Osteoarthritis of the Glenohumeral Joint
Nonsurgical Treatment Options
David G. Carfagno, DOTodd S. Ellenbecker, MS, PT, SCS
THE PHYSICIAN AND SPORTSMEDICINE - VOL 30 - NO. 4 - APRIL 2002
In Brief: Glenohumeral osteoarthritis is a relatively uncommon type of osteoarthritis characterized by loss of anterior or forward flexion. Assessing range of motion, impingement, and strength, combined with radiologic imaging, can help determine the extent of damage. Published studies focus primarily on surgical treatment, but commonly used nonsurgical approaches include anti-inflammatory medications, oral and injectable viscosupplementation, and physical therapy. These conservative measures can be very effective for active patients and also appeal to their physicians who consider shoulder surgery as a last resort.
Glenohumeral osteoarthritis (GHOA) results when the articular cartilage between the glenoid fossa of the scapula and the humerus is damaged by trauma or instability. Although osteoarthritis (OA) is more common in the weight-bearing joints of the knee, hip, and spine, non-weight-bearing joints, such as the shoulder, can undergo the same degenerative process.
Who Is at Risk?
Degenerative arthritis of the glenohumeral joint accounts for only 3% of all reported osteoarthritis lesions. [1] GHOA can be classified as primary (having no apparent antecedent cause) or secondary (resulting from fracture or trauma, avascular necrosis, "burned-out" rheumatoid arthritis, or crystalline arthropathy). In athletes, GHOA is usually secondary.
Athletes at risk include weight lifters, baseball players, softball players, and those who play racket sports such as tennis, racquetball, and squash. [2] GHOA seems to result from pure instability, rotator cuff arthropathy, fracture, or postsurgical trauma and predominately affects older men. GHOA generally involves the glenoid rather than the humeral side of the joint, [3] which will influence rehabilitation.
Pathogenesis
At the macroscopic level, eburnation of the cartilage surface and, eventually, frank cartilage loss result in bone-on-bone contact. Inflammatory cells appear early in the degenerative process, but this effect is transient, and inflammation is not considered to play a major long-term role. Biochemically, OA is associated with a decrease in glycosaminoglycans, including chondroitin sulfate, hyaluronic acid, and keratin sulfate; increased water content as water diffuses into the cartilage as glycosaminoglycans are lost; and increased enzymatic activity from matrix metalloproteinases (MMPs). The MMPs play an important role in degeneration of the extracellular matrix of cartilage. [4]
Many theories have been proposed to explain the degradation of cartilage in OA. The initial event is attributed to mechanical stress that leads to multiple microfractures. Subsequently, altered chondrocyte metabolism and production of MMPs lead to gradual loss of cartilage, altered joint architecture, and osteophyte formation. [4]
Signs and Symptoms
Generally, a person who has GHOA reports pain, decreased function, and loss of shoulder motion. Pain is typically worse with activity and better with rest. Characteristically, the patient who has GHOA lacks anterior or forward flexion. In contrast, adhesive capsulitis displays global decreased motion, and shoulder tendinitis produces pain at certain arcs of motion and decreased strength. Concomitant arthritic rotator cuff tendinitis and adhesive capsulitis may also occur.
Mechanisms of pain in OA include periostitis at sites of bony remodeling, subchondral microfractures, irritation of sensory nerve endings in the synovium, periarticular muscle spasm, and synovial inflammation. [5]
Musculoskeletal Evaluation
The musculoskeletal exam focuses on posture, range of motion (ROM), muscle strength measurement, and provocative maneuvers to identify rotator cuff or labral pathology.
Posture. Evaluation of standing and sitting posture provides valuable insight for the clinician. [6] Uninjured patients typically stand with the dominant shoulder lower than the nondominant. Elevation of the injured dominant shoulder in a resting stance may indicate muscular guarding and spasm of the upper trapezius and levator scapulae. Additionally, a prominent medial or inferior border of the scapula may indicate weakness of the serratus anterior and lower trapezius, as well as tightness of the anterior pectorals. [6] Placing the patient's hands on his or her hips also exaggerates any atrophy present in the infraspinous fossa and periscapular regions. The degree of thoracic kyphosis and cervical lordosis is also of interest, because changes in the resting posture during scapular protraction and retraction may aggravate subacromial impingement. [7]
Range of motion. Patients who have GHOA will experience a loss of both passive and active ROM, so careful measurements are indicated. During active antigravity elevation, patients with force-couple imbalances often "hike" their involved shoulder to compensate for rotator cuff and scapular weakness. Kibler [5] termed this "superior scapular dysfunction." This finding, common in patients with rotator cuff disease and GHOA, signals the need for appropriate, focused strengthening during rehabilitation. The uninvolved shoulder serves as the baseline for initial evaluation and goal setting.
Additionally, internal and external rotational ROM is performed and documented, if possible, in 90° of abduction. Significant loss of internal rotation increases glenohumeral joint shear force in both anterior and superior directions. [7] Posterior capsular tightness causes obligate translation of the humeral head anteriorly and superiorly, away from the tightness, which aggravates the impingement. Rotational ROM measurement guides mobilization and stretching techniques during rehabilitation.
Strength. Evaluation of strength is typically limited to manual techniques for the rotator cuff, deltoid, and scapular muscles. Isokinetic testing offers greater sensitivity and delineation of muscle strength but is often contraindicated during the initial evaluation because it's too painful. Specific manual tests to determine the competency of the external and internal rotators, supraspinatus, and deltoid muscles convey the baseline degree of muscle stabilization when treatment is initiated.
Special tests. Impingement testing is widely recommended for evaluating the patient with a painful shoulder. Tests described by Neer [8]and Hawkins and Kennedy [9] can determine the degree of primary impingement of the rotator cuff tendons against the coracoacromial arch. Impingement signs are typically positive but provide information by reproducing pain. Of particular note for patients who have primary GHOA is the point at which impingement occurs. Erosion of the glenoid, associated rotator cuff tears, osseous deformities, and spurring can all increase superior humeral head migration and exaggerate impingement in less than the normal end-range of motion. Comparison is made to the contralateral extremity. Palpating the shoulder during passive movement on the impingement tests will also indicate the degree of crepitation and grinding in the subacromial space and glenohumeral articulation.
Another critical test is humeral head translation. The sulcus sign is invaluable for identifying multidirectional instability and generalized joint capsular laxity. [10] Lack of translation when compared with the uninvolved shoulder is the diagnostic clue and helps guide rehabilitation efforts to increase ROM.
To assess anterior and posterior humeral head translation, the examiner can apply the load-and-shift test (Figure 1) to evaluate the degree of translation between the humeral head and the glenoid. [10] Translation over the glenoid rim, with relocation upon removal of the examiner's stress, indicates grade 2 translation, according to Altchek et al. [11] (A discussion of how the different grades affect treatment selection is beyond the scope of this article.)
Patients with increased humeral head translation are optimal candidates for strengthening programs designed to improve humeral head compression and rotator cuff stability. [12, 13] Inability to move the humeral head relative to the glenoid, either anteriorly or posteriorly, often demonstrates capsular tightness caused by adhesions, disuse, or altered mechanics, which indicates the need for selective joint mobilization techniques and stretching. Identifying glenohumeral joint instability and selective capsular hypomobility helps guide nonoperative treatment. Improved humeral head control and normalization of capsular restrictions help improve function.
 |
Radiography
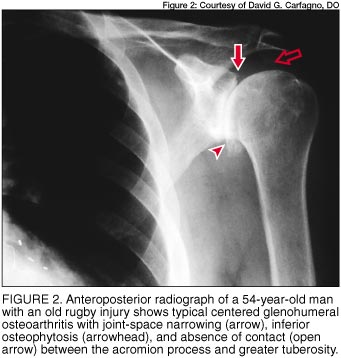
Radiographs are used to confirm the clinical diagnosis of GHOA. Findings may include glenohumeral joint-space narrowing, subchondral bone changes, osteophyte formation, glenoid bone loss, and humeral head displacement (Figure 2). The standard views--scapular anteroposterior and true axillary--demonstrate the relative thickness of the cartilage between the humerus and the glenoid, the relationship between the humeral head and glenoid, and the presence of features such as osteophytes and joint erosion.
Patients who have GHOA should also be evaluated for rotator cuff degeneration. The incidence of partial and full-thickness tears of the rotator cuff in asymptomatic patients is over 50% in patients older than 60. [10] Autopsy studies [14] have revealed that 75% of shoulders with cartilage degeneration also show evidence of attrition or rupture of the cuff. Magnetic resonance imaging or ultrasound may be used to rule out concomitant rotator cuff pathology (seen as an elevation of the humeral head) and must be closely correlated with physical examination findings. Further imaging, including computed tomography, should be reserved for preoperative planning.
Medication Options
Several pharmacologic strategies are available for treating the pain and inflammation of GHOA. Explaining the cause of GHOA pain will help the patient understand the reasoning behind pharmacologic treatment.
Oral agents. Oral medications include acetaminophen; nonsteroidal anti-inflammatory drugs (NSAIDs) including cyclooxygenase-2 (COX-2) inhibitors; and supplements such as chondroitin sulfate and glucosamine. Two studies [14, 15] demonstrate that the short-term efficacy of acetaminophen is comparable to ibuprofen in patients who have OA of the knee. Many physicians prefer COX-2 inhibitors, primarily because they have fewer side effects than traditional NSAIDs.
Oral viscosupplementation is used with all forms of OA. Chondroitin and glucosamine are both over-the-counter supplements. Glucosamine stimulates chondrocyte production and acts as a mild anti-inflammatory. [16] Among more than 30 studies of these supplements (most are small, several are double-blinded, and few are prospective), chondroitin, the most abundant glycosaminoglycan, inhibits degenerative enzymes. There is no definite proof that glucosamine and chondroitin are cartilage protectors, at what stage of OA these supplements are most efficacious, or if glucosamine is more effective when taken with chondroitin. More high-quality, long-term trials in large populations are needed before definitive indications can be established. Patients should be advised that supplements may or may not work, and that side effects, though minimal, may include gastrointestinal distress.
Intra-articular treatments. In the United States, viscosupplementation with hyaluronic acid has become more popular over the past 4 years, primarily for OA of the knee. Some insurance companies allow hyaluronic acid treatments for the shoulder. Hyaluronic acid helps maintain the articular cartilage surface by lubricating and providing a medium to retard the deterioration of the cartilage matrix in degenerative joints. Although many studies have investigated the treatment of OA of the knee with hyaluronic acid, few studies have explored its use for the shoulder.
Leardini et al [17] studied the use of hyaluronic acid injections in 29 patients with shoulder pain. Although not an elaborate study, 23 of the 29 patients who had shoulder pain had varying degrees of OA (not subclassified). Hyaluronic acid injections provided 21 patients with some degree of pain relief and improved ROM. The use of hyaluronic acid in GHOA is based on the parallel findings of the osteoarthritic knee. For now, its use is considered purely empiric.
Intra-articular corticosteroid injections may be used as an adjunct in refractory cases of GHOA if oral anti-inflammatory medications do not result in significant improvement after 4 to 6 weeks. These injections should be used no more than three to four times per year.
Physical Therapy
The primary components of a physical therapy program for patients who have GHOA consist of modalities, ROM exercises, and strength and endurance training. Goals are to improve ROM, rotator cuff stability, and scapular strength. Decreased translation with increased strength will normalize mechanics and vice versa.
Initial goals for the patient who has GHOA are to reduce pain to enable activities of daily living and independence, and to improve ROM and strength. In patients who have unilateral GHOA, the contralateral extremity serves as a goal for regaining ROM and strength.
Therapeutic modalities. Many modalities, such as electrical stimulation, ultrasound, heat, ice, phonophoresis, and iontophoresis, have been used to treat GHOA. During early rehabilitation they are used mainly to reduce pain and increase local blood flow.
Prospective, randomized studies of GHOA patients provide little guidance in the use of therapeutic modalities. Lewis et al [18] reported no significant difference in the analgesic response of electrical stimulation and NSAIDs compared with placebo. White and Sage [19] presented a prospective placebo-controlled study of 14 patients with OA and 16 patients with rheumatoid arthritis. Following application of a topical ointment, 27 of the 30 subjects reported pain relief and a feeling of warmth. Despite limited evidence in the literature regarding modalities, patient reports of pain relief, coupled with decreased muscular inhibition during rehabilitation, warrants limited use. Range of motion. Mobilization and passive stretching are used along with other modalities to decrease abnormal glenohumeral joint shear forces [8] and improve gross ROM of the glenohumeral joint. ROM losses after a shoulder injury follow a predictable pattern described by Cyriax and Cyriax [20] (external rotation, abduction, and internal rotation are most limited, followed by forward flexion). Actively, patients who have GHOA can't forward flex; passively, they will follow this hierarchy of movement.
To address selective capsular tightness caused by capsular adhesions and abnormal ROM patterning, posterior glides of the humeral head relative to the glenoid, with varying degrees of internal rotation of the glenohumeral joint, are used to mobilize the posterior capsule and address limitations in internal glenohumeral joint rotation. Anterior glides of the humeral head are also often used to address limitations in external rotation. Optimization of capsular length between the anterior and posterior capsule may minimize humeral head shear within the glenoid when the glenohumeral joint moves. [8] In addition to glenohumeral joint mobilization, passive stretching using a low load and long duration is also recommended. [21] The effectiveness of manual therapy for patients with knee OA has been studied, with favorable results [22]; however, no such investigation has been done for GHOA.
Strengthening. Of all the nonoperative physical therapy treatments recommended for patients with GHOA, progressive strengthening of the rotator cuff and scapular musculature holds the greatest theoretical advantage. The importance of the rotator cuff muscle-tendon units in controlling and centering the humeral head, especially during midrange movement patterns, cannot be underestimated. [12] Submaximal strengthening exercises that selectively recruit the rotator cuff musculature and exercise patterns that place the shoulder in neutral, nonimpinging positions form the basis for clinic and home-based rehabilitation.
Electromyograph analyses have documented high levels of posterior rotator cuff activation in four exercises--prone extension with external rotation, scapular plane elevation with thumbs down, prone horizontal abduction, and side-lying external rotation. [23, 24] As a general rule, exercises that keep the shoulder below 90° of elevation and the arm anterior to the scapular plane are recommended. Positions with 90° of glenohumeral joint abduction in the coronal plane and 90° of external rotation have been found to increase the joint compressive load and posterior shear forces and may not be indicated for patients with GHOA. [25]
Exercise for the scapula-stabilizing muscles are also indicated. Exercises that strengthen the serratus anterior and lower trapezius are particularly recommended to improve scapular upward rotation during elevation. [5] Patterns with light weights, medicine balls, or resistive bands can be used to perform shoulder punches that emphasize maximal scapular protraction (termed the "plus" position) to recruit the serratus anterior. [12] Scapular retraction exercises, such as rowing with multiple positions of arm abduction, are also indicated.
To improve strength and local muscle endurance, resistive exercises are performed using several sets of 15 to 20 repetitions. A low-resistance, high-repetition strengthening program is used with particular emphasis on proper glenohumeral joint arthrokinematics. Lower resistance levels allow rotator cuff activation with less compensation and shoulder girdle elevation than with higher resistance levels and movement patterns characterized by full, end-range, overhead elevation. Care must be taken to ensure that resistive exercise does not elevate pain levels, which can lead to muscular inhibition and compensation.
References:
Badet R, Boileau P, Noel E, et al: Arthrography and computed arthrotomography study of seventy patients with primary glenohumeral osteoarthritis. Rev Rhum Engl Ed 1995;62(9):555-562
Andrews J: Arthroscopic debridement for glenohumeral arthritis: arthritis of the glenohumeral joint in the young patient, abstracted. American Orthopaedic Society of Sports Medicine Symposium 2000; March, abstract unpublished.
Meachim G: Effect of age on the thickness of adult articular cartilage at the shoulder joint. Ann Rheum Dis 1971;30(1):43-46
Klippel JH, Weyand CM, Wortmann R (eds): Primer on the Rheumatic Diseases, ed 11. Atlanta, Arthritis Foundation, 1997, pp 216-221
Kibler WB: The role of the scapula in athletic shoulder function. Am J Sports Med 1998;26(2):325-337
Solem-Bertoft E, Thuomas KA, Westerberg CE: The influence of scapular retraction and protraction on the width of the subacromial space: an MRI study. Clin Orthop 1993;296(Nov):99-103
Harryman DT II, Sidles JA, Clark JM, et al: Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Joint Surg Am 1990;72(9):1334-1343
Neer CS II: Impingement lesions. Clin Orthop 1983;173(Mar):70-77
Hawkins RJ, Kennedy JC: Impingement syndrome in athletes. Am J Sports Med 1980;8(3):151-158
Hawkins RJ, Bokor DJ: Clinical evaluation of shoulder problems, in Rockwood CA, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, WB Saunders, 1998, pp 164-196
Altchek DW, Skyhar MJ, Warren RF: Shoulder arthroscopy for shoulder instability. Instr Course Lect 1989;38:187-198
Lee SB, Kim KJ, O'Driscoll SW, et al: Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion: a study in cadavera. J Bone Joint Surg Am 2000;82(6):849-857
Petersson CJ: Degeneration of the gleno-humeral joint: an anatomical study. Acta Orthop Scand 1983;54(2):277-283
Bradley JD, Brandt KD, Katz BP, et al: Comparison of an antiinflammatory dose of ibuprofen, an analgesic dose of ibuprofen, and acetaminophen in the treatment of patients with osteoarthritis of the knee. N Engl J Med 1991;325(2):87-91
Williams HJ, Ward JR, Egger MJ, et al: Comparison of naproxen and acetaminophen in a two-year study of treatment of osteoarthritis of the knee. Arthritis Rheum 1993;36(9):1196-1206
Reginster JY, Deroisy R, Rovati LC, et al: Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomized, placebo-controlled, clinical trial. Lancet 2000;357(9252):251-256
Leardini G, Perbellini A, Franceschini M, et al: Intra-articular injections of hyaluronic acid in the treatment of painful shoulder. Clin Ther 1988;10(5):521-526
Lewis B, Lewis D, Cumming G: The comparative analgesic efficacy of transcutaneous electrical nerve stimulation and a non-steroidal anti-inflammatory drug for painful osteoarthritis. Br J Rheumatol 1994;33(5):455-460
White JR, Sage JN: Effects of a counterirritant on muscular distress in patients with arthritis. Phys Ther 1971;51(1):36-42
Cyriax J, Cyriax P: Illustrated Manual of Orthopaedic Medicine. London, Butterworths, 1983
Bonutti PM, Windau JE, Ables BA, et al: Static progressive stretch to reestablish elbow range of motion. Clin Orthop 1994;303(Jun):128-134
Deyle GD, Henderson NE, Matekel RL, et al: Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med 2000;132(3):173-181
Townsend H, Jobe FW, Pink M, et al: Electromyographic analysis of the glenohumeral muscles during a baseball rehabilitation program. Am J Sports Med 1991;19(3):264-272
Moseley JB Jr, Jobe FW, Pink M, et al: EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med 1992;20(2):128-134
Conzen A, Eckstein F: Quantitative determination of articular pressure in the human shoulder joint. J Shoulder Elbow Surg 2000;9(3):196-204
Dr Carfagno is an internist at Southwest Sports Medicine and Orthopaedic Surgery Clinic, Ltd in Scottsdale, Arizona and holds a certificate of added qualifications in sports medicine. Mr Ellenbecker is a physical therapist and clinic director at Physiotherapy Associates Scottsdale Sports Clinic in Scottsdale. Address correspondence to David G. Carfagno, DO, Southwest Sports Medicine and Orthopaedic Surgery Clinic, Ltd, 9023 E Desert Cove, #101, Scottsdale, AZ 85260; e-mail to sports7doc@aol.com.
Disclosure information: Dr Carfagno and Mr Ellenbecker disclose no significant relationship with any manufacturer of any commercial product mentioned in this article. No drug is mentioned in this article for an unlabeled use.
Copyright (C) 2002. The McGraw-Hill Companies. All Rights Reserved
