

Community-based Free Clinics: Opportunities for
Interprofessional Collaboration, Health Promotion,
and Complex Care ManagementThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Education 2016 (Mar); 30 (1): 25-29 ~ FULL TEXT
OPEN ACCESS Martha A. Kaeser , MEd, DC, Cheryl Hawk , DC, PhD,
Michelle L. Anderson , Richard Reinhardt DC
Logan University
1851 Schoettler Rd,
Chesterfield, MO, 63017Objective: Free or outreach clinics offer students the opportunity to work with diverse patient populations. The objective of this study was to describe the demographics and clinical characteristics of a sample of chiropractic patients at a free community-based clinic to assess clinical and educational opportunities for students to work with diverse populations, collaborate with other professions and practice health promotion through patient education.
Methods: This was a prospective, descriptive cross-sectional study conducted over 2 months. Data on demographics, health status, and health risks were collected from patients and their interns.
Results: Of the 158 patients, 50.6% were women and 50.6% African-American, while only 20.9% were employed full-time. Of the 24.7% tobacco users, 48.7% expressed interest in cessation. Of 80.0% overweight or obese patients, 48.8% expressed interest in weight loss. By self-report, 16.5% were diabetic, 10.1% took hypertension medication, 36.7% used prescription pain medication (9.4% opiate use), 33.5% used nonprescription pain medication, and 9.4% were under the care of a mental health professional.
Conclusion: This patient population is demographically diverse. A high proportion of patients who used tobacco, or were overweight or obese expressed interest in information on those topics. A substantial proportion reported being under care with a mental health professional. This clinic provides opportunities for students to work with diverse populations, collaborate with other professions, and practice health promotion.
Keywords: Community Health Centers, Health Promotion, Interprofessional Relations, Cultural Diversity
From the FULL TEXT Article
INTRODUCTION
Many chiropractic institutions operate free or outreach clinics. [1-3] Health care services are offered for no cost to low-income, uninsured, or underinsured individuals with the overarching goal of decreasing health disparities. [4] The Council on Chiropractic Education requires that an institution “conducts and supports service activities congruent with its mission, goals, and objectives.” [5] This can be achieved through “low cost or free health care to underserved populations in either Doctor of Chiropractic Program managed clinics or in clinical settings controlled by external agencies.” [5] These clinics typically are located in economically disadvantaged locations and offer students the opportunity to work with diverse patient populations. They also provide students the educational experience of managing patients who may not traditionally enter a chiropractic clinic. [2]
These clinics also provide opportunities for interprofessional education and collaboration. Approximately half of the medical schools in the United States have one or more student-run clinics that teach students clinical skills, medical humanism, systems-based practice, collaboration, and multidisciplinary approaches and leadership skills. [6] Interprofessional collaboration provides educational benefits for students and improves patient outcomes. [2, 7] Healthcare profession students who plan to work as providers in interprofessional collaborative practices must learn in interprofessional settings. [8] Community-based clinics can be excellent examples of such settings where students collaborate with other health care professionals to provide chronic disease management. [9] Students also develop an understanding of the value and contribution of other professionals when they cooperate with and share resources across professions. [8]
Opportunities for health promotion and disease prevention counseling also are available at community-based free clinics. For example, uninsured smokers are approximately one-third to one-half as likely to receive tobacco cessation services. [9] Hawk et al. [10] investigated the feasibility of incorporating tobacco cessation counseling into the chiropractic curriculum, and emphasized the importance of providing students opportunities to assess and counsel patients in the health care curriculum, including outpatient clinical training. Community-based free clinics would provide excellent opportunities to a population of tobacco users that aren't traditionally receiving cessation services.
The purpose of this study is to describe the demographics and clinical characteristics of a sample of chiropractic patients at a free community-based clinic for the purpose of assessing opportunities to broaden students' experiences with diverse populations, provide opportunities for interprofessional collaboration, and practice health promotion skills.
METHODS
This was a descriptive prospective, cross-sectional study conducted over two, 2-month intervals (June–July 2014 and October–November 2014). All patients, new and established, who presented for care at the university's free community-based clinic, were eligible to participate. There were no exclusions. The Logan University institutional review board approved the study before data collection was started.
Data Collection Site: A Free Community-Based Health Care Clinic
One of the centers where the university offers community-based health care services assists the homeless or those at risk for homelessness in finding housing, employment, and health opportunities. The center is located centrally in a large metropolitan area with a 2013 population of approximately 318,000. United States 2008 to 2012 census data report that 27% of individuals living within the city where the clinic resides were below the poverty level, with a median household income of $34,384. In 2013, African Americans made up 47.9% of the population of the city, while whites comprised 46.4%. Chiropractic health care has been offered through the free clinic since 2003.
The clinic is open every weekday from 11:30 AM to 4:30 PM with an average of 20 patients per day. Five chiropractic student interns are assigned to the clinic each day with 2 additional student interns serving as senior intern assistants. The clinic has 5 patient treatment areas and provides patients with all institution-sanctioned adjusting procedures, moist heat, intersegmental traction, and interferential and soft tissue techniques. They also provide advice on exercise, nutrition, and ergonomics. Patient treatment and management are overseen by a licensed chiropractic physician with 42 years of experience, 6 years of which have been with economically disadvantaged patients. Currently patients are accepted regardless of their underlying condition, mental status, income, ethnicity, or age.
The chiropractic clinic worked closely with a student-run free medical and dental clinic, also within the center until the medical and dental clinics moved in 2012. This provided an opportunity for students to co-manage and refer those patients who required care outside the chiropractic scope of practice. At the same time, the medical and dental facilities referred patients to the chiropractic clinic. Currently, patients are referred to medical or dental providers, or emergency departments elsewhere in the city. Mental health services currently are provided at the center. Currently, this is the only interprofessional opportunity available to the students.
Data Collection
Data were collected via paper forms completed by patients and their student interns at the clinic. Data collection forms were based on forms used in previous practice-based research studies. [11, 12] Two forms were used: one to be completed by patients and the other by the patient's student intern. The forms were linked using the patient's identification code; no other personal identifiers were used. The patient form included some demographics, health status information, chiropractic care, and their choice of clinic, and their interest in receiving health education information on specific topics. These items were all closed-ended questions. The student intern form collected age, sex, chief complaint (pain, nonpain-related complaint, or “no problem today”), height, weight, blood pressure, tobacco use, diabetes status, concurrent care, medications, and supplements.
Patients were to be provided with the patient form by the receptionist or intern when they presented for care within the study period. Those administering the form were instructed by an investigator to give patients the form only once, regardless of how many visits they had during the study period. They, in turn, instructed patients verbally not to complete the form if they had already done so; this also was specified on the form.
Data Analysis
Data from the paper forms were key entered and double-entry verified in an SPSS version 22 (IBM Corporation, Armonk, NY) database. Only patients with a patient form and intern form were included in the analysis; duplicates and unmatched forms were removed. Body mass index (BMI) was calculated using the standard formula and categorized as normal (BMI < 25); overweight (BMI 25–29.9) or obese (BMI > 30).13
Hypertension was defined as per the definition of the National Heart Lung and Blood Institute as systolic pressure > 139 mm Hg or diastolic pressure > 89 mm Hg.14 Descriptive statistics were computed using SPSS.
RESULTS
A total of 158 patients had complete data. There were a total of 168 patient-completed forms; 10 were duplicates, leaving 158. There were 160 intern-completed forms; 2 were eliminated because they did not have a matching patient form.
Of the 158 patients, 41 (26.0%) said that the current visit was their first one. An additional 42 (26.6%) had last visited the clinic over 3 months previously. Most patients (60.1%) reported ever having had chiropractic care before visiting this clinic. Patients' reasons for selecting this clinic were: referral from family/friend (44.3%), cost (34.8%), other referral (30.4%), and convenience (24.7%). Patients most frequently reported traveling to the clinic by driving themselves (50.6%) or having someone else drive them (16.5%); they also travelled by public transportation (18.4%) or walking (10.8%).

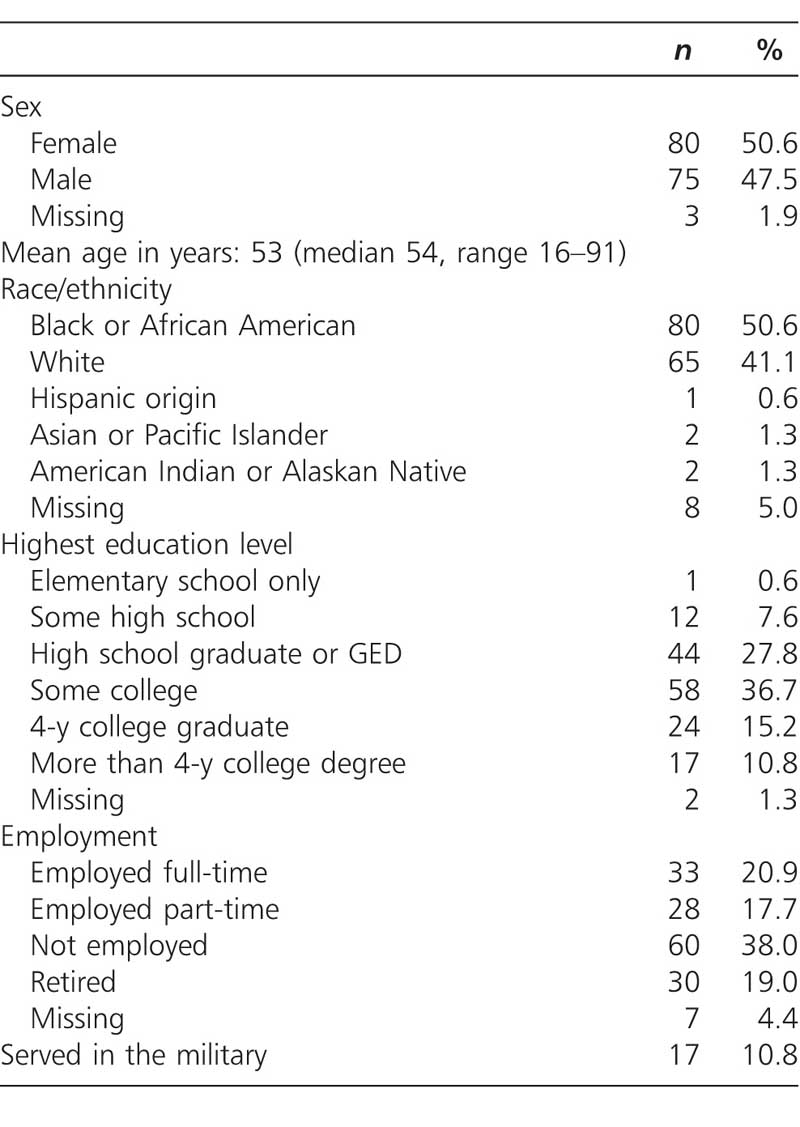
Table 1
Table 2 Table 1 summarizes the patients' demographics. There was a slightly higher proportion of women than men (50.6% vs. 47.5%, respectively). The majority of patients were African-American (50.6%) or white (41.1%), with some college education (36.7%). More than one-third (38.0%) were unemployed, while 20.9% were employed full-time. Veterans comprised 10.8% of the sample.
A large majority (91.1%) presented with a pain-related chief complaint, with 36.7% reporting use of prescription pain medication (9.4% reported opiate use) and 33.5% reporting use of nonprescription pain medications. Approximately half (53.8%) were currently under concurrent care for either their chief complaint or other health issues. Of these, 36.5% reported being under care with a primary care provider (Medical Doctor [MD] or Nurse Practitioner [NP]). Eight (9.4%) reported being under the care of a mental health professional.
DISCUSSION
Students at our institution have numerous opportunities to volunteer or be assigned to work at any of the 3 clinics for socioeconomically disadvantaged patients. A previous study at this institution identified gaps in students' exposure at our fee-for-service clinics to the full spectrum of patient characteristics and complaints. [15] The current study explored opportunities presented by 1 of our community-based free clinics to fill these gaps.
Experience With Diverse Populations and Complex Care Needs
Opportunities to work with diverse populations are available at community-based free clinics. For example, in our free clinic, patient demographics are significantly different than those of the fee-for-service clinics at the institution. African-American patients make up 7.1% of patients at the fee-for-service clinics versus 51% at the free clinic. Mean age also is considerably different, with a mean age of 37.3 at the fee-for-service clinics and 53 seen at the free clinic.
Patients with complex care needs and multiple comorbidities often are seen at community-based health clinics and are, in fact, becoming increasingly prevalent in the general population. [16] The most common comorbidities are cardiovascular disease, hypertension, and diabetes. [4] It is important that students experience caring for such patients during their training. Data from our free clinic suggest that many of the patients have multiple comorbidities and complex health care needs. A total of 18% report having been diagnosed as diabetic; 10% taking opiates for pain, 10% using hypertension medication, and 9% seeing a mental health professional. A total of 46% are obese, which often is accompanied by a number of comorbid conditions.
Interprofessional Collaboration
Opportunities for interprofessional collaboration are important during clinical education. The definition of a free health clinic is a “private, nonprofit, community-based organization that offers services, such as primary and secondary medical and dental care, along with pharmaceutical, laboratory, and/or mental health services.” [4] Our free chiropractic clinic currently is the only physical health care facility at the community center. Currently, there is a nonprofit mental health foundation at the center with professionals from a local university's department of psychiatry. The mental health foundation with a presence at the clinic site states that they collaborate with experts from a number of disciplines to encourage healthy behavior in patients. Since 9% of our patients reported seeing a mental health professional, an opportunity for collaboration already is present. However, merely putting health care providers in proximity does not equate to successful collaboration. Attention must be paid to frequent participation, training, and physical space for sharing patient information, cross-disciplinary networking, and reflection. [8] We hope to explore such aspects in the future.
Health Promotion
Data were collected from this study regarding patients' health status and risk factors. Body mass index (BMI) indicated that 44% of patients were obese (BMI ≥ 30); 37% percent were overweight (BMI 25–29.9). Self-reported current tobacco use among study participants was 25%. For tobacco users and obese/overweight patients, approximately half (49% for each) expressed interest in advice on quitting or weight management.
As part of the coursework at our institution, all students are instructed in weight management and tobacco cessation counseling. [10] Clearly, this clinic provides an opportunity to practice these skills.
Future Action Steps
The purpose of the current project was to assess opportunities at a local free clinic to broaden students' experiences with diverse populations, provide opportunities for interprofessional collaboration, and practice health promotion skills. A logical future project may be to ask the question, “Do student interns at this particular clinic perceive the same benefits and opportunities presented in this manuscript”? This can be done through surveys, focus groups, discussion groups, or a combination of the two as a follow-up qualitative project. In addition, patients at this community-based clinic expressed an interest in health promotion advice or counseling; therefore, a next step might be to provide an intervention to answer the question, “Will students provide health promotion advice and counseling based on patient interest alone”?
Limitations
This study has several limitations. First, much of the information was self-reported. Second, the information obtained was from only one clinic and so cannot be generalized to other community-based free clinics. Third, some information (such as drug use, income, homelessness) was not collected due to its sensitive nature. Finally, data or patients may have been missed due to oversight during the data collection process.
CONCLUSION
Our community-based free clinic provides opportunities for students to work with a diverse patient population, co-manage complex care needs through interprofessional collaboration, and practice health promotion.
FUNDING AND CONFLICTS OF INTEREST
This work was funded internally. The authors have no conflicts of interest to declare relevant to this work.
References:
Morschhauser E, Long CR, Hawk C, et al.
Do chiropractic colleges' off-campus clinical sites offer diverse opportunities for learning? A preliminary study.
J Manipulative Physiol Ther. 2003;26(2):70–76Kopansky-Giles D, Vernon H, Steiman I, et al.
Collaborative community-based teaching clinics at the Canadian Memorial Chiropractic College: addressing the needs of local poor communities.
J Manipulative Physiol Ther. 2007;30(8):558–565Stevens GL.
Demographic and referral analysis of a free chiropractic clinic servicing ethnic minorities in the Buffalo, NY area.
J Manipulative Physiol Ther. 2007;30(8):573–577Notaro SJ, Khan M, Bryan N, et al.
Analysis of the demographic characteristics and medical conditions of the uninsured utilizing a free clinic.
J Community Health. 2012;37(2):501–506The Council on Chiropractic Education.
CCE Accreditation Standards Principles,
Processes & Requirements for Accreditation.
Scottsdale, AZ: The Council on Chiropractic Education; 2013Rebholz CM, Macomber MW, Althoff MD, et al.
Integrated models of education and service involving community-based health care for underserved populations: Tulane student-run free clinics.
South Med J. 2013;106(3):217–223Sanders J, Solberg B, Gauger M.
Breaking barriers to care: a community of solution for chronic disease management.
J Am Board Fam Med. 2013;26(3):311–315Sick B, Sheldon L, Ajer K, Wang Q, Zhang L.
The student-run free clinic: an ideal site to teach interprofessional education?
J Interprof Care. 2014;28(5):413–418Foley KL, Pockey JR, Helme DW, et al.
Integrating evidence-based tobacco cessation interventions in free medical clinics: opportunities and challenges.
Health Promot Pract. 2012;13(5):687–695Hawk C, Kaeser MA, Beavers DV.
Feasibility of using a standardized patient encounter for training chiropractic students in tobacco cessation counseling.
J Chiropr Educ. 2013;27(2):135–140Evans M, Hawk C, Ndetan H, Rupert R,
Patient characteristics, screening use, and health education advice in a chiropractic practice-based research network.
Top Integrative Health Care. 2012;3(1Hawk C, Evans MW, Rupert R, Ndetan H.
Opportunities to integrate prevention into the chiropractic clinical encounter: a practice-based research project by the Integrated Chiropractic Outcomes Network (ICON).
Top Integr Health Care. 2011;2(3United States Preventive Services Task Force.
Guide to Clinical Preventive Services.
Washington, DC: Agency for Healthcare Research and Quality (AHRQ); 2014National Heart LaBI.
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
NIH Publication No. 04-5230.
Washington DC: U.S. Department of Health and Human Services; 2004Kaeser M, Hawk C, Anderson M.
Patient characteristics upon initial presentation to chiropractic teaching clinics: a descriptive study conducted at one university.
J Chiropr Educ. 2014;28(2):146–151Centers for Medicare and Medicaid Services.
Chronic Conditions among Medicare Beneficiaries, Chartbook.
Baltimore, MD: Centers for Medicare and Medicaid Services; 2012
Return to HEALTH PROMOTION
Return to MAINTENANCE CARE
Since 5-04-2016

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |