

A Comparative Risk Assessment of Burden of Disease and
Injury Attributable to 67 Risk Factors and Eisk Factor
Clusters in 21 Regions, 1990-2010: A Systematic
Analysis for the Global Burden of Disease Study 2010This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Lancet. 2012 (Dec 15); 380 (9859): 2224–20260 ~ FULL TEXT
OPEN ACCESS Dr Stephen S Lim, PhD, Prof Theo Vos, PhD, Abraham D Flaxman, PhD, Goodarz Danaei, MD, Prof Kenji Shibuya, MD, Heather Adair-Rohani, MPH et al.
Institute for Health Metrics and Evaluation,
Seattle, WA 98121, USA.
stevelim@uw.edu
BACKGROUND: Quantification of the disease burden caused by different risks informs prevention by providing an account of health loss different to that provided by a disease-by-disease analysis. No complete revision of global disease burden caused by risk factors has been done since a comparative risk assessment in 2000, and no previous analysis has assessed changes in burden attributable to risk factors over time.
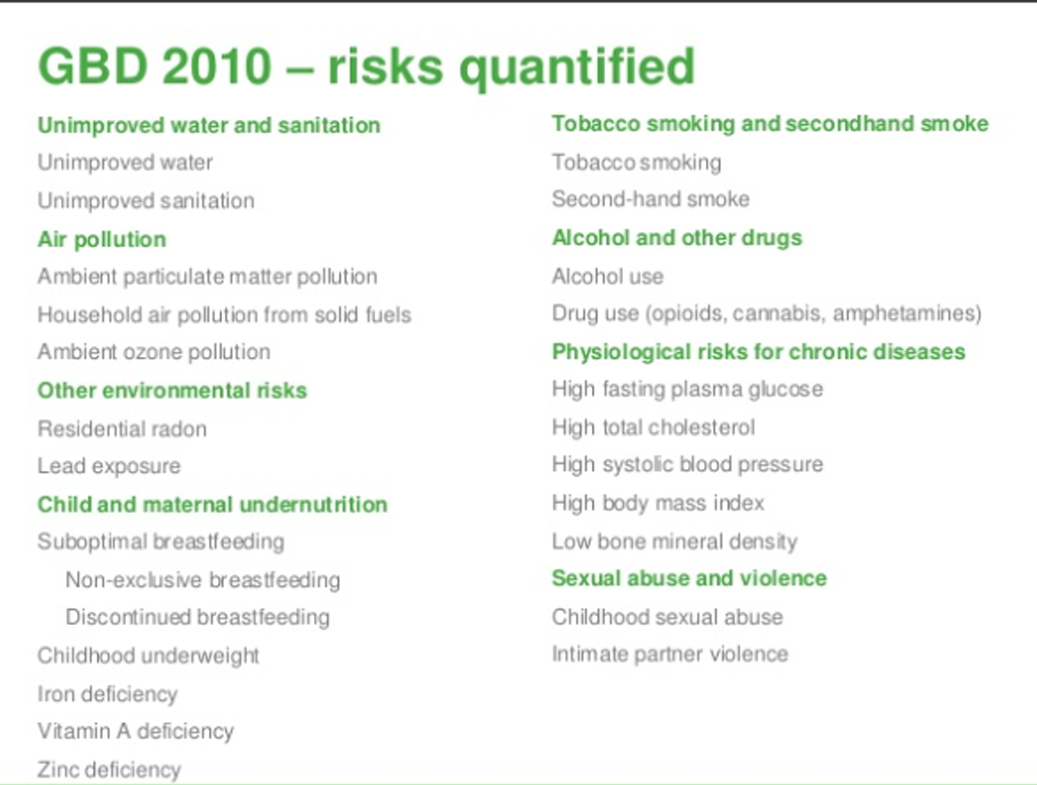
METHODS: We estimated deaths and disability-adjusted life years (DALYs; sum of years lived with disability [YLD] and years of life lost [YLL]) attributable to the independent effects of 67 risk factors and clusters of risk factors for 21 regions in 1990 and 2010. We estimated exposure distributions for each year, region, sex, and age group, and relative risks per unit of exposure by systematically reviewing and synthesising published and unpublished data. We used these estimates, together with estimates of cause-specific deaths and DALYs from the Global Burden of Disease Study 2010, to calculate the burden attributable to each risk factor exposure compared with the theoretical-minimum-risk exposure. We incorporated uncertainty in disease burden, relative risks, and exposures into our estimates of attributable burden.
FINDINGS: In 2010, the three leading risk factors for global disease burden were high blood pressure (7·0% [95% uncertainty interval 6·2-7·7] of global DALYs), tobacco smoking including second-hand smoke (6·3% [5·5-7·0]), and alcohol use (5·5% [5·0-5·9]). In 1990, the leading risks were childhood underweight (7·9% [6·8-9·4]), household air pollution from solid fuels (HAP; 7·0% [5·6-8·3]), and tobacco smoking including second-hand smoke (6·1% [5·4-6·8]). Dietary risk factors and physical inactivity collectively accounted for 10·0% (95% UI 9·2-10·8) of global DALYs in 2010, with the most prominent dietary risks being diets low in fruits and those high in sodium. Several risks that primarily affect childhood communicable diseases, including unimproved water and sanitation and childhood micronutrient deficiencies, fell in rank between 1990 and 2010, with unimproved water and sanitation accounting for 0·9% (0·4-1·6) of global DALYs in 2010. However, in most of sub-Saharan Africa childhood underweight, HAP, and non-exclusive and discontinued breastfeeding were the leading risks in 2010, while HAP was the leading risk in south Asia. The leading risk factor in Eastern Europe, most of Latin America, and southern sub-Saharan Africa in 2010 was alcohol use; in most of Asia, North Africa and Middle East, and central Europe it was high blood pressure. Despite declines, tobacco smoking including second-hand smoke remained the leading risk in high-income north America and western Europe. High body-mass index has increased globally and it is the leading risk in Australasia and southern Latin America, and also ranks high in other high-income regions, North Africa and Middle East, and Oceania.
INTERPRETATION: Worldwide, the contribution of different risk factors to disease burden has changed substantially, with a shift away from risks for communicable diseases in children towards those for non-communicable diseases in adults. These changes are related to the ageing population, decreased mortality among children younger than 5 years, changes in cause-of-death composition, and changes in risk factor exposures. New evidence has led to changes in the magnitude of key risks including unimproved water and sanitation, vitamin A and zinc deficiencies, and ambient particulate matter pollution. The extent to which the epidemiological shift has occurred and what the leading risks currently are varies greatly across regions. In much of sub-Saharan Africa, the leading risks are still those associated with poverty and those that affect children.
FUNDING: Bill & Melinda Gates Foundation.
Return to GLOBAL BURDEN OF DISEASE
Since 2-29-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |