

Value of Chiropractic Services at
an On-site Health CenterThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Occupat Enviro Med 2012 (Aug); 54 (8): 917–921 ~ FULL TEXT
Curt A. Krause, DC; Lisa Kaspin, PhD; Kathleen M. Gorman, MPH;
Ross M. Miller, MD, MPH
From the Cerner Healthe Clinic
Kansas City, MO
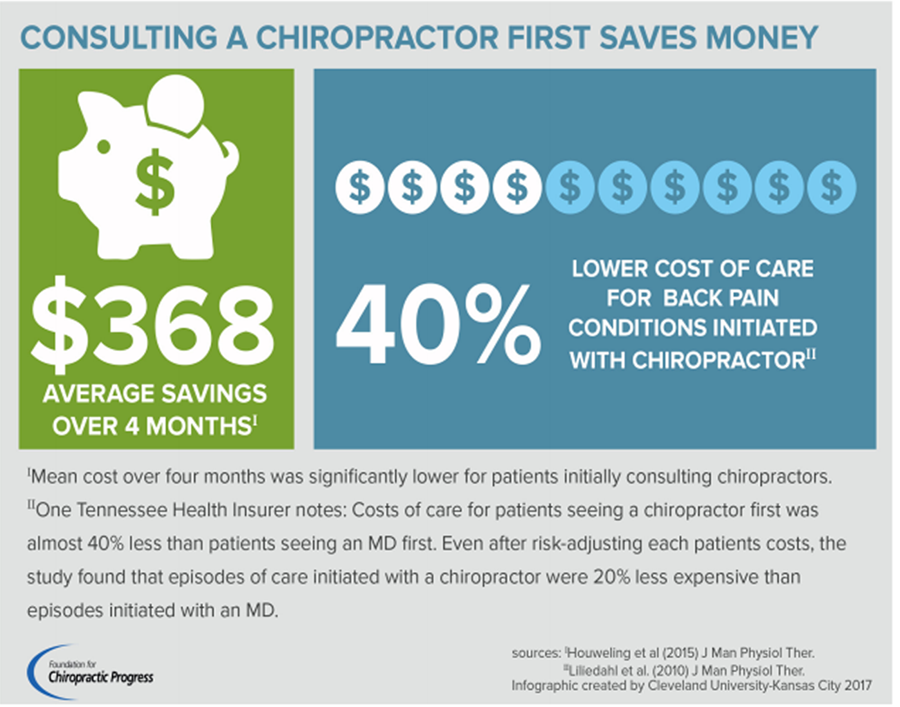
FROM: Houweling, JMPT 2015 Liliedahl, JMPT 2010
There has been conflicting research and an ongoing debate regarding the cost value of chiropractic. At the center of the debate is the question: Does chiropractic add to or reduce the total cost of care? The most recent and better designed studies suggest that chiropractic care can not only reduce the immediate cost of an episode of care, but reduce the recurrence of subsequent bouts of conditions such as low back pain. These musculoskeletal conditions are a heavy financial burden on society often requiring expensive tests to pinpoint the exact diagnosis.
This study, offering on-site chiropractic care, versus off-site physical therapy, concluded that “[These results suggest that] chiropractic services offered at on-site health centers may promote lower utilization of certain health care services, while improving musculoskeletal function.” Additionally, patients who receive chiropractic treatment often have a more conservative, less invasive treatment profile which can significantly reduce the overall cost of treatment.
Enjoy both these extra files:
The Exucutive Summary
The Study OutlineOBJECTIVE: Chiropractic care offered at an on-site health center could reduce the economic and clinical burden of musculoskeletal conditions.
METHODS: A retrospective claims analysis and clinical evaluation were performed to assess the influence of on-site chiropractic services on health care utilization and outcomes.
RESULTS: Patients treated off-site were significantly more likely to have physical therapy (P < 0.0001) and outpatient visits (P < 0.0001). In addition, the average total number of health care visits, radiology procedures, and musculoskeletal medication use per patient with each event were significantly higher for the off-site group (all P < 0.0001). Last, headache, neck pain, and low back pain-functional status improved significantly (all P < 0.0001).
CONCLUSIONS: These results suggest that chiropractic services offered at on-site health centers may promote lower utilization of certain health care services, while improving musculoskeletal function.
From the FULL TEXT Article:
Discussion
Although previous research has demonstrated the benefits of chiropractic care, to the best of our knowledge this study is the first to evaluate its impact when offered at an on-site health center. [6–10, 14–17] Given the convenience and quality of care provided by on-site health centers, it was hypothesized that on-site chiropractic care would be more beneficial than off-site clinic care. Despite some limitations that may have weakened the conclusions, the findings suggest on-site chiropractic services are associated with lower health care utilization of certain services and improved functional status of musculoskeletal conditions.
Specifically, patients receiving chiropractic care on-site were less likely to have a physical therapy visit (P < 0.0001) and outpatient visit (P < 0.0001). Moreover, the average total numbers of health care visits, radiology procedures, and musculoskeletal medication use per associate with each event were significantly lower for the on-site group (all P < 0.0001). Metz et al [18] assessed health plan members with and without chiropractic coverage and found that patients were directly substituting chiropractic care for medical care when it was available. Although all patients in our study had access to chiropractic care, the convenience of having it on-site may have eliminated the access barriers for patients who may have received other types of medical care instead. This trend is most evident in the finding that the on-site group averaged significantly fewer physical therapy and physician visits compared with the off-site group (both P < 0.0001), given that chiropractic care is a common alternative for both of these services. [18, 19]
Lower health care utilization among the on-site group may also be related to the characteristics of effective chiropractic care. On the basis of a large claims analysis, Legorreta et al [14] reported that chiropractic services were associated with less invasive, more conservative treatments. That is, patients with chiropractic coverage seemed to be avoiding more surgeries, hospitalizations, and radiographic imaging procedures. Similarly, Phelan et al [16] observed that chiropractic patients had lower utilization of ancillary medical services. In this study, associates who received care on-site were less likely to have an outpatient visit (P < 0.0001), but average utilization among associates who had a visit was similar between groups. This finding suggests that on-site chiropractic care may be lowering the occurrence of outpatient visits among associates on the cusp of requiring these services, but utilization is not affected for more serious cases.
Nonetheless, despite the reported benefits, in the literature there is also continued critique that chiropractic services can have variable quality and lack of adherence to evidence-based practice guidelines. [20–25] In particular, several reviews have described how the profession is divided into two types of practices: one faction maintains the use of nonscientifically supported techniques, whereas the other observes evidence-based guidelines. [20, 21, 23] Those who conform to the evidence-based approach perform services that are perceived as being more effective, better able to integrate with other health care services, and less likely to result in complications. [21–23] In addition, Hinton et al [25] performed a survey of chiropractors to assess their use of outcome measures in daily practice and found that the majority did not use psychosocial questionnaires or condition-specific disability indices to record changes in health status. Although this study did not measure the effectiveness or quality of chiropractic care off-site, given the on-site health center's focus on providing quality, effective, and holistic care, the lower health care utilization trends found in this study may be due to a greater adherence to evidence-based practices and integration with other health services on-site than off-site. Further investigation, however, is needed to fully understand the consistency and quality of off-site chiropractic care.
Further evidence of the on-site chiropractic care's effectiveness is the change in patient-reported functional status after treatment. That is, over the study period, there was a statistically significant decrease in the average HADI, NPDI, and OLBQ scores (all P < 0.001). Although a comparison with off-site cannot be made because the questionnaire data were not available for patients treated off-site, these findings confirm that on-site chiropractic care successfully improved patients' daily functioning. Previous research has shown that functional improvements resulting from chiropractic care increase the ability to perform work-related activities. [9]
The improved functional status found in this analysis indicates potential for reduced indirect costs, including absenteeism, presenteeism, and productivity losses, with on-site chiropractic services. Phelan et al 16 reviewed claims for musculoskeletal injuries treated by medical doctors and chiropractors. Treatment performed by chiropractors, on average, resulted in fewer lost workdays and lower workers' compensation payment.
In addition, direct cost savings may result through lower rates of health care utilization. Compared with alternatives, including physician visits, hospitalizations, and surgery, chiropractic care is considered a cost-effective treatment. [14–17] A retrospective analysis [14] of administrative claims data compared health plan members with and without chiropractic coverage, and found that annual medical care costs were 12% lower among members with chiropractic coverage due to less utilization of high-cost services.
Table 1.

CONCLUSION
The results of this study support the value of chiropractic services offered at on-site health centers. Offering patients evidence-based, integrative, and convenient care, treatment at on-site chiropractic services was associated with lower utilization of certain health care services, as well as improved functional outcomes. Future research into potential indirect and direct cost savings would supplement this study and further demonstrate the advantages of on-site chiropractic care.
References:
US Department of Health and Human Services. Centers for Disease Control and Prevention, National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD. Table 52. Severe headache or migraine, low back pain, and neck pain among adults 18 years of age and over, by selected characteristics: United States, selected years 1997–2009.
Available at: http://www.cdc.gov/nchs/data/hus/hus10.pdf#126. Accessed November 7, 2011
Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, Hollingworth W, et al.
Expenditures and Health Status Among Adults With Back and Neck Problems
JAMA 2008 (Feb 13); 299 (6): 656–664Centers for Disease Control and Prevention.
Prevalence and most common causes of disability among adults—United States, 2005.
Morb Mortal Wkly Report. 2009;58:421
Chapter 2. Spine: low back and neck pain. In: United States Bone and Joint Decade: The Burden of Musculoskeletal Diseases in the United States. Prevalence, Societal and Economic Cost. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008.
Available at:
http://www.boneandjointburden.org/pdfs/BMUS_chpt2_spine.pdf
Accessed November 8, 2011.
Centers for Disease Control and Prevention. Worker Health eChartbook. Number and percent distribution of nonfatal occupational injuries and illnesses and musculoskeletal disorders involving days away from work by number of days away from work, Private industry, 2007.
Available at: http://wwwn.cdc.gov/niosh-survapps/echartbook/Chart.aspx?id=1298&cat=568. Accessed February 5, 2012.
Hoiriis KT, Pfleger B, McDuffie FC, Cotsonis G, Elsangak O, Hinson R, et al.
A Randomized Clinical Trial Comparing Chiropractic Adjustments to Muscle Relaxants
for Subacute Low Back Pain
J Manipulative Physiol Ther 2004 (Jul); 27 (6): 388-398Vernon H, Humphreys K, Hagino C.
Chronic Mechanical Neck Pain in Adults Treated by Manual Therapy:
A Systematic Review of Change Scores in Randomized Clinical Trials
J Manipulative Physiol Ther 2007 (Mar); 30 (3): 215–227Roland Bryans, DC, Martin Descarreaux, DC, PhD, Mireille Duranleau, DC, Henri Marcoux, DC, Brock Potter, DC, Rick Ruegg, PhD, DC, Lynn Shaw, PhD, Robert Watkin, LLB, Eleanor White, DC
Evidence-Based Guidelines for the Chiropractic Treatment of Adults With Headache
J Manipulative Physiol Ther. 2011 (Jun); 34 (5): 274–289
Donald Aspegren, DC, MS, Brian A. Enebo, DC, PhD, Matt Miller, MD, Linda White, MD, Venu Akuthota, MD, Thomas E. Hyde, DC, James M. Cox, DC
Functional Scores and Subjective Responses of Injured Workers With Back or Neck Pain
Treated With Chiropractic Care in an Integrative Program:
A Retrospective Analysis of 100 Cases
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 765-771
Baldwin ML, Cote P, Frank JW, et al.
Cost-effectiveness Studies of Medical and Chiropractic Care for
Occupational Low Back Pain. A Critical Review of the Literature
Spine J. 2001 (Mar); 1 (2): 138–147Jacobson GP, Ramadan NM, Aggarwal SK, Newman CW.
Headache Disability Inventory (HDI): The Henry Ford Hospital Headache Disability Inventory (HDI)
Neurology. 1994 (May); 44 (5): 837-842
Hains F, Waalen J, Mior S.
Psychometric properties of the neck disability index
J Manipulative Physiol Ther. 1998 (Feb); 21 (2): 75-80
Fairbank JC, Couper J, Davies JB, O'Brien JP.
The Oswestry low back pain disability questionnaire
Physiotherapy. 1980;66:271–273
Legorreta, AP, Metz, RD, Nelson, CF, Ray, S, Chernicoff, HO, and Dinubile, NA.
Comparative Analysis of Individuals With and Without Chiropractic Coverage:
Patient Characteristics, Utilization, and Costs
Archives of Internal Medicine 2004 (Oct 11); 164 (18): 1985–1892Haas M, Sharma R, Stano M.
Cost-effectiveness of Medical and Chiropractic Care for Acute and Chronic Low Back Pain
J Manipulative Physiol Ther 2005 (Oct); 28 (8): 555–563Phelan S, Armstrong R, Knox D, Hubka M, Ainbinder D.
An Evaluation of Medical and Chiropractic Provider Utilization and Costs:
Treating Injured Workers in North Carolina
J Manipulative Physiol Ther 2004 (Sep); 27 (7): 442–448Smith J.
Fighting to help lower costs: making a financial case for chiropractic
J Chiropr Med. 2002;1:189–198
Metz, RD, Nelson, CF, LeBrot, T, and Pelletier, KR.
Chiropractic Care: Is It Substitution Care or Add-on Care in Corporate Medical Plans?
J Occup Environ Med 2004 (Aug); 46 (8): 847–855Chevan J, Riddle DL.
Factors associated with care seeking from physicians, physical therapists, or chiropractors by persons with spinal pain: a population-based study.
J Orthop Sports Phys Ther. 2011 (Jul); 41 (7): 467-476
Simpson JK.
The Five Eras of Chiropractic & the Future of Chiropractic
As Seen Through the Eyes of a Participant Observer
Chiropractic & Manual Therapies 2012 (Jan 19); 20 (1): 1Ernst E.
Chiropractic: a critical evaluation.
J Pain Symptom Manage. 2008 (May); 35 (5): 544-62
Jason W Busse, Janey Jim, Craig Jacobs, Trung Ngo, Robert Rodine, David Torrance, Abhaya V Kulkarni, Brad Petrisor, Brian Drew and Mohit Bhandari
Attitudes Towards Chiropractic: An Analysis of Written Comments
From a Survey of North American Orthopaedic Surgeons
Chiropr Man Therap. 2011 (Oct 4); 19 (1): 25Reggars J.
Chiropractic at the Crossroads or Are We Just Going Around in Circles?
Chiropractic & Manual Therapies 2011 (May 21); 19: 11Meeker, W., & Haldeman, S. (2002).
Chiropractic: A Profession at the Crossroads of Mainstream and Alternative Medicine
Annals of Internal Medicine 2002 (Feb 5); 136 (3): 216–227Dr. Paul M. Hinton, DC, FCCRS(C), Dr. Randall McLeod, DC, FCCRS(C), DACRB, Dr. Blaine Broker, DC, FCCRS(C), Dr. C. Elizabeth MacLellan, BSc, DC, FCCRS(C)
Outcome Measures and Their Everyday Use in Chiropractic Practice.
J Can Chiropr Assoc. 2010 (Jun); 54 (2): 118-131
Return to COST-EFFECTIVENESS
Since 8-14-2012
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |