

Etiology of Foot Hyperpronation:
Embryological PerspectiveThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


Note: This paper is a redaction of an earlier paper published in the
Journal of Bodywork and Movement Therapy Jan 2002
"Medial Column Foot Systems. An innovative tool for improving posture"; 6 (1) : 37-46
Brian A Rothbart, D.P.M., Ph.D., FACFOAbstract:
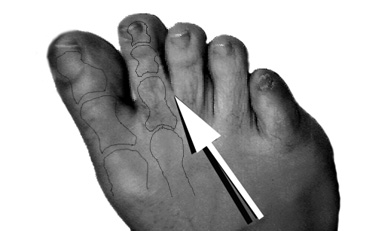
Morton (1935) describes a foot in which the 1st metatarsal is shorter than the 2nd, visually identified as a deep 1st web space (See Figure 1). Rothbart describes a foot in which the 1st metatarsal is elevated and inverted, the Rothbart foot structure {RFS} (Travell 1995, Gilmore 1996, Dols 1997, Svae 2000, GRD BioTech Inc 2000). Both authors are describing the same foot structure. Rothbart (1988) demonstrates that it is this elevated position of the 1st metatarsal that destabilizes {hyperpronates} the walking foot ( See Figure 2). Hyperpronation shifts the posture forward. The body’s center of gravity falls to the inside of the medial {inner} malleolus, the knees hyperextend, the pelvis unlevels producing a functional leg length discrepancy, the shoulder protract {become rounded} and the head moves forward relative to the spine, a process termed BioImplosion. (See Figure 3). (Rothbart McCombs et.al. 1992, Rothbart and Yerratt 1994, Rothbart Hansen et.al. 1995, Schneider 1995, Filner 1996, Liley 1996). The body compensates. Slowly and progressively, strain and deformation patterns develop that lead the patient into chronic pain (Rothbart McCombs et.al.1992, Rothbart and Esterbrook 1988, Rothbart and Yerratt 1994, Rothbart Hansen et.al. 1995, Petersen 1995, Schneider 1995, Filner 1996, Liley 1996).
Travell and Simons (1992) state: "Morton’s foot structure is a major initiator and perpetuator of trigger points". Since Morton’s foot structure and Rothbart’s foot structure are basically the same foot type, one can reasonably deduct that RFS also initiates and perpetuates trigger points.
This monograph discusses the etiology of hyperpronation from an embryological perspective and then introduces an innovative foot system, designed to improve posture, in patients with Morton/Rothbart’s Foot Structure. This foot system (appliance) visually reduces [1] pelvic tilts {levels the pelvis}, [2] shoulder protractions {straightens the shoulders} and [3] forward head positions (in the absence of orthodontic bite reconstruction, moves the head posteriorly over the spine). The drawn forward posture is reversed. And with improved posture, trigger points/chronic pain syndromes are more easily managed or resolved.
Introduction:
Intuitively we know feet affect posture. Structural Engineers use this concept daily: as goes the foundation {foot}, so goes the building {posture}. Rothbart describes the foot-posture relationship dynamically, e.g., the impact Rothbart/Morton’s foot structure has on the walking foot and thus posture. While Morton (1932) asserts that a short 1st metatarsal {relative to the 2nd and 3rd metatarsals} prevents it from fully participating in weight bearing, this is an incomplete explanation of the pathodynamics engaging hyperpronators. Rothbart (2002) asserts an elevated 1st metatarsal head destabilizes the walking foot. Embryologically the foot goes through a series of rotational changes [Streeter 1945, Lash et.al. 1997]. If these rotations end prematurely, the 1st metatarsal and big toe {proximal phalanx and hallux} remain elevated {in elevatus} relative to the lesser metatarsals and phalanges (Straus 1927, Olivier 1962). It is this retained elevatus that forces the walking foot into hyperpronation (Rothbart and Esterbrook 1988, Rothbart and Yerratt 1994, Rothbart Hansen et.al. 1995, Filner 1996, Liley 1996). It is hyperpronation that draws the posture forward (Rothbart McCombs et.al.1992, Rothbart and Yerratt 1994, Rothbart Hansen et.al.1995, Schneider 1995, Filner 1996, Liley 1996). And it is this forward posture and resulting adaptations {compensations} that lead the patient into chronic pain (Rothbart and Esterbrook 1988, Rothbart McCombs et.al.1992, Rothbart and Yerratt 1994, Rothbart Hansen et.al.1995, Petersen 1995, Schneider 1995, Filner 1996, Liley 1996).
Section 1 {Embryology} outlines the normal ontogenetic development within the lower limb bud and the two possible embryological aberrations that can occur in the developing footplate: Clubfoot deformity and Rothbart foot structure. {This paper does not deal with postnatal positional or structural deformations that can occur in the adult foot or leg, e.g., rearfoot varum resulting from massive trauma to the ankle joint, short leg syndrome resulting from trauma to the femoral epiphysis, etc.} Section 2 {RFS. Clinical Significance of PME} discusses RFS impact on posture and provides a methodology for diagnosing RFS in the adult foot. Section 3 {Stablizing RFS} presents an innovative approach in reducing hyperpronation in the standing and gaiting RFS.
- embryology

1.21 Ontogenetic Retention of Talar Supinatus: The Rothbart foot structure.
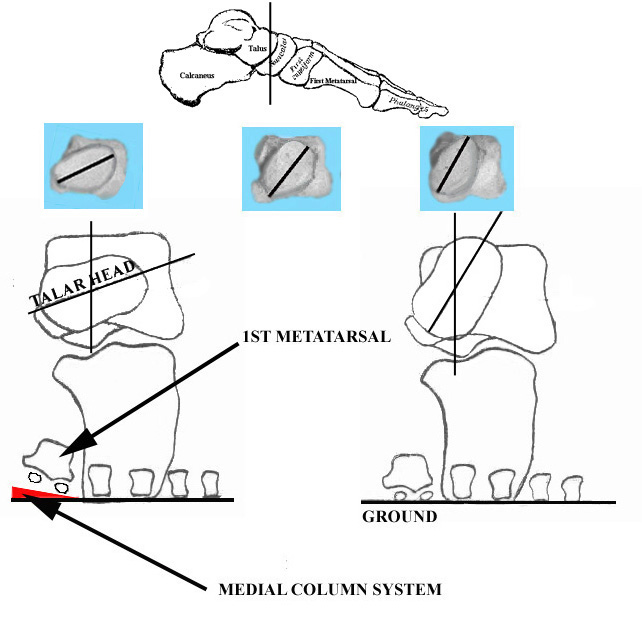
Sewell (1906) examined 1006 Egyptian feet for talar supinatus. He reported angular variances, up to 20ş. If the talar head remains in relative supinatus, the entire medial column of the foot. (See Figure 4). remains in supinatus {structurally twisted inward and upward relative to the calcaneus}. That is, the unwinding of the talar head during fetal development, shapes and contours the navicular, internal cuneiform; which in turn, determines the structural position of the 1st metatarsal/big toe (Sewell 1906, Straus 1927, Streeter 1945 and Olivier 1962). Retention of talar supinatus in the postnatal foot results in a visibly elevated 1st metatarsal/big toe {standing position, subtalar joint neutral}. Rothbart terms the retained structural elevation of the 1st metatarsal and big toe: Primus Metatarsus Elevatus {PME} (Rothbart 2002).
Figure 5) demonstrates the unwinding process of the talar head and its impact on the 1st metatarsal. As the talar head unwinds (see upper photographs, left to right), the elevation of the 1st metatarsal head {PME} is decreased. The lower left diagram illustrates the relationship between PME > 10mm and the 1st metatarsal head (elevated and inverted). The lower right diagram illustrates the relationship between PME < 10mm and the 1st metatarsal head (plantargrade) (US Patent Number 6,092,314 Sheet 3, Figure 4. Adapted and reproduced with permission from GRD BioTech Inc., 2000).
1.22 Ontogenetic Retention of Calcaneal Supinatus: The Clubfoot deformity.
If the calcaneus fails to unwind {remains in supinatus}, the cuboid remains relatively supinated, and with it, the lateral two cuneiforms, lesser four metatarsals and accompanying phalanges (Bohn 1929). The footplate temporally unwinds heel to toe (Streeter 1945, 1948, 1951). Thus retention of calcaneal supinatus is always accompanied by talar supinatus, the Clubfoot deformity {Cfd} (Bohn 1929) (See Figure 6).In the postnatal foot, the calcaneus articulates with the cuboid, which in turn articulates with the navicular, lateral cuneiform and lateral two metatarsals. From a structural point of view, one might deduce that the calcaneus only impacts these structures. From an embryological prospective, this is not the case. Bohn stresses that the ontogenetic unwinding of the calcaneus affects the lateral column of the embryonic foot. That is, the relative structural position of the cuboid, the lateral two cuneiforms and four lateral metatarsals/phalanges are determined by the sculpturing of the calcaneus. Retention of calcaneal supinatus in the postnatal foot is manifested as the Clubfoot deformity.
2. RFS. Clinical Significance of PME
Rothbart’s foot structure is difficult to detect in the newborn’s foot due to the bulging longitudinal fat pad and incomplete ossification of the tarsal bones. At birth, the primary ossification site of the talus has already appeared (Sewell, 1906). However, the onset of ossification of the navicular is variable {2.7 to 4.0 years of age} and late compared to the other tarsal bones (Caffey, 1972; Lang, 1972; Bardeen, 1905; Hoeer, et.al., 1962). The topographical contouring of the inner longitudinal arch {ILA} starts to develop between 12-16 months of age. A definite ILA is present by age 2, By age 30 months, maximal inner longitudinal arching is attained, the apex corresponding to the navicular tuberosity (Blais and Green, 1956). As the ILA takes on its adult contour and the navicular bone ossifies, PME becomes more visible. However, measuring PME in a child less than 4 years of age is prone to error because the navicular bone has not yet ossified.
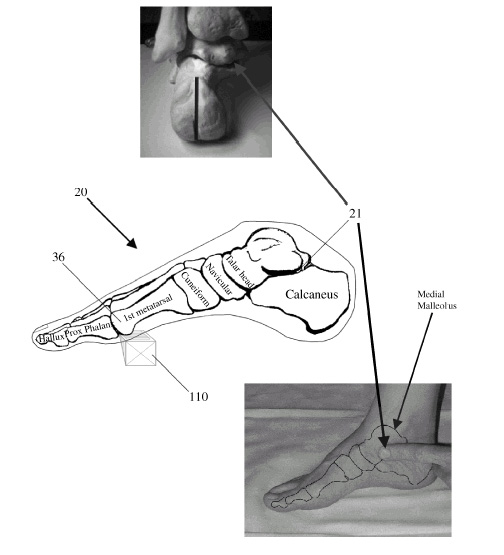
2.1 Measuring PME (See Figure 7).
With the patient standing, locate the talocalcaneal (subtalar) joint (21) as follows: one finger width anterior and below to the medial malleolus (see bottom photograph). Keeping your finger over the subtalar joint space (suscentaculum tali), have your patient transfer 90% of their weight to the other foot. With your free hand, slowly guide the foot through pronation (eversion) – supination (inversion) until the margins of the subtalar joint space feel congruous (parallel) to one another (see top photograph). If the subtalar joint is supinated, the joint space gaps. If the subtalar joint is
pronated, the joint space disappears. Slide the microwedge (110) under the 1st metatarsal head (ball of the foot) until slight resistance is encountered from the bottom of the foot. Record the PME value off of the calibrated microwedge.
In the adult foot {age 4 and over}, PME values between 10mm-25mm are pathognomic of RFS. Zitzlesperger (1960) and Elftman’s (1960) foot models demonstrate an inverse relationship between pronation and arch stability: as pronation increases, the arch deforms (flattens). Clinical data from GRD BioTech (2001) suggest a similar relationship between PME and arch stability: as PME increases, the arch deforms (See Table 1 Below). In this study, 317 patients are divided into 5 separate groups relative to their dynamic arch type (e.g., stable, flexible, flat). PME values are
Table 1 – Correlation Between PME Values and Arch Stability
PME Range Dynamic ILA Contour Description < 10mm Stable Arch Same arch height, sitting or standing 10mm – 20mm Flexible Arch Arch height higher sitting than standing 20mm - 25mm Flexible Flatfeet Arch sitting, No arch standing 30mm – 35mm Functionally Deformed No arch sitting, No arch standing >40mm Structurally Deformed Clubfoot Deformity
then calculated using microwedges (See Figure 7). 96% {306} demonstrate a RFS {PME Values between 10-25mm} with a mean PME of 16mm {Distance {freeway space} between the 1st metatarsal and ground, subtalar joint in neutral {joint congruity} position}. 4% demonstrate a non-RFS. Statistical analysis yielded mean PME values and rate of incidence for each type of arch type (See Table 2 Below).
Table 2 – Clinical Study
Mean PME Value Arch Contour {Walking} # Patients % Patients 06 mm Stable Arch 010 03% 14 mm Flexible Arch 271 85% 24 mm Flexible Flatfeet 035 11% 31 mm Structural Flatfeet 001 <1% TOTAL 317 100%
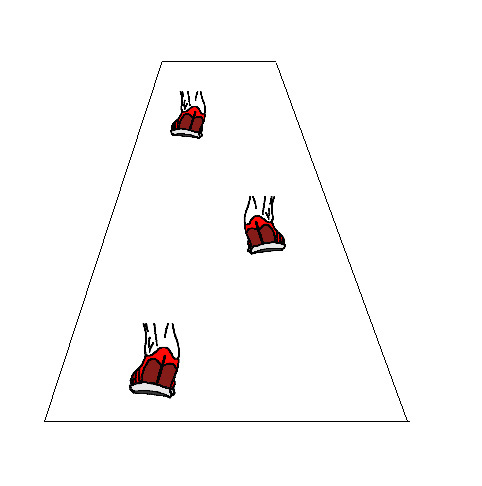
The supinatory ‘strike’, in which the body’s weight is carried on the outside margins of the heel, is a common compensation associated with RFS. Visual inspection of these shoes reveals an excessive wear pattern on the outside margins of the heels. Gait analysis of these apparent ‘supinators’ demonstrates an abrupt outside heel strike and an exaggerated inrolling {hyperpronation} of the foot from midstance to toe off.PME {>10mm} significantly forces the walking foot to roll inward, forward and downward {hyperpronate typically left > right} until the 1st metatarsal reaches the ground (Rothbart and Esterbrook 1988, Rothbart Hansen et.al. 1995, Schneider 1995, Filner 1996, Liley 1996). This shifts the body’s center of gravity forward and downward, which in turn, pulls the innominates forward and downward {typically left > right}. The pelvis is unleveled, resulting in a functional leg length discrepancy {left longer than right}. As these displacements cascade up the axial framework, scoliotic and kyphotic curves are exaggerated, the shoulders protract. The head and upper teeth move forward. This gravity-induced skeletal ‘collapse’ is termed BioImplosion (Rothbart McCombs et.al.1992, Rothbart and Yerratt 1994, Schneider 1995, Petersen, 1995, Filner 1996, Liley 1996), which over time can initiate strain and trigger point patterns, foot to jaw (Rothbart McCombs et.al.1992, Rothbart and Yerratt 1994, Rothbart Hansen et.al. 1995, Schneider 1995, Petersen 1995, Filner 1996, Liley 1996). For example, chronic shoulder protraction can lead to a functional thoracic outlet syndrome.
From clinical observations, hyperpronation appears to be a dominant Mendelian characteristic. This is consistent with the familial diathesis and inordinate rate of expansion in the genetic pool (Garbalosa, et.al., 1994). During the late 1940s, Harris and Beath (1949) looked at 3619 Canadian enlisted men. Their study, evaluating the relative length patterns of the metatarsals, suggests a 40% incidence of Morton’s foot structure {short 1st metatarsal} and associated hyperpronation. A more recent investigation presented at the Annual Conference of the American Academy of Pain Management suggests a significantly greater than 50% incidence of RFS {elevated and inverted 1st metatarsal} and associated late stance hyperpronation (Rothbart 1995).
3. Stabilizing RFS3.1 Heel Wedges and Arch supports. Calcaneal wedging decreases standing hyperpronation. However, calcaneal wedging does not decrease dynamic {gaiting} hyperpronation in feet with RFS. In fact, heel wedging can destabilize the walking RFS, reducing the mechanical efficiency of the foot appliance. Arch supports decrease midstance hyperpronation, but are ineffective as the forefoot engages in weight bearing. Paradoxically, arch supports affect feet like immobilization casts affect muscles: function is improved at the price of muscle strength. In time, these same feet become weaker/more pronated (when barefooted) than they were prior to arch support therapy. For this reason, the author rarely fits any orthosis incorporating an arch support, and now only uses medial column systems in RFS.
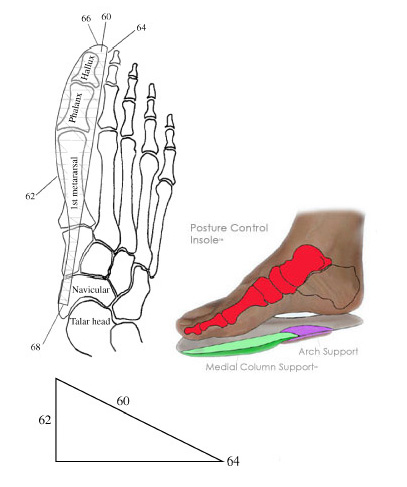
3.2 Medial Column Systems. "Medial column systems effectively reduce dynamic hyperpronation associated with RFS. The effect of these systems extend from the navicular, medial cuneiform, 1st metatarsal bone, to the proximal phalanx and hallux ( See Figure 8). With each step, a tactile feedback loop appears to be triggered which auto corrects the hyperpronation initiated by RFS. The suggested rule of thumb is: 30% tactile = 70% improvement {the 30-70 rule is observational, based on empirical data derived through gait evaluation of 317 patients at the GRD BioTech facility, 1996-1998, and hence not meant to be definitive or all inclusive}. For example, a 6mm medial column system {See Figure 8(62)} under a foot measuring 20mm PME {assuming no significant hypertonicity patterns or cranial deformations} tends to decrease the observable hyperpronation by approximately 70%. Via proprioception, this system provides feedback to the big toe {proximal phalanx and hallux} and 1st metatarsal. All the other weight bearing structures proximal to the big toe and 1st metatarsal {ankle, knee, pelvis, spine, neck, head and jaw} tend to spontaneously correct themselves around this change. The body’s center of gravity shifts posteriorly. The posture is visually more vertical. The inner longitudinal arch is not supported in feet with flexible arches. {Arch supports are used in flatfeet to facilitate the transfer of vector forces across the ILA.} The heel is neither cupped nor wedged." (Rothbart 2002)
"Tactile feedbacks systems are based on the observation that small repetitive stimuli bring about significant changes {e.g., fractal analysis}. Interesting enough, in terms of foot mechanics, this occurs through kinesthetic reposturing. The foot-brain connection recognizes this proprioceptive input as innately correct. The foot is reminded where it should be {not here, but over there} and automatically makes the adjustment. With each step, the foot becomes stronger, the posture straighter. Hyperpronation is reduced. And not surprisingly, as the soft tissue and cranial adaptations are addressed, the tactile input in the medial column system is reduced. An unexpected outcome using foot tactile systems is the observation that trigger points can become disassociated from Morton’s/Rothbart’s foot structure. That is, these trigger points evolve into self-perpetuating loops. Their associated pain referral patterns prove intractable to foot therapy alone. This underscores the importance of concurrent foot and soft tissue therapy when dealing with chronic pain issues." (Rothbart 2002)
"Medial column foot systems {Mcfs} are used as a proprioceptive stimulator. Mcfs are not meant to be used/dimensioned as a supportive foot appliance. Utilizing triangular wedges, mcfs partially diminish the structurally present ‘freeway space’ between the 1st metatarsal/big toe and ground [See Figure 5]. This is an important point to keep in mind. If the mcfs is dimensioned to diminish the entire ‘freeway space’, it becomes a supportive foot appliance. Such devices over a period of time weaken the foot." (Rothbart 2002)
Using a medial column foot system in a non-RFS places a disruptive upward load on the 1st metatarsal head. This can dramatically limit the range of dorsiflexion within the 1st metatarsal-phalangeal articulation and lead to a functional hallux limitus.
Summation:
The foetal development of the lower limb bud, and specifically the footplate, is reviewed. Ontological studies link talar supinatus to RFS and calcaneal/talar supinatus to Clubfoot deformity. RFS and Clubfoot deformity are the two most common ontogenetic deformations seen in the neonatal foot. Progressively and over time, these two structural aberrations orchestrate a predictable postural shift {BioImplosion}. Published studies link BioImplosion to the development of chronic pain syndrome.
PME values between 10-25mm are pathognomonic of Morton/Rothbart foot structure. {Rothbart foot structure is defined as a foot in which the 1st metatarsal is structurally inverted and elevated relative to the lesser metatarsals, the PME values falling between 10mm and 25mm.} As the PME value increases, the distance between the 1st metatarsal/big toe and ground increases. As the distance between the 1st metatarsal/big toe and ground increases, hyperpronation increases {gravity forces the walking foot to roll inward, forward and downward until the 1st metatarsal/big toe rests on the ground}. As hyperpronation increases, Inner Longitudinal Arch {ILA} instability increases. ILA instability is a major biomechanical determinant in the development of postural deformations. From these observations, a very valuable diagnostic tool is devised, the microwedge.
Rearfoot posts and arch supports destabilize and weaken RFS. Rarely are either incorporated into a medial column foot system. Root’s forefoot posts (1971){posting metatarsals one through five in varum} structurally and functionally strain metatarsals II, III and IV in RFS and therefore are counter-indicated {The terms supinatus and varum have been used interchangeable in the literature. By convention, supinatus is used to describe a torsionally inverted relationship in the fetus. Whereas, varum is used to describe the same torsional relationship in the newborn and adult foot.} Measuring forefoot varum across the entire sole of the RFS {metatarsals 1-5} is a misdirected clinical assessment, since talar supinatus only affects the 1st metatarsal.
Clinical studies link high PME values to hyperpronation and hyperpronation to forward postural shifts. Dimensioning medial column systems at 30% of the measured PME tends to decrease dynamic hyperpronation by 70% ± 10%. This in turn reduces pelvic tilts by 50% ± 20%, shoulder protractions by 40% ± 20%. In the absence of any significant psychological or nutritional imbalances, trigger points become significantly more amendable to deactivation as posture becomes more vertical.
References:
Cummins H 1929 The topographic history of the volar pads in human embryo. Contributions Embryology Vol 20:105
Bardeen C R 1905 Studies of the development of the human skeleton. American Journal Anatomy Vol 4:265
Blais MM, Green W T, et.al. 1956 Lengths of the growing foot. Bone Joint Surgery, Vol 38[A]: 998
Bohm M 1929 The embryologic origin of clubfoot. Journal Bone Joint Surgery, Vol 11:2, pp 229
Caffey J P 1972 Pediatric X-Ray Diagnosis. Vol 2:884. 6th Edition, YearBook Medical Publishers, Chicago
Cichoke A J 1999 The Back Pain Bible. Ch. IV, pp 35. Keats Publishing, Chicago
Cummings G 1994-95 Personal communications with Author and on campus visit: Blind study-using microwedges to measure vertical dimensions under patients seen by students. Clinical Director, Department of Physical Therapy, Georgia State University, Atlanta GA
Dols T 1997 Personal Communication with Author, FootTech Inc., Olympia WA
Elftman H 1960 The transverse tarsal joint and its control. Clinical Orthopedics, Vol 16:41
Filner B, et.al. 1995 The relationship of anterior upper torso muscular dysfunction with structural hyperpronation in chronic pain patients. Annual Meeting, American Academy of Pain Management, Dallas September
Filner B 1996 Postural Analysis: Differential Diagnosis. Annual Conference, American Academy of Pain Management, Washington DC
Fusco M A 2000 Textbook & Atlas of Plantar Posturology. 1st ed. Scuderi Editrice, Italy.
Fusco MA Website: http://www.healthmarque.com.au/Prof/BkDetails.html
Garbalosa J C, et.al. 1994 The frontal plane relationship of the forefoot to the rearfoot in an asymptomatic population. JOSPT, Vol 24:4, pps 200-206
Gilmore A 1996 Personal Communication with Author, Capable Spirit Prosthetics and Orthotics, Lakewood WA
GRD BioTech Inc 2001 317 clients evaluated between 1996-1998 using microwedges and visual gait analysis, with and without postural insoles. Seattle WA
GRD BioTech Inc 2000 Foot Support {Medial Column} System and Use in Shoe Lasts. United States Patent Number 6,092,314. Seattle WA, July
Harris R I, Beath T 1949 The short first metatarsal: Its incidence and clinical significance. Journal Bone Joint Surgery [Am] 31:553-565
Hoerr L N, et.al. 1962 Radiographic Atlas of Skeletal Development of the Foot and Ankle – A Standard Reference. Charles C Thomas, Springfield
Lang J et.al. 1972 Praktische Anatomic Erster Band Vierter Teil – Bein und Statik, Pg 31. Berlin, Springer Verlag
Lash J, Alonso L, Benke L, Chang A, Dietrich A and Nathan D 1997 Basic Embryology Review Program: Embryo images. University of Pennsylvania, School of Medicine. Web Home Page: http://www.med.upenn.edu.meded/
Liley P 1996 Postural Analysis: Head guidance and ground support. Annual Conference American Academy Pain Management, Washington DC
Morton D J 1935 The Human Foot. Its evolution, physiology and functional disorders. Columbia University Press, New York
Morton D J 1932 Means for compensating for foot abnormalities. US Patent Number 1,847,973, USPTO, March
O’Rahilly R, Gardner E, et.al. 1956 The ectodermal thickening and ridge in the limbs of staged human embryos. Journal Embryology and Experimental Morphology, Vol 4:256
Olivier G 1962 Formation du Squelette des members. Pgs 145-189. Paris, vigot Freres
Petersen M, et.al. 1995 The relationship of lower leg muscular dysfunction with structural hyperpronation in chronic pain syndrome patients. Posterboard Presentation, Annual Conference, American Academy Pain Management, Dallas
Root M L, Orien W P, Weed J H, Hughes R J (1971) Biomechanical examination of the foot. 1st Ed. Los Angeles: Clinical Biomechanical Corporation
Rothbart B A, McCombs A, Riniker L 1992 BioImplosion. The treatment of chronic pain syndrome. Posterboard Presentation, Annual Conference, American Academy of Pain Management, Albuquerque
Rothbart B A 1995 Postural Kinetics. Annual Conference, American Academy of Pain Management, Dallas
Rothbart B A, Yerratt M 1994 An innovative mechanical approach to treating chronic knee pain: A BioImplosion Model. American Journal Pain Management, Vol 4:3, pps 123-128 July
Rothbart B A, Esterbrook L 1988 Excessive Pronation: a major biomechanical determinant in the development of chondromalacia and pelvic lists. Journal Manipulative Physiologic Therapeutics, Vol 11:5, pp 373-379, October
Rothbart B A, Liley P, Hansen K, Yerratt K 1995 Resolving chronic low back pain: The foot connection. American Journal Pain Management, Vol 5:3, pps 84-89, July
Rothbart B A, Hansen K 1995 Postural Analysis: Definition of terms. Posterboard Presentation. Annual Conference, American Academy Pain Management, Dallas
Rothbart B A 1996 Postural Analysis: The relationship between hyperpronation and Posture. Annual Conference, American Academy Pain Management, Washington DC
Rothbart B A 2002 Medial Column Foot Systems. An innovative tool for improving posture. Journal Bodywork and Movement Therapies, Vol 6:1, pps 37-46.
Svae B 2000 Personal Communication with Author, Postural Dynamics, Seattle WA
Scammon R E, Calkins L A 1929 The development and growth of the external dimensions of the human body in the fetal period. Pgs 245-246. Minneapolis, University of Minnesota Press
Schneider M, et.al. 1995 The importance of controlling hyperpronation with a postural control device in resolving musculoskeletal pain in chronic syndrome patients. Posterboard Presentation, Annual Meeting, American Academy Pain Management, Dallas
Sewell R S 1906 A study of the astragalus {talus}. Part IV. Journal Anatomy Physiology, Vol 40:152
Straus W L 1927 Growth of the human foot and its evolutionary significance. Contributions in Embryology, Vol 19:95
Streeter G L 1920 Weight, sitting height, head size, foot length and menstrual age of the human embryo. Contributions Embryology Vol 11:55, pg 156
Streeter G L 1945, 1948, 1951 Developmental horizons in human embryos. In Contributions to Embryology, Vols 21, 32, 34. Washington DC. Carnegie Institution of Washington
Svae B 2000 Personal Communication with Author, Postural Dynamics Inc., Seattle WA
Travell J G, Simons D G 1992 Myofascial Pain and Dysfunction. The Trigger Point Manual. Vol 2:20, pgs 379-392, Williams and Wilkins, Baltimore
Travell J G 1995 Personal Communication with Author, Washington DC, July and August
Zitzlesperger S 1960 The mechanics of the foot based on the concept of the skeleton as a statically indetermined space framework. Clinical Orthopedics, Vol 16:47-63
Return to ChiroZINE ARTICLES
Since 5-07-2002

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |