatomic neck of the humerus are rare. When present, they have a high incidence of avascular necrosis. In the area of the subacromial or subdeltoid bursae, calcification may simulate a fracture of the greater tuberosity. A calcification shadow appears more dense and irregular than that of bone and is not trabeculated.
As with the elbow joint, the epiphyseal lines in the shoulder make interpretation difficult unless contralateral views are taken. The epiphysis for the lateral end of the acromion process does not unite until about 20 years of age. In the young, the upper humeral epiphysis may be damaged from excessive throwing ("Little League shoulder").
Injuries of the Scapular Area
Chronic shoulder girdle pain and discomfort are often seen in people who work overhead with repetitive motions for long durations with little postural change. Trigger points will inevitably be found along the vertebral borders of one or both scapulae. Most authorities feel the cause can usually be traced to muscular overuse leading to lower cervical or upper thoracic subluxations. Subluxations may be found in the shoulder girdle itself, especially when the scapulae are chronically affected. Acute or chronic fibrositis of the trapezius and rhomboids with trigger points is often superimposed or inconsequential.
ACUTE TRAPEZIUS STRAINS
Most trapezius injuries will be seen at the proximal portion, rarely distal to the scapular spine. That aspect between the occiput and the shoulder is the only significant muscle that can resist forceful shoulder depression.
FIBROSITIS
Fibrositis is a generalized term which refers to a syndrome featuring spasm, stiffness through the range of motion without limitation, a dull gnawing ache at rest which is aggravated by exercise, localized tenderness, possible soft-tissue crepitus, and one or more palpable trigger points. Strains and associated fibrositis are often seen in the musculature attachments to the vertebral border of the scapula from throwing heavy objects. The initial trauma may not be remembered.
The disorder is most often seen in the rhomboids and trapezius (Fig. 10.18). However, the levator scapulae, scalene group, or erector spinae are often involved. Fibrofatty nodules herniate through the superficial fascia of the involved muscles. Palpation and movements may cause pain to radiate up the posterior neck and/or over the shoulder and sometimes down the arm. Cervical motions cause a vague soreness in the affected tissues. This is usually worse in the morning after arising and during cold, damp weather.
SCAPULAR FIXATIONS
Restricted movements are commonly found in the scapular area. They affect both performance and posture. Their usual causes are (1) the consequence of injury, (2) trigger-point spasm, or (3) viscerosomatic reflexes. The local source of the difficulty may be local, at the spine, or at the shoulder. The common sites to search are a costovertebral or upper dorsal subluxation, or contraction of any muscle that has a scapular attachment such as the rhomboids, trapezius, levator scapulae, supraspinatus, infraspinatus, and/or teres major and minor muscles.
SCAPULAR FRACTURES
Scapular fractures are not frequently seen, but in severe trauma, fractures of the scapular body and spine can occur. Strong muscular attachments usually prevent significant displacement. All that is usually required in therapy is rest in a sling until acute pain subsides, then early mobilization. Infrequently, the brachial plexus or axillary nerve may be injured. Fractures of the scapular neck (uncommon) are usually impacted and present little displacement. Acromion fractures are the result of a downward blow on the shoulder, often leading to avulsion of the brachial plexus roots. Fractures of the coracoid process, easily confused with an ununited epiphysis, are uncommon. When they occur, they are usually associated with acromioclavicular separations.
Injuries of the Clavicle
At the acromioclavicular and sternoclavicular joints, a wide range of injury and displacement may occur. The tip of the shoulder, near the lateral aspect of the clavicle, is a common site of extremely painful and tender contusions to the trapezius. Localized swelling is easily seen and palpable. The patient will depress the entire shoulder girdle in an attempt at relief. Care must be taken not to confuse this contusion with acromioclavicular separation.
ACROMIOCLAVICULAR SPRAIN
The acromioclavicular joint is relatively weak and inflexible, yet must bear constant stress in contact sports. Those who expose the joint to excessive and repeated trauma risk contusion, sprain, and separation. Posttraumatic arthritis is a typical consequence. Any force which tends to spring the clavicle from its attachments to the scapula is bound to cause severe sprain to the acromioclavicular, coronoid, and trapezoid ligaments unless the clavicle fractures beforehand. Keep in mind that the acromioclavicular ligament can be considered a part of the acromioclavicular joint capsule, thus severe sprain must involve a degree of capsule tear.
Major sprain consists of a degree of severe stretching and tearing of the tough coracoclavicular ligaments. Carefully palpate for evidence of conoid or trapezoid sprain. Acute tenderness and possible swelling will be found in the area of the coracoclavicular ligament below the clavicle. There is distinct abnormal mobility of the clavicle relative to the acromion process. After a week or more, a subcutaneous discoloration may appear. An aftermath of an old injury may be exhibited by laxity of the acromioclavicular joint without localized tenderness.
ACROMIOCLAVICULAR SEPARATION
The acromioclavicular joint serves as a roof for the head of the humerus. It is one of the weakest joints of the body but assisted by the strong coracoclavicular ligament. The ends of the joint are bound loosely so the scapula can raise the glenoid fossa. During shoulder injury, the scapula often rotates around the coracoid which acts as a fulcrum. The intrinsically weak superior and inferior acromioclavicular ligaments give way and the joint dislocates. In other instances, a downward force of great intensity lowers the clavicle onto the 1st rib which acts as a fulcrum, tearing the acromioclavicular and coracoacromial ligaments, resulting in complete acromioclavicular separation. Continued force can fracture the clavicle. Incomplete luxation can tear the intra-articular meniscus and lead to degenerative arthritis of the joint.
Initial Evaluation. Sternoclavicular sprains vary from minor to complete dislocation, either posteriorly (retrosternal) or anterior-inferior to overlap the 1st rib. In any acute separation, the most significant sign is that of demonstrable and significant false motion of the acromioclavicular joint from joint laxity. If examination of the seated patient can be made before swelling develops, good evaluation can be made by pivoting the joint after the scapula has been stabilized by the nonpalpating hand. The swollen joint may give a false impression of a tender but stable joint.
Schultz's Test. Standing behind the sitting patient, face the affected side. Place one hand under the flexed elbow and push up while the other hand placed over the acromioclavicular joint applies firm pressure. The more "give" that is felt in the joint, the greater the separation.
Chronic Cases. Signs of posttraumatic arthritis may appear such as pain over the shoulder region with little or no radiation to the arm, tenderness over the acromioclavicular joint, and pain-free movement until the scapula begins to move. Shrugging the shoulders usually elicits pain.
The proximal ulna forms the most important articulation in the elbow, while the distal radius forms the most important articulation in the wrist.
Flexion and Extension. The excursion of the head of the radius over the capitulum in full flexion is about 140°. Active flexion is judged by having the patient touch an ipsilateral shoulder with the supinated hand, and extension is checked by the patient straightening the elbow as far as possible. Some females normally reach 5° of hyperextension. The easiest testing maneuver is to have the patient flex and extend both elbows at the same time in one continuous movement. Flexion is limited normally by the biceps muscle mass, and extension is limited when the olecranon touches the olecranon fossa.
Flexion. Elbow flexion is controlled by the brachialis (C5-C6) and biceps brachii (C5-C6) with assistance offered by the brachioradialis (C5-C6) and supinator (C6). See Tables 10.4 and 10.5. Strength is tested with the examiner in front of the patient. Place your stabilizing hand cupped under the patient's 90° flexed elbow and your active hand gripping the patient's wrist. Add increasing resistance as the patient attempts to flex the elbow.
THE COSTOCLAVICULAR SYNDROME
This syndrome is due to the neurovascular bundle being compressed between the 1st rib and the clavicle at the point where the brachial plexus joins the subclavian artery and courses over the first rib. Symptoms are similar to those of the scalenus anticus syndrome and reproduced by the costoclavicular maneuver.
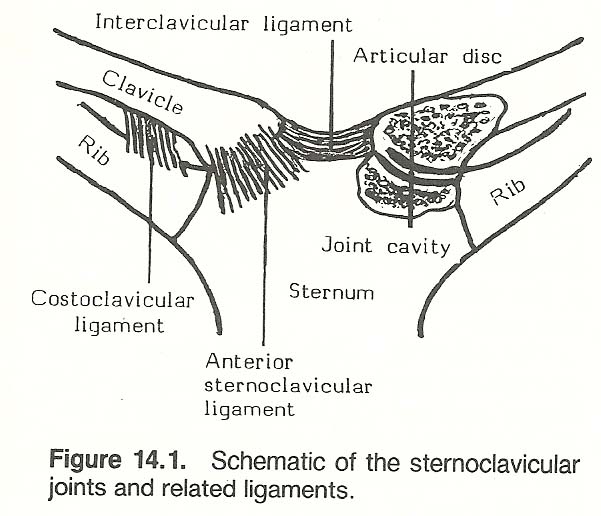
STERNOCLAVICULAR DISC INJURY
In some injuries to this joint that are just below the severity of a dislocation, the articular disc may be pulled from its sternal attachment in a manner similar to a semilunar tear of the knee. The patient will complain of localized pain on movement. A "catch" may be felt by the patient, especially during ipsilateral shoulder flexion and circumduction. As in the knee if the cartilage is fragmented, referral for surgery may be required if conservative measures fail.
Subluxations of the Clavicle
During correction of a subluxation, even mild dynamic thrusts should be reserved for nonacute, fixated situations. When subluxation accompanies an acute sprain, correction should be more in line with gentle traction pressures after the musculature has been relaxed. Obviously, the probability of fracture fragments, infection, osteoporosis, etc, must be eliminated prior to any form of manipulation.
ANTERIOR MEDIAL CLAVICULAR SUBLUXATION
The typical mechanism of force is one of a posterolateral impact which drives the shoulder anterior and medial. If sternoclavicular subluxation does not occur in the young, a green-stick midshaft fracture often results. Acute disability ensues, and sometimes false joint motion can be palpated. Pain is acute and aggravated by joint motion. There is severe tenderness at the sternoclavicular joint. Secondary capsule injury may be expressed by intracapsular swelling, edema, and generalized tenderness. Exhibited crepitus suggests attending fracture fragments or articular comminution, thus making adjusting procedures contraindicated.
Evaluate the integrity of the pectoralis major and subclavius muscles. In older cases, a degree of fixation will inevitably be present. This is easily determined by placing two finger pads upon the sternoclavicular joint and widely circumducting the patient's abducted arm.
CLAVICULAR FIXATIONS
Gillet feels that clavicular fixations, especially at the sternal joint, are frequently related to readily palpable fixated ligamentous and muscular tissues in the C7-T1 area that extend laterally from the spine. Immobility at either the medial or lateral joint of the clavicle can be easily determined by placing a thumb firmly upon the joint and moving the patient's shoulder back and forth in an A-P direction. Then cup the patient's ipsilateral elbow with your stabilizing hand and move the shoulder in a superior-inferior direction.
Dislocations of the Clavicle
Clavicular dislocations are common but not as frequently seen as clavicular fractures. Analysis of complications should be made by roentgenography prior to considered reduction.
ACROMIOCLAVICULAR DISLOCATION
In injuries of the lateral clavicle, the clavicle is usually elevated, which increases the distance between the clavicle and the coracoid process. Thus, a distinct palpable and visible "step" will be noted in the supraspinatus region. If the prominent lateral clavicle is depressed, it will spring back to its elevated position once pressure is released. The scapula falls away from the clavicle, and the acromion lies below and anterior to the clavicle. Fracture of the coracoid process is often associated.
In roentgenography, Dalinka states that an increase of the coracoclavicular distance by 5 mm or greater than 50% of the contralateral side indicates a true acromioclavicular dislocation. Complete dislocation cannot occur unless the conoid and trapezoid ligaments are severely torn. The soft tissues within this area frequently ossify after injury. After chronic injury, signs of erosion or tapering may be observed, along with indications of soft-tissue calcification subsequent to an old hematoma.
ANTERIOR STERNOCLAVICULAR DISLOCATION
The sternoclavicular joint is the least stable major joint of the body, although complete dislocations are rare. Shoulder girdle movement at the sternoclavicular joint is slight but essential. At the medial end of the clavicle, displacement may occur either anterior, as is more common, or posterior in relation to the sternum. The latter is often associated with dyspnea and cervical edema from vasculature compression. When dislocations occur and are reduced, a deformity often persists. The displacement of the clavicle in anterior dislocation is typically anterior, superior, and medial.
POSTERIOR STERNOCLAVICULAR DISLOCATION
These luxations are often hidden by soft-tissue swelling. In chronic cases, a distinct depression is palpable. Acute posterior dislocations can be a medical emergency requiring the attention of a thoracic surgeon. Pure dislocations should be reduced by a specialist because of possible weakening of the vital tissues behind the sternum.
Fractures of the Clavicle
Fractured ends sometimes can be felt under the skin. The involved shoulder may be lower than the other, and the patient is unable to raise the involved arm above the shoulder. Characteristically, the patient will support the elbow of the involved side with the contralateral palm.
The most common site of clavicular fracture is near the midpoint, but both ends also deserve careful evaluation. In midshaft fracture, there is sometimes inferior, anterior, and medial displacement of the lateral section. Fractures of the inner third are uncommon and often represent an epiphyseal injury as the medial clavicular epiphysis does not close until about the age of 25 years. Most fractures (66%) of the outer third of the clavicle present intact ligaments with no significant displacement. About 30% of outer-third fractures present detached ligaments medially and attached ligaments distally, with displacement inferior and medial on the trapezius muscle. Early active shoulder movements should be encouraged.
If this injury is due to a fall on an outstretched hand, the impact is transferred from the palm to the carpals, to the radius and ulnar, to the elbow and humerus, to the scapula and clavicle, and to the spine and thoracic cage (Fig. 10.19). Thus, all structures involved in the line of impact deserve careful evaluation, not just the immediate area of obvious fracture.
The Elbow and Forearm
Basic Functional Anatomy
The arm and forearm are joined by a trochoginglymus joint – a hinge and a pivot. The semilunar notch of the ulna is hinged with the hyperboloid trochlea of the humerus. The proximal head of the radius pivots with the spherical capitulum of the humerus and also glides against both the proximal and distal ends of the ulna. Because the distal humerus curves slightly forward, its articulating surface faces somewhat posteriorly. This places the forearm in slight flexion in its resting position, which increases the mechanical advantage of the flexor muscles.
The distal aspect of the humerus presents an articular surface that is cylindrical and smooth except for about 35° of its circumference. The distal end of the humerus can be viewed as two columns, a larger one medial (trochlea) that articulates with the semilunar notch of the ulna and a smaller one lateral that articulates with the head of the radius. The pulley-like trochlea apparatus has (1) a depression at the front that lodges the coronoid process of the ulna and (2) a depression at the rear that holds the olecranon process of the ulna when the elbow is extended. The olecranon process restricts hypertension of the elbow and protects the ulnohumeral articulation posteriorly. The concave head of the radius glides against the spherical capitulum of the humerus. The capitulum and trochlea are separated by a bony crest that fits into the opening between the proximal ulna and the radius and serves as a fixed rudder to guide elbow motion. The elbow flexors originate from the medial epicondyle, and the extensors originate from the lateral epicondyle.
Elbow and Radioulnar Movements
The basic range of elbow joint motion involves elbow flexion (135°) and extension (0°), and forearm supination (90°) and pronation (90°). The patient may be examined in either the standing or sitting position. If a blockage is obtained in active motion, passive motion should be checked and the type of block and degree of restriction noted.
During extension, the elbow functions as a first-class lever. The mechanical advantage is poor because of the short lever arm between the insertion of the triceps and the center of the joint. During flexion, the elbow functions as a third-class lever. Force from the biceps and brachialis act between the fulcrum and weight of the forearm.
ELBOW MOTION
Pronation and Supination. During forearm pronation, the ulna remains fixed and the radius crosses over it. In supination, the bones merely uncross. Active pronation and supination is checked with the patient's elbow 90° in flexion and firmed against the waist. The patient is then instructed to turn the closed fist first downwards to that the palmar surface is parallel with the floor (pronation) and then upward so that the dorsal surface is parallel with the floor (supination). Restriction in pronation suggests pathology at the elbow, radioulnar articulation at the wrist, or within the forearm; restriction in supination is associated with a disorder of the elbow or radioulnar articulation at the wrist.
KINESIOLOGY OF THE ELBOW
Extension. Extension of the elbow is provided by the triceps (C7-C8)) with help from the anconeus (C7-C8). The examiner's stabilizing and active hands are in the same position, and increasing resistance is offered as the patient attempts elbow extension.
Supination. Forearm supination is conducted by the biceps (C5-C6) and supinator (C6), which are aided by the brachioradialis (C5-C6). The examiner's stabilizing hand remains cupped under the elbow, and the active hand grips the patient's pronated wrist. Increasing resistance is applied as the patient attempts to turn the forearm from pronation to supination.
Pronation. Pronation of the forearm is provided by the pronator teres (C6-C7) and pronator quadratus (C8-T1), with assistance from the flexor carpi radialis (C7-C8). The examiner's stabilizing hand remains in place as above, and the active hand grips the patient's supinated wrist. Increasing resistance is applied as the patient attempts to turn the forearm from supination to pronation.
Table 10.4. Elbow and Forearm Motion
| Joint Motion | Prime Movers | Accessories |
| ELBOW | ||
| Flexion | Brachialis Brachioradialis | Flexor carpi radialis Flexor digitorum superficialis Pronator teres Extensor carpi radialis longus Palmaris longus |
| Extension | Triceps | Anconeus |
| FOREARM | ||
| Supination | Supinator Biceps brachii | |
| Pronation | Pronator teres Pronator quadratus | |
| Muscle | Major Function | Spinal Segment |
| Anconeus | Extension | |
| Biceps brachii | Flexion, supination | |
| Brachialis | Flexion | |
| Brachioradialis | Flexion, supination | |
| Extensor carpi ulnaris | Extension | |
| Flexor carpi radialis | Flexion | |
| Flexor carpi ulnaris | Flexion | |
| Palmaris longus | Flexion | |
| Pronator quadratus | Pronation | |
| Pronator teres | Pronation, flexion | |
| Supinator | Supination, flexion | |
| Triceps | Extension (long head) |
GONIOMETRY OF THE ELBOW
Restricted Flexion or Extension Motion of the Elbow. Place the supine patient in the neutral position, center the goniometer next to the elbow, and record the neutral reading with the goniometer arm along the axis of the forearm. Note any extension loss, and record the deviation from the neutral. Then have the patient flex the arm, and record the end of the motion.
Restricted Rotation Motion of the Elbow. Place the patient in the neutral supine position. The goniometer is not used to evaluate rotation. Have the patient supinate and pronate the forearm, then record each estimated arc at the end of the motions.
Most forearm injuries are the result of direct blows or falls. Commonly seen are avulsion-type injuries of the elbow as a result of acute or chronic strain at a site of tendon or ligament attachment (Fig. 10.21).
(1) axial compression forces throughout the limb;
Hyperextension Sprain. Hyperextension sprains strongly mimic posterior dislocation of the elbow. Swelling and tenderness will be found at the joint capsule posteriorly, bicipital tendon, olecranon fossa, lateral and medial collateral ligaments, and attachments of the flexors at the medial condyle. Pain is relieved by flexion and increased on attempted extension. If the joint proper is involved, extension is chiefly limited, and it may persist for weeks or years.
Cozen's Test. With the patient's forearm stabilized, instruct him to make a fist and extend his wrist. Grip the elbow with your stabilizing hand and grip the top of the patient's fist with your active hand and attempt to force the wrist into flexion against resistance (Fig. 10.25). A sign of tennis elbow is a severe sudden pain at the lateral epicondyle area.
Anterior Olecranon Subluxation. Subluxation of the olecranon anteriorly is seen in relation to hyperextension sprains and restricted posterior olecranon motion.
The carpals articulate with the ulna only during extreme wrist abduction. The distal radius enlarges to form the seat of the articulation of the proximal row of carpals.
Trigger Points
The most common trigger points in the forearm are those of the supinator, the extensor carpi radialis, and the extensor of the middle finger. These are shown in Figure 10.20.
Selected Clinical Problems of the Elbow and Forearm
Roentgenographic Considerations
As a consequence of avulsion injury, bone fragments may be seen in the area of the epicondyles or olecranon process, and epicondyle spurs may point to chronic stress.
THE SOFT TISSUES
Displacement of fat pads is often found at the elbow after injury. It can occur in any injury that distends the joint capsule. A pad appears as a thin strip of radiolucent fat density. The anterior fat pad is normally seen on lateral views, but the posterior humeral pad is hidden by the epicondyles' posterior extensions. However, as Bowerman points out, the posterior pad will become visible at the posterior edge of the humerus on lateral views if effusion causes displacement of the pad. The most important complication is ischemia of the forearm, which may cause an irreversible contracture deformity.
GROWTH CENTERS
Normal ossification of distal humeral epiphyses is not an even process, especially during the periods of rapid growth and development; thus knowledge of secondary ossification centers of the elbow is necessary in dealing with children or teenagers. One or more bony centers may remain uneven in density and irregular on the margins, especially the trochlea and olecranon epiphyses. Because of this irregularity, careful differentiation must be made from osteochondrosis and epiphysitis. The trochlear center is irregularly mineralized and always develops from several small foci. The lateral epicondyle does not fuse directly with the humerus as the medial epicondyle does; rather, it fuses first with the neighboring epiphyseal ossification center, the capitellum, then the fused mass joins the end of the shaft of the humerus. After injury, the position of various centers must be evaluated for possible displacement and incarceration into the joint.
Elbow Strains
There may be an injury to the upper radioulnar articulation by sudden overpronation or oversupination followed by pain over the articulation with limitation of rotation (Fig. 10.22). Trigger points are commonly found just below the horizontal midline of the antecubital fossa over the proximal radius and ulna. When the joint proper is involved, motion is limited chiefly in extension and may persist indefinitely. An associated injury to the brachialis anticus muscle with contracture is common. In children, a strip of periosteum may be torn from the anterior humerus, followed by bone formation and blocked joint motion. Local myositis ossificans may also develop in the tendon of the brachialis anticus. Some cases will be complicated by ulnar neurapraxia.
Strains of the bicipital attachment to the ulna are not common. They occur in elbow hyperextension injuries. The course of the tendon will be tender on palpation. Management consists of rest in a sling for a few days along with standard sprain therapy.
Elbow Sprains
Articular or extra-articular injuries to the elbow without fracture are not uncommon and are peculiarly resistant to treatment. There may be a primary or secondary injury to the upper radioulnar articulation by sudden overpronation or oversupination, followed by pain over the articulation and limited rotation. Overlooking radial-head dislocation is a common orthopedic error.
Forced joint movement beyond full extension, abduction, or adduction causes ruptures within the capsular apparatus and its reinforcing ligaments from their attachment to the humerus, radius, and ulna. The capsule is tender and frequently distended with blood. Movement in the direction of injury aggravates the pain, and there is some restriction at extreme ranges.
TRAUMA IN EXTENSION
The proximal forearm, elbow joint, and distal humerus are frequently injured when the mechanism of trauma is a fall on the outstretched hand (Fig. 10.23). When the elbow is extended, the upper extremity acts as a mechanical brace that transmits force from the point of hand contact to the torso. The axial compression combined with a bending moment to sharply dorsiflex the wrist produces a force couple that compresses the wrist dorsally and stretches the ventral soft tissues. If a portion of this strut is weakened by age, for instance, where bone is weaker than the involved ligaments and tendons, this weakness will determine the type of injury. It is for this reason that falls on the outstretched hand usually involve the wrist of the elderly and the distal humerus of the young.
When a fall is made on the outstretched hand, several mechanisms are effected:
(2) bending moments at
the wrist, elbow, and shoulder joints;
(3) torsion about the long axis of the limb; and
(4) violent lateral flexion of the cervical spine. The moment of axial loading (impact force X lever arm) must be resisted by the elbow tissues to prevent failure. If the elbow holds, the force not absorbed is transmitted to the shoulder.
COMMON TYPES OF ELBOW SPRAIN
Hyperabduction Sprain. Tenderness is found below the lateral epicondyle, indicating sprain of the ulnar collateral ligament. Pain is increased by forcing the elbow into valgus stress.
Hyperadduction Sprain. Tenderness is exhibited below the medial epicondyle, indicating sprain of the radial collateral ligament. Pain is increased by forcing the elbow into varus stress.
LIGAMENTOUS STABILITY TEST
To roughly judge the stability of the medial and lateral collateral ligaments of the elbow, hold the patient's wrist with one hand and cup your stabilizing hand under the patient's distal humerus. As the patient is directed to slightly flex his elbow, (1) push medially with your active hand and laterally with your stabilizing hand, then (2) push laterally with your active hand and medially with your stabilizing hand. With the fingers of your stabilizing hand, note any joint gapping felt during either the valgus or varus stress maneuver (Fig. 10.24).
Tennis Elbow
"Tennis elbow" is a painful condition of traumatic origins not limited to tennis that occurs about the external epicondyle of the humerus. The term incorporates a group of conditions, especially epicondylitis or radiohumeral bursitis. It is caused by repeated violent elbow extension combined with sharp twisting supination or pronation of the wrist against resistance. The result is severe contraction of the extensor-supinator muscles of the forearm.
The clinical picture is one of synovitis, subperiosteal hematoma, fibrositis, or partial rupture of the fibrous origin of muscles and ligaments at the affected epicondyle, with some associated periostitis. Radial nerve entrapment may be involved. If the medial epicondyle is sore, the flexor-pronator muscles and medial ligaments are involved. The lateral epicondyle area is affected seven times more often than the medial epicondyle.
ROENTGENOGRAPHIC CONSIDERATIONS
The x-ray features in the elbow may include soft-tissue calcification at the margin of the lateral joint, lateral epicondyle and capitellum erosion and fragmentation, and spur development at the coronoid process of the ulna. A medial slope deformity of the lateral condyle of the humerus is frequently related. Strenuous unilateral use of the active upper extremity (eg, tennis) often leads to hypertrophy of muscle and bone in the forearm and hands as compared to the nondominant side. Increased radial length and width is frequently found.
TYPICAL PHYSICAL SIGNS
Hasemeir describes the typical symptomatic picture as pain over the outer or inner side of the elbow, distal to the affected epicondyle. Pain may be severe and radiate when the patient extends his arm. The pain is usually sharp and lancinating on exertion, but it may be dull, aching, and constant. Squeezing an object with the fingertips is usually painful (writer's cramp). Tenderness, heat, and swelling are found over the affected epicondyle, and limited passive movement on extension may be found. This syndrome is the result of microscopic and macroscopic tears at the common origin of the extensor and flexor muscle groups – occurring as a consequence to overstress of tendon fibers. The supinator has its tendinous origin just behind the common extensor tendon. Grip strength as well as supination and pronation strength are affected.
TESTS
The easiest and surest test is to have the patient put forward his relaxed limb (flexed about 30°) and attempt supination against resistance. Moderate finger-pressure resistance will produce sharp pain at the lateral epicondyle.
Mills' Test. The patient makes a fist; flexes the forearm, wrist, and fingers; pronates the forearm, and then attempts to extend the forearm against the examiner's resistance. This stretches the extensors and supinators attached to the lateral epicondyle. Pain at the elbow during this maneuver is an indication of radiohumeral epicondylitis.
Olecranon Bursitis
Smooth mobility of the elbow is provided by this fluid-filled bursa, which is exposed to injury when the elbow is fixed on a firm surface. It is subject to direct impact and indirect mechanisms that may cause chronic inflammation, thickening of synovium, and formation of excessive fluid. The mechanism of injury is usually one of repetitive direct injury, constant friction of extensor tendons as in tennis elbow, and/or repetitious local injuries with synovial irritation. Local pain, tenderness, swelling, and movement restrictions are exhibited. Secondary infection readily converts the inflammation into an abscess.
Subluxations of the Elbow
Most subluxations in the elbow area will offer dramatic relief upon correction. Generally, the adjustment is made with a quick, short thrust to minimize the pain (and time) of relocation. It is essential that the patient's muscles be relaxed or correction will be inhibited and extremely painful. Naturally, quick thrusts are contraindicated in arthritic and advanced fibrotic conditions.
POSTERIOR-MEDIAL RADIAL HEAD SUBLUXATION
This "pulled elbow" injury results when the radial head is jerked from the annular ligament. Pain and tenderness in the area of the radial head result. Motion is severely limited in pronation and supination, but flexion and extension are normal. The arm is held in a pronated position, and pain is fairly localized at the elbow. X-ray films are negative. This type subluxation is commonly associated with tennis elbow or wrist trauma, lateral elbow pain, and restricted anterolateral radial-head motion.
OLECRANON SUBLUXATIONS
Posterior Olecranon Subluxation. This type of subluxation is associated with elbow or wrist trauma, epicondyle and bursa tenderness, triceps dyskinesia, and restricted anterior olecranon movement.
Medial Olecranon Subluxation. Subluxation of the olecranon medially is often seen in association with ulna nerve paresthesias, wrist or elbow trauma, medial elbow pain, triceps dyskinesia, decreased distance between olecranon and medial epicondyle, and restricted lateral olecranon joint motion.
Lateral Olecranon Subluxation. This type of subluxation is related to elbow or wrist trauma, lateral elbow pain, triceps dyskinesia, decreased distance between olecranon and lateral epicondyle, and restricted medial olecranon motion.
SUPERIOR ULNA SUBLUXATION
Subluxation of the ulna superiorly is usually related to elbow or wrist trauma – often a consequence of a falling person catching himself with an outstretched hand. This results in the ulna being jammed upward towards the shoulder.
Fractures and Dislocations of the Elbow Area
Fractures in the area of the elbow frequently involve the joint. In the order of frequency, the most common fractures are supracondylar humeral, olecranon, radial head, and coronoid process. Olecranon fractures result from a fall on the elbow or excessive triceps action. Displacement may be severe because of the strong pull of the triceps. Olecranon stress fractures are usually seen after overuse throwing injuries.
The radial head at the elbow transmits the force of a fall on the hand to the shoulder; this explains why the radial head is a common site of fracture in the elbow area. Subtle impaction fractures of the distal humerus and radial head are common, but they are often not witnessed on x-ray films until after a week or two. Acute signs are local swelling, tenderness about the radial head, and severe pain increased on pronation or supination. Severe displacement is not typical.
PHYSICAL ASSESSMENT
If obvious deformity and crepitus are not present, check the range of motion, and determine the radial pulse. Assess sensation by light touch and distal motion function by having the patient appose his thumb and forefinger. Elbow fractures and dislocations should be reduced by an orthopedist. Splint in the "as is" position, sling, and refer immediately. Delay in referral can easily result in massive heterotopic bone formation.
Myositis ossificans, nerve damage, brachial arterial compression, contractures, abnormal carrying angle, and joint stiffness may complicate recovery from any severe elbow injury. Poorly reduced supracondylar fractures, resulting in cubitus valgus, readily lead to ulnar neuritis.
ROENTGENOGRAPHIC CONSIDERATIONS
Elbow dislocations are usually the result of excessive hyperextension where the olecranon and radial head are displaced posteriorly. Severe soft-tissue damage is associated, usually resulting in subperiosteal hematoma. Comminuted or marginal fracture fragments from the radial head are frequently related with elbow dislocations. In uncomplicated cases, gentle forward traction on the forearm with the humerus stabilized can be conducted to ease pain prior to referral. Roentgenography is required to analyze possible complications prior to considering even simple dislocation reduction.
Especially in the adolescent, trochlea, capitellum, and epicondyle growth centers may be enlarged, fragmented, displaced, or prematurely fused. Epiphyseal lines cause the most errors in interpretation of this area. Epiphyseal cartilage may be lacerated and the ossification centers displaced, sometimes into the articular cavity.
The most common fracture is a line running from the anterior to the posterior surface of the humeral shaft (supracondylar) with the proximal fragment shifted anteriorly. A fracture line between the condyles (intercondylar) or through one or both of the condyles (diacondylar) may be seen. Fracture of the ulnar shaft with dislocation of the radial head (Monteggia injury) and fracture of the radial head may also be present.
Nerve Compression Injuries
RADIAL NERVE COMPRESSION AT THE ELBOW
This nerve compression syndrome features pain and disturbed sensation in the area of distribution of the superficial branch and is thus frequently confused with De Quervain's disease. If the deep branch is involved, pain is at or below the lateral epicondyle. On palpation, the nerve trunk is tender near the origin of the extensors, and active extension of the fingers initiates or aggravates pain. If the elbow is extended and the 3rd finger is actively extended against resistance, pain is acutely increased because the extensor carpi radialis inserts at the base of the 3rd metacarpal.
ULNAR NERVE COMPRESSION AT THE ELBOW
The ulnar nerve is often injured – just slightly less in incidence than the the radial nerve. The injuries are usually at the inner side of the elbow where it is quite vulnerable in its superficial position along the elbow's posteromedial aspect. After damage, a characteristic "claw hand" results, with sensory loss of the medial side of the hand.
Ulnar nerve compression is often called cubital tunnel syndrome or tardy ulnar nerve palsy. It is the result of trauma or compression of the ulnar nerve at the elbow when the medial ligament ruptures during elbow dislocation. It may also be involved if the medial epicondyle becomes fractured. Disability and pain occur along the ulnar aspect of the forearm and hand. Early signs are inability to separate the fingers and disturbed sensation of the 4th and 5th digits. Interosseous atrophy is usually evident, and light pressure on the cubital tunnel initiates or aggravates pain. Nerve conduction studies help to confirm the diagnosis.
The Wrist
Basic Functional Anatomy
The radial facet is concave and sheathed with a triangular cartilage. The convexity of the transverse proximal carpal surface is sharper than the concavity of the radioulnar surfaces to afford a good range of joint motion. The proximal carpals rock and glide toward the ulnr during wrist abduction and toward the radius during adduction. Adduction is slightly greater in pronation because the styloid process of the ulna restricts motion when the hand is supinated. During adduction, the styloid swings backward out of the way. Because the A-P curve of the proximal carpals is more acute than the transverse curve, greater excursion is allowed in wrist flexion and extension than in lateral motion, but the exact degree of wrist motion varies considerably from patient to patient. It appears that the more delicate the bone structure, the greater the mobility.
The distal row of carpals form a complex joint with the proximal row. Because they are loosely connected, the navicular and trapezium spread during wrist abduction and approximate during adduction. The volar surfaces of the carpals present eminences that serve as attachment points, allowing increased mechanical advantage for the muscles and ligaments of the hand. They also guide tendon passages.
Wrist Movements
The intricate anatomic architecture of the wrist allows flexion (80°), extension (70°), radial deviation (30°), ulnar deviation (20°), supination and pronation of the forearm.
See Tables 10.6 and 10.7.
Table 10.6. Wrist Motion
| Joint Motion | Prime Movers | Accessories |
| Flexion | Flexor carpi radialis Flexor carpi ulnaris | Palmaris longus Flexor digitorum superficialis Flexor digitorum profundus Abductor pollicis longus |
| Extension | Extensor carpi radialis longus Extensor carpi radialis brevis Extensor carpi ulnaris | Extensor digitorum Extensor indicis Extensor digiti minimi Extensor pollicis longus |
| Radial deviation | Flexor carpi radialis Extensor carpi radialis longus | Extensor pollicis longus Extensor pollicis brevis Abductor pollicis longus |
| Ulnar deviation | Extensor carpi ulnaris Flexor carpi ulnaris |
| Muscle | Major Function | Spinal Segment |
| Abductors pollicis | Flexion, radial deviation | |
| Extensor carpi radialis | Extension, radial deviation | |
| Extensor carpi ulnaris | Extension, ulnar deviation | |
| Extensor digiti minimi | Extension | |
| Extensor digitorum | Extension | |
| Extensor indicis | Extension | |
| Extensor pollicis longus | Extension, radial deviation | |
| Extensor pollicis brevis | Radial deviation | |
| Flexor carpi radialis | Flexion, radial deviation | |
| Flexor carpi ulnaris | Flexion, ulnar deviation | |
| Flexor digiti profundus | Flexion | |
| Flexor digiti superficialis | Flexion | |
| Flexor pollicis longus | Flexion | |
| Palmaris longus | Flexion |
WRIST MOTION
Active flexion, extension, ulnar deviation, and radial deviation are tested simply by having the patient flex and extend the wrist, then deviating the wrist medially and laterally (Fig. 10.26). Supination and pronation tests have been discussed previously in conjunction with the forearm.
KINESIOLOGY OF THE WRIST
Flexion. Flexion of the wrist is provided by the flexor carpi radialis (C7-C8) and flexor carpi ulnaris (C8-T1). See Figure 10.27. To judge strength, the patient makes a fist, the examiner stabilizes the wrist, and the patient flexes the closed fist. At the end of flexion, the examiner applies increasing extension resistance to the patient's fist with the active hand.
Extension. Wrist extension is controlled by the extensor carpi radialis longus (C6-C7), extensor carpi radialis brevis (C6-C7), and extensor carpi ulnaris (C7). See Figure 10.28. Strength is tested by having the examiner stabilize the patient's forearm by firmly grasping the patient's wrist with one hand and applying increasing flexion pressure against the dorsum of the patient's hand after motion has reached maximum extension.
Wrist supination and pronation strength has been discussed previously with the forearm.
COUPLED WRIST AND FINGER DYNAMICS
The muscles of the wrist are placed obliquely to the parts to be moved. This requires coordination with other muscles whenever the wrist is moved. Wrist strength in flexion is nearly double that in extension, and the power of extension is greatly lessened when the wrist is flexed. During extreme flexion of the wrist, it is impossible to strongly curl the fingers in full flexion because the flexor tendons are slackened. When the wrist is hyperextended, the extensors become slackened and the fingers cannot fully hyperextend.
GONIOMETRY OF THE WRIST
Restricted Dorsal and Palmar Flexion Motion of the Wrist. Place the patient in the neutral position, center the goniometer under the patient's wrist, and record the neutral reading with the goniometer arm between the patient's ring and middle fingers. Have the patient dorsiflex the wrist as far as possible, and record the reading at the end of the motion. To evaluate palmar flexion, have the patient palmar flex the wrist as far as possible, and record the end of the motion.
Restricted Abduction and Adduction Motion of the Wrist. Place the patient in the neutral position with the hand and forearm pronated, center the goniometer over the wrist with the goniometer arm over the third metacarpal, and record the neutral reading. Have the patient radial deviate the wrist as far as possible, and record the reading at the end of the motion. Then have the patient ulnar deviate the wrist as far as possible, and record the reading at the end of the motion.
Restriction in pronation suggests pathology at the elbow, radioulnar articulation at the wrist, or within the forearm (Fig. 10.29). Restriction in supination is associated with a disorder of the elbow or radioulnar articulation at the wrist. Thickened tissues may cause compression symptoms, and nerve injury is often secondary to epicondylar fracture or severe trauma.
Separated Distal Radius and Ulna. This type of subluxation is commonly seen in association with carpal tunnel syndrome, chronic wrist pain, and after wrist trauma.
Anterior Carpal Subluxation. Subluxation of a carpal anteriorly is related to carpal tunnel syndrome, chronic wrist pain, extension sprain, and restricted posterior wrist flexion. The lunate is commonly involved (Fig. 10.33).
Carpal Tunnel Syndrome. This is a nerve compression syndrome featuring median nerve entrapment at the carpal tunnel resulting in symptoms in the hand and fingers, often extending up the arm to the elbow. The cause may be either an increase of structural volume within the tunnel or any condition that tends to narrow the tunnel. The history will often indicate an old scaphoid fracture, paralunar dislocation, or tendinitis at the wrist. Frequently, the history tells of a fall stopped abruptly by the palm of the hand when the wrist was sharply dorsiflexed or of overstress in people who strongly manipulate their wrists. A syndrome may also be produced by radial or ulnar arterial impairment since they also pass beneath the transverse carpal ligament. Such symptoms may be aggravated by pressure of the sphygmomanometer cuff during blood pressure evaluation.
Signs and Symptoms. Entrapment of the deep branch produces a motor loss exhibited by a weak pinch, weak little finger and thumb abduction, inability to actively flex the metacarpophalangeal joints, and interosseous atrophy. Compression of the superficial branch features burning sensations in the 4th and 5th digits. Palpation of the pisiform-hamate tunnel initiates or aggravates pain. In roentgenography, a hamate fracture or pisiform dislocation may be found in tangential views.
The metacarpal of the thumb conforms to the articular surface of the trapezium. This saddle joint allows a wide range of mobility in all directions so that the pad of the thumb can appose any finger pad. The two sesamoids of the flexor pollicis brevis ride upon two eminences on the volar surface of the 1st metacarpal. These protect the joint between the thumb's 1st metacarpal and proximal phalanx.
Extension. Thumb extension is provided essentially by the extensor pollicis brevis (C7-C8) at the metacarpophalangeal joint and the extensor pollicis longus (C7-C8) at the interphalangeal joint. Test strength by stabilizing the patient's wrist and having the patient extend the thumb as far as possible. Apply increasing flexion resistance and record degree.
Abduction. Thumb abduction is provided by the abductor pollicis longus (C6-C7, radial) and abductor pollicis brevis (C8-T1, median). Strength is tested by stabilizing the patient wrist, especially on the ulnar side. The patient fully abducts the thumb, and, at the end of motion, the examiner increasingly applies reverse pressure (Fig. 10.37).
Restricted Motion of the Interphalangeal Joint of the Thumb. Place the patient's hand in the neutral position, center the goniometer over the dorsum of the interphalangeal joint, and record the neutral position. Have the patient flex the interphalangeal joint as far as possible, then record the end of the motion.
Finger motion is versatile because of the dynamic balance between muscles and tendons that creates an equilibrium of static and dynamic forces. This is an excellent example of viscoelastic forces that resist tendon-unit lengthening. The components involved are the fascia, tendon sheath, perimyseum, joint capsule, and joint inertia. If the viscoelastic forces on the anterior aspect exceed those on the posterior aspect and the extensors relax, for example, the digit will flex.
Flexion. Flexion of the fingers is controlled essentially by the lateral (C7, median) and medial (C8, ulnar) lumbricals for the metacarpophalangeal joint, the flexor digiti superficialis (C7– T1) for the proximal interphalangeal joint, and the flexor digiti profundus (C8-T1) for the distal interphalangeal joint (Fig. 10.39). See Tables 10.10 and 10.11. To test the strength of the flexors as a whole, have the patient tightly flex the fingers with the wrist pronated. The examiner stabilizes the patient's wrist with one hand, and with the active supinated hand curls his fingertips under those of the patient's, then grasps the patient's fingers in the palm, and increasingly applies extension pressure (Fig. 10.40).
Restricted Motion of the Metacarpophalangeal Joint of Any Finger. Place the patient's hand in the neutral position, center the goniometer over the dorsum of metacarpophalangeal joint, then record the neutral reading. Have the patient attempt to make a fist, and record the reading at the end of the motion.
Finger subluxations are often left untreated by the unaware, resulting in long-term disability and, possibly, permanent deformity. Capsulitis and later arthritis are common complications.
Retinacular Test. To distinguish between intrinsic muscle tightness and capsule contractures, let the involved metacarpophalangeal joint flex slightly, relaxing the intrinsics, and move the proximal interphalangeal joint into flexion. Full flexion of the joint shows tight intrinsics; limited flexion indicates probable contracture of the interphalangeal joint capsule. This procedure is often called the Bunnel-Littler Test.
Selected Clinical Problems of the Wrist Area
Trauma of the Wrist Area
Tenderness over the medial collateral ligament as it arises from the medial epicondyle is a sign of valgus sprain. Muscle tenderness in the wrist flexor-extensor group is characteristic of flexor-pronator strain (Fig. 10.30). Tenderness in the first tunnel on the radial side is a common site for stenosing tenosynovitis associated with a positive Finkelstein's sign. Check for rupture of the tendon in the third tunnel, often resulting from a healed Colles' fracture defect at the dorsal radial tubercle or arthritis causing tendon wearing. Tenderness in the 5th or 6th tunnel is characteristic of synovitis, dorsal carpal subluxation, dislocation of the ulnar head, or rheumatoid arthritis. Check the easily fractured scaphoid by sliding it out from under the radial styloid with ulnar deviation of the wrist. Radial deviate the wrist and check the triquetrum, a common site of fracture. Pain, tenderness, and swelling about the ulnar styloid process suggest a Colle's fracture or a local pathology such as arthritic erosion.
FOREARM STRAINS
These usually affect the flexors. Simple strains such as from overenthusiastic weight lifting respond quickly to rest and standard strain management, but chronic strain can develop into a frustrating problem if the patient insists on continuing irritating activities. Avulsion at the bicipital tubercle and stress fracture of the olecranon are sometimes associated.
CONTRACTURES
After cerebral lesions involving the arm center and in almost any spinal or peripheral nerve lesion that involves one set of muscles and spares another, healthy muscles contract (or overact) and permanent deformities result. In trauma-related hysteria, similar contractures occur. Contractures have in themselves little or no diagnostic value but indicate a late and stubborn stage of whatever lesion is present.
BRACHIALIS CALCIFICATION
Following brachialis strain, a local myositis ossificans may develop in the brachialis anticus tendon. This is usually the result of recurrent bruising and bleeding.
UNILATERAL WASTING
Rapid atrophy occurs in all types of neuritis, as well as in poliomyelitis and progressive muscular atrophy. In the latter, it occurs without complete paralysis, though the wasted muscles are, of course, weak. Progressive muscular atrophy usually begins in the muscles at the base of the thumb and between it and the index finger. Less often, the process begins in the deltoid. In either case, the rest of the arm muscles become involved later. In the atrophies just mentioned, a lack of the trophic or nourishing functions that should flow down the nerve is assumed to explain the trophic wasting. From this, we can distinguish atrophy due simply to disuse of the muscles without nerve lesions. Slow atrophy of disuse occurs in the arm in hemiplegia (infantile or adult) and in other cerebral lesions involving the arm center or the fibers leading down from it. A cervical rib disorder occasionally leads to wasting as well as pain in the corresponding arm.
Wrist Sprains and Related Disorders
WRIST SPRAIN
Wrist sprain (eg, a jammed wrist) is quite common and may be associated with fractures and dislocations of the carpals, elbow, or shoulder girdle. Consequently, all severe wrist joint injuries should include roentgenography of the elbow and shoulder. The symptoms of wrist sprain are the same as in any other extremity joint sprain and may be associated with tenosynovitis. Severe wrist sprains are frequently accompanied by carpal and/or radial subluxations (Fig. 10.31).
On the dorsal aspect of the wrist, the scaphoid is the common carpal problem; on the ventral aspect, it is the lunate, hamate, and pisiform. Extension sprain with radial deviation is characterized by tenderness along the ulnar-metacarpal collateral ligament. Dorsiflexion sprain features tenderness along the volar aspect of the wrist and distal radius. In either case, pain is short of fracture and crepitus is absent. Palpation of the anterior wrist is greatly hampered by the tendon bulk of the area and useless on either aspect after swelling has taken place. Keep in mind that scaphoid fracture, a dangerous situation, is often mistaken for a sprain (Fig. 10.32).
TENOSYNOVITIS
The extensor muscles of the forearm are often affected in tenosynovitis. The clinical picture is one of pain along the dorsal forearm, crepitus along the extensor tendons, swelling (palpable and visible), and possible hypertrophy of the extensors and abductors of the thumb.
GANGLION
A ganglion is a cystic swelling occurring in association with a joint or tendon sheath – apparently formed as a defense mechanism when the wrist is repeatedly twisted and strained. It has a fibrous outer coat and an inner synovial layer containing a thick gelatinous fluid. A common site is in the wrist or hand; they are rarely found in the ankle or foot. A firm localized swelling and possibly weakened grip strength are found. Aching or sometimes pain from pressure on adjacent structures is typically exhibited.
Subluxations of the Wrist
As in any adjustive procedure, fracture, dislocation, and pathology must be ruled out prior to adjustment.
DISTAL FOREARM SUBLUXATIONS
Approximated Distal Radius and Ulna. Jamming of the distal radius and ulna are often seen in chronic wrist pain or following wrist and hand trauma.
Inferior Radius Subluxation. An inferiorly subluxated radius is often a consequence of wrist sprain from a fall on the outstretched hand.
COMMON CARPAL SUBLUXATIONS
Posterior Carpal Subluxation. This type of subluxation is frequently associated with wrist trauma, chronic pain upon motion, carpal tunnel syndrome, and restricted wrist extension.
METACARPAL BASE POSTERIOR SUBLUXATION
A metacarpal base subluxated posteriorly is associated with pain especially increased by wrist flexion, excessive wrist flexion sprain, wrist ganglion, and restricted wrist extension.
Fractures and Dislocations of the Wrist Area
Uncomplicated distal-forearm fractures and dislocations should immediately be aided somewhat by steady axial traction. Assess motor and sensory function of the hand, and note circulation by capillary filling of the fingernails with finger pressure. Pad, splint in the position of function, and refer. Roentgenography is required to analyze possible complications prior to considered reduction.
ROENTGENOGRAPHY OF INJURIES AT THE PROXIMAL FOREARM
Fractures of the bones in the forearm usually involve both bones. Sometimes, however, these bones do not fracture at the same level. The bulk of forearm bone injuries are from falls or direct blows. When a midarm blow fractures the radius or ulna, both ends of each bone must be evaluated for possibly associated subluxation, dislocation, and rotational abnormality. Dislocation of the proximal radius accompanies midulna fracture in Monteggia injury, while midradius fracture is accompanied by distal ulnar subluxation in Galeazzi's fracture. The ulna is usually displaced posteriorly when the distal ulna is subluxated. In radial or ulnar fractures, ulnar rotational abnormalities may be a complication. Malposition of the bicipital tubercle proximally and the ulnar styloid distally are helpful clues to rotational abnormalities. Comparison should be made with views of the contralateral (uninjured) arm.
In cases where a fracture of the distal radius is difficult to view on film, careful inspection of the pronator muscle fat pad should be made just proximal to the wrist. It may be the only radiographic sign present. This fat pad, which separates the pronator quadratus muscle and tendons of the flexor digitorum profundus, is normally viewed on lateral films of the wrist. Blurring, bowing, or obliteration of the fat pad may be seen as a consequence of injury or disease of the radius or volar soft tissues.
Fracture of the distal radius (Colles') is the first consideration in wrist injuries, but the close relationship of both forearm and wrist bones and all articulations must be carefully evaluated (Fig. 10.34). The joint spaces between the carpal bones are normally uniform. Epiphyseal fractures and fractures through the growth plate with or without shifting are not uncommon in youth. The typical deformity in this injury is a compression of the posterior margin of the radius, resulting in a backward tilting of the anterior surface as viewed in the lateral view. The articular margin of the radius will be disturbed, and the distal radius may be fragmented and impacted. Old fractures are differentiated from recent ones by the presence of rarefaction and the absence of a distinct fracture line.
On the lateral view, the radiocarpal articulation should be carefully evaluated. The radial longitudinal axis normally extends through the lunate's midpoint. On the P-A view, disruption of the distal radioulnar articulation is seen as joint widening or narrowing. During an impacted fracture of the radius, bone fragments are frequently telescoped and both styloid processes are seen at the same but more distal level; ie, the radial styloid is normally seen 1-cm distal to the ulnar styloid process.
CARPAL FRACTURE-DISLOCATIONS
Any carpal may be a potential fracture or dislocation site. A common predisposing factor to fracture is general osteoporosis. In order of frequency, the bones usually involved are the scaphoid, lunate, and capitate – all of which may be associated with injuries of the radius or ulna. Of the carpals, the lunate is the most frequently dislocated; the scaphoid is the most frequently fractured. The scaphoid is the most lateral of the four bones in the proximal row of carpals; the lunate, second from thumb side.
Even slight tenderness in the anatomic "snuffbox" around the scaphoid and swelling obliterating the space between the thumb's extensor tendons suggest the danger of scaphoid fracture which may not appear on film for 10– 14 days. Axially directed percussion on the knuckle of the patient's index finger when his fist is closed will usually elicit scaphoid pain if it is fractured. Bone necrosis and nonunion are always a danger as the bone is poorly nourished in a third of the population.
LUNATE INJURY
This dislocation-fracture may be seen after a fall on the outstretched hand but is most common in boxers whose hands are carelessly wrapped. Damage to the median nerve is a complication. The clinical picture is one of anterior wrist swelling, with stiff and semiflexed fingers. Carpal dislocations, especially lunate or paralunate, are frequently missed during evaluation. These are often associated with a trans-scaphoid fracture and necrosis.
The lunate usually dislocates posteriorly or anteriorly, disrupting its relationship with the neighboring carpals and the distal radius. Anterior displacement is the common mechanism, where the bone rests deep in the annular ligament and may affect the median nerve. The lunate is loosely stabilized by anterior and posterior ligaments that contain small nutritive blood vessels. A torn ligament thus interferes with the lunate's nutrition, resulting in necrosis. On a P-A view, the lunate's normal quadrilateral shape becomes triangular, and the third metacarpal and capitate usually move proximally. With paralunate dislocation, the lunate keeps normal alignment with the radius but the distal carpals become displaced from their normal position with associated changes in intercarpal joint spaces.
Compression Syndromes
MEDIAN NERVE ENTRAPMENT AT THE WRIST
The median nerve is commonly injured in trauma of the anterior wrist. Consequently, sensation and motion of the fingers should be carefully studied. It is difficult to injure any of the flexors of the medial anterior wrist without damaging the median nerve. When severely bruised, the characteristic "flat hand" deformity results. Median nerve paresthesiae may have their cause in the spine, but they are just as common from interference in the thoracic outlet, the shoulder, the elbow, or at the wrist. Correction must be directed to where the interference is located and not where it should be located.
Signs and Symptoms. There is a history of pain, numbness, and tingling, which worsen at night and with wrist compression, in the first two or three digits and/or the area proximal to the wrist. Weakness is exhibited by a history of dropping light objects and difficulty in holding a pen or pencil while writing. Venous engorgement and a bulge may be seen of the flexor mass in the distal wrist which is characteristic of tenosynovitis or hypertrophied muscles. The first sign is swelling at the volar wrist. Later, thenar atrophy and sensation impairment of the thumb, forefinger, middle finger, and medial half of the ring finger exhibit. In many cases, there is distinct difficulty in pronating or supinating the forearm. Compression or percussion of the carpal ligament usually initiates or increases pain. Electromyogram and nerve conduction studies offer confirmative data for a diagnosis. Misdiagnosis is sometimes made by attributing a unilateral or bilateral syndrome to slight arthritic changes of the midcervical vertebrae.
Phalen's Test. Have the patient place both flexed wrists into opposition and apply slight pressure for 30– 45 seconds (Fig. 10.35). A positive sign of carpal tunnel syndrome is the production of symptoms (eg, pain, tingling).
ULNAR NERVE ENTRAPMENT AT THE WRIST
This compression syndrome features ulnar nerve entrapment, usually in the canal of Guyon. Entrapment may be of the superficial or the deep branch of the ulnar nerve, but the superficial branch is rarely affected by itself. The pisiform-hamate tunnel syndrome is similar to but less frequently seen than that of carpal tunnel syndrome.
Froment's Test. In paralysis of the ulnar nerve, there is an inability to approximate the tips of fingers to the thumb to form a cone (cone sign) or to make an "O" with the thumb and index finger.
The Hand and Thumb
Thumb Movements
The thumb is capable of metacarpophalangeal flexion (50°) and extension (0°) and interphalangeal flexion (90°) and extension (20°). Abduction (70°) and adduction (0°) occur at the carpometacarpal joint.
See Tables 10.8 and 10.9.
THUMB MOTION
Test active overall thumb flexion, extension, abduction and adduction by having the patient touch the tip of his thumb to the base of his little finger, to each fingertip, then extending the thumb as far as possible laterally. If joint restriction is noted, check both joints passively.
KINESIOLOGY OF THE THUMB
Flexion. Flexion of the thumb is controlled by the medial (C8, ulnar) and lateral (C6-C7, median) flexor pollicis brevis at the metacarpophalangeal joint and by the flexor pollicis longus (C8-T1) at the interphalangeal joint. Test strength by having the patient touch the tip of the thumb firmly against the pad below the little finger. Note the power it takes to pull the patient's thumb out of flexion (Fig. 10.36).
Table 10.8. Thumb Motion
Joint Motion Prime Movers Accessories
Metacarpopha- Flexor pollicis brevis Flexor pollicis longus
langeal Abductor pollicis brevis
flexion
Interphalan- Flexor pollicis longus
geal flexion
Metacarpopha- Extensor pollicis brevis Abductor pollicis longus
langeal Extensor pollicis longus
extension
Interphalan- Extensor pollicis longus
geal extension
Adduction Adductor pollicis Flexor pollicis brevis,
deep head
Abduction Abductor pollicis brevis
Abductor pollicis longus
Opposition Opponens pollicis
Opponens digiti minimi
Table 10.9. Major Muscles of the Thumb
Spinal
Muscle Major Function Segment
Abductor pollicis brevis Thumb metacarpophalangeal flexion,
abduction C8-T1
Abductor pollicis longus Thumb abduction and metacarpophalan-
geal extension C6-C7
Adductor pollicis Thumb adduction C8-T1
Extensor pollicis brevis Thumb metacarpophalangeal extension C7-C8
Extensor pollicis longus Thumb metacarpophalangeal and inter-
phalangeal extension C7-C8
Flexor pollicis brevis Thumb adduction, metacarpophalangeal
flexion C8-T1
Flexor pollicis longus Thumb metacarpophalangeal and inter-
phalangeal flexion, abduction C8-T1
Opponens digiti minimi Opposition C8-T1
Opponens pollicis Opposition C6-C7
Note: Spinal innervation varies somewhat in different people. The spinal nerves
listed here are averages and may differ in a particular patient; thus, an
allowance of a segment above and below those listed in most text tables should
be considered.
Adduction. Adduction of the thumb is controlled by the adductor pollicis (C8-T1, ulnar). Strength is tested by stabilizing the patient's wrist along the ulnar border and having the patient adduct the thumb against the examiner's increasing resistance.
GONIOMETRY OF THE THUMB
Restricted Motion of the Carpometacarpal Joint of the Thumb. Place the patient's hand in the neutral position with the goniometer next to the carpometacarpal joint, and record the neutral position reading. Have the patient flex the thumb, then record the reading at the end of the motion. Next, have the patient extend the thumb from the index finger in the palm's plane, and record the reading at the end of the motion.
Trigger Points
The most common trigger point found in the hand is that of the adductor pollicis. This is shown in Figure 10.38.
Dislocation of the Thumb
A fracture of the 4th and/or 5th metacarpal, especially at the neck of the bone, is often referred to as a "fighter's" dislocation-fracture. The bone's head and neck are sometimes pushed into the palm. This is most often seen in the bare-knuckled fighter or during riots rather than with the gloved boxer who more often presents a fracture at the proximal third of the 1st metacarpal.
Selected Clinical Problems of the Hand and Thumb
Direct Trauma
The hand, being the least protected and most active part of the upper extremity, is easily hurt. From a structural standpoint, the hand is made for grasping, not for hitting.
Sprained Thumb
A severe injury can occur to the inner thumb ligaments from a fall on a thumb directed outward or when caught in someone's clothing. This often results in a complete tear which requires surgery. The thumb is also often jammed, and the medial or lateral ligaments sprained, when hitting with the closed fist.
Ulnovolar neuroma (bowler's thumb) is the result of trauma to the digital nerve from the edge of the thumb hole in the ball. After repeated bowling, fibrous proliferation and enlargement of the 3rd and 2nd fingers are frequently seen. Bony callus formation may be evident on roentgenography.
A rupture to the ulnar collateral ligament of the thumb may occur during a fall when the leather loop of a women's purse or at the handle of the ski pole is wrapped around the thumb. Chronic sprain associated with forearm supinator strain is becoming quite common among video game players.
The Fingers
Basic Functional Anatomy
In the fingers, the carpal-metacarpal articulations are fortified by a complex ligamentous apparatus that surrounds the joints in all directions. This tends to greatly restrict carpometacarpal motion. All reciprocally concaveconvex metacarpophalangeal joints are freely movable with the exception of abduction and adduction. The convex metacarpal heads fit snugly against the shallow sockets of the proximal phalanges. The interphalangeal joints are true hinge joints that allow considerable flexion but only slight hyperextension.
Finger Movements
Black/Dumbleton point out that there is a distinct relationship between finger joint position and the position of more proximal joints; ie, joint motion is the effect of involuntary viscoelastic forces in addition to normal active contraction. Active wrist flexion, for example, increases the viscoelastic forces on the posterior of the digit. The result is finger extension even without active contraction of the finger extensors. Likewise, active wrist extension affects finger flexion.
FINGER MOTION
Gross movements of the fingers are regulated by the extrinsic muscles of the hand, while the intrinsics control the finer movements and tend to counterbalance the extrinsics. Finger extension is associated with finger spreading, and flexion tends to draw the fingers together.
Finger motion involves flexion and extension at the metacarpophalangeal and interphalangeal joints. Abduction and adduction occur at the metacarpophalangeal joints. Test active metacarpophalangeal motion by stabilizing the patient's wrist and having him extend (30– 45°) and flex (90°) with the digits straight. Check active proximal interphalangeal motion by stabilizing the metacarpophalangeal joints and having the patient extend (0°) and flex (100°) the proximal interphalangeal joints. Judge active distal interphalangeal movement by stabilizing the proximal interphalangeal joints and having the patient extend (10°) and flex (90°) the distal interphalangeal joints. Inspect finger abduction (20°) and adduction by having the patient place the hand flat and spread the fingers apart and then tight. Note individual joint-motion restriction in all normal directions, and test passively if necessary.
KINESIOLOGY OF THE FINGERS
During contraction of the flexor digiti group, for example, their tendons move proximally, and this exerts a pull on the attached phalanges. The degree of tendon excursion decreases distally with each joint from about 4 cm at the wrist to less than 1 cm at the metacarpophalangeal joint, thus determining the movement of the joint involved.
Extension. Primary finger extension is provided by the extensor digitorum (C6– C8), extensor indicis (C7-C8), and extensor digiti minimi (C8-T1). Strength is tested by stabilizing the wrist in the neutral position, having the patient extend the metacarpophalangeal joints while he or she flexes the proximal interphalangeal joints. The examiner then places the active hand on the back of the patient's proximal phalanges and increasingly applies flexion pressure (Fig. 10.41).
Table 10.10. Finger Motion
Joint Motion Prime Movers Accessories
Metacarpopha- Interossei, dorsal Flexor digitorum profundus
langeal Interossei, volar Flexor digitorum superficialis
flexion Lumbricales
Flexor digiti minimi
Proximal in- Flexor digitorum superficialis Flexor digitorum profundus
terphalangeal
flexion
Distal inter- Flexor digitorum profundus
phalangeal
flexion
Extension Extensor digitorum
Extensor digiti minimi
Extensor indicis
Lumbricales
Interossei, dorsal and volar
Abduction Interossei, dorsal
Abductor digiti minimi
Adduction Interossei, volar
Table 10.11. Major Muscles of the Fingers
Spinal
Muscle Major Function Segment
Abductor digiti minimi Abduction, flexion C8-T1
Dorsal interosse Abduction, flex proximal, extend mid
and distal phalanges C8-T1
Extensor digiti minimi Extension C6-C8
Extensor digitorum Extension C6-C8
Extensor indicis Extension C7-C8
Flexor digiti minimi Flex metacarpophalangeal joint C8-T1
Flexor digiti profundus Flex metacarpophalangeal, proximal, and
distal interphalangeal joints C8-T1
Flexor digiti superficialis Flex metacarpophalangeal and proximal
interphalangeal joints C7-T1
Lumbricales Flex metacarpophalangeal joints, extend
mid and distal phalanges C7-C8
Palmar interossei Adduction, flex proximal, extend mid
and distal phalanges C8-T1
Abduction. Finger abduction is produced by the dorsal interossei (C8-T1) and the abductor digiti minimi (C8-T1). Test strength by having the patient extend and fan the fingers. The examiner, with the thumb and first finger, applies increasing pressure to force any two fingers together being measured.
Adduction. Adduction of the fingers is controlled by the palmar interossei (C8-T1). Test strength by having the patient extend the fingers, keeping them together. Slip a sheet of paper between any two fingers being tested, have the patient apply maximum pressure, and pull out the slip of paper noting resistance.
Bilateral grip strength is best tested with a dynamometer and pinch strength by a pinch meter if objective data records are necessary.
BASIC FINGER MECHANICS
Finger motion is less difficult to appreciate when the proximal bone of the joint is stabilized while the distal bone moves about it. For example, the axis of flexion for an interphalangeal joint is considered to be at that point which does not move in relation to either involved digit.
The digit's flexor tendon lies close to the axis when the finger is extended, but it moves further from the axis during flexion. This creates better mechanical advantage because of the longer moment arm produced. From a biomechanic viewpoint, each tendon is considered to exert tension on the end of a lever whose vector extends from the joint axis perpendicular to the tendon.
Each tendon is held in a sling of fibrous tissue to create a series of pulleys parallel along the finger bones. If these pulleys were absent, the tendons would bowstring between the joints during flexion and fingertip control would be lost. Another important effect of these pulleys is that when the tendon changes direction across a pulley, there is an equal and opposite reaction force at the pulley that establishes a state of equilibrium; ie, the plus and minus factors total zero.
GONIOMETRY OF THE FINGERS
Restricted Motion of the Proximal Interphalangeal Joint of Any Finger. Place the patient's hand in the neutral position, center the goniometer over the dorsum of proximal interphalangeal joint, and record the neutral reading. Have the patient flex the proximal interphalangeal joint as far as possible, and record the reading at the end of the motion for the joint being measured.
Restricted Motion of the Distal Interphalangeal Joint of Any Finger. Place the patient in the neutral position, center the goniometer over the dorsum of the distal interphalangeal joint, and record the neutral reading. Have the patient flex the distal interphalangeal joint of the finger being tested. After flexion is made as far as possible, record the reading.
Trigger Points
The most common area of referred trigger-point pain in the hand is found at the distal 2– 4 metacarpal area. This is shown in Figure 10.42.
Structural Fixations in the Hands
Gillet feels that extraspinal fixations in the hands are second in frequency only to those found in the feet. It has been his experience that these fixations are common in "hand laborers" who must grasp their tools tightly for extended periods. This tends to form a "claw hand" even during rest. If this is the case, extension will be resisted at the involved joints. Gillet reports that release of these fixations, for some unknown reason, appear to have an influence on upper midthoracic fixations, especially in the T4– T6 area.
Selected Clinical Problems of the Fingers
Metacarpophalangeal and Interphalangeal Sprains
The mechanism of metacarpophalangeal injury is one of sudden hyperextension or a severe lateral force. Subluxation, pain, and disability are often severe, and recovery is slow until the involved ligaments tighten to prevent recurring subluxation.
The interphalangeal joints are easily sprained, torn, and dislocated. This is due to their thin capsule, delicate collateral ligaments, and slender articulations. In acute sprain, the ligament tears and allows the bone ends to subluxate and disrupt the integrity of the joint structure. Local pain, tenderness, swelling, and motion restriction are exhibited. A previously torn ligament may predispose a joint to recurring luxation because of laxity of the stabilizers.
Mallet Finger
A hard object may strike a finger resulting in an extensor digitorum tendon injury where the tendon avulses from its insertion at the posterior base of the terminal phalanx. The jammed distal phalanx assumes a position of about 70°. It appears "dropped" and is rigidly flexed with active distal interphalangeal extension severely limited. In such an injury, small bone fragments may be seen at the distal interphalangeal joint's posterior aspect on roentgenography. Both phalangeal fractures and extensor tendon abnormalities may produce mallet finger.
Trigger Finger
This is an entrapment syndrome produced by scar tissue compressing an extensor tendon, often a consequence of de Quervain's disease (Fig. 10.43). Squeezing action by the constricted sheath tends to develop a pea-like mass distal to the thickening. It is most often seen in the thumb, but several fingers are sometimes affected.
Contractures
Hold the metacarpophalangeal joint in slight extension and try to flex the proximal interphalangeal joint of any finger being tested. If the joint cannot be flexed in this position, it is a sign that the intrinsic muscles are tight or capsule contractures exist.
Fractures and Dislocations of the Fingers
All severe hand trauma have a high incidence of metacarpal fractures, but severe displacement is not common.
FINGER FRACTURES
The incidence of metacarpophalangeal thumb joint fracture-dislocation is quite high. A fracture of a proximal phalanx tends to displace anteriorly in an angular fashion because of lumbrical pull. A rotated phalanx, often noted by a finger nail's relationship with its neighbors, is an indication of fracture. Take caution that fracture symptoms mimic severe sprain plus abnormal bone or joint contour. Crepitus is not always exhibited in finger fractures.
FINGER DISLOCATIONS
Many finger dislocations often spontaneously reduce themselves. Dislocation of the proximal interphalangeal joint usually entails severe injury of the collateral ligaments and is likely to heal with an unstable, swollen, stiff joint.
Judge bone length of a suspected fracture or dislocation by comparing it with the uninjured hand. Check for abnormal motion by applying axial and leverage pressure to patient tolerance. Keep in mind that incomplete and impacted fractures may be present, yet associated tendon, nerve, and vascular damage are not common. Comparative x-ray views of the sound limb are frequently helpful.