

Burden of Disability Due to
Musculoskeletal (MSK) DisordersThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Best Pract Res Clin Rheumatol. 2014 (Jun); 28 (3): 353–366 ~ FULL TEXT
Lyn March, Emma U.R. Smith, Damian G. Hoy, Marita J. Cross, Lidia Sanchez-Riera, Fiona Blyth, Rachelle Buchbinder, Theo Vos, Anthony D. Woolf
University of Sydney Institute of Bone and Joint Research,
and Royal North Shore Hospital,
St Leonards, NSW, Australia.
This chapter summarises the global and regional prevalence, disability (Years Lived with Disability (YLDs)) and overall burden (Disability Adjusted Life Years (DALYs)) and costs for the common musculoskeletal disorders including low back and neck pain, hip and knee osteoarthritis, rheumatoid arthritis, gout, and a remaining combined group of other MSK conditions. The contribution of the role of pain in disability burden is introduced. Trends over time and predictions of increasing MSK disability with demographic changes are addressed and the particular challenges facing the developing world are highlighted.
KEYWORDS: Burden; Costs; DALYs; Developing countries; Global trends; MSK disorders; Pain; Prevalence; YLDs
From the FULL TEXT Article:
Introduction
Over the past century, global health priorities in health have been largely focussed on communicable diseases. With the world's population growth, increased average age and decreased death rates [1], people are now living longer and becoming increasingly susceptible to non-communicable diseases, including musculoskeletal (MSK) disorders. In the recent Global Burden of Disease (GBD) 2010 Study, the burden disability of all MSK disorders was estimated in 187 countries and 21 regions of the world for the years 1990 and 2010. In the burden estimates, there were five major defined conditions and all other MSK disorders (the rest) captured in a group titled ‘other MSK disorders’.
The defined conditions were(1) osteoarthritis (OA),
(2) rheumatoid arthritis (RA),
(3) gout,
(4) lowback pain (LBP) and
(5) neck pain (NP).Throughout the world, the prevalence and burden from MSK conditions were exceptionally high. [2–10] Globally, all MSK disorders combined accounted for 21.3% of the total years lived with disability (YLDs), second to mental and behavioural problems (23.2%). [2, 11]When taking into account both death and disability, all MSK disorders combined accounted for 6.7% of the total global disabilityadjusted life years (DALYs), which was the fourth greatest burden on the health of the world's population (third greatest in developed countries). [2, 11] Out of the 291 conditions studied, LBP ranked first (highest) for disability (YLDs) and sixth for the overall burden (DALYs). For NP, the condition ranked fourth highest for YLDs and 21st for DALYs. ‘Other MSK disorders’ ranked sixth highest for YLDs and 23rd for DALYs. OA, RA and gout were also significant contributors to the global disability burden.
Osteoporosis represented by low bone mineral density (BMD) was included in the GBD 2010 Study for the first time as one of the 67 risk factors studied. Population-attributable fractions (PAFs) were determined for low BMD as a risk factor for fractures. Additionally, PAFs were also determined for occupation as a risk factor for LBP, and elevated body mass index as a risk factor for LBP and OA. In this chapter, aspects related to the burden of disability due to MSK disorders are described, including the prevalence, disability and role of pain related to disability, costs associated with MSK disorders and predictions of increasing MSK disability with demographic changes and socio-economic impact.
Prevalence of musculoskeletal disorders
The prevalence and incidence of a series of MSK disorders reported in population-based epidemiological studies were systematically reviewed and published. [12–19] In the GBD 2010 Study, extensive systematic reviews of the prevalence of each of theMSK disorders (knee and hip OA, RA, LPB, NP, gout and otherMSK disorders) were conducted fromthe years 1980 to 2009. [3–6, 9, 10] Searches were carried out in MEDLINE, EMBASE, CINAHL, CAB abstracts, WHOLIS and SIGLE databases, with no age, gender or language restrictions. The datawere required to be population based and were excluded if they were not representative of the general population. For some conditions, prevalence data from a number of data sets, including world health surveys and national health surveys, were also included. Some variability observed in the datawere the case definition used, age groupings and the reported prevalence periods. In addition, there were some missing data for specific age groups, regions and years of interest.
To deal with these challenges and to estimate the prevalence rates for each of the world regions, a Bayesian meta-regression tool, DisMod-MR [20], was utilised. The tool was developed by the GBD core team, at the Institute for Health Metrics and Evaluation (IHME), University ofWashington, Seattle,WA, USA. It was used to pool heterogeneous data presented in different age groups, to adjust data for methodological differences, to check data for internal consistency and to predict values for countries and regions with little or no data. DisMod-MR produced a full set of age/sex/region/year-specific estimates for prevalence. Using the available data from the systematic reviews and population-based data sets, age-standardised prevalence estimates were modelled for the years 1990 and 2010. The prevalence estimates for the MSK disorders within each of the 21 world regions are shown below.
Low back pain
LBP was defined as pain in the area on the posterior aspect of the body from the lower margin of the 12th rib to the lower glutaeal folds with or without pain referred into one or both lower limbs that lasts for at least 1 day. The global age-standardised point prevalence of LBP in 2010 was estimated to be 9.4% (95% confidence interval (CI) 9.0–9.8). The prevalence was higher in males (mean: 10.1%; 95% CI 9.4–10.7) compared with females (mean: 8.7%; 95% CI 8.2–9.3), and peaked at approximately 80 years of age. The prevalence did not change significantly from 1990 to 2010.
Neck pain
NP was defined as pain in the neck with or without pain referred into one or both upper limbs that lasts for at least 1 day. Unlike LBP, the prevalence of NP was higher in females (mean: 5.8%; 95% uncertainty interval (UI): 5.3–6.4) than in males (mean: 4.0%; 95% UI: 3.7–4.4), with the prevalence peaking at a much younger age of 45 years. The global point prevalence of NP in 2010 was estimated to be 4.9% (95% UI: 4.6–5.3), and it did not change significantly from 1990 to 2010.
Osteoarthritis
The OA (knee and hip combined) global prevalence was estimated to be 3.8% (95% UI: 3.6–4.1). A higher prevalence was seen in females (mean 4.8%; 95% UI 4.4–5.2) than in males (mean 2.8%; 95% UI 2.6–3.1). Radiographically confirmed symptomatic knee OA was a common condition with prevalence rising with age, peaking at the age of 50 years. The prevalence was higher in females (mean 0.98%; 95% UI 0.82–1.29) than in males (mean 0.70%; 95% UI 0.58–0.90). Hip OA prevalence was also observed to increase consistently with age, although it was less common than knee OA. Globally, the prevalence of hip OA in 2010 was estimated to be 0.85% (95% UI 0.74–1.02).
Rheumatoid arthritis
The optimal definition of RA used was the American College of Rheumatology 1987 criteria. RA is not as common as OA and NP. The prevalence was estimated to be 0.24% (95% CI 0.23–0.25) and was observed to increase with age. Similar to OA, the prevalence of RA was higher in females (mean 0.35%; 95% CI 0.34–0.37) than in males (mean 0.13%; 95% CI 0.12–0.13). No discernable change in prevalence from 1990 to 2010 was detected.
Gout
Gout, as defined by the American Rheumatism Association 1977 criteria, is a disease that is more common in males (mean: 0.125%; 95% UI 0.116–0.136) than in females (mean: 0.032%; 95% UI 0.030–0.035). The global prevalence of gout in 2010 was 0.076% (95% UI 0.072–0.082). The prevalence increased steadily from the age of 30 years; however, relative to males, there is a low prevalence of gout in females before the age of 45 years, which could be explained by the link between menopause and gout. [21]
Other MSK disorders
All other MSK disorders (the rest) undefined in the GBD 2010 Study were captured in a group titled ‘other MSK disorders’. The global prevalence of other MSK disorders was estimated to be 8.4% (95% UI 8.1–8.6) in 2010. The prevalence increased with age to a plateau of 20–40% at age 80, and was slightly higher in females (mean 8.7%; 95% UI 8.4–9.1) than in males (mean 8.0%; 95% UI 7.7–8.3). There was no significant change in prevalence estimates from 1990 to 2010.
Summary
With the exception of LBP and gout, MSK disorders predominantly affect females more than males. The prevalence of MSK disorders largely increased with age. However, DisMod-MR modelling used in the GBD 2010 Study did not produce evidence of a change in the age-standardised prevalence between 1990 and 2010 for any of the MSK conditions. This was unexpected as the increasing obesity rates and ageing of the world's population would likely suggest the increased MSK prevalence. Possible explanations could be the modelling process within DisMod-MR, the heterogeneity of all available data input, and that the 20-year period was not sufficient to detect an increase, or that there was, in fact, no increased prevalence over this time period.
Age is one of the common risk factors for all MSK conditions, and the prevalence estimates indicate that rates increase with age. The prevalence of MSK disorders in low- and middle-income countries has been highlighted, and it has been reported that the greatest increase in the ratio of older to younger people will take place in these less developed countries. [22] By 2050, an estimated 3.53 billion people 40 years or older will be living in low- and middle-income countries compared to 645 million people in high-income countries. [22] In addition to this ageing population, many of the risk factors associated with the MSK conditions in high-income countries are also likely to become more common exposures in low- and middle-income countries. Work demands are extensive in subsistence communities, and studies have found that activities such as the collection of water and farming activities can increase the risk of low back and knee pain. [23–25] The increasing proportion of older populations, with increasing prevalence of MSK conditions in less developed countries, is expected to become a major global health problem in the coming decades.
For some MSK conditions in the GBD 2010 Study, there was considerable methodological variation among population-based studies relating to the prevalence period, case definition used and the way the results were reported. Researchers are strongly encouraged to adopt international recommendations for defining MSK conditions. [26–30] This applies both to MSK-specific surveys and, more importantly, to general health and disability surveys. This practice will greatly enhance the validity and comparability of future estimates of the prevalence for MSK disorders.
Disability related to MSK disorders
DALY is the standard metric used to measure the overall burden of diseases. [31] DALY consists of fatal and non-fatal components, namely years of life lost due to premature mortality (YLLs) and YLDs, respectively. Disability weights (DWs) are required to derive the YLDs. Together with the description of disability related to all MSK disorders, these interrelated units of measurement used to quantify the disability are briefly explained.
Disability weights
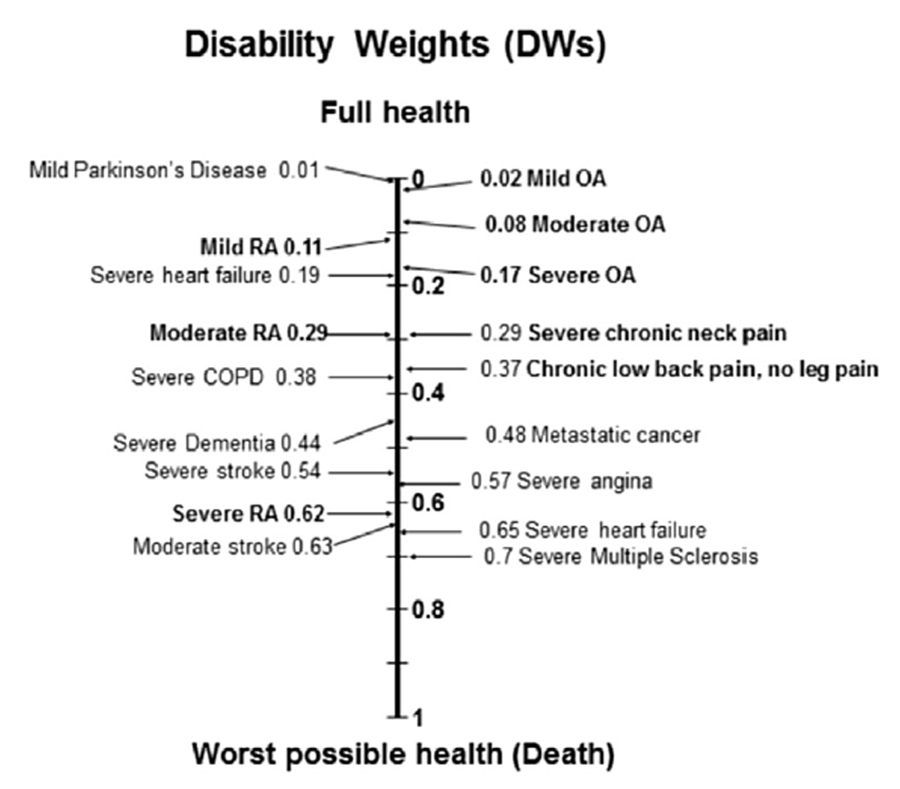
The MSK Expert Group identified the main disabling sequelae for each MSK condition through a series of systematic reviews. [12–19] Sequelae refer to consequences of diseases and injuries, particularly the different levels of disease severity. The sequelae of MSK conditions were represented by the health states described in lay terms, according to a specific set of health domains. These were chosen and defined according to the condition's natural history and the main functional states associated with the condition, as well as the availability of sufficient epidemiological data to estimate prevalence. The MSK health-state descriptions [7] were designed to reflect the average case for the particular health state in the general population. These lay descriptions were then used in the GBD DW Measurement Survey 2010. Large-scale household surveys and an openaccess web-based survey were conducted by a DW group to produce a comprehensive set of DWs for the GBD 2010 Study. [32] The set of DWs produced were required for the calculation of YLDs. DWs reflect the level of severity of each health state on a continuum from zero (equivalent to full health) to one (equivalent to death). Some DWs of the MSK health states are shown in the diagram below.
Years lived with disability
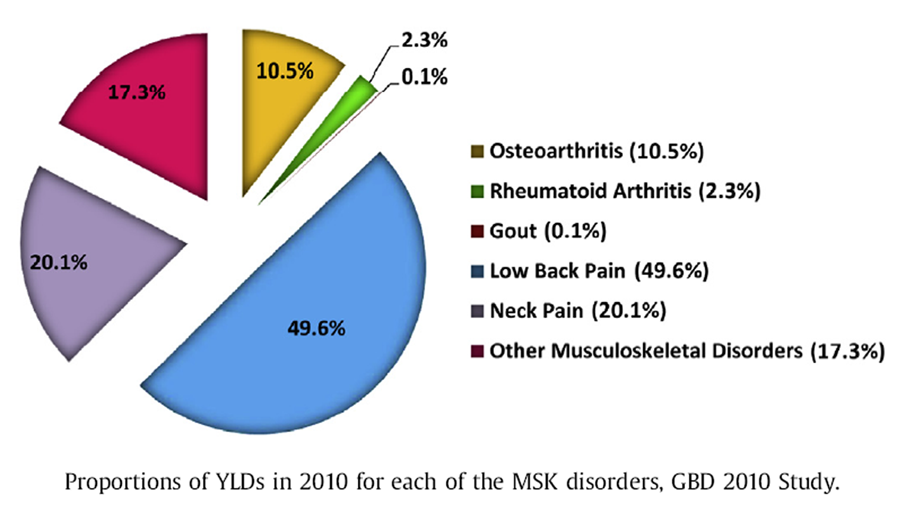
YLDs quantify disease disability related to any short-term or long-term health loss. For each MSK condition studied, YLD was calculated by multiplying the average DW with the DisMod-MR-generated prevalence estimates. [7] A correction for co-morbidity was applied in the calculation using simulation methods to get co-morbidity-adjusted YLD estimates. Detailed global disability (YLDs) and the breakdown of YLD estimates in 21 world regions of eachMSK disorder for both 1990 and 2010were recently reported. [2–10] The proportions of the global disability burden (YLDs) in 2010 for eachMSK disorder are shown in the pie chart below (the calculation was based on the data extracted from http://www.healthdata.org/ results/data-visualizations in August 2014). About half of the total disability burden (49.6%) was from LBP.NP (20.1%), otherMSK disorders (17.3%) andOA (10.5%) also caused substantial disability burden. There was a relatively small amount of burden from RA (2.3%), with the least burden contributed by gout (0.1%).
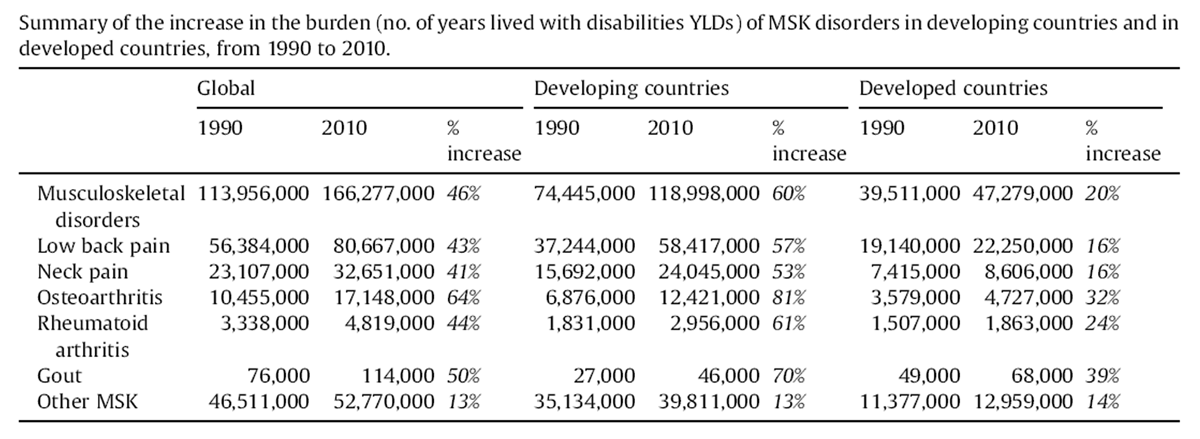
For the years 1990 and 2010, the global YLDs and YLDs of 21 world regions due to all MSK disorders combined for males and females in all ages, reported in millions with 95% uncertainty interval (UI), are shown in the table below(the data extracted in August 2014 from http://www.healthdata.org/results/datavisualizations). Over the span of 20 years, the global YLDs of all the MSK disorders were on the rise, approximately by 45% from 1990 to 2010, for both males and females. Among the 21 GBD 2010 regions, the largest increases of the disabilityestimateswere observed in SouthAsia (increased by 12.1 million), followed by East Asia (increased by 10.6 million). In terms of proportion, the YLDs in Oceaniaweredoubled,with 100% increase from 1990 to 2010 although the actual amount of the YLDs was, in fact, the smallest. The proportional increases were also remarkably high in central sub-Saharan Africa (87.5%), North Africa and Middle East (80.7%) and east sub-Saharan Africa (75.8%). The least increasewas noted in Eastern Europe (4.5%).
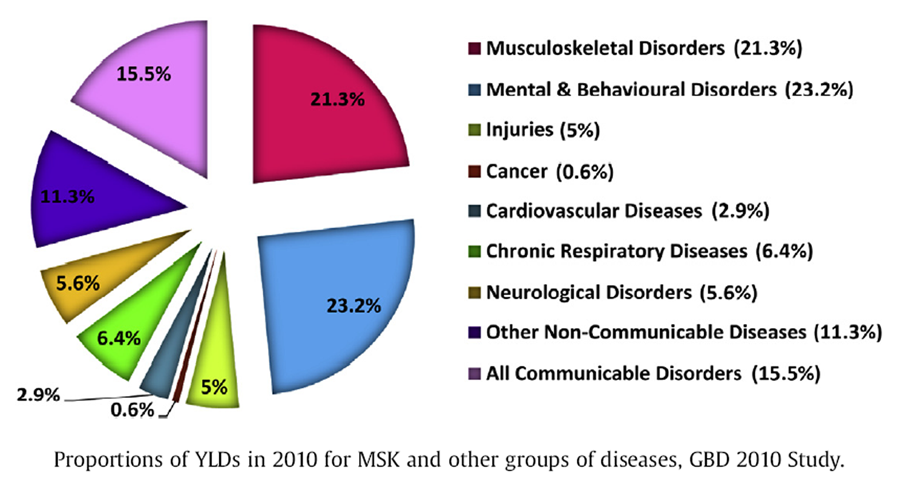
To compare with the other groups of diseases, the proportions of the global disability burden (YLDs) in 2010 for all the MSK disorders combined and other groups of diseases in the GBD 2010 Study are shown in the pie chart below (the calculation was based on the data extracted from http://www. healthdata.org/results/data-visualizations in August 2014). ‘All Communicable Disorders’ refers to communicable, maternal, neonatal and nutritional disorders. ‘Other Non-Communicable Diseases’ is the remaining category of all other unspecified non-communicable diseases in the GBD 2010 Study captured and put together in a group. In 2010, all MSK disorders combined accounted for 21.3% of the total YLDs, globally, second to mental and behavioural disorders (23.2%).
Disability-adjusted life year
DALY is the standard metric used to quantify burden [31], defined as years of healthy life lost. DALYs are the sum of YLLs and YLDs, that is, any short- or long-term health loss. One DALY equals one lost year of healthy life. Among the burden estimates of all the MSK conditions in the GBD 2010 Study, RA and other MSK disorders were the only two conditions with the YLL component for the DALY estimate. Where there was no evidence for cause-specific mortality associated with the disease, YLD and DALY estimates for the disease reported in the GBD 2010 Study were the same. Particularly, this applied to the MSK conditions studied, with the exception of RA [3] and other MSK disorders. [10]
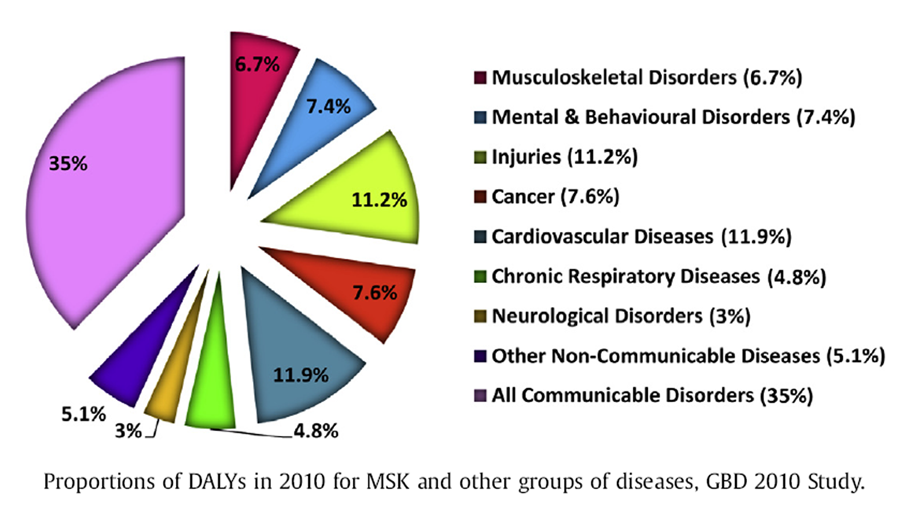
Detailed global DALYs and the breakdown of DALY estimates in 21 world regions of each of the MSK disorders for both 1990 and 2010 were recently reported. [2–10] The proportions of the overall global burden of diseases (DALYs) in 2010 for all the MSK disorders combined compared to the other groups of diseases in the GBD 2010 Study are shown in the pie chart below (the calculationwas based on the data extracted from http://www.healthdata.org/results/data-visualizations in August 2014). In the year 2010, when both YLLs and YLDs were taken into account, all MSK disorders contributed 6.7% to the total overall global burden of diseases.
Role of pain in disability
The experience of episodes of site-specific pain, defined by the average duration (number of hours per episode) and average frequency (number of days per week that these episodes were experienced), was used in the MSK health-state descriptions that were used to derive DWs and calculate YLDs for all of the common MSK conditions identified by systematic reviews of the epidemiological literature. There was significant variability in population studies in defining and characterising the course of episodes of pain over time, and future studies of the natural history and typical trajectories over time of pain episodes are needed, particularly in low- and middle-income countries.
In the GBD 2010 Study, LBP and NP were key contributors and drivers of global disability burden (highest and sixth highest rank causes contributing to global YLDs, respectively). The inclusion of two common regional MSK pain conditions (neck and LBP) in the GBD 2010 Study was an important step in improving the estimation of the global burden of MSK disorders. The inclusion of additional regional MSK pain conditions particularly common in low- and middle-income countries, such as knee pain, should be considered in future.
The identification of people with MSK pain conditions at a population level in the epidemiological literature includes both ‘disease-specific’ approaches, for example, examining the relationship between pain and disability in people with diagnosed OA, and more ‘pain-focussed approaches’ that characterise MSK pain conditions independent of a formal diagnosis of an MSK disorder. The latter approach is especially relevant in low- and middle-income countries, where access to health care (and hence a diagnosis) is limited, yet the life impact of pain-related disability is likely to be high.
Contribution of low BMD to falls and fractures
In the GBD 2010 Study, low BMD was defined as a risk factor and grouped within the MSK disorders. The contribution of low BMD to the burden of fractures due to falls was limited to populations aged 50 years or older, as osteoporotic fractures have little burden at younger ages in the general population. [7] Fractures due to osteoporosis formed a proportion of the global burden from falls. This proportion, however, was likely to be significantly underestimated, influenced by a number of aspects related to the data available/gathered for the estimate. [33] Nonetheless, the calculated population-attributable fractions (PAFs) demonstrated that low BMD is an increasing global health burden. In 2010, low bone density accounted for 0.21% of global DALYs which represented a 75% increase from 0.12% in 1990. Asia East and South were the major contributors to the increase in global burden. [8]
Costs associated with MSK disorders
MSK disorders have a great cost to individuals and society through the associated disability as well as health-care needs. Most costs are associated with their impact on activities of daily living, in particular on productivework along with the need for social support rather than health-care costs. The costs of support may be borne by the welfare system or by family and carers depending on systems of social care. The costs are easiest to quantify when the health and social costs are borne by the state or another third party, and it is much more challenging to put a monetary value on disability in countries, commonly low to middle income, where the cost falls on the family who provide support.
There are several national cost-of-illness studies in developed countries within which the costs related to MSK conditions can be identified. These reflect the expenditure on health care for the management of these conditions, and some also include their societal costs. These costs reflect the current provision of health and social care for people with these conditions, and do not measure the unmet need due to lack of provision of adequate services, such as access to joint arthroplasty for OA or biologic therapy for RA. An examination of comparable studies shows that between 5.4% and 12.6% of health expenditure was attributable to MSK conditions. [34] In Ireland, the General Medical Services Scheme expenditure on drugs, medicines and appliances for conditions relating to the MSK system in 2008 was 67.14 million Euros (5.86% of total expenditure). The expenditure on drugs for MSK conditions was 3048 million Euros (6.01% of total drug expenditure).
In 2006, the Belgian Federal Knowledge Centre in Healthcare (KCE) estimated the direct cost of back pain in Belgium to be 272 million Euros. [35] In the UK, the estimated cost of general practitioner (GP) consultations for diseases of the MSK system in 2003 was Ł1340 million; only the costs of diseases of the respiratory system (Ł1790 million) and diseases of the circulatory system (Ł1350 million) were higher. In the USA, the annual average direct cost, in 2006 dollars, was estimated to be $US576 billion, equivalent to 4.5% of the national gross domestic product (GDP). [36] These costs relate to ambulatory visits, surgery, rehabilitative interventions and drugs. Some are easier to collate such as drugs, surgery and inpatient care, but the costs due to ambulatory visits and community care are often underestimated.
Many MSK problems are managed predominantly in primary care and account for 10–18% primary-care consultations. [37] In the UK, in 2006, 10.1 million patients consulted their GP at least once for MSK problems. This means that one in four of the registered population and one in seven of all recorded primary-care consultations during 2006 were for an MSK problem. Back problem was the most common reason for consultation, followed by problems with the knee, chest and neck. [38] They are also a common reason for visits to therapists, and short- and long-term use of drugs, mainly analgesics. In a large-scale pan-European survey, when asked about their reasons for long-term medical treatment, 24% stated that it was for long-standing problems with muscles, bones and joints. [39] The effective use of biologic drugs to control RA and prevent disability has resulted in their widespread use, mainly limited by affordability of individuals or health-care systems. Joint replacement surgery is a major and increasing cost. At present, accessibility is inconsistent across the globe but, with increasing need and wealth, the main limitation will be the skilled workforce to perform the procedure.
The cost of individual disease has been estimated. A report of the UK National Audit Office in 2009 estimated that RA health-care costs in England amounted to Ł560 million per year. [40] The annual excess health-care costs of RA patients in the USA have been estimated to be $8.4 billion in 2005 dollars. [42] In Europe, the cost of RA has been estimated for 2006 to be 45 million Euros [42], with an estimated average annual cost per patient of 13,000 Euros. The medical cost excluding drugs was nearly 9.5 million Euros. The direct costs of illness in a patient with advanced OA of the hip and knee in Austria, estimated by a self-administered questionnaire covering the period of 12 months prior to joint replacement, were 2,747 Euros. [43] The medical costs amounted to 1,148 Euros and non-medical costs 1,599 Euros associated with personal care and household assistance required due to severe loss of function. Back pain is the greatest cause of disability, but its costs are predominantly related to work loss. In addition, there is the out-of-pocket expenditure incurred by people affected by an MSK problem, which includes their contribution to health-care costs and complementary therapies they may use. This is a significant cost for these long-term conditions where conventional therapy does not always achieve people's expectations of health improvement.
The disability associated with MSK disorders needs support from family, carers and society. There may need to be adaptations to enable independent activities with associated economic impacts. If support is given by the family, then they may be prone to income loss. Impact on work is one of the greatest costs to individuals and society. MSK conditions are one of the greatest causes of loss of productivity and economic independence through absenteeism (time off work for those in paid work), presenteeism (lost productivity because of diminished capacity while at work) and work disability (permanent partial or complete disablement for work purposes). In the USA, 13% of the total workforce experienced a loss in productive time during a 2–week period due to common pain conditions such as arthritis, back, headache and other MSK pain. [44] The majority (76.6%) of lost productive time was explained by reduced performance while at work, and not by work absence. It is estimated that the indirect cost of MSK diseases for persons aged 18–64 years with a work history was $US 373.1 billion or 2.9% of the GDP in 2004–2006. [36] In Europe, one in four workers cite problems with backache and more than one in five claim to suffer from muscular pain in the shoulders and neck or limbs. [45] MSK disorders constitute 38% of occupational diseases [46], and, of those workers reporting a work-related problem in the past 12 months, 60% was due to MSK problems. [47]
In the UK, 131 million days were lost due to sickness absences in 2013, and 31 million days were lost to back, neck and muscle pain, and this was more than any other causes. [48] In Germany, back pain causes the longest periods of inability to work. In 2008, it was ranked number one with >14 million recorded days of inability to work. [49] The estimated productivity loss due to MSK conditions was 95 million days lost (23.7% of total days lost) at a cost of 23.9 billion Euros or 1.1% of the gross national product (GNP) for 2006. [50] In Austria, 35% of all new disability pensions in 2001 were due to MSK disorders. [51] In the UK, 38% of those claiming Disability Living Allowance (a benefit for people <65 years who are so disabled as to have personal care needs and/or mobility) in 2010 were doing so because of MSK conditions. [52]
MSK disorders cost the European Union (EU) from 0.5% to 2% of GDP annually. [53] Studies from several European countries (which often have disease registries that allow one to track employment status by the presence of chronic conditions) reported that the increasing severity of MSK disorders increases the propensity of workers to retire earlier. [54] A study of workers aged 50–65 years in the UK reported that, after controlling for demographics, economic well-being, and various measures of health status, a person's reported difficulty walking a quarter of a mile, especially when symptoms included lower limb pain and/or shortness of breath, was predictive of early work exit (odds ratio = 2.23). [55]
In summary, the increase in the prevalence and impact of MSK disorders with age will have an impact on the ability of extending people's working lives, which is occurring in many societies in response to increased longevity.
Predictions of increasing MSK disability with demographic changes and socio-economic impact

From 1990 to 2010, the burden attributable to MSK disorders increased by 46%. This increase in DALYs was relatively consistent across MSK conditions (range: 41–64%), except for ‘other MSK conditions’, which increased by 13%.
The increase in the burden of MSK conditions was due to population growth and ageing [2–6, 9, 10] A cause for great concern is that population growth, ageing and other risk factors for the burden of MSK conditions will increase dramatically over the coming decades, particularly in developing countries. The global population is predicted to increase by 38% from 2010 (6.9 billion) to 2050 (9.5 billion). [56] In developing countries, the increase is predicted to be 45% from 5.7 to 8.2 billion, and in developed countries the increase is predicted to be 5% from 1.2 to 1.3 billion. [56]
Age is one of the most common risk factors for MSKs. [13] In 2010, there were 2.3 billion people over the age of 40 years: 1.7 billion in developing countries and 0.62 billion in developed countries. This is predicted to increase by 87% by 2050, where it is estimated that there will be 4.3 million over the age of 40 years, globally, with 3.6 billion in developing countries (a 112% increase) and 0.72 billion in developed countries (a 16% increase). [56] By 2050, there will be five times as many people over the age of 40 living in developing countries compared to wealthier countries. [22] A demographic change has occurred gradually in most of the developed world following steady socio-economic growth over several decades. [57] However, in many developing countries, the demographic change is taking place over just two or three decades, and, thus, health systems and national economies are ill-equipped to deal with the change.
Other risk factors associated with MSK disorders include obesity, increased motorisation and workrelated issues. [12, 13] Many of these are present in both developed and developing countries. Kelly et al. [58] estimated that, in 2005, 9.8% (95% CI: 9.6–10) of the world's adult populationwas obese, and this translated to 396 million (95% CI: 388 to 405 million) people. They predicted that, by 2030, this number would increase to 573 million to 1.12 billion people, depending on whether secular trends were utilised or not in their analysis. While developed countries had a higher proportion of obese adults compared to developing countries, the actual and predicted number of obese individuals in developing versus developed countries was much larger. The study concluded that the epidemic of obesity in developing countries is and will continue to be heavily influenced by population growth and ageing, urbanisation and lifestyle changes, including increased calorie intake and low levels of physical activity.
The levels of motorisation are on the rise and this is resulting in larger numbers of motor accidents [59], and these are often consequent whiplash-associated disorders and other motor vehicular-related trauma. In developing countries, it is estimated that 80–90% of the population are involved in ‘heavy work’. [60] In subsistence communities, work demands are extensive and activities such as the collection of water and farming have been shown to increase the risk of LBP. [23, 24] Urban areas are seeing rapid industrial growth, and the prevalence of occupational MSK conditions is already very common. [61]
As a consequence of all the factors mentioned above, the number of people suffering from MSK disorders throughout the world will increase dramatically over the coming decades, and this will result in an exponential increase in the burden from MSK disorders. This impact will be particularly profound in developing countries and has the potential to decimate national economies. Health promotion and treatment services in these countries do not receive the resources seen in high-income developed countries, and health insurance and social security frequently do not exist. Moreover, a large proportion of those affected are in the most productive years of life when functioning is often a necessity to support both younger and older family members.
Sensible and practical planning for this increase is critical. The pace of the demographic and epidemiological change in developing countries necessitates a forward-looking approach to endeavouring to reduce this future burden. Research to assess the most effective and affordable strategies for the prevention and management of the burden from MSK disorders is urgently needed.
References:
Lozano R, Naghavi M, Foreman K, et al.
Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010:
a systematic analysis for the Global Burden of Disease Study 2010.
Lancet 2013 Dec 15;380(9859):2095–128.Murray CJ, Vos T, Lozano R, et al.
Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010:
a systematic analysis for the Global Burden of Disease Study 2010
Lancet 2013 Dec 15;380(9859):2197–223.Cross M, Smith E, Hoy D, et al.
The global burden of rheumatoid arthritis: estimates from the Global Burden of Disease 2010 Study.
Ann Rheum Dis 2014;73:1316–22.Cross M, Smith E, Hoy D, et al.
The global burden of hip and knee osteoarthritis:
estimates from the Global Burden of Disease 2010 Study.
Ann Rheum Dis 2014;73:1323–30.Hoy D, March L, Brooks P, et al.
The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 study
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Hoy D, March L, Woolf A, et al.
The Global Burden of Neck Pain: Estimates From the Global Burden of Disease 2010 Study.
Ann Rheum Dis. 2014 (Jul); 73 (7): 1309–1315Hoy D, Smith E, Cross M, et al.
The Global Burden of Musculoskeletal Conditions for 2010: An Overview of Methods
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Sanchez-Riera L, Carnahan E, Vos T, et al.
Global burden attributable to low bone mineral density.
Ann Rheum Dis 2014; 73:1635–45.Smith E, Hoy D, Cross M, et al.
The global burden of gout: estimates from the Global Burden of Disease 2010 Study.
Ann Rheum Dis 2014;73:1470–6.Smith E, Hoy D, Cross M, et al.
The Global Burden of Other Musculoskeletal Disorders:
Estimates From the Global Burden of Disease 2010 Study
Ann Rheum Dis. 2014 (Aug); 73 (8): 1462–1469Vos T, Flaxman AD, Naghavi M, et al.
Years Lived with Disability (YLDs) for 1160 Sequelae of 289 Diseases and Injuries
1990-2010: A Systematic Analysis for the Global Burden of Disease Study 2010
Lancet. 2012 (Dec 15); 380 (9859): 2163–2196Hoy DG, Bain C, Williams G, et al.
A systematic review of the global prevalence of low back pain.
Arthritis Rheum 2012; 64(6):2028–37.Hoy DG, Brooks P, Blyth F, et al.
The epidemiology of low back pain.
Best Pract Res Clin Rheumatol 2010;24(6):769–81.Hoy DG, Protani M, De R, et al.
The epidemiology of neck pain.
Best Pract Res Clin Rheumatol 2010;24(6):783–92.Busija L, Bridgett L, Williams SR, et al.
Osteoarthritis.
Best Pract Res Clin Rheumatol 2010;24(6):757–68.Carmona L, Cross M, Williams B, et al.
Rheumatoid arthritis.
Best Pract Res Clin Rheumatol 2010;24(6):733–45.Mourao AF, Blyth FM, Branco JC.
Generalised musculoskeletal pain syndromes.
Best Pract Res Clin Rheumatol 2010;24(6): 829–40.Sanchez-Riera L, Wilson N, Kamalaraj N, et al.
Osteoporosis and fragility fractures.
Best Pract Res Clin Rheumatol 2010; 24(6):793–810.Smith EU, Diaz-Torne C, Perez-Ruiz F, et al.
Epidemiology of gout: an update.
Best Pract Res Clin Rheumatol 2010;24(6): 811–27.Murray C, Ezzati M, Flaxman A, et al.
The Global Burden of Disease Study 2010: design, definitions and metrics.
Lancet 2012;380:2063–6.Hak AE, Curhan GC, Grodstein F, et al.
Menopause, postmenopausal hormone use and risk of incident gout.
Ann Rheum Dis 2010;69:1305–9.The World Bank Group.
Population projections. [cited 2014]; Available from:
http://web.worldbank.orgGeere JA, Hunter PR, P J.
Domestic water carrying and its implications for health:
a review and mixed methods pilot study in Limpopo Province, South Africa.
Environ Health. 9(52).Hoy DG, Toole MJ, Morgan D, et al.
Low back pain in rural Tibet.
Lancet 2003;361:225–6.Hoy DG, Fransen M, March L, et al.
In rural Tibet, the prevalence of lower limb pain, especially knee pain, is high:
an observational study.
J Physiother 2010;56(1):49–54.Dionne CE, Dunn KM, Croft PR, et al.
A consensus approach toward the standardization of back pain definitions for use in prevalence studies.
Spine 2008;33(1):95–103.Guzman J, Hurwitz EL, Carroll LJ, et al.
A New Conceptual Model Of Neck Pain: Linking Onset, Course, And Care Results of the
Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S14–23Arnett FC, Edworthy SM, Bloch DA, et al.
The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis.
Arthritis Rheum 1988;31(3):315–24.Kellgren JH, L JS.
Radiological assessment of osteo-arthrosis.
Ann Rheum Dis 1957;16(4):494–502.Wallace SL, Robinson H, Masi AT, et al.
Preliminary criteria for the classification of the acute arthritis of primary gout.
Arthritis Rheum 1977;20(3):895–900.Murray C, Lopez A.
The global burden of disease: a comprehensive assessment of mortality and disability from diseases,
injuries and risk factors in 1990 and projected to 2020.
Boston: Harvard University Press; 1996.Salomon JA, Vos T, Hogan DR, et al.
Common values in assessing health outcomes from disease and injury:
disability weights measurement study for the Global Burden of Disease Study 2010.
Lancet 2013;380(9859):2129–43.Hoy D, Smith E, Blyth F, et al.
Reflecting on the global burden of musculoskeletal conditions: lessons learnt, next steps.
Ann Rheum Dis 2014 Jun 9.
pii: annrheumdis-2014-205393.
http://dx.doi.org/10.1136/annrheumdis-2014-205393. [Epub ahead of print].Slobbe LCJ, Kommer GJ, Smit JM, et al.
Cost of illness in the Netherlands. 2003. Available from: URL,
http://www.rivm.nl/bibliotheek/rapporten/270751010.pdfManzina, et al. 2006.
The burden of musculoskeletal disease in the United States.
USBJI; 2011.
http://www.boneandjointburden.org/chapter_downloads/index.htmEUMUSC report. 2012.
Jordan, et al. 2010.
European Commission. 2007.
Ref.
Birnbaum H, Pike C, Kaufman R, et al.
Societal cost of rheumatoid arthritis patients in the US.
Curr Med Res Opin 2010;26: 77–90.Lundkvist, et al. 2008.
Ref from EUMUSC pg 132.
Stewart, et al. 2003.
2005 European Working Conditions Survey (EWCS)
European Foundation for the improvement of living and working conditions. 2007.European Occupational Disease Statistics. 2005.
2007 Labour Force Survey in the EU27.
http://www.ons.gov.uk/ons/dcp171776_353899.pdf
German Federal Bureau of Statistics. 2011.
Sicherheit und Gesundheit bei der Arbeit.
Bundesministeium fur Arbeit und Soziales; 2006.Lang, et al. Available from:
http://www.surrey.ac.uk/Psychology/stressimpact/publications/wp2/wp2_reportAustria.pdf
2003.http://www.UKresearch.dwp.gov.uk/.../dla_award_by_disabling_condition_age_group_aug10.xls
http://www.theworkfoundation.com/Assets/Docs/
FitforWorkLaunchpressrelease_250909_FINAL_FORDISTRIBUTION.pdfDall, et al.
Modeling the indirect economic implications of musculoskeletal disorders and treatment.
Cost Eff Resour Alloc 2013;11:5.Rice NE, Lang IA, Henley W, et al.
Common health predictors of early retirement: findings from the English Longitudinal Study of Ageing.
Age Ageing 2011;40:54–61.United Nations Population Division.
World population prospects: the 2012 revision New York 2012. August 15, 2014. Available from:
http://esa.un.org/unpd/wpp/index.htmFransen M, Bridgett L, March L, et al.
The epidemiology of osteoarthritis in Asia.
Int J Rheum Dis 2011;14:113–21.Kelly T, Yang W, Chen CS, et al.
Global burden of obesity in 2005 and projections to 2030.
Int J Obes (Lond) 2008;32(9): 1431–7.Ngo AD, Rao C, Hoa NP, et al.
Road traffic related mortality in Vietnam: evidence for policy from a national sample mortality
surveillance system.
BMC Public Health 2012;12:561.Volinn E, Deyo RA.
The epidemiology of low back pain in the rest of the world:
a review of surveys in low- and middleincome countries.
Spine 1997;22(15):1747–54.Joshi TK, Menon KK, Kishore J.
Musculoskeletal disorders in industrial workers of Delhi.
Int J Occup Environ Health 2001; 7(3):217–21.
Return to GLOBAL BURDEN OF DISEASE
Since 1-27-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |