

When Radiculopathy Isn't Radiculopathy: A Clinical Series
Part 1: The Limits of Dermatomes and Disc-Centric ThinkingThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Dynamic Chiropractic (Apr 1); 44 (4) ~ FULL TEXT
OPEN ACCESS Ken Kaufman, DC
The Cleveland ClinicWHAT YOU NEED TO KNOW
Radicular-like pain of the upper and lower extremities is among the most common presentations in musculoskeletal and spine-related practice. Traditionally, these symptoms are interpreted through a disc-centric and dermatomal framework.
While this approach is appropriate in cases of true radiculopathy, it frequently falls short when symptoms fail to follow consistent dermatomal patterns or correlate poorly with imaging findings.
Radicular-like symptoms do not automatically equate to radiculopathy. Before invasive spinal procedures are considered, clinicians must first determine whether the presentation reflects true nerve-root pathology or a functional mimic.
Radicular-like pain of the upper and lower extremities is among the most common presentations in musculoskeletal and spine-related practice. Traditionally, these symptoms are interpreted through a disc-centric and dermatomal framework, often leading clinicians to attribute limb pain, paresthesia or perceived weakness to spinal nerve-root pathology.
While this approach is appropriate in cases of true radiculopathy, it frequently falls short when symptoms fail to follow consistent dermatomal patterns or correlate poorly with imaging findings.
In recent decades, clinicians have increasingly recognized that not all radicular-like symptoms arise from discogenic or neural compression mechanisms. Piriformis syndrome is one such example, widely accepted as a cause of sciatic-like pain in the absence of lumbar nerve-root compromise. Despite this recognition in the lower extremity, a comparable diagnostic construct for the upper extremity has remained underdeveloped.
The Radiculopathy Clinical Conundrum
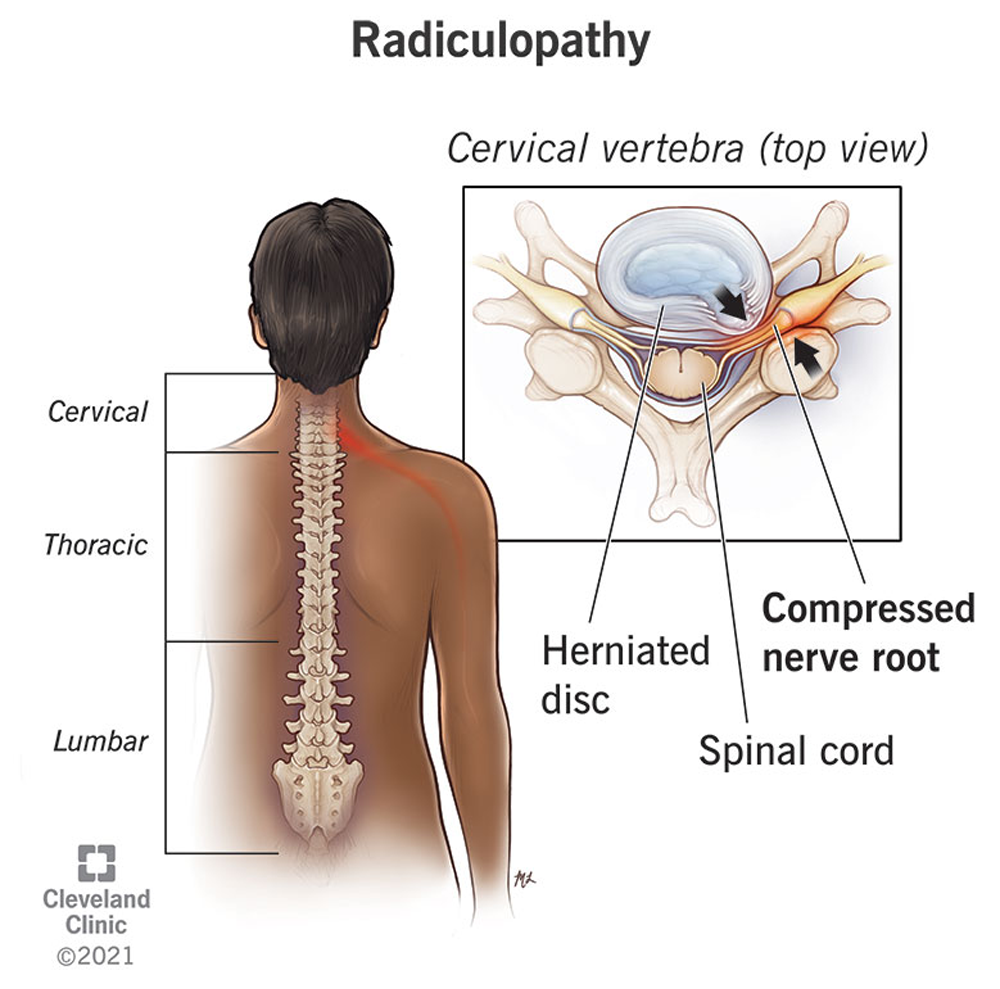
Radiculopathy is a well-defined neurological condition characterized by nerve-root irritation or compression, typically producing pain, sensory disturbance, or weakness in a predictable dermatomal or myotomal distribution. In clinical practice, however, many patients labeled as “radiculopathic” do not meet these criteria. Instead, they present with generalized, migrating or poorly localized limb symptoms that resist clean anatomical classification.
Despite this inconsistency, the presence of disc degeneration, bulging or herniation on imaging often becomes the dominant driver of diagnosis. This disc-centric approach assumes causality based on structural findings, even though numerous studies have demonstrated that asymptomatic individuals commonly exhibit significant disc pathology. When imaging findings are emphasized over clinical behavior, there is a risk of attributing symptoms to structures that may be incidental rather than causative.
The dermatomal model itself, while essential for neurological screening, represents a simplified construct. Sensory overlap, individual anatomical variation and central nervous system modulation frequently blur dermatomal boundaries. As a result, symptoms driven by non-neural tissues may mimic radiculopathy without reproducing classic dermatomal patterns.
This becomes particularly relevant when patients report diffuse pain, inconsistent paresthesia, or subjective weakness that fluctuates with movement, posture, or load rather than spinal position alone.

This series introduces subscapularis syndrome as a clinically relevant, yet underrecognized, contributor to non-dermatomal upper extremity symptoms.
Rather than positioning subscapularis syndrome as a replacement for established cervical diagnoses, it is presented as a critical addition to the differential diagnosis process, particularly in patients whose symptoms do not behave like true cervical radiculopathy despite the presence of imaging or orthopedic findings.
By framing piriformis and subscapularis syndromes within the broader concept of myogenic pseudo-radiculopathy, this series aims to improve diagnostic precision, guide conservative case management, and reduce unnecessary escalation toward invasive spinal procedures.
Each installment will build progressively – from foundational diagnostic principles to practical clinical application – providing clinicians with a structured framework for identifying when limb pain is driven by deep myogenic dysfunction rather than primary disc pathology.
Appreciating Non-Discogenic Contributors to Pain
True discogenic radiculopathy typically presents with a recognizable constellation of findings:reproducible dermatomal symptoms,
objective sensory loss,
myotomal weakness,
reflex changes, or
progressive neurological deficit.
When these findings are absent – or when symptoms fail to evolve in a predictable neurological manner – clinicians must resist the temptation to escalate care based solely on imaging abnormalities.
Failure to recognize non-discogenic contributors to radicular-like pain has meaningful clinical consequences. Patients may be directed toward epidural corticosteroid injections, nerve ablation procedures or surgical consultation despite limited evidence that these interventions address the primary pain generator. In such cases, outcomes are often inconsistent and symptoms may persist or recur, reinforcing a cycle of escalating intervention rather than diagnostic reconsideration.
Radicular-Like Symptoms Do Not Automatically Mean Radiculopathy
This series begins with a simple but critical premise: Radicular-like symptoms do not automatically equate to radiculopathy. Before invasive spinal procedures are considered, clinicians must first determine whether the presentation reflects true nerve-root pathology or a functional mimic.
Subsequent installments will introduce myogenic pseudo-radiculopathy as a framework for understanding these mimics, using piriformis syndrome as an established lower extremity model and subscapularis syndrome as an emerging upper extremity counterpart.
If radicular-like symptoms do not always represent true radiculopathy, the next question becomes unavoidable: What is actually driving these presentations?
Part 2 will introduce myogenic pseudo-radiculopathy as a functional framework for understanding non-dermatomal limb pain beyond disc-centric models.
References
Brinjikji W, et al.
Systematic literature review of imaging features of
spinal degeneration in asymptomatic populations.
Am J Neuroradiol, 2015 Nov;36(4):811-816.Chou R, et al.
Interventional Therapies, Surgery, and Interdisciplinary
Rehabilitation for Low Back Pain: An Evidence-based
Clinical Practice Guideline From
the American Pain Society
Spine (Phila Pa 1976) 2009 (May 1); 34 (10): 1066–1077Deyo RA, et al.
Overtreating Chronic Back Pain: Time to Back Off?
J Am Board Fam Med. 2009 (Jan); 22 (1): 62–68Gerwin RD.
Classification, epidemiology, and natural history
of myofascial pain syndrome.
Curr Pain Headache Rep, 2001 Oct;5(5):412-420.Jensen MC, et al.
Magnetic resonance imaging of the lumbar spine in
people without back pain.
N Engl J Med, 1994 Jul;331(2):69-73.Manchikanti L, et al.
Epidural interventions in the management of chronic
spinal pain: American Society of Interventional
Pain Physicians (ASIPP) comprehensive
evidence-based guidelines.
Pain Physician, 2021 Jan;24(S1):S27-S208.Bogduk N.
On the definitions and physiology of back pain,
referred pain, and radicular pain.
Pain, 2009 Dec 15;147(1-3):17-9.Travell JG, Simons DG.
Myofascial Pain and Dysfunction.
Baltimore: Williams & Wilkins, 1999.
Return to RADICULOPATHY
Since 4-01-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |