

Quality Of Life In Chiropractic Patients With
Low Back And Neck Pain: A 3-Month
Longitudinal Observational StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Contemporary Chiropractic 2026 (Mar 4); 9 (1): 223Ė227 ~ FULL TEXT
OPEN ACCESS Joseph Canillo, Ph.D., D.C. ē John Williams, D.C. ē Luisanna Ciuti, D.C.
Italian Chiropractors Association
https://chiropratica.it/aic/contatti/
Objective To evaluate changes over 3 months in health-related quality of life (HRQoL) in Italian adults with non-specific low back pain (LBP) and/or neck pain (NP) receiving routine chiropractic care, using the SF-36v2 Physical and Mental Component Summary scores.
Methods A longitudinal observational study was conducted in 37 Italian chiropractic practices between December 2023 and December 2024. Adults (≥18 years) with non-specific LBP and/or NP were consecutively recruited at presentation. Patients completed an electronic SF-36v2 questionnaire at baseline and then monthly for 3 months. The primary outcomes were the Physical Component Summary (PCS) and Mental Component Summary (MCS) scores. PreĖand Post-changes from baseline to three months were analyzed using the Wilcoxon signed-rank test for paired non-parametric data. No control group was included, and usual clinical decision-making was not constrained.
Results A total of 163 patients were enrolled. Statistically significant improvements were observed in both PCS and MCS after three months of chiropractic care (p<0.001 for both comparisons). Median PCS increased from 44.7 at baseline to 51.0 at three months, indicating better perceived physical health. Median MCS increased from 41.8 to 46.0, reflecting improved mental health-related quality of life over the same period. Monthly trajectories suggested progressive gains across the follow-up period.
Conclusion In this 3-month longitudinal observational study of 163 adults with low back and/or neck pain receiving chiropractic care in Italian practices, statistically significant improvements in SF-36v2 Physical and Mental Component Summary scores were observed. These findings suggest that chiropractic care may be associated with improved health-related quality of life in patients with spinal musculoskeletal pain.
From the FULL TEXT Article:
Introduction
Musculoskeletal disorders include a wide range of conditions affecting muscles, bones, joints, and connective tissues, and are among the most common health problems worldwide and a leading cause of disability. Low back pain is one of the most prevalent musculoskeletal disorders, affecting about 20% of adults in the United States and Europe, generating substantial economic burden. [1, 2] Chiropractors are healthcare professionals who specialize in the diagnosis and treatment of musculoskeletal disorders, particularly those affecting the spine, using manual manipulation techniques such as spinal adjustments to alleviate pain and improve function. [3, 4] Chronic low back and neck pain are frequent reasons for seeking chiropractic care, yet evidence is limited by a scarcity of large, high-quality randomized trials and the individualized nature of treatment.
Clinical trials investigating chiropractic care for patients experiencing spinal pain primarily focus on quantitative outcomes such as pain scales, ranges of motion, orthopedic tests, and changes in various questionnaires (e.g. Oswestry, Roland-Morris). Patient-reported outcome measures are essential because patients usually provide the best assessment of their own health status, but such data are not routinely collected in chiropractic practice. The Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) and its revision, SF-36v2 were developed as brief, generic self-reported measures usable across a wide range of ages and medical conditions. [5Ė8]
The SF-36v2 provides 8 scale scores and 2 summary scores (Physical Component Summary [PCS] and Mental Component Summary [MCS]) and has demonstrated good reliability and validity, including in populations with spinal disorders. [5Ė9] There is a relative paucity of longitudinal studies in chiropractic settings that employ such broad, generic health-related quality-of-life instruments alongside traditional quantitative clinical outcomes, which motivated the choice of SF-36v2 in this study to monitor changes in both physical and mental health over time.
This study aimed to evaluate changes in health-related quality of life over three months in adult patients with low back and/or neck pain undergoing chiropractic care only in Italian private practices. The primary objective was to assess changes in SF-36v2 PCS and MCS scores from baseline to three months in this observational cohort.
Methods
Ethical Approval and Participating Chiropractors
This research was conducted in 37 Individual Chiropractic Private Practices in Italy and in accordance with the Declaration of Helsinki. The study protocol was approved by the University of Bari, Italy, Research Ethics Board (REB #: 1045). The study was also reviewed and approved by the Italian Chiropractic Association Ethics Committee and Scientific Committee. Thirty-seven licensed Italian chiropractors in private practice participated in the study in their individual practices throughout Italy.
Study Population
One hundred and sixty-three adult patients were divided into 81 adult male and 82 female patients aged 18-65 years old, presenting with neck pain and associated disorders or non-specific low back pain. Patients recruited in the study were patients who presented to individual Chiropractic practitioners in private practice between December 2023 and December 2024. All patients underwent a physical examination to confirm eligibility for chiropractic care and rule out obvious contraindications (spinal metastasis, severe osteoporosis, severe spinal stenosis, severe herniated discs with radiculopathy). Chiropractors informed eligible patients about the study objectives and invited them to participate; written informed consent was obtained from all participants.
Data Collection
An electronic web-based SF-36v2 questionnaire was used to collect data. SF-36 consists of 36 items that are employed to calculate scores on 8 dimensions:Physical Functioning,
Role Limitations due to Physical Health Problems,
Bodily Pain,
General Health,
Vitality,
Social Functioning,
Role Limitations due to Emotional Problems, and
Mental Health. [5Ė8]The PCS and MCS scores are weighted summations of these 8 scales. [8, 9] Higher scores indicate better health status.
Patients completed the first questionnaire before beginning care, and then monthly for 3 consecutive months. The first month was considered acute care, followed by 2 months of maintenance care. An alpha level of p<0.05 was considered statistically significant for all measured variables.
Chiropractic Management
At each visit, patients received a full-spine chiropractic assessment, including sacroiliac joints, to identify dysfunction warranting adjustment. Clinical indicators included joint tenderness or pain on palpation, restricted intersegmental range of motion, asymmetric segmental muscle tension, skin and connective tissue changes. These can includealtered texture (e.g., bogginess),
color changes (redness, paleness),
vasomotor disorders (affecting blood flow),
electro-resistance changes, trophic changes,
tissue thermal variation, and
Derifield-Thompson leg-length inequality.Patients underwent full spine chiropractic adjustments only; no other modalities or physical therapy was used.
Patients were initially seen 1-2 times per week for the first month, then monthly. Chiropractic manual or instrument-assisted adjustments were administered usingdiversified,
Activator,
Thompson,
sacro-occipital technique (SOT),
upper cervical, or
Gonstead techniques,all at the chiropractorís discretion. No physical therapy modalities were used as adjunctive therapy; patients underwent chiropractic adjustments only for the duration of 3 months.
Statistical Analysis
Data were analyzed using R software (version 4.3.1). A non-parametric Wilcoxon signed-rank test was used to compare paired PCS and MCS scores before and after 3 months of chiropractic care. Statistical significance was defined as p<0.05.
Results
.png)
Figure 1
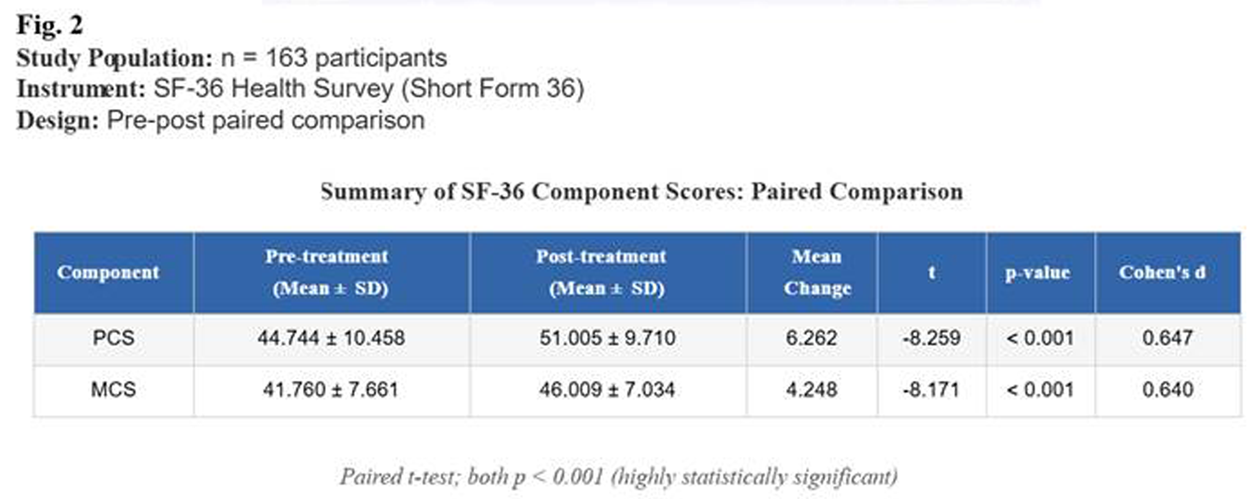
Figure 2 One hundred and sixty-three patients completed all three SF-36v2 questionnaires over the three months. Pre and Post treatment result show improvement in all parameters (Figure 1). The statistical analysis demonstrated highly statistically significant (p<0.001) changes for both physical and mental components. Among participants, the mean PCS score increased from 44.7Ī10.5 at baseline to 51.0Ī9.7 at 3 months. The mean MCS score increased from 41.8Ī7.7 to 46.0Ī7.0 over the same period (Figure 2). Wilcoxon signed-rank tests confirmed that changes in both PCS and MCS were highly significant (p<0.001).
Discussion
In this cohort of Italian adults with non-specific low back and/or neck pain, 3 months of chiropractic care were associated with statistically significant improvements in both physical and mental health-related quality of life. The magnitude of change (approximately 6.3 points for PCS and 4.2 points for MCS) suggests clinically meaningful improvement, although minimally important differences for SF-36v2 can vary by population and condition.
Possible Mechanisms
The improvements observed may relate to changes in pain and disability, mediated by complex biochemical and neurophysiological processes. Pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) contribute to acute and chronic pain and neuropathic hyperalgesia. [10, 11] Anti-inflammatory cytokines such as IL-10 act as inhibitors of pro-inflammatory cytokines and are reduced in chronic diffuse pain. Chiropractic care and spinal manipulative therapy (SMT) have been linked to modulation of inflammatory mediators. [12Ė14]
Other proposed mechanisms include modulation of the endocannabinoid system, which may mediate analgesic and mood effects of joint and spinal manipulation, and neuroplastic changes in central nervous system processing. SMT has been associated with altered somatosensory activation, sensorimotor integration, motor unit behaviour, and corticospinal excitability, potentially improving motor control and reducing recurrent neuromusculoskeletal pain. [15Ė18] Mechanotransduction at the cellular levelówhere cells sense mechanical cues and translate them into biochemical signalling, in part through cytoskeletal structuresómay also be involved in the response to spinal loading.
Improvements in MCS may be partly explained by reduced pain and disability and the known associations between chronic musculoskeletal pain, depression, anxiety, social functioning, and interoceptive awareness. [19Ė22] Regulation of the autonomic nervous system and endocannabinoid system has also been suggested as a mechanism by which chiropractic care might improve mood and related symptoms. [23, 24]
These mechanistic explanations are speculative in the context of this study, as no biochemical or neurophysiological measures were collected; they are based on prior research and provide possible pathways linking chiropractic care to changes in pain and quality of life. In our future study, we will be including blood biochemical parameters during Chiropractic acute care and follow-up maintenance care. These will include saliva Cytokines and Endocannabinoid levels and their precursors.
Limitations
Key limitations include:Recruitment from Italian chiropractic practices, which may limit generalizability to other settings.
Exclusive reliance on self-reported SF-36v2; no objective clinical measures or biomarkers were obtained
Analysis focused on baseline versus three-month outcomes without detailed exploration of trajectories or subgroup effectsNevertheless, the study demonstrates the feasibility of collecting standardized patient-reported outcomes in routine chiropractic practice and suggests that patients with spinal musculoskeletal pain report substantial improvements in physical and mental health over three months of chiropractic care.
Conclusion
In this 3-month longitudinal observational study of 163 adults with low back and/or neck pain receiving chiropractic care in Italian practices, statistically significant improvements in SF-36v2 Physical and Mental Component Summary scores were observed. These findings suggest that chiropractic care may be associated with improved health-related quality of life in patients with spinal musculoskeletal pain. Because of the uncontrolled design and potential confounding, causal conclusions cannot be drawn. Future controlled studies with longer follow-up and inclusion of mechanistic measures are needed to confirm these associations and clarify underlying biological and neurophysiological mechanisms.
References:
Vos T, Flaxman AD, Naghavi M, et al.
Years Lived with Disability (YLDs) for 1160 Sequelae of
289 Diseases and Injuries 1990-2010: A Systematic
Analysis for the Global Burden of Disease Study 2010
Lancet. 2012 (Dec 15); 380 (9859): 2163Ė2196Gaskin DJ, Richard P.
The economic costs of pain in the United States.
In: Relieving Pain in America: A Blueprint for Transforming
Prevention, Care, Education, and Research
National Academies Press; 2011.World Health Organization.
WHO Guidelines on Basic Training and Safety in Chiropractic
WHO; 2005.Deyo RA.
The Role of Spinal Manipulation
in the Treatment of Low Back Pain
JAMA. 2017 (Apr 11); 317 (14): 1418Ė1419Ware JE Jr, Sherbourne CD.
The MOS 36-Item Short-Form Health Survey (SF-36). I.
Conceptual framework and item selection.
Med Care. 1992;30:473-483.
doi:10.1097/00005650-199206000-00002McHorney CA, Ware JE Jr, Raczek AE.
The MOS 36-Item Short-Form Health Survey (SF-36): II.
Psychometric and clinical tests of validity in measuring
physical and mental health constructs.
Med Care. 1993;31:247-263.
doi:10.1097/00005650-199303000-00006McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD.
The MOS 36-Item Short-Form Health Survey (SF-36): III.
Tests of data quality, scaling assumptions, and
reliability across diverse patient groups.
Med Care. 1994;32:40-66.
doi:10.1097/0005650-199401000-00004Ware JE, Kosinski M, Dewey JE.
How to Score Version 2 of the SF-36 Health Survey.
QualityMetric Inc.; 2000.Jenkinson C, Wright L, Coulter A.
Criterion validity and reliability of the SF-36 in a population sample.
Qual Life Res. 1994;3:7-12.
doi:10.1007/BF00647843Gevers-Montoro C, Puente-Tobares M, Monrťal A, et al.
Urinary TNF-α as a potential biomarker for chronic
primary low back pain.
Front Integr Neurosci. 2023;17:1207666.
doi:10.3389/fnint.2023.1207666Zhang JM, An J.
Cytokines, inflammation, and pain.
Int Anesthesiol Clin. 2007;45(2):27-37.
doi:10.1097/AIA.0b013e318034194eGevers-Montoro C et al.
Presence of tumor necrosis factor-alpha in urine samples
of patients with chronic low back pain undergoing
chiropractic care: preliminary findings from
a prospective cohort study.
Front Integr Neurosci. 2022;16:879083.
doi:10.3389/fnint.2022.879083Teodorczyk-Injeyan JA, Injeyan HS, Ruegg R.
Spinal Manipulative Therapy Reduces Inflammatory Cytokines
but Not Substance P Production in Normal Subjects
J Manipulative Physiol Ther 2006 (Jan); 29 (1): 14Ė21Song XJ, Huang ZJ, Song WB, et al.
Attenuation Effect of Spinal Manipulation on
Neuropathic and Postoperative Pain Through
Activating Endogenous Anti-Inflammatory
Cytokine Interleukin 10 in Rat Spinal Cord
J Manipulative Physiol Ther 2016 (Jan); 39 (1): 42Ė53Pickar JG, Bolton PS.
Spinal Manipulative Therapy and Somatosensory Activation
Electromyogr Kinesiol. 2012 (Oct); 22 (5): 785Ė794Cecen S, Niazi IK, Nedergaard RW, et al.
Posture modulates the sensitivity of the H-reflex.
Exp Brain Res. 2018;236:829-835.
doi:10.1007/s00221-018-5182-xRobinault L, Holobar A, Crťmoux S, et al.
The effects of spinal manipulation on motor unit behavior.
Brain Sci. 2021;11(1):105.
doi:10.3390/brainsci11010105Haavik H, Niazi IK, Jochumsen M, et al.
Chiropractic spinal manipulation alters TMS-induced
I-wave excitability and shortens the cortical silent period.
J Electromyogr Kinesiol. 2018;42:24-35.
doi:10.1016/j.jelekin.2018.06.010Trivedi MH.
The link between depression and physical symptoms.
Prim Care Companion J Clin Psychiatry. 2004;6(Suppl 1):12-16.Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K.
Association of depression and anxiety alone and in
combination with chronic musculoskeletal pain
in primary care patients.
Psychosom Med. 2008;70(8):890-897.
doi:10.1097/PSY.0b013e318185c510. PMID:18799425Nicolson PJA, Williamson E, Morris A, et al.
Musculoskeletal pain and loneliness, social support
and social engagement among older adults:
analysis of the Oxford Pain, Activity and Lifestyle cohort.
Musculoskeletal Care. 2021;19(3):269-277.
doi:10.1002/msc.1526Craig AD.
Interoception: the sense of the physiological condition
of the body.
Curr Opin Neurobiol. 2003;13(4):500-505.
doi:10.1016/S0959-4388(03)00090-4Onifer SM, Sozio RS, Long CR.
Role for endocannabinoids in spinal manipulative therapy analgesia?
Evid Based Complement Alternat Med. 2019;2019:2878352.
doi:10.1155/2019/2878352Werner NS et al.
Interoceptive awareness moderates neural activity
during decision-making.
Biol Psychol. 2013;94(3):498-506.
doi:10.1016/j.biopsycho.2013.09.002
Return to LOW BACK PAIN
Return to CHRONIC NECK PAIN
Since 3-18-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |