
NSAIDs and Musculoskeletal Treatment
What Is the Clinical Evidence?
Steven D. Stovitz, MD
Robert J. Johnson, MD
THE PHYSICIAN AND SPORTSMEDICINE - VOL 31 - NO. 1 - JANUARY 2003
In Brief: Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed for musculoskeletal injuries because the conditions are believed to be inflammatory in nature. However, because inflammation is a necessary component in the healing process, decreasing inflammation may prove counterproductive. Also, many tendon injuries called 'tendinitis' are, in fact, degenerative and not inflammatory conditions. An analysis of the pathophysiology and healing of musculoskeletal injuries questions the use of NSAIDs in many treatment protocols. Because NSAIDs have profound side effects, they should not automatically be the first choice for treating musculoskeletal injuries.
Musculoskeletal concerns rank with upper respiratory illness as the most common reason patients seek medical attention in family practice. [1] Treatment algorithms for musculoskeletal injuries tend to reflexively include the use of nonaspirin, nonsteroidal anti-inflammatory drugs (NSAIDs). Currently, NSAIDs are among the most widely prescribed drugs in this country. [2]
Despite the widespread use of NSAIDs, we question their role in many treatment protocols for musculoskeletal complaints — in particular, the clinical value of their anti-inflammatory properties. Although originally marketed as the "safe" alternative to aspirin, NSAIDs are known to have serious gastrointestinal toxicity and other side effects. We review the pathophysiology and healing of musculoskeletal injuries and the clinical evidence regarding the efficacy of NSAIDs in treating a variety of nonrheumatic musculoskeletal injuries.
Mechanism of Action
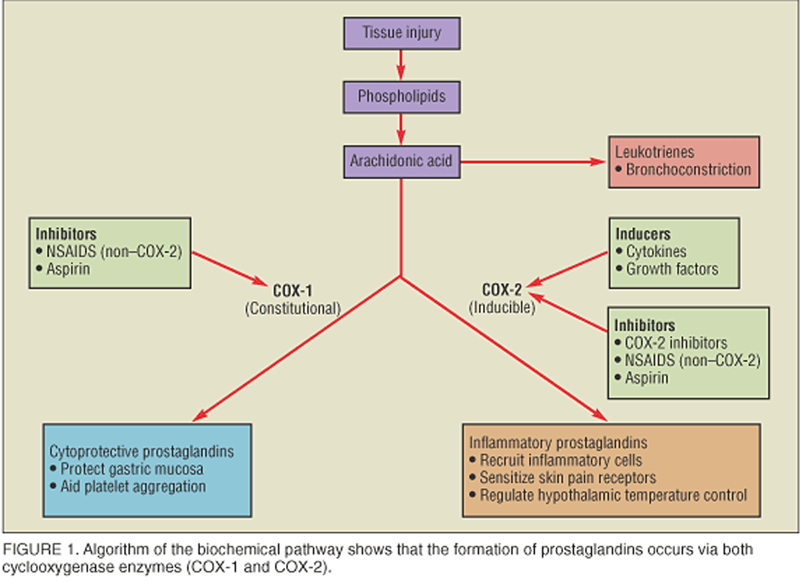
NSAIDs are used for their analgesic, anti-inflammatory, and antipyretic properties. Their therapeutic actions are thought to stem primarily from their ability to block the formation of certain prostaglandins through inhibition of the cyclooxygenase (COX) enzymes (Figure 1). In general, COX-1 catalyzes the production of several cytoprotective prostaglandins that coat the stomach lining with mucus and aid platelet aggregation, among other functions. COX-2 catalyzes the conversion of arachidonic acid into the inflammatory prostaglandins that are involved in three key biological functions: sensitizing skin pain receptors, elevating body temperature through the hypothalamus, and recruiting inflammatory cells toward injured body parts. (The delineation between COX-1 and COX-2 enzymes may be more complex, as described in the section on COX-2 inhibitors below.)
In addition to their effects on prostaglandins, NSAIDs exhibit other properties that have uncertain clinical relevance (eg, inhibition of neutrophil migration, oxidative phosphorylation, and lysosomal enzyme release). [3]
Inflammation and Healing
A major rationale for using NSAIDs in the treatment of musculoskeletal injuries has been their anti-inflammatory quality. The prevailing argument is that healthy tissue is not inflamed; therefore, if we stop the inflammation in an injured tissue, the tissue will be healthy. The problem with this viewpoint is that, in addition to being a sign of injury, inflammation is a necessary component of the healing process. As noted by Leadbetter, [4] "inflammation can occur without healing, but healing cannot occur without inflammation."
Whether the injured tissue is a ligament, tendon, or muscle, the body responds to injury with a sequence of events that begins with an influx of inflammatory cells and blood. The inflammatory cells remove debris and recruit cytokines and other growth factors toward the injury site. This inflammatory phase is partly mediated by the same prostaglandins that are blocked by NSAIDs. In a healthy healing process, a proliferative phase consisting of a mixture of inflammatory cells and fibroblasts naturally follows the inflammatory phase. The fibroblasts build a new extracellular matrix and persist into the final phase of repair, the maturation phase, where, if all goes well, functional tissue is laid down. The key point is that each phase of repair is necessary for the subsequent phase. By blocking the inflammatory phase, NSAIDs can, at least theoretically, delay the healing of musculoskeletal injuries.
NSAIDs and Musculoskeletal Injuries
NSAIDs are commonly prescribed for the treatment of musculoskeletal complaints such as muscle injuries, ligament sprains, tendon injuries, low-back pain, and osteoarthritis. However, an examination of the pathophysiology and healing of such injuries, as well as a remarkable dearth of clinical trials supporting the efficacy of NSAIDs, raises questions about their use in many treatment protocols.
Muscle injuries.
Whether caused by direct trauma or excessive strain, muscle injury is the most common sports injury. [5] Although NSAIDs are commonly recommended in treatment protocols, clinical studies documenting their efficacy are notably lacking. We searched MEDLINE (1966 to 2002) using keywords "anti-inflammatories, nonsteroidal," "NSAIDs," "skeletal muscle," or "athletic injuries" and "randomized controlled trials" and found none involving oral NSAIDs. A recent review of studies on strains, contusions, and delayed-onset muscle soreness revealed minimal benefit at best when NSAIDs are compared with placebo. [5]
While some literature [6, 7] suggests that NSAIDs may delay the rate of muscle fiber regeneration, the clinical ramifications of this remain unclear. Clinical outcome studies of muscle injuries are difficult to conduct because the injuries tend to heal within days without intervention. Many clinicians in our sports medicine community are turning to short (24- to 48-hour) courses of NSAIDs, hoping to combine the benefits of pain relief and decreased swelling without affecting the regenerative phases of healing. Furthermore, several physicians in our community are now advocating the newer COX-2 inhibitors (discussed below) for muscle injuries with the idea that the drugs' lack of platelet inhibition might further diminish bleeding and swelling in the injured tissue. We are unaware of any studies to substantiate these claims.
Interestingly, users of anabolic steroids anecdotally report that these drugs — which actually increase inflammation — hasten the healing of muscle injuries. A recent animal study [8] supports these claims. If anabolic steroids prove helpful for tissue healing in humans, the medical profession may be faced with some interesting ethical decisions.
Ligament injuries. Data on the efficacy of NSAIDs in the treatment of ligament sprains is extremely limited. In 1990, a review by Almekinders [9] found only 15 studies that he felt were "carried out in a scientifically appropriate manner," and 8 of those focused on a single joint. NSAIDs were beneficial in half of these single-joint studies (2 of the 6 that examined ankle ligament sprains and the 2 that focused on knee ligament injuries). In 1995, a clinical review [10] on treatment modalities for soft-tissue injuries of the ankle stated that "NSAIDs tended to offer significant improvement in recovery time and symptomatic relief over placebo." However, the authors do not state how the papers were selected for review or assessed for validity. Our own search of MEDLINE (1966 to 2002) using keywords "anti-inflammatories, nonsteroidal" or "NSAIDs," "ligaments," and "clinical trials" revealed no studies using oral NSAIDs in the outpatient setting. A 1997 study [11] of 364 Australian army recruits who had ankle sprains showed that the group given NSAIDs returned to activity sooner, but had increased instability and decreased range of motion, compared with those given placebo.
The study of ligament sprains is limited, because sprains tend to heal with time and because the outcomes are subjective and favor NSAIDs, which are excellent analgesics. Controlled mobilization of injured ligaments assists healing, [12] and, in this context, if NSAIDs decrease pain and thus encourage activity, they may provide some therapeutic benefit. It is unknown whether a similar effect could be obtained with other analgesics, including simply ice.
Tendon injuries. When it comes to tendinitis, the use of NSAIDs as anti-inflammatory agents becomes especially controversial. Contrary to what their name implies (the suffix "itis" denotes an inflammatory process), these injuries may not be inflammatory in nature. Indeed, several experts in this area have pointed out this misnomer and emphasized its unfortunate effect of furthering a false perception that an anti-inflammatory medicine should be used in treatment. [13–15]
Several large studies [14, 16, 17] have looked at tissue biopsies from chronic injuries of the extensor carpi radialis brevis ("tennis elbow"), Achilles, patellar, and rotator cuff tendons. Results show the tendons to be degenerative and lacking in inflammatory cells. Thus, a more proper term would be either "tendinosis," meaning tendon degeneration, or "tendinopathy," signifying nonspecific tendon pathology. Some have argued that a poor inflammatory process is the precipitant that causes tendon degeneration. [13, 16]
Controlled trials of NSAID use have not resolved this issue. A review [15] of MEDLINE from 1966 to 1996 found only 9 prospective studies comparing NSAIDs with placebo. The review noted that NSAIDs provided better pain relief in 5 of the 9 studies. This result is hardly unexpected, given the potent analgesic effect of NSAIDs. The maximum study follow-up was only 1 to 4 weeks; therefore, the long-term effect of NSAIDs on these tendons is unknown.
Low-Back Pain and Osteoarthritis
NSAIDs are frequently used to treat common musculoskeletal conditions, such as low-back pain and osteoarthritis, though they are not classically sports-related injuries.
Low-back pain. The study of treatments for low-back pain is limited by its multiple and poorly understood causes. Two large meta-analyses [18, 19] were recently conducted, including a Cochrane review in 2000. Both searched MEDLINE for literature from the 1960s to the 1990s; the Cochrane study [19] also included Embase studies from 1988 to 1998. Both found very few well-designed trials, and those that were found had small numbers of patients. There were some subtle differences in the reviews, but overall their methods and conclusions were similar.
Koes et al [18] found 10 acceptable trials comparing NSAIDs with placebo and concluded that NSAIDs "might be effective for short-term symptomatic relief in patients with uncomplicated low-back pain." The Cochrane review [19] identified 11 controlled studies of adequate design and concluded that there is "conflicting evidence that NSAIDs provide better pain relief than placebo for acute low-back pain." The Cochrane review found 5 "acceptable" studies comparing NSAID efficacy to that of acetaminophen and only 1 that was considered "high quality." This high-quality study included only 30 patients. It concluded that there is, at best, level 3 (ie, conflicting or limited) evidence that NSAIDs are more effective than acetaminophen for acute or chronic low-back pain.
Osteoarthritis. Eighty percent of individuals older than 65 have radiographic signs of osteoarthritis (OA), and a large percentage have symptoms. [20] Given the chronic nature of the disease and the high incidence of medication side effects in the elderly, an understanding of the risks and benefits of NSAIDs in treating OA is crucial. The two main issues are pain relief and disease progression.
In reviews of clinical trials on OA of the hip and knee, NSAIDs perform significantly better as analgesics compared with placebo. [21, 22] Most studies comparing different NSAIDs have found no significant difference in their analgesic effects and provide no strong basis for recommending one NSAID over another. A recent randomized controlled trial [23] comparing NSAIDs with acetaminophen found a significant benefit in using NSAIDs for moderate-to-severe OA. Previously, only two studies on OA had compared an NSAID with acetaminophen; neither supported a benefit for either medication. Given that the adverse effects of NSAIDs (see below) tend to disproportionately strike the elderly (hence, sufferers of OA), numerous guidelines, including those put forth by the American College of Rheumatology, recommend trying acetaminophen before an NSAID. [24–26] An increasing number of small trials are being conducted that compare glucosamine and chondroitin sulfate with NSAIDs. The emerging evidence suggests a trend whereby pain relief during the first 4 weeks is superior with an NSAID, but then plateaus after 1 month. [27, 28]
Whether NSAIDs hasten, attenuate, or have no effect on the progression of OA is unknown. In vitro studies are beginning to show evidence that certain NSAIDs stimulate the synthesis of glycosaminoglycan, whereas others either have no effect or degrade it. [29, 30] Given this variation in response among NSAIDs, their effects on articular cartilage are likely mediated by a mechanism other than prostaglandin inhibition. If certain NSAIDs prove beneficial to articular cartilage while others prove harmful, future treatment recommendations could change dramatically.
Weighing Side Effects
Although strong and consistent evidence is lacking that NSAIDs clinically benefit the healing of musculoskeletal injuries, they remain potent pain relievers. Their use in this capacity, however, is limited by notable side effects; gastrointestinal (GI) effects are the most common and serious.
GI bleeding secondary to NSAID use is the 15th leading cause of death in the United States. [31] Unfortunately, dyspepsia cannot be used as a screening criterion, because only 40% of those who have NSAID-induced GI bleeding report abdominal symptoms before the bleed. [32] This might be due to their analgesic effects. Perhaps as a result of their inhibition of platelet aggregation, individuals who have GI bleeding while taking NSAIDs have a significantly higher mortality than those with GI bleeds who are not taking NSAIDs. [32]
The renal and cardiovascular systems are also affected, because prostaglandins are necessary for renal blood flow and the secretion of sodium and chloride. Prostaglandin inhibition has been shown to raise mean arterial blood pressure by an average of 3 to 5 mm Hg, a small but potentially harmful amount. [33] Endurance athletes are often hypohydrated as a consequence of prolonged training. NSAIDs can superimpose further decreases in renal blood flow through prostaglandin inhibition. This combination has been implicated in case reports of acute renal failure in marathoners. [34, 35] NSAIDs have historically been perceived to be either neutral or beneficial regarding cardiovascular occlusive events. However, a recent study [36] suggests that the drugs' temporary platelet inhibition may limit the cardioprotective effects of aspirin by antagonizing aspirin's irreversible platelet inhibition.
Another potential complication for athletes involves the respiratory system. Blocking cyclooxygenase can shunt arachidonic acid toward the formation of the bronchoconstricting leukotrienes (see figure 1). It is estimated that 10% of patients who have asthma experience a decline in their respiratory function as a result of NSAID inhibition of cyclooxygenase. [37]
COX-2 Inhibitors
The new COX-2 inhibitors are being marketed as the safe alternative to other NSAIDs. Given the recent entry of COX-2 inhibitors into the market, little is known about their in vivo effects (either intended or adverse). Data from clinical trials suggest that their analgesic effects are similar to traditional NSAIDs. [38]
As their name implies, the COX-2 inhibitors preferentially block the COX-2 enzyme while allowing the pathways catalyzed by COX-1 to proceed. Theoretically, this inhibits the formation of the inflammatory prostaglandins while allowing the production of the homeostatic prostaglandins. Unfortunately, as Oscar Wilde said, "the pure and simple truth is rarely pure and never simple." [39] In fact, increasing evidence indicates that the COX-2 enzyme also has some homeostatic functions.
Breyer and Harris [40] suggest that the COX-2 enzyme plays an integral role in kidney function and will likely affect blood pressure to an extent similar to traditional NSAIDs. COX-2 inhibitors seem to cause fewer new GI ulcers, although this has not been definitively shown to decrease the number of complications from GI bleeds. [41] Interestingly, this might be because the inflammatory pathway is necessary for healing preexisting ulcers.
A concern is that selective inhibition of antithrombotic prostaglandins might increase cardiovascular events. Patients receiving rofecoxib during the VIGOR study [42] suffered cardiovascular events at a higher rate than those in the naproxyn group. This prompted a meta-analysis of trials with COX-2 inhibitors [43] to state that "the available data raise a cautionary flag about the risk of cardiovascular events with COX-2 inhibitors." A more recent analysis [44] suggests that the increased rate of cardiovascular events noted above was actually due to a cardioprotective effect of naproxen and not to increased events in the rofecoxib group.
The expense of COX-2 inhibitors is another major concern; treatment can cost as much as $70 or more than generic NSAIDs per month. [45] Certainly, if this decreases other medical costs, this might prove beneficial. Finally, given their inhibition of the inflammatory pathway, all of the concerns regarding delayed healing of injured tissues remain the same when using COX-2 inhibitors.
Clarifying the Role of NSAIDs
Reviewing the most current updates on the use of NSAIDs in the treatment of musculoskeletal injuries is challenging. Although we mention randomized controlled trials, or lack thereof, this review is not intended to be a meta-analysis. Any attempt at a meta-analysis on this topic would be fraught with either a tremendous lack of data (if stringent criteria were used) or controversy (if criteria were loosened).
Given the paucity of data, we are unable to draw any definitive conclusion in support of or against the use of NSAIDs. We realize that many clinicians use anti-inflammatories for musculoskeletal conditions so routinely that any suggestion that little evidence supports their use is interpreted as a condemnation. This discussion is meant to clarify, not simply diminish, the role of NSAIDs. To effectively treat musculoskeletal injuries, the clinician must have realistic expectations about the capabilities of NSAIDs and convey them to the patient. NSAIDs are rarely a substitute for rehabilitation and activity modification.
When used properly, NSAIDs can be a useful, but limited, adjunct. They certainly play a key therapeutic role in the treatment of the crystalline and rheumatoid arthritides and may be beneficial in treating pathologic edema of bursa and synovial tissue (eg, tenosynovitis). For most common sprains, strains, and overuse injuries, however, their therapeutic properties are unproven. It is crucial to keep a proper perspective regarding the role of NSAIDs, especially given their risk of side effects and their potential to blunt the normal healing response. Too many physicians and patients view NSAIDs as critical to recovery. Additional research is needed to define more explicitly the role of NSAIDs in interfering with or delaying healing and the role of other, potentially safer, means to control the pain of musculoskeletal injuries.
References:
Rosenblatt RA, Cherkin DC, Schneeweiss R, et al:
The structure and content of family practice: current status and future trends.
J Fam Pract 1982;15(4):681-722
Golden BD, Abramson SB:
Selective cyclooxygenase-2 inhibitors.
Rheum Dis Clin North Am 1999;25(2):359-378
Leadbetter WB:
Anti-inflammatory therapy in sports injury: the role of nonsteroidal drugs and corticosteroid injections.
Clin Sports Med 1995;14(2):353-410
Leadbetter WB:
An introduction to sports-induced soft-tissue inflammation,
in Leadbetter WB, Buckwalter JA, Gordon SL (eds):
Sports-induced Inflammation: Clinical and Basic Science Concepts.
Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, p 13
Almekinders LC:
Anti-inflammatory treatment of muscular injuries in sport: an update of recent studies.
Sports Med 1999;28(6):383-388
Best TM, Hunter KD:
Muscle injury and repair.
Phys Med Rehab Clin N Am 2000;11(2):251-266
Weiler JM:
Medical modifiers of sports injury: the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in sports soft-tissue injury.
Clin Sports Med 1992;11(3):625-644
Beiner JM, Jokl P, Cholewicki J, et al:
The effect of anabolic steroids and corticosteroids on healing of muscle contusion injury.
Am J Sports Med 1999;27(1):2-9
Almekinders LC:
The efficacy of nonsteroidal anti-inflammatory drugs in the treatment of ligament injuries.
Sports Med 1990;9(3):137-142
Ogilvie-Harris DJ, Gilbart M:
Treatment modalities for soft tissue injuries of the ankle: a critical review.
Clin J Sport Med 1995;5(3):175-186
Slatyer MA, Hensley MJ, Lopert R:
A randomized controlled trial of piroxicam in the management of acute ankle sprain in Australian Regular Army recruits: the Kapooka Ankle Sprain Study.
Am J Sports Med 1997;25(4):544-553
Frank CB:
Ligament healing: current knowledge and clinical applications.
J Am Acad Orthop Surg 1996;4(1):74-83
Khan KM, Cook JL, Taunton JE, et al:
Overuse tendinosis, not tendinitis. Part 1: a new paradigm for a difficult clinical problem.
Phys Sportsmed 2000;28(5):38-48
Khan KM, Cook JL, Bonar F, et al:
Histopathology of common tendinopathies: update and implications for clinical management.
Sports Med 1999;27(6):393-408
Almekinders LC, Temple JD:
Etiology, diagnosis, and treatment of tendonitis: an analysis of the literature.
Med Sci Sports Exerc 1998;30(8):1183-1190
Kraushaar BS, Nirschl RP:
Tendinosis of the elbow (tennis elbow): clinical features and findings of histological, immunohistochemical and electron microscopy studies.
J Bone Joint Surg Am 1999;81(2):259-278
Astrom M, Rausing A:
Chronic Achilles tendinopathy: a survey of surgical and histopathologic findings.
Clin Orthop 1995;316(July):151-164
Koes BW, Scholten RJ, Mens JM, et al:
Efficacy of non-steroidal anti-inflammatory drugs for low back pain: a systematic review of randomised clinical trials.
Ann Rheum Dis 1997;56(4):214-223
van Tulder MW, Scholten RJ, Koes BW, et al:
Nonsteroidal anti-inflammatory drugs for low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group.
Spine 2000;25(19):2501-2513
Phillips AC, Polisson RP, Simon LS:
NSAIDs and the elderly: toxicity and economic implications.
Drugs Aging 1997;10(2):119-130
Towheed TE, Hochberg MC:
A systematic review of randomized controlled trials of pharmacological therapy in osteoarthritis of the hip.
J Rheumatol 1997;24(2):349-357
Towheed TE, Hochberg MC:
A systematic review of randomized controlled trials of pharmacological therapy in osteoarthritis of the knee, with an emphasis on trial methodology.
Semin Arthritis Rheum 1997;26(5):755-770
Pincus T, Koch GG, Sokka T, et al:
A randomized, double-blind, crossover clinical trial of diclofenac plus misoprostol versus acetaminophen in patients with osteoarthritis of the hip or knee.
Arthritis Rheum 2001;44(7):1587-1598
American College of Rheumatology Subcommittee on Osteoarthritis Guidelines:
Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update.
Arthritis Rheum 2000;43(9):1905-1915
Cole BJ, Harner CD:
Degenerative arthritis of the knee in active patients: evaluation and management.
J Am Acad Orthop Surg 1999;7(6):389-402
Eccles M, Freemantle N, Mason J:
North of England evidence based guideline development project: summary guideline for non-steroidal anti-inflammatory drugs versus basic analgesia in treating the pain of degenerative arthritis.
The North of England Non-Steroidal Anti-Inflammatory Drug Guideline Development Group.
BMJ 1998;317(7157):526-530
Deal CL, Moskowitz RW:
Nutraceuticals as therapeutic agents in osteoarthritis: the role of glucosamine, chondroitin sulfate, and collagen hydrolysate.
Rheum Dis Clin North Am 1999;25(2):379-395
McAlindon TE, LaValley MP, Gulin JP, et al:
Glucosamine and chondroitin for treatment of osteoarthritis: a systematic quality assessment and meta-analysis.
JAMA 2000;283(11):1469-1475
Pelletier JP:
The influence of tissue cross-talking on OA progression: role of nonsteroidal anti-inflammatory drugs.
Osteoarthritis Cartilage 1999;7(4):374-376
Lequesne MG:
Is there preliminary in-vivo evidences of an influence of nonsteroidal anti-inflammatory drug treatment on osteoarthritis progression? Part 1.
Osteoarthritis Cartilage 1999;7(3):350
Wolfe MM, Lichtenstein DR, Singh G:
Gastrointestinal toxicity of nonsteroidal anti-inflammatory drugs.
N Engl J Med 1999;340(24):1888-1899 [published erratum N Engl J Med 1999;341(7):548]
Hayllar J, Macpherson A, Bjarnason I:
Gastroprotection and nonsteroidal anti-inflammatory drugs (NSAIDs): rationale and clinical implications.
Drug Saf 1992;7(2):86-105
MacFarlane LL, Orak DJ, Simpson WM:
NSAIDs, antihypertensive agents and loss of blood pressure control.
Am Fam Physician 1995;51(4):849-856
Walker RJ, Fawcett JP, Flannery EM, et al:
Indomethacin potentiates exercise-induced reduction in renal hemodynamics in athletes.
Med Sci Sports Exerc 1994;26(11):1302-1306
Vitting KE, Nichols NJ, Seligson GR:
Naproxen and acute renal failure in a runner, letter.
Ann Intern Med 1986;105(1):144
Catella-Lawson F, Reilly MP, Kapoor SC, et al:
Cyclooxygenase inhibitors and the antiplatelet effects of aspirin.
N Engl J Med 2001;345(25):1809-1817
Szczeklik A, Stevenson DD:
Aspirin-induced asthma: advances in pathogenesis and management.
J Allergy Clin Immunol 1999;104(1):5-13
Noble SL, King DS, Olutade JI:
Cyclooxygenase-2 enzyme inhibitors: place in therapy.
Am Fam Physician 2000;61(12):3669-3676
Ruddy S, Harris ED, Sledge CB, et al (eds):
Kelley's Textbook of Rheumatology, ed 6.
Philadelphia, WB Saunders, 2001, p 801
Breyer MD, Harris RC:
Cyclooxygenase 2 and the kidney.
Curr Opin Nephrol Hypertens 2001;10(1):89-98
Lichtenstein DR, Wolfe MM:
COX-2 selective NSAIDs: new and improved?
JAMA 2000;284(10):1297-1299
Bombardier C, Laine L, Reicin A, et al:
Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis: VIGOR Study Group.
N Engl J Med 2000;343(21):1520-1528, 2 p following 1528
Mukherjee D, Nissen SE, Topol EJ:
Risk of cardiovascular events associated with selective COX-2 inhibitors.
JAMA 2001;286(8):954-959
Dalen JE:
Selective COX-2 inhibitors, NSAIDs, aspirin, and myocardial infarction.
Arch Intern Med 2002;162(10):1091-1092
Valdecoxib (Bextra): a new COX-2 inhibitor.
Med Lett Drugs Ther 2002;44(1129):39-40
The authors thank Anne Marie Weber-Main, PhD, for her editorial assistance with this manuscript.
Dr Stovitz is an assistant professor and coordinator of sports medicine education in the department of family practice and community health at the University of Minnesota in Minneapolis. Dr Johnson is the director of primary care sports medicine in the department of family practice at Hennepin County Medical Center in Minneapolis and is president of the American Medical Society for Sports Medicine. Address correspondence to Steven D. Stovitz, MD, Smiley's Clinic, 2615 E Franklin Ave, Minneapolis, MN 55406; e-mail to stovi001@umn.edu.
Disclosure information: Drs Stovitz and Johnson disclose no significant relationship with any manufacturer of any commercial product mentioned in this article. No drug is mentioned in this article for an unlabeled use.

Return to the SHOULDER Page
Return to the IATROGENIC INJURY Page
|