A Patient's Guide to Carpal Tunnel Syndrome
Introduction
Carpal tunnel syndrome (CTS) is a common
problem affecting the hand and wrist. Symptoms begin
when the median nerve gets squeezed inside the
carpal tunnel of the wrist, a medical condition known
as nerve entrapment. Any condition that
decreases the size of the carpal tunnel or enlarges
the tissues inside the tunnel can produce the symptoms
of CTS.
This syndrome has received a lot of attention in
recent years because of suggestions that it may be
linked with occupations that require repeated use of
the hands, such as typing on a computer keyboard or
doing assembly work. Actually, many people develop
this condition regardless of the type of work they
do.
This guide will help you understand
- where the carpal tunnel is located
- how CTS develops
- what can be done for the
condition
Anatomy
Where is the carpal tunnel, and what does it
do?
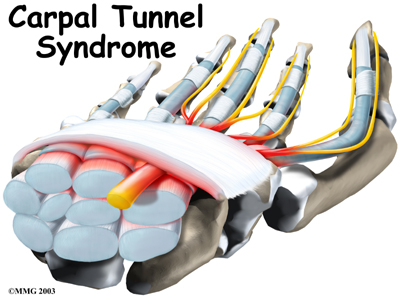
The carpal tunnel is an opening
through the wrist to the hand that is formed by
the bones of the wrist on one side and the
transverse carpal ligament on the other.
(Ligaments connect bones together.) This opening forms
the carpal tunnel.
The median
nerve passes through the carpal tunnel into
the hand. It gives sensation
to the thumb, index finger, long finger, and half of
the ring finger. It also sends a nerve branch to
control the thenar muscles of the thumb. The
thenar muscles help move the thumb and let you touch
the pad of the thumb to the tips each of each finger
on the same hand, a motion called opposition.
The median nerve and flexor tendons pass
through the carpal
tunnel. The median nerve rests on top of the
tendons, just below the transverse carpal ligament.
The flexor tendons are important because they allow
movement of the fingers, thumb, and hand, such as when
grasping. The tendons are covered by a material called
tenosynovium.
The tenosynovium is a slippery covering that allows
the tendons to glide next to each other as they are
worked.
Related Document: A
Patient's Guide to Hand Anatomy
Causes
What causes CTS?
Any condition that makes the area inside the carpal
tunnel smaller or increases the size of the tissues
within the tunnel can lead to symptoms of CTS. For
example, a traumatic wrist injury may cause swelling
and extra pressure within the carpal tunnel. The area
inside the tunnel can also be reduced after a wrist
fracture or dislocation if the bone pushes into the
tunnel.
Any condition that causes abnormal pressure in the
tunnel can produce symptoms of CTS. Various types of
arthritis can cause swelling and pressure in the
carpal tunnel. Fractured wrist bones may later cause
CTS if the healed fragments result in abnormal
irritation on the flexor tendons.
Other conditions in the body can produce symptoms
of CTS. Pregnancy can cause fluid to be retained,
leading to extra pressure in the carpal tunnel.
Diabetics may report symptoms of CTS, which may be
from a problem in the nerve (called neuropathy)
or from actual pressure on the median nerve. People
with low thyroid function (called
hypothyroidism) are more prone to problems of
CTS.
The way people do their tasks can put them at more
risk for problems of CTS. Some of these risks
include
- force
- posture
- wrist alignment
- repetition
- temperature
- vibration
One of these risks alone may not cause a problem.
But doing a task that involves several factors may
pose a greater risk. And the longer a person is
exposed to one or more risks, the greater the
possibility of having a problem with CTS. However,
scientists believe that other factors such as smoking,
obesity, and caffeine intake may actually be more
important in determining whether a person is more
likely to develop CTS.
In other instances, CTS can start when the
tenosynovium thickens from irritation
or inflammation. This thickening causes pressure
to build inside the carpal tunnel. But the tunnel
can't stretch any larger in response to the added
swelling, so the median nerve starts to squeeze
against the transverse carpal ligament. If the
pressure continues to build up, the nerve is
eventually unable to function normally.
When pressure builds on the median nerve, the blood
supply to the outer covering of the nerve slows down
and may even be cut off. The medical term for this is
ischemia. At first, only the outside covering
of the nerve is affected. But if the pressure keeps
building up, the inside of the nerve will start to
become thickened. New cells (called
fibroblasts) form within the nerve and create
scar tissue. This is thought to produce the feelings
of pain and numbness in the hand. If pressure is taken
off right away, the symptoms will go away quickly.
Pressure that isn't eased right away can slow or even
stop the chances for recovery.
Symptoms
What does CTS feel like?
One of the first symptoms of CTS is gradual
tingling and numbness in the areas supplied by the
median nerve. This is typically followed by dull,
vague pain where the nerve gives sensation in the
hand. The hand may begin to feel like it's asleep,
especially in the early morning hours after a night's
rest.
.jpg)
Sometimes pain may even spread up the arm to the
shoulder. If the condition progresses, the thenar
muscles of the thumb can weaken, causing the hand to
be clumsy when picking up a glass or cup. If the
pressure keeps building in the carpal tunnel, the
thenar muscles may begin to shrink (atrophy).
Touching the pad of the thumb to the tips of the
other fingers becomes difficult, making it hard to
grasp items such as a steering wheel, newspaper, or
telephone.
Diagnosis
How do doctors identify the condition?
Your doctor begins the evaluation by obtaining a
history of the problem, followed by a thorough
physical examination. Your description of the symptoms
and the physical examination are the most important
parts in the diagnosis of CTS. Commonly, patients will
complain first of waking in the middle of the night
with pain and a feeling that the whole hand is
asleep.
Careful investigation usually shows that the little
finger is unaffected. This can be a key piece of
information to make the diagnosis. If you awaken with
your hand asleep, pinch your little finger to see if
it is numb also, and be sure to tell your doctor if it
is or isn't. Other complaints include numbness while
using the hand for gripping activities, such as
sweeping, hammering, or driving.
If your symptoms started after a traumatic wrist
injury, X-rays may be needed to check for a fractured
bone.
If more information is needed to make the
diagnosis, electrical studies of the nerves in the
wrist may be requested by your doctor. Several tests
are available to see how well the median nerve is
functioning, including the nerve
conduction velocity (NCV) test. This test
measures how fast nerve impulses move through the
nerve.
Treatment
What can be done for CTS?
Nonsurgical Treatment
Activities that are causing your symptoms need to
be changed or stopped if at all possible. Avoid
repetitive hand motions, heavy grasping, holding onto
vibrating tools, and positioning or working with your
wrist bent down and out. If you smoke, talk to your
doctor about ways to help you quit. Lose weight if you
are overweight. Reduce your caffeine intake.
A wrist
brace will sometimes decrease the symptoms in the
early stages of CTS. A brace keeps the wrist in a
resting position, not bent back or bent down too far.
When the wrist is in this position, the carpal tunnel
is as big as it can be, so the nerve has as much room
as possible inside the carpal tunnel. A brace can be
especially helpful for easing the numbness and pain
felt at night because it can keep your hand from
curling under as you sleep. The wrist brace can also
be worn during the day to calm symptoms and rest the
tissues in the carpal tunnel.
Anti-inflammatory medications may also help control
the swelling and reduce symptoms of CTS. These include
common over-the-counter medications such as ibuprofen
and aspirin. Oral steroid medication may also offer
some relief. In some studies, high doses of vitamin
B-6 have been shown to help in decreasing CTS
symptoms. Some types of exercises have also shown to
help prevent or at least control the symptoms of
CTS.
If these simple measures fail to control your
symptoms, an injection of cortisone into the carpal
tunnel may be suggested. This medication is used to
reduce the swelling in the tunnel and may give
temporary relief of symptoms.
.jpg)
A cortisone injection may help ease symptoms and
can aid your doctor in making a diagnosis. If you
don't get even temporary relief from the injection, it
could indicate that some other problem is causing your
symptoms. When your symptoms do go away after the
injection, it's likely they are coming from a problem
within the carpal tunnel. Some doctors feel this is a
signal that a surgical release of the transverse
carpal ligament would have a positive result.
Your doctor may suggest that you work with a
physical or occupational therapist. The main focus of
treatment is to reduce or eliminate the cause of
pressure in the carpal tunnel. Your therapist may
check your workstation and the way you do your work
tasks. Suggestions may be given about the use of
healthy body alignment and wrist positions, helpful
exercises, and tips on how to prevent future problems.
You might also receive treatments to reduce
inflammation and to encourge normal gliding of the
tendons and median nerve within the carpal tunnel.
Surgery
If all attempts to control your symptoms fail,
surgery may be suggested to reduce the pressure on the
median nerve. Several different surgical procedures
have been designed to relieve pressure on the median
nerve. By releasing the pressure on the nerve, the
blood supply to the nerve improves, and most people
get relief of their symptoms. However, if the nerve
pressure has been going on a long time, the median
nerve may have thickened and scarred to the point that
recovery after surgery is much slower. Open
Release
The standard surgery for CTS is called open
release. Open surgical procedures use a
large skin incision. In open release for CTS, a
sizeable incision is made down the front of the wrist
and palm, usually about two inches long. By creating a
large incision, the surgeon is able to clearly see the
wrist structures and to carefully do the operation.
The surgeon cuts the transverse carpal ligament in
order to take pressure off the median nerve.
.jpg)
After dividing
the transverse carpal ligament, the surgeon stitches
just the skin together and leaves the loose ends of
the transverse carpal ligament separated. The loose
ends are left apart to keep pressure off the median
nerve. Eventually, the gap between the two ends of the
ligament fills in with scar tissue.
Related Document: A
Patient's Guide to Open Carpal Tunnel Release Endoscopic
Release
Some surgeons are using a newer procedure called
endoscopic carpal tunnel release. The surgeon
merely nicks the skin in order to make one or two
small openings for inserting the endoscope. An
endoscope is a thin, fiber-optic TV camera that
allows the surgeon to see inside the carpal tunnel as
the transverse carpal ligament is carefully
released.
Upon inserting the endoscope, the surgeon can see
the wrist structures on a TV screen. A special
knife is used to cut only the transverse carpal
ligament. The palmar fascia and the skin over the
wrist are not disturbed.
As in open release, the loose ends of the
transverse carpal ligament are left apart after
endoscopic release to keep pressure off the median
nerve. The gap eventually fills in with scar
tissue.
Related Document: A
Patient's Guide to Endoscopic Carpal Tunnel
Release
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
If nonsurgical treatment is successful, you may see
improvement in four to six weeks. You may need to
continue wearing your wrist splint at night to control
symptoms and keep your wrist from curling under as you
sleep. Try to do your activities using healthy body
and wrist alignment. Limit activities that require
repeated motions, heavy grasping, and vibration in the
hand.
After Surgery
It generally takes longer to recover after open
carpal tunnel release. Pain and symptoms usually begin
to improve, but you may have tenderness in the area of
the incision for several months after surgery.
When the stitches are removed, your surgeon may
have you work with a physical or occupational
therapist for six to eight weeks. Treatments are used
at first to ease pain and inflammation. Gentle massage
to the incision can help reduce sensitivity in and
around the incision and limit scar tissue from
building up. Special exercises are used to encourage
normal gliding of the tendons and median nerve within
the carpal tunnel.
As you progress, your therapist will give you
exercises to help strengthen and stabilize the muscles
and joints in the hand, wrist, and arm. Other
exercises are used to improve fine motor control and
dexterity of the hand. Your therapist will work with
you to help you do your daily and work activities
safely and with the least amount of strain on your
wrist and hand. | ){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}