

Symptomatic, Magnetic Resonance Imaging-Confirmed Cervical
Disk Herniation Patients: A Comparative-Effectiveness
Prospective Observational Study of 2 Age- and Sex-Matched
Cohorts Treated With Either Imaging-Guided Indirect Cervical
Nerve Root Injections or Spinal Manipulative TherapyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther. 2016 (Mar); 39 (3): 210-217 ~ FULL TEXT
OPEN ACCESS Cynthia K. Peterson, RN, DC, MMedEd, Christian W.A. Pfirrmann, MD, MBA,
Jürg Hodler, MD, MBA, Serafin Leemann, DC, Christof Schmid, DC,
Bernard Anklin, DC, B. Kim Humphreys, DC, PhD
Orthopaedic University Hospital Balgrist,
University of Zürich, Switzerland;
Professor, Chiropractic Medicine Department,
Orthopaedic University Hospital Balgrist,
University of Zürich, Switzerland.
xraydcpeterson@yahoo.ca
Thanks to JMPT for permission to reproduce this Open Access article! OBJECTIVE: The purpose of this study was to compare the outcomes of overall improvement, pain reduction, and treatment costs in matched patients with symptomatic, magnetic resonance imaging-confirmed cervical disk herniations treated with either spinal manipulative therapy (SMT) or imaging-guided cervical nerve root injection blocks (CNRI).
METHODS: This prospective cohort comparative-effectiveness study included 104 patients with magnetic resonance imaging-confirmed symptomatic cervical disk herniation. Fifty-two patients treated with CNRI were age and sex matched with 52 patients treated with SMT. Baseline numerical rating scale (NRS) pain data were collected. Three months after treatment, NRS pain levels were recorded and overall "improvement" was assessed using the Patient Global Impression of Change scale. Only responses "much better" or "better" were considered "improved." The proportion of patients "improved" was calculated for each treatment method and compared using the χ2 test. The NRS and NRS change scores for the 2 groups were compared at baseline and 3 months using the unpaired t test. Acute and subacute/chronic patients in the 2 groups were compared for "improvement" using the χ2 test.
RESULTS: "Improvement" was reported in 86.5% of SMT patients and 49.0% of CNRI patients (P = .0001). Significantly more CNRI patients were in the subacute/chronic category (77%) compared with SMT patients (46%). A significant difference between the proportion of subacute/chronic CNRI patients (37.5%) and SMT patients (78.3%) reporting "improvement" was noted (P = .002).
CONCLUSION: Subacute/chronic patients treated with SMT were significantly more likely to report relevant "improvement" compared with CNRI patients. There was no difference in outcomes when comparing acute patients only.
KEYWORDS: Cervical Spine; Comparative-Effectiveness Research; Disk Herniation; Injections; Manipulation, Spinal; Nerve Root; Outcomes Assessment; Radiculopathy
From the Full-Text Article:
Introduction
Cervical nerve root compression (radiculopathy) can be severely disabling in some patients and is caused by either disk herniation or more commonly spinal degeneration affecting the intervertebral foramina and subsequent exiting nerve root. [1] The most common nerve roots to be involved are the C6 and C7 levels, with the symptoms arising because of compression of the nerve root, inflammation of the nerve root, or both. [1, 2] Typical clinical signs and symptoms of cervical radiculopathy include pain in the distribution of the involved nerve root, paresthesias in a dermatomal pattern, weakness of the muscles innervated by the involved nerve root, and/or a decrease in the reflex. [3] In some patients, arm pain predominates over the neck pain. [3, 4]
The diagnosis of cervical nerve root compression is made with magnetic resonance imaging (MRI) scans. It is important, however, to recognize that disk protrusions seen on MRI are not always symptomatic, so it is critical that imaging abnormalities are linked to patient symptoms to determine whether or not the imaging findings are clinically relevant. [5–7] However, more severe disk herniations such as extruded disks with compression of the spinal cord are uncommon in asymptomatic people.7
Patients with symptomatic cervical disk herniations are initially treated conservatively, with surgery reserved for those cases that remain unresponsive to conservative care. [2–4, 8] A variety of different conservative treatments are used for these patients, including pain medications, physiotherapy treatment, lifestyle changes, nerve root injections, or even spinal manipulative therapy (SMT). However, most treatments, other than cervical transforaminal epidural steroid injections (cervical nerve root injections [CNRIs]), are not well documented with research evidence. [2, 3, 8–13] Recently, the use of imaging-guided CNRIs has come under scrutiny because of rare but extremely serious adverse events in some patients including ischemic myelopathy, transient or permanent tetraplegia, brain infarctions leading to death, and arterial dissections or cortical blindness. [14, 15] Because of the risk of such serious adverse events, a few institutions have modified the procedure to significantly reduce these risks to the new procedure called the imaging-guided indirect CNRI. [14, 16] Comparing short-term outcomes of this new indirect approach with the traditional direct nerve root injection showed no significant differences in the level of pain reduction. [16] The research evidence for SMT as a treatment for patients with symptomatic cervical disk herniations is sparse but slowly increasing, with a recent cohort outcomes study showing that more than 3/4 of patients with subacute and chronic symptoms reported clinically relevant improvement at 3 months after start of treatment. [10–13, 17] However, SMT to the cervical spine is not without controversy either. The issue of vertebral artery dissection and stroke after manipulation is often quoted. [18, 19] Unfortunately, accurate estimations of the frequency of this association cannot be calculated because of its rarity but are estimated at 1 of 200,000 treatments to 1 in several million treatments. [18, 19]
It is also important to recognize that the natural history for patients with acute symptoms from disk herniation (less than 4–8 weeks) is reported to be favorable, and thus, it is difficult to determine whether or not improvement in acute patients undergoing various treatments including CNRIs or SMT is due to the treatment or to the natural history of the condition. [19, 20] Randomized, controlled, clinical trials (RCTs) would be considered the “criterion standard” to compare specific treatments with patients not treated at all. However, subacute and especially chronic patients should have passed the time point for the effects of natural history to have occurred. Thus, evaluating the outcomes of these patients treated with various conservative therapies could provide useful evidence for clinicians.
Recently, comparative-effectiveness research has been promoted rather than RCTs to compare treatment outcomes for similar patients using databases from prospective cohort studies. [21, 22] It is argued that patients in prospective cohort outcomes databases may be more representative of patients seen in daily clinical practice as compared with patients included in RCTs. Based on this premise, the purpose of this study is to compare the outcomes of overall improvement, pain reduction, and treatment costs in age- and sex-matched patients with symptomatic, MRI-confirmed cervical disk herniations who were treated with either SMT or CNRI using a comparative-effectiveness prospective cohort design.
Methods
This is a comparative-effectiveness observational outcomes study on patients with symptomatic, MRI-confirmed cervical disk herniations. This study follows the same research protocol as done in a similar study using lumbar disk herniation patients. [23] One cohort of patients was from the radiology database for imaging-guided indirect CNRIs, and the other cohort was from the chiropractic medicine database for cervical SMT in cervical disk herniation patients. Both databases were started to monitor treatment outcomes as part of the research and quality assurance projects at this specialized orthopedic/rheumatology university hospital.
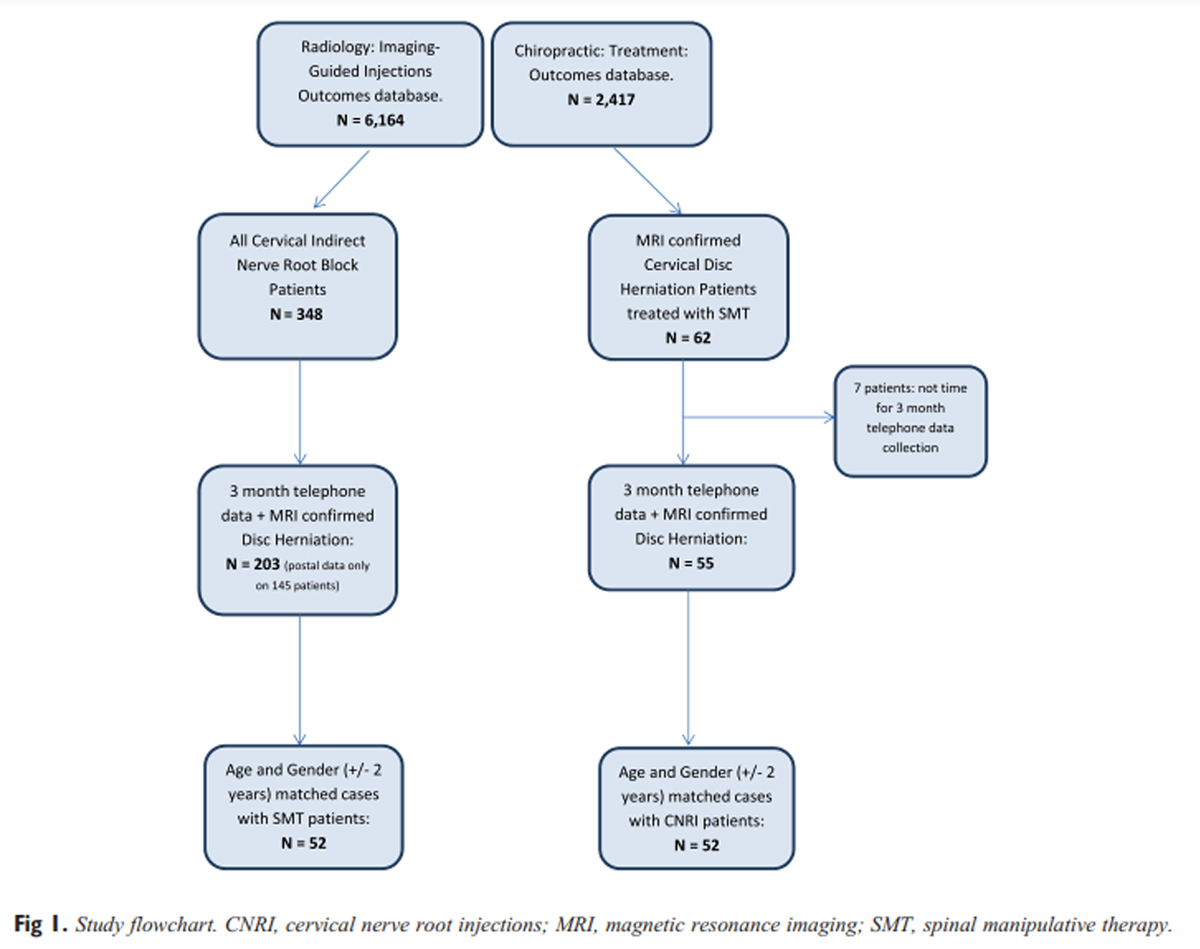
Figure 1 The CNRI patients were all treated in the radiology department at this hospital. The SMT patients were all treated by 1 of 3 different chiropractors in a single chiropractic practice which is involved in research studies with the university chiropractic medicine department. There was no crossover of patients switching treatments or having both interventions. Data for the CNRI patients were collected between January 2010 and August 2013. Data for the SMT patients were collected between October 2010 and February 2014. Patients in the 2 cohorts were age and sex matched (±2 years) blinded to the clinical outcomes, providing 52 patients in each group (Figure 1). As no further data collection telephone calls are being done for the CNRI patients, no additional subjects will be available from this treatment cohort for age and sex matching in the future. Thus, this study uses a convenience sample. Orthopaedic University Hospital Balgrist and the Canton of Zürich ethics committees approval was obtained before starting both databases (EK-08/2009 and EK-21/2009), and all patients signed informed consent. In both cohorts, the patients’ clinical signs and symptoms had to correspond to the MRI findings of disk herniation level.
Exclusion criteria for SMT patients included specific pathologies of the cervical spine that are contraindications for spinal manipulative treatment such as fractures, inflammatory arthropathies, infections, tumors, severe osteoporosis, and Paget disease. [17] Exclusion criteria for CNRIs included bacterial infection and bleeding diathesis. Relative contraindications included allergy to injected drugs and corticosteroid intolerance.
Before the first SMT treatment or the CNR injection, all patients were required to indicate their current pain level (baseline) using the 11-point numerical rating scale for pain (NRS) where 0 = no pain and 10 = the worst pain imaginable. Three months after the first SMT treatment or CNRI, follow-up data collection was done using telephone interviews. These were done by research assistants from the university hospital unknown to the patients. One research assistant phoned only the CNRI patients, whereas a different research assistant phoned only the SMT patients. Therefore, they were not blinded to the treatment applied. The NRS for pain was used to assess the current pain level experienced by the patient at 3 months. In addition, the Patients’ Global Impression of Change (PGIC) scale was used to evaluate overall improvement in terms of disability, function, and well-being. The PGIC is a 7-item scale and includes the responses much better, better, slightly better, unchanged, slightly worse, worse, and much worse. [24] Only the responses much better and better were considered clinically relevant “improvement” consistent with other published studies. [17, 23] This was the primary outcome measure. All other patients were classified as not improved including the response slightly better. In addition, the responses slightly worse, worse, and much worse were considered as worsening of the condition. This was a secondary outcome measure, as were the NRS 3-month actual scores and the 3-month NRS change scores.
Duration of complaint data was routinely collected before the first SMT treatment and available for all patients in this cohort. A review of the electronic patient files was done to obtain these same data for all CNRI patients. This was categorized as acute (?4 weeks) or subacute/chronic (>4 weeks).
Cervical Indirect Nerve Root Injection Procedure

Figure 2 All cervical indirect nerve root injections were performed as outpatient procedures with computed tomography (CT) fluoroscopic guidance (40–detector row CT, Philips Brilliance; Philips Medical Systems, Best, the Netherlands) by musculoskeletal radiologists experienced in spinal interventions using the detailed protocol previously published. [16] Injections were performed under sterile conditions using a 23-gauge needle aimed at the lateral aspect of the relevant facet joint. Using CT fluoroscopy, the needle was advanced until it touched the bone of the facet joint. An injection of 0.5 mL iopamidol (Iopamiro 200, 200 mg of iodine per milliliter; Bracco, Milan, Italy) was performed to verify the correct position of the needle tip. The contrast distribution was monitored with a single CT fluoroscopic scan (4 slices with a slice thickness of 3.75 mm; field of view, 15 cm; bone window setting). Following the injection of contrast, 4 mg (1 mL) of the nonparticulate corticosteroid preparation dexamethasone (Fortecortin Inject; Merck, Darmstadt, Germany) was slowly injected. This was followed by a slow injection of 1 mL of 0.2% ropivacaine (Naropin 0.2%; Astra-Zeneca, Södertälje, Sweden) (Figure 2).
Spinal Manipulation Procedure
The high-velocity, low-amplitude cervical spine manipulation to the level of the disk herniation was described in detail in a previous publication. [17] All patients were treated in the same way by 1 of the 3 chiropractors with between 6 and 30 years of clinical experience working together in the same practice and who had all completed the 2-year postgraduate residency program mandatory in Switzerland. The goal was to produce an audible release, which was reported in most patients. Treatments were repeated 3 to 5 times per week for the first 2 to 4 weeks and then 1 to 3 times per week thereafter if needed. No additional therapeutic measures were done during the chiropractic visits.
Statistical Analysis
In addition to descriptive statistics, the proportion of patients reporting clinically relevant “improvement” (responses of “much better” or “better” on the PGIC scale) were calculated for each treatment group and compared using the χ2 statistic. This was the primary outcome measure. In addition, the proportion of patients reporting “worsening” of their condition was also calculated and compared using the χ2 test. The χ2 test was also used to compare the proportions of “acute” and “subacute/chronic” patients between the 2 treatment groups as well as to compare the proportions of patients “improved” or “worse” for each treatment in each of these 2 chronicity categories.
The baseline and 3-month NRS scores were compared using the paired Student t test for each of the treatment groups individually. The baseline and 3-month NRS scores were compared between the 2 groups using the unpaired t test to assess for significant differences. In addition, the unpaired t test was used to compare the 3-month NRS change scores for significant differences. The median 3-month PGIC scores were also assessed for differences using the Mann-Whitney U test as these data were nonparametric.
The proportion of patients treated at the specific cervical nerve root levels was calculated for each of the 2 treatments. The average treatment cost for the SMT patients was calculated, and the actual treatment cost for the CNRI procedure was obtained from the hospital billing department.
Discussion
This is the first study to have the necessary resources and databases to be able to compare the outcomes of 2 different conservative treatments for patients suffering from cervical radiculopathy. Although not a randomized, blinded, clinical trial, using these prospective cohort outcomes databases allows the inclusion of patients who are representative of those seen in routine clinical practice and follows the recommendations of Tinetti and Studenski [21] in performing comparative-effectiveness research.
Although the outcomes for the cervical disk herniation patients treated with SMT were markedly better than those treated with CNRI, some of this difference is due to the fact that a significantly higher proportion of patients in the CNRI cohort were subacute/chronic. Indeed, when comparing the outcomes for only the acute patients (symptoms < 4 weeks), there was no significant difference between the 2 treatments, as most of the acute patients improved. Much of this may be due to the natural history of the condition and not related to the specific treatment. [9, 20] Therefore, it was important to compare the outcomes for those patients with symptoms longer than 4 weeks. This did reveal a significant difference between the SMT- and CNRI-treated patients, with more than 78% of the SMT cohort reporting clinically relevant improvement compared with 37.5% of those treated with CNRI. However, it is important to point out that the CNRI patients only received a single nerve root block treatment, whereas the SMT patients were treated several times based on their follow-up clinical assessments during the 3–month time period from baseline to collection of the outcome data. This may have influenced the results in favor of the SMT cohort even though the literature reports that a single nerve root injection containing corticosteroid and anesthetic may result in at least a 50% reduction in pain (considered clinically relevant improvement) for 3–6 months. [25] However, when comparing the results of the entire CNRI cohort of 52 patients in this study where 49% were “improved” at 3 months with the shorter-term 1–month outcomes of all CNRI patients (n = 195) currently listed in the radiology database, there is surprisingly little difference, as only 43% of patients reported clinically relevant improvement even at the 1–month data collection time point. [26] Therefore, the longer data collection time point of 3 months does not appear to have been a negative factor in the proportion of clinically improved CNRI patients. Comparing the treatment costs between the SMT and CNRI patients shows a minimal difference of only CHF 42.47 even though the SMT patients were treated multiple times.
A recently published systematic review on the effectiveness of CNRI states that the minimal standard of a successful outcome is at least 50% relief of radicular pain that lasts a minimum of 4 weeks postinjection and further states that the quality and quantity of the research studies on direct, transforaminal nerve root injections are low. [25] The various studies included in this systematic review reported a range of postinjection data collection time points as well as clinically relevant improvement in as few as 20% of patients to as many as 56%. The results from this current study of 49% of CNRI patients reporting clinically relevant improvement are better than those reported in a recent retrospective practice audit where only 35.4% of patients receiving a direct transforaminal nerve root block had at least a 50% pain reduction 1 month postinjection. [27] A comparison of our results with those previously published is important because the method of injection in this current study is the so-called indirect nerve root block procedure, whereas the results in all previous research studies used the direct transforaminal approach. [16] As reported in detail in a previous publication, this indirect nerve root block procedure should have a much lower level of potential risk for serious adverse events compared with the traditional direct transforaminal approach due to the injection technique, and yet the outcomes, at least in the medium term, are comparable. [16]
Unfortunately, there are no similar outcome studies with which to compare the SMT patients, as spinal manipulation has often been considered a controversial treatment for patients with known cervical disk herniations and radiculopathy. There were no adverse events in either of the 2 treatment cohorts in this study, and none of the SMT patients reported that they were worse at the 3–month data collection time point.
Limitations
As noted previously, this is not a randomized, blinded, clinical trial (RCT), so the outcomes cannot be directly attributed to the treatments. A follow-up RCT should be done and would be possible in the university clinical environment of this hospital which includes chiropractic medicine as an integral component of the university teaching within the faculty of medicine and the hospital therapeutic options. The sample sizes are also relatively small with 52 patients per group. However, further telephone data collection for the CNRI cohort has ceased, and thus, additional patients are not available. This factor should not have negatively influenced the results because even with these relatively small sample sizes, large statistical and more importantly clinically significant differences were found for the subacute/chronic patients.
There was no attempt to match the patients for comorbidities in this study, and that may be a limitation because many of the CNRI patients referred to this hospital are complex patients. Importantly, however, there was no difference in the baseline NRS scores between the 2 groups as was found when doing the lumbar disk herniation similar study. [23]
Although the treatment costs between the 2 groups were very similar, no attempt was made to collect associated costs or time off work data to do a proper cost-effectiveness comparison.
Conclusions
Most acute patients with MRI-confirmed symptomatic cervical disk herniations treated with either CNRI or SMT reported clinically relevant improvement at 3 months with no significant difference in outcomes between the 2 treatment methods. However, when comparing the 3–month outcomes for the subacute/chronic patients, more than 78% of patients treated with spinal manipulative therapy (SMT) reported clinically relevant improvement compared with 37.5% of patients receiving a single imaging-guided cervical nerve root injection (CNRI). The treatment costs between the 2 groups were very similar. There were no adverse events for either cohort.
Practical Applications
Subacute and chronic patients treated with spinal manipulation
were statistically and clinically significantly more likely to
report improvement at 3 months compared with
the nerve root injection cohort.There was no significant difference in outcomes between acute
patients treated with cervical nerve root blocks and those
treated with spinal manipulation at 3 months.There were no adverse events for patients in either treatment group.
The cost of treatment was similar for the 2 treatment procedures.
Funding Sources and Conflicts of Interest
The following provided funding for this study: Vontobel Stiftung, Zürich, Switzerland; European Chiropractor’s Union; The Balgrist Foundation; and Uniscientia Foundation.
No conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): C.K.P., C.W.A.P., J.H., S.L., C.S., B.A., B.K.H.
Design (planned the methods to generate the results): C.K.P., S.L., C.S., B.K.H., J.H., C.W.A.P.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript):C.K.P.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): S.L., C.S., B.A., C.W.A.P., J.H.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): C.K.P.
Literature search (performed the literature search): C.K.P.
Writing (responsible for writing a substantive part of the manuscript): C.K.P.
Critical review (revised manuscript for intellectual content; this does not relate to spelling and grammar checking): C.W.A.P., J.H., S.L., C.S., B.A., B.K.H.
References:
Radhakrishnan K Litchy WJ O’Fallon WM Kurland LT
Epidemiology of cervical radiculopathy.
A population-based study from Rochester, Minnesota, 1976 through 1990.
Brain. 1994; 117: 325-335Murphy DR, Hurwitz EL, Gregory A, Clary R.
A Nonsurgical Approach to the Management of Patients With Cervical Radiculopathy:
A Prospective Observational Cohort Study
J Manipulative Physiol Ther. 2006 (May); 29 (4): 279–287Wainner RS Fritz JM Irrgang JJ Boninger ML Delitto A Allison S
Reliability and diagnostic accuracy of the clinical examination
and patient self-report measures for cervical radiculopathy.
Spine. 2003; 28: 52-62Murphy DR
Herniated Disc with Radiculopathy Following
Cervical Manipulation: Nonsurgical Management
Spine J 2006 (Jul); 6 (4): 459–463Healy JF Healy BB Wong WHM Olson EM
Cervical and lumbar MRI in asymptomatic older male lifelong athletes:
frequency of degenerative findings.
J Comput Assist Tomogr. 1996; 20: 107-112Matsumoto M Fujimura Y Suzuki N et al.
MRI of cervical intervertebral discs in asymptomatic subjects.
J Bone Joint Surg Br. 1998; 80-B: 19-24Ernst CW Stadnik TW Peeters E Breucq C Osteaux MJC
Prevalence of annular tears and disc herniations on MR images
of the cervical spine in symptom free volunteers.
Eur J Radiol. 2005; 55: 409-414Lin EL Lieu V Halevi L Shamie AN Wang JC
Cervical epidural steroid injections for symptomatic disc herniations.
J Spinal Disord Tech. 2006; 19: 183-186Kolstad F Leivseth G Nygaard OP
Transforaminal steroid injections in the treatment of cervical radiculopathy.
A prospective outcome study.
Acta Neurochir (Wien). 2005; 147: 1065-1070Vernon HT Humphreys BK Hagino CA
A systematic review of conservative treatments for
acute neck pain not due to whiplash.
J Manipulative Physiol Ther. 2005; 28: 443-448Bronfort G Haas M Evans RL et al.
Efficacy of Spinal Manipulation and Mobilization for Low Back Pain and
Neck Pain: A Systematic Review and Best Evidence Synthesis
Spine J (N American Spine Soc) 2004 (May); 4 (3): 335–356BenEliyahu DJ
Magnetic Resonance Imaging and Clinical Follow-up: Study of 27 Patients
Receiving Chiropractic Care for Cervical and Lumbar Disc Herniations
J Manipulative Physiol Ther 1996 (Nov); 19 (9): 597—606Gross AR Hoving JL Haines RA et al.
A Cochrane review of manipulation and mobilization
for mechanical neck disorders.
Spine. 2004; 29: 1541-1548Hodler J Boos N Schubert M
Must we discontinue selective cervical nerve root blocks?
Report of two cases and review of the literature.
Eur Spine J. 2013; 22: S466-S470Scanlon GC Moeller-Bertram T Romanowsky SM Wallace MS
Cervical transforaminal epidural steroid injections.
More dangerous than we think?
Spine. 2007; 32: 1249-1256Sutter R Pfirrmann CWA Zanetti M Hodler J Peterson CK
CT-guided cervical nerve root injections: comparing the immediate
post-injection anesthetic-related effects of the
transforaminal injection with a new indirect technique.
Skeletal Radiol. 2011; 40: 1603-1608Peterson CK Schmid C Leemann S Anklin B Humphreys BK
Outcomes from magnetic resonance imaging–confirmed symptomatic cervical
disk herniation patients treated with high-velocity, low-amplitude
spinal manipulative therapy: a prospective cohort study
with 3-month follow-up.
J Manipulative Physiol Ther. 2013; 36: 461-467Thiel HW, Bolton JE, Docherty S, Portlock JC:
Safety of Chiropractic Manipulation of the Cervical Spine:
A Prospective National Survey
Spine (Phila Pa 1976). 2007 (Oct 1); 32 (21): 2375–2378Cassidy JD, Boyle E, Cote P, et al.
Risk of Vertebrobasilar Stroke and Chiropractic Care: Results of a
Population-based Case-control and Case-crossover Study
Spine (Phila Pa 1976) 2008 (Feb 15); 33 (4 Suppl): S176–183Rao R
Neck pain, cervical radiculopathy and cervical myelopathy.
Pathophysiology, natural history and clinical evaluation.
J Bone Joint Surg Am. 2002; 84-A: 1872-1881Tinetti ME Studenski SA
Comparative effectiveness research and patients with multiple chronic conditions.
N Engl J Med. 2011; 364: 2478-2481Neumann PJ
Communicating and promoting comparative-effectiveness research findings.
N Engl J Med. 2013; 369: 209-211Peterson CK Leemann S Lechmann M Pfirrmann CWA Hodler J Humphreys BK
Symptomatic magnetic resonance imaging–confirmed lumbar disc herniation patients:
a comparative effectiveness prospective observational study of 2 age-and
sex-matched cohorts treated with either high-velocity, low-amplitude
spinal manipulative therapy or imaging-guided lumbar nerve root injections.
J Manipulative Physiol Ther. 2013; 36: 218-225Fischer D Stewart AL Bloch DA Lorig K Laurent D Holman H
Capturing the patient’s view of change as a clinical outcome measure.
JAMA. 1999; 282: 1157-1162Engel A King W MacVicar J
The effectiveness and risks of fluoroscopically guided cervical
transforaminal injections of steroids: a systematic review
with comprehensive analysis of the published data.
Pain Med. 2014; 15: 386-402Peterson C Pfirrmann CWA Hodler J
The development and implementation of an outcomes database for
imaging-guided therapeutic musculoskeletal injections.
Skeletal Radiol. 2014;
https://doi.org/10.1007/s00256-014-1881-yKlessinger S Freund W Karpel-Massler G Halatsch ME
Response to transforaminal injection of steroids and correlation to
MRI findings in patients with cervical radicular pain or
radiculopathy due to disc herniation of spondylosis.
Pain Med. 2014; 15: 929-937
Return to RADICULOPATHY
Return to CHRONIC NECK PAIN
Return to CHIROPRACTIC AND SCIATICA
Return to DISC HERNIATION & CHIROPRACTIC
Since 6-04-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |