

Illness Perceptions and Healthcare Use Among People
with Low Back Pain in General PracticeThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Musculoskelet Sci Pract 2026 (Jun 15): 84: 103602 ~ FULL TEXT
OPEN ACCESS Bodil A Arnbak • Jan Hartvigsen • John S Andersen • Anne Mřller • Birgitte Nřrgaard • Alice Kongsted
Center for Muscle and Joint Health,
Department of Sports Science and Clinical Biomechanics,
University of Southern Denmark,
Denmark
Background: Illness perceptions, reflecting cognitive and emotional representation of a condition, may influence how people with low back pain (LBP) seek care. Evidence in this area remains limited. This study examines whether illness perceptions are associated with healthcare visits and diagnostic imaging in people seeking care for LBP.
Design and methods: In this prospective cohort study, patients consulting general practice for LBP completed the Brief Illness Perception Questionnaire (BIPQ; 0-80) at baseline. Two outcomes were assessed after three months: repeated healthcare visits (≥2 vs < 2 visits) and diagnostic imaging (X-ray, CT, or MRI; yes/no). Associations were analysed using logistic regression, adjusted for baseline pain intensity, disability, and episode duration.
Results: Analysis included 214 adults (mean age, 55 years; 56% women). At three-month follow-up, 31% had ≥2 healthcare visits, and 19% had undergone diagnostic imaging. More threatening illness perceptions were associated with multiple healthcare visits (adjusted OR 1.04 per BIPQ point; 95% CI, 1.00-1.07) and diagnostic imaging (adjusted OR 1.04 per point; 95% CI, 1.00-1.08). The estimated odds corresponded to predicted probabilities increasing from 26% to 36% of healthcare visits and from 14% to 22% for imaging, comparing the highest and lowest BIPQ quartiles. For individual BIPQ items, emotional response (BIPQ8) was associated with visits, whereas recovery expectations (BIPQ2) were associated with diagnostic imaging.
Conclusion: Illness perceptions were associated with healthcare visits and diagnostic imaging in people with LBP, independent of pain, disability, and episode duration, and addressing these perceptions may support guideline-concordant care.
Keywords: Diagnostic imaging; Healthcare utilisation; Illness perceptions; Low back pain; Primary care.
Highlights
Threatening illness perceptions [are] associated with increased healthcare use.
Associations were independent of pain, disability, and episode duration.
Stronger emotional impact of back pain related to repeated consultations.
Expecting back pain to last a long time related to [use of] diagnostic imaging.
Addressing illness perceptions may support guideline-concordant care.
From the FULL TEXT Article:
Introduction
Psychological and social factors are recognised as important contributors to the course and prognosis of low back pain (LBP) (Otero-Ketterer et al., 2022; Cruz et al., 2020). Among these, people's illness perceptions, i.e., their cognitive and emotional understanding of the condition, have received increasing attention in recent years. According to the Common-Sense Model of Self-Regulation, illness perceptions influence coping strategies, health behaviour, and ultimately outcomes (Leventhal et al., 2016).
More threatening illness perceptions - such as strong beliefs about severe consequences, long duration, or lack of control - have been associated with higher pain intensity, poorer function, and maladaptive coping (Kragting et al., 2024; Ginnerup-Nielsen et al., 2022; de Raaij et al., 2018; Gron et al., 2019; Glattacker et al., 2013; Fors et al., 2022).
In contrast, more positive perceptions, such as stronger personal control, are associated with a more positive prognosis (Fors et al., 2022; Unal et al., 2019; Foster et al., 2008; Leysen et al., 2018). A widely used instrument to assess illness perceptions is the Brief Illness Perception Questionnaire (BIPQ) (Broadbent et al., 2006), which has demonstrated acceptable measurement properties across conditions (Broadbent et al., 2015).
Illness perceptions may also affect healthcare-seeking behaviour. When symptoms are viewed as serious, long-lasting, or poorly controlled, people may be more likely to consult healthcare providers and seek diagnostic testing (Morton et al., 2021). This is particularly relevant in people with LBP, where clinical guidelines emphasise self-management and staying active, recommend attention to psychosocial factors, and discourage routine diagnostic imaging (WHO guidelines on the management, 2023). People's perceptions influence expectations of care, interpretation of symptoms, and willingness to accept reassurance without further testing (Lullo et al., 2025).
Many people with LBP consult multiple healthcare providers, suggesting that their needs and expectations may not be fully met, and a substantial proportion undergo diagnostic imaging, despite evidence that routine imaging does not improve clinical outcomes (WHO guidelines on the management, 2023; Hall et al., 2021). When people hold strong beliefs about severe consequences or the need for diagnostic certainty, clinicians may feel pressured to provide imaging or other interventions not recommended by guidelines (Sharma et al., 2020; Robinson et al., 2025; De Silva et al., 2023; Haslam-Larmer et al., 2025).
Recognising illness perceptions may help clinicians anticipate barriers and tailor communication to patients’ concerns, potentially supporting more guideline-concordant care (Hagger et al., 2017). Across different conditions, illness perceptions have been associated with health-related behaviours that influence how people seek and utilise healthcare (Petrie et al., 2007; Fahrni et al., 2022; Frostholm et al., 2005). However, previous studies have often relied on cross-sectional designs or have focused primarily on pain and disability outcomes (de Raaij et al., 2018; Morton et al., 2019). In addition, most existing evidence comes from heterogeneous populations and settings, and relatively few studies have examined healthcare utilisation in relation to illness perceptions specifically among people consulting general practice for LBP (Morton et al., 2021; Huysmans et al., 2020).
Because illness perceptions are closely intertwined with symptom experiences, clinical factors such as symptom severity and duration may influence both illness perceptions and healthcare utilisation, highlighting the importance of accounting for these characteristics when examining their association (Morton et al., 2019).
This study examined whether the way people think and feel about their LBP at the time of a general practitioner (GP) consultation was associated with subsequent healthcare use, including repeat healthcare visits and diagnostic imaging, after accounting for baseline pain intensity, disability, and episode duration.
Methods
Study design and setting
This was a longitudinal analysis of data from a prospective observational cohort study conducted in Danish general practice (Arnbak et al., 2024). Data collection and storage were approved by SDU Research & Innovation Organization (RIO) (ref. no. 11.481), and ethical approval was obtained from SDU Research Ethics Committee (ref. no. 22/37275). All participants provided written informed consent.
General practice clinics were recruited through telephone contact, practice visits, promotion at courses and seminars, and via the project website. Participating GPs were compensated for their time spent on data collection and patient recruitment, according to the agreement on physician remuneration between Danish Regions and the Danish Organization of General Practitioners. A total of 42 clinics participated between August 2022 and June 2023. Patient management followed usual care in Danish general practice, and no specific diagnostic or treatment protocol was imposed as part of the study.
Participants
Adults aged 18 years or older consulting their GP for LBP, with or without leg pain, were invited to participate. To reflect the range of LBP presentations seen in Danish general practice, patients with both acute and persistent LBP were eligible, regardless of whether the consultation was their first or a subsequent consultation for the current LBP episode. Participants were required to be able to provide informed consent and complete the study questionnaire. Patients received no compensation.
Data collection
At enrolment, questionnaires were distributed via the secure Danish electronic mailing system (e-Boks) and completed electronically using REDCap, hosted by the Open Patient Data Explorative Network (Harris et al., 2009). Follow-up questionnaires were distributed 3 months after the baseline consultation.
Baseline measures
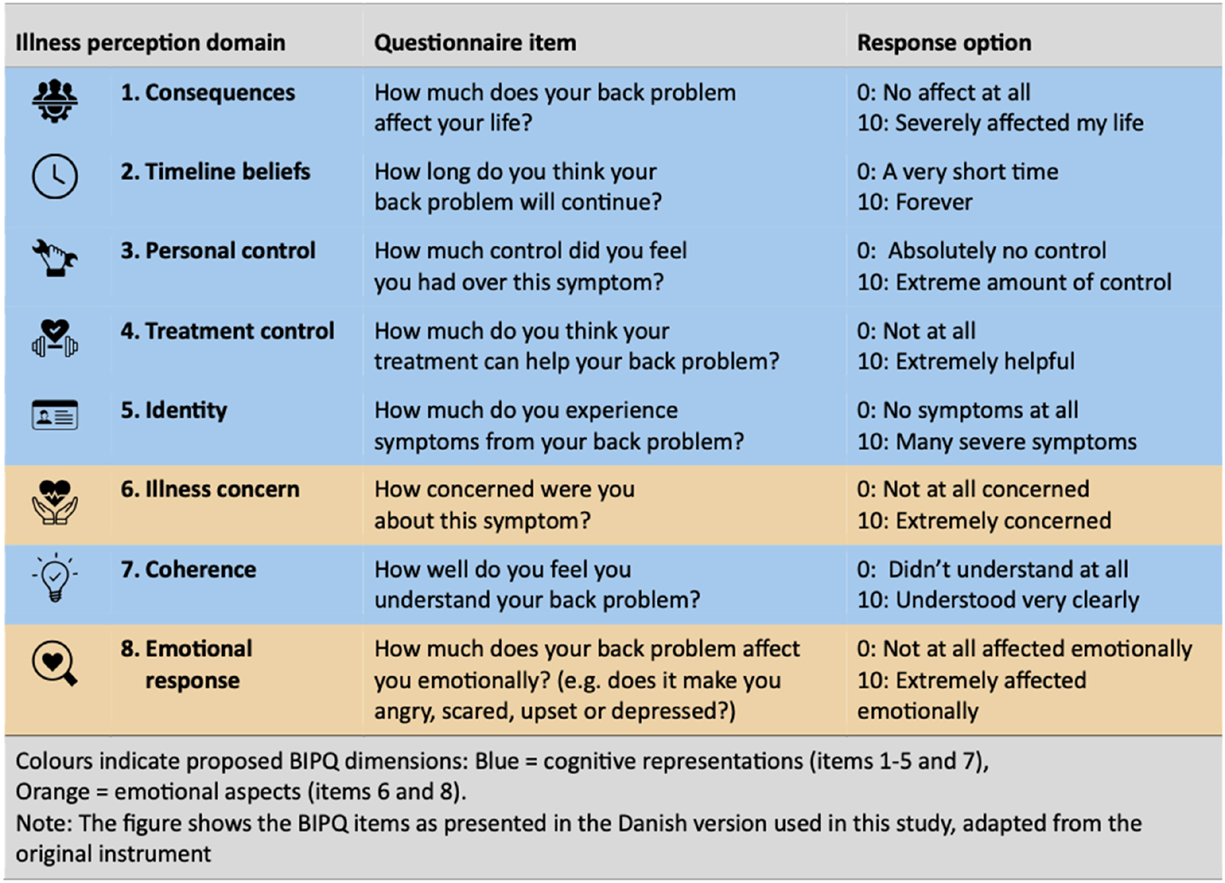
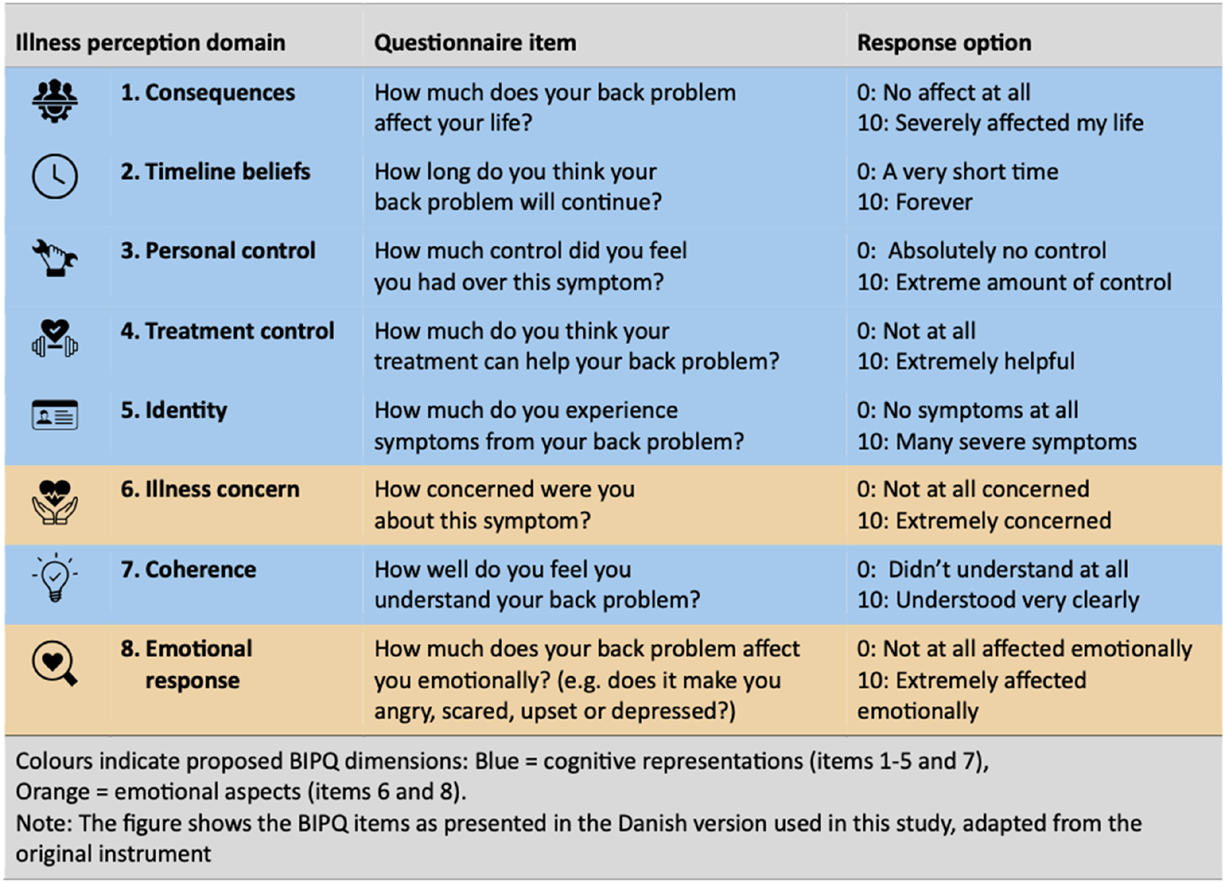
Figure 1 Illness perceptions: At baseline, patients completed the Brief Illness Perception Questionnaire (BIPQ) (Broadbent et al., 2006), a brief and widely used instrument with acceptable psychometric properties across several conditions (Broadbent et al., 2015). The Danish version has been used in Danish musculoskeletal populations, and its measurement properties have been examined in these populations (Ginnerup-Nielsen et al., 2022, 2024). The questionnaire consists of eight items scored on a numeric rating scale (0-10). The questionnaire covers cognitive (consequences, timeline, personal control, treatment control, identity, coherence) and emotional representations (concern, emotional response) of illness (Figure 1). A total score (range 0-80) was calculated by summing all items, reversing items 3, 4, and 7, with higher scores indicating a more threatening perception.
Clinical covariates: Pain intensity was assessed using a 0-10 Numeric Rating Scale (NRS) reflecting participants’ typical LBP during the past week (0 = no pain, 10 = worst imaginable pain) (Manniche et al., 1994). Disability was measured using the Oswestry Disability Index (ODI) (Lauridsen et al., 2006). Participants reported how long ago their current back pain had started, i.e., the duration of their current pain episode up to the time of the consultation. Duration was categorised as 1-7 days, 1 week to 3 months, 3-12 months, or >1 year and included as a covariate in the analyses to account for differences in symptom duration.
Outcome measures
At the three-month follow-up, healthcare utilisation was assessed with two questions:1) “How many times in the past month have you, because of your LBP, consulted your GP, chiropractor, physiotherapist, municipal rehabilitation, hospital, or other healthcare providers?”
(Response options: 0 times, 1 time, 2-5 times, 6-10 times, more than 10 times).
2) “During the past three months, have you had any imaging or surgery because of your LBP?”
(response options: X-ray, MRI scan, CT scan, back surgery, none of these; response options for each item: yes/no).For the present study, only the responses regarding imaging were used as the outcome variable. Outcomes were dichotomised as ≥2 vs. <2 visits to healthcare providers, and any imaging (X-ray, MRI, or CT) vs. no imaging. The cut-off for healthcare visits was chosen to distinguish between single, potentially routine consultations and repeated care-seeking.
Statistical analysis
Data analysis was performed using STATA 18.0 (StataCorp, College Station, TX, USA).
Internal consistency of the total score was assessed using McDonald's omega, which indicated acceptable reliability (ω = 0.76), and the total score was used alongside item-level analyses.

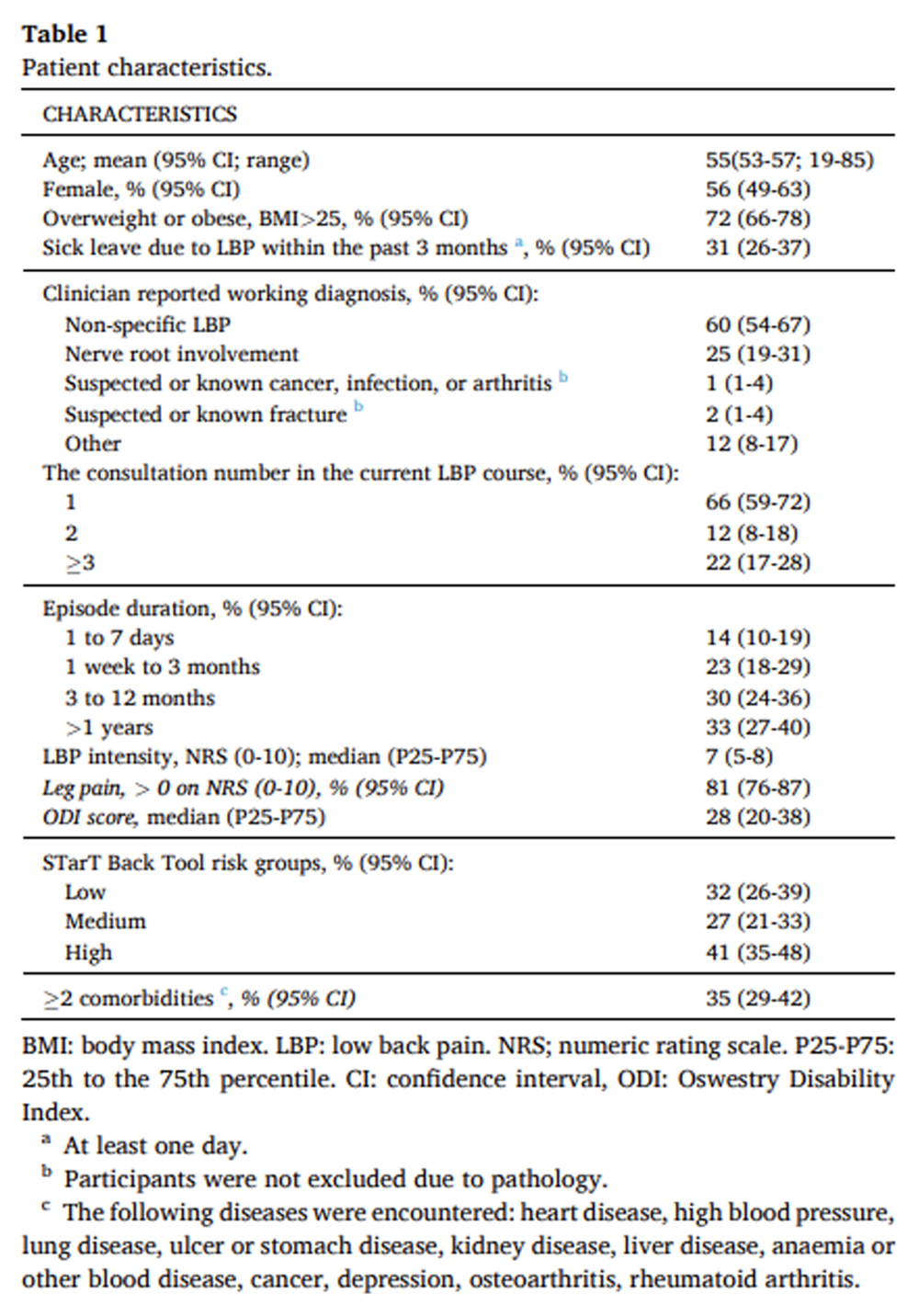
Table 1 Only patients with complete data on exposure, outcomes, and covariates were included in the analyses. Descriptive statistics were used to summarise patient characteristics, and differences in baseline characteristics (variables included in Table 1) between included and non-included patients were compared using Mann-Whitney U-tests for continuous variables and chi-square tests for categorical variables.
Associations between illness perceptions (total score and each BIPQ item) and healthcare utilisation outcomes were analysed using logistic regression models.
Analyses were conducted unadjusted and adjusted for baseline pain intensity (NRS), baseline disability (ODI), and episode duration, as these clinical factors could plausibly influence both illness perceptions and healthcare utilisation.
Age and sex were considered in the analytical planning but were not included in the primary models. In our conceptual model, age and sex were considered more distal factors that may influence healthcare utilisation partly through their influence on illness perceptions.
Given the sample size, we prioritised adjustment for the most clinically relevant confounders. Models including age and sex were also analysed to assess whether their inclusion influenced the results.
Results are reported as odds ratios (OR) with 95% confidence intervals (CI). We also estimated predicted probabilities to illustrate the absolute differences associated with varying illness perception scores, as the OR represents the change per one-point increase in the BIPQ score (range 0–80).
Sample size was determined by the available participants from the parent cohort; no formal sample size calculation was performed for this analysis.
Results
Patient characteristics
A total of 294 patients were enrolled in the original cohort. Of these, 214 (73%) had complete three-month follow-up data and were therefore included in the present analyses; the remaining 80 patients were excluded due to missing follow-up data.
The included participants had a mean age of 55 years (range 19-85); 56% were female (Table 1). A total of 63% reported a current LBP duration exceeding one month. For most participants (66%), the baseline consultation represented their first GP visit for the current LBP episode. The most common working diagnosis was non-specific LBP (60%), followed by nerve root compression (25%). Diagnoses indicating known or suspected serious pathology, including cancer, infection, arthritis, or fracture, were reported in 1-2% of patients. The remaining responses (12%) were categorised as ‘other’.
Included patients were older (mean age 55 years, 95% CI 53-57) compared with non-included patients (49 years, 95% CI 45-52), were more often overweight or obese (72%, 95% CI 66-78 vs. 51%, 95% CI 40-62), more frequently reported leg pain (81%, 95% CI 76-87 vs. 71%, 95% CI 60-81), and had a higher prevalence of multiple comorbidities (35%, 95% CI 29-42 vs. 20%, 95% CI 13-30). Baseline episode duration also differed between included and non-included patients, with fewer included patients reporting a short symptom duration of 1-7 days (14% vs 29%).
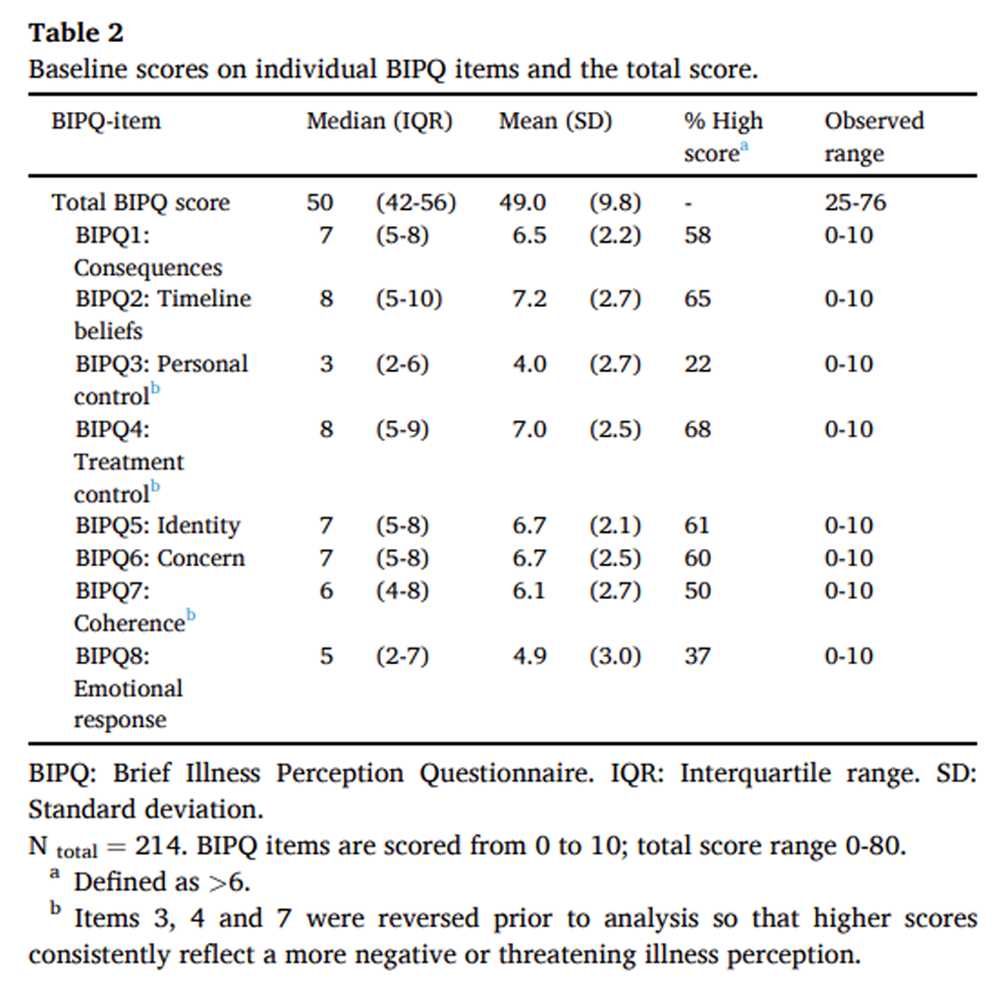
Table 2 Participants’ responses showed clear variation across BIPQ items (Table 2). Timeline beliefs (BIPQ2) and treatment control (BIPQ4) had both high mean scores (7.2 and 7.0, respectively) and the largest proportions of participants scoring >6 (65% and 68%). In contrast, personal control (BIPQ3) and emotional response (BIPQ8) had the lowest mean scores (4.0 and 4.9) and comparatively few scores >6 (22% and 37%). The mean total BIPQ score was 49.0 (SD 9.8).
At three months follow-up, 67 patients (31%) had two or more visits to healthcare providers during the previous month, and 40 patients (19%) had undergone diagnostic imaging since baseline.
Associations with healthcare use
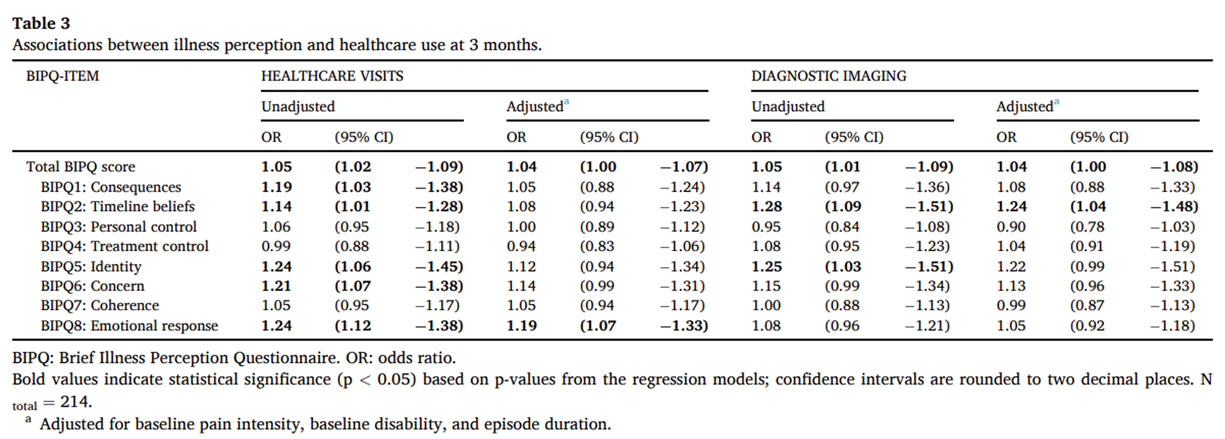
More threatening illness perception scores were associated with increased healthcare utilisation within three months (Table 3). In addition to odds ratios, we estimated predicted probabilities to illustrate the magnitude of these associations. The total BIPQ score was associated with healthcare use in both unadjusted and adjusted analyses (adjusted OR, 1.04 per point; 95% CI, 1.00-1.07). These estimates corresponded to increases in the predicted probability of healthcare use from 26% (95% CI 18-33%) in the lowest BIPQ quartile (≤42) to 36% (95% CI 28-44%) in the highest quartile (≥56).
Table 3 Among the individual items, consequences (BIPQ1), timeline beliefs (BIPQ2), identity (BIPQ5), concern (BIPQ6), and emotional response (BIPQ8) were all related to higher healthcare use in the unadjusted analyses. After adjustment, only the association with emotional response (BIPQ8, OR 1.19 per point, 95% CI 1.07-1.33) remained significant (Table 3).
Associations with diagnostic imaging
A similar pattern was observed for diagnostic imaging (Table 3). The total BIPQ score was associated with imaging in both unadjusted and adjusted analyses (adjusted OR 1.04 per point, 95% CI 1.00-1.08). The corresponding predicted probabilities increased from 14% (95% CI 8-20%) in the lowest quartile (≤42) to 22% (95% CI 16-29%) in the highest quartile (≥56).
Among individual items, timeline beliefs (BIPQ2) and identity (BIPQ5) were significantly associated with higher odds of imaging in unadjusted analyses, while only timeline beliefs (BIPQ2) remained significant after adjustment (OR 1.24 per point, 95% CI 1.05-1.48).
Additional adjustment for age and sex resulted in similar effect estimates and did not change the overall pattern of results for either healthcare visits or diagnostic imaging (Supplemental Table S1).
Discussion
In this study, we found that people consulting their GP for LBP who had more threatening illness perceptions were more likely to use healthcare services within three months than those with less threatening illness perceptions, independent of baseline pain, disability, and episode duration. The estimated odds ratio corresponded to an increase in the predicted probability of multiple healthcare visits from 26% in the lowest quartile of BIPQ scores to 36% in the highest quartile. For diagnostic imaging, the corresponding probabilities were 14% and 22%, respectively. These findings suggest that the way people emotionally respond to, and form expectations about their condition, may contribute to healthcare-seeking behaviour in LBP, as one element within a broader and multifaceted pattern of influences.
Our findings are consistent with previous research showing that more negative illness perceptions are associated with increased healthcare-seeking behaviour, both in general practice and in other primary care settings (de Raaij et al., 2018; Frostholm et al., 2005). Most studies in people with LBP have focused on associations with pain, disability, or quality of life (Fors et al., 2022; Unal et al., 2019; Foster et al., 2008; Leysen et al., 2018; Hallegraeff et al., 2021), while few have addressed healthcare use (Morton et al., 2019). One population-based study identified distinct clusters of illness perceptions among individuals with back pain, where more threatening perceptions were associated with greater healthcare use and less self-care (Morton et al., 2021). However, those effect estimates were based on comparisons between cluster groups and are therefore not directly comparable to the continuous BIPQ-based estimates in the present study (Morton et al., 2021). The present study extends this by showing that specific cognitive and emotional illness perceptions were associated with both subsequent healthcare visits and diagnostic imaging over time.
The associations observed were not uniform across BIPQ items, with emotional response linked to healthcare use and timeline beliefs to imaging. Previous research has shown that longer symptom duration is associated with stronger beliefs that imaging is necessary (Jenkins et al., 2022). Our findings extend this by indicating that expectations of long duration were associated with imaging even after adjusting for actual symptom length, suggesting that perceived persistence rather than actual symptom history may influence the perceived need for imaging. This pattern may reflect that people who perceive their LBP as emotionally distressing have unmet needs for support. In comparison, those expecting a long-lasting problem may be particularly motivated to request diagnostic imaging as a means of obtaining an explanation for their pain (Hayden et al., 2019; Lim et al., 2019).
Given current guideline recommendations discouraging routine imaging (WHO guidelines on the management, 2023), it is known that patients’ beliefs may partly drive the demand for diagnostic imaging (Jenkins et al., 2022). A better understanding of these perceptions and how they influence consultations in general practice could help reduce unnecessary imaging, support guideline-concordant care, and limit low-value practices (WHO guidelines on the management, 2023; Hall et al., 2021; Kjelle et al., 2024). Open discussions about expected symptom course, the role of self-management, and the limited benefits of imaging may not only validate patient concerns but also enhance trust, reduce patient anxiety, and promote adherence to active treatment strategies rather than passive investigation (Lim et al., 2019; Cashin et al., 2022; Traeger et al., 2015). Interventions commonly recommended for LBP - such as patient education, cognitive functional therapy, cognitive-behavioural approaches, and reassurance-based communication - can influence illness perceptions and related beliefs, which may contribute to improved engagement and reduced anxiety (Cashin et al., 2021, 2022; Traeger et al., 2015; Alaiti et al., 2022).
Healthcare utilisation is driven by a complex interplay of factors, often conceptualised within the Behavioural Model of Health Services Use, which integrates predisposing, enabling, and need-related factors (Andersen, 1995). Illness perceptions may contribute particularly to the perceived-need component by shaping how people interpret their symptoms and decide when care is required (Huysmans et al., 2020; Esteve et al., 2020; Ferreira et al., 2010). Future studies should aim to clarify how people form and maintain these perceptions, and how clinicians can address them in practice. It would also be valuable to examine how illness perceptions interact with clinical, biological, and broader contextual factors in shaping healthcare-seeking and recovery trajectories.
A strength of this study is the use of a well-characterised cohort of people with LBP recruited directly from general practice, which enhances the clinical relevance. The follow-up rate was acceptable (73%), and although the included patients were slightly older and somewhat more clinically burdened on some measures than non-responders, attrition bias is unlikely to have substantially influenced the associations. The use of a widely used instrument (BIPQ) to assess illness perceptions enables comparison with previous research across different conditions. Although the BIPQ has yielded mixed findings regarding dimensionality in previous studies (Broadbent et al., 2015), the internal consistency in this sample was acceptable, supporting the use of the total score as a summary measure. Moreover, defining healthcare utilisation through both healthcare visits and diagnostic imaging provides a comprehensive perspective on how patient beliefs may influence care pathways in LBP.
This study also has limitations to consider. The findings are intended to inform understanding of illness perceptions and healthcare utilisation among people with LBP who seek care in general practice. Associations likely differ across healthcare systems and patient populations, and replication in other contexts is warranted. Participating practices and non-consecutive patient inclusion may also have introduced selection bias, although this is unlikely to have affected the patient-level associations examined. In addition, healthcare utilisation was self-reported, and the questionnaire did not distinguish between patient-initiated consultations and visits scheduled as part of ongoing treatment plans. The measure, therefore, reflects overall healthcare utilisation rather than patient-initiated care-seeking alone. The Danish BIPQ has not been systematically validated in Danish LBP populations, which may have introduced some measurement uncertainty.
The study population included patients with varying symptom durations, reflecting presentations typically seen in general practice. Illness perceptions may differ depending on pain intensity and symptom duration, as prolonged or severe pain experiences may influence expectations and concerns. Baseline pain intensity and symptom duration were therefore included as covariates in the analyses.
Age and sex were considered during the analytical planning; however, given the sample size, we limited the number of covariates in the adjusted models and prioritised clinical factors considered most directly related to both illness perceptions and healthcare utilisation. Additional analyses, including age and sex, showed similar effect estimates and did not change the overall pattern of results, suggesting that confounding by age and sex was limited in this study. However, residual confounding by other unmeasured factors cannot be ruled out. In addition, previous diagnostic imaging for LBP before study enrolment may have influenced both patient expectations and clinicians’ decisions regarding further imaging and may therefore have affected imaging utilisation during follow-up.
In conclusion, this study shows that how people think and feel about their LBP may influence their use of healthcare services, including repeat consultations and diagnostic imaging, even when accounting for pain, disability, and symptom duration. Emotional reactions and expectations of prolonged symptoms were particularly influential, underscoring the relevance of discussing these concerns during consultations. While these perceptions represent just one element within a broader set of factors influencing healthcare behaviour, even small individual-level associations may accumulate into a meaningful overall impact given the high prevalence of LBP and frequent healthcare use. A better understanding of these perceptions may support clearer communication, help align care with guidelines, and reduce unnecessary imaging, while also highlighting the need for future work on how such beliefs develop and how best to address them in clinical practice.
Ethics and data protection
The project was carried out according to responsible research practice. Participation was voluntary, and all participants gave their written informed consent; patients’ management and treatment were not affected by participation. Data collection and storage were approved by SDU Research & Innovation Organization (RIO) (ref. no. 11.481), and the study received ethical approval from SDU Research Ethics Committee (ref. no.: 22/37275).
Appendix A Supplementary data
Ethics and data protection
The project was carried out according to responsible research practice. Participation was voluntary, and all participants gave their written informed consent; patients’ management and treatment were not affected by participation. Data collection and storage were approved by SDU Research & Innovation Organization (RIO) (ref. no. 11.481), and the study received ethical approval from SDU Research Ethics Committee (ref. no.: 22/37275).
Funding
The Danish Regions funded the study. The funders had no role in the design, conduct, analysis, or reporting of the study.
CRediT authorship contribution statement
Bodil A. Arnbak: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing.
Jan Hartvigsen: Conceptualization, Methodology, Writing – review & editing.
John S. Andersen: Conceptualization, Methodology, Writing – review & editing.
Anne Mřller: Conceptualization, Methodology, Writing – review & editing.
Birgitte Nřrgaard: Conceptualization, Methodology, Writing – review & editing.
Alice Kongsted: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
Bodil Arnbak reports financial support was provided by The Danish Regions.
The other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
We would like to thank the patients, clinic staff and GPs who participated and contributed to this study.
References:
Alaiti, R.K. Castro, J. Lee, H.
What are the mechanisms of action of cognitive-behavioral, mind-Body, and exercise-based interventions for pain and disability in people with chronic primary musculoskeletal pain?: a systematic review of mediation studies from randomized controlled trials
Clin. J. Pain. 2022; 38:502-509Andersen, R.M.
Revisiting the behavioral model and access to medical care: does it matter?
J. Health Soc. Behav. 1995; 36:1-10Arnbak, B.A. Jensen, T.S. Lund, R.A.
Usual care for low back pain and barriers to best practice: a cross-sectional study in Danish general practice
Muscoskel. Care. 2024; 22:e1911Broadbent, E. Petrie, K.J. Main, J.
The brief illness perception questionnaire
J. Psychosom. Res. 2006; 60:631-637Broadbent, E. Wilkes, C. Koschwanez, H.
A systematic review and meta-analysis of the Brief Illness Perception Questionnaire
Psychol. Health. 2015; 30:1361-1385Cashin, A.G. Lee, H. Traeger, A.C.
Feeling reassured after a consultation does not reduce disability or healthcare use in people with acute low back pain: a mediation analysis of a randomised trial
J. Physiother. 2021; 67:197-200Cashin, A.G. Lee, H. Traeger, A.C.
Producing clinically meaningful reductions in disability: a causal mediation analysis of a patient education intervention
J. Pain. 2022; 23:236-247Cruz, E.B. Canhao, H. Fernandes, R.
Prognostic indicators for poor outcomes in low back pain patients consulted in primary care
PLoS One. 2020; 15, e0229265de Raaij, E.J. Ostelo, R.W. Maissan, F.
The Association of Illness Perception and prognosis for pain and physical function in patients with noncancer musculoskeletal pain: a systematic literature review
J. Orthop. Sports Phys. Ther. 2018; 48:789-800De Silva, L. Baysari, M. Keep, M.
Patients' requests for radiological imaging: a qualitative study on general practitioners' perspectives
Health Expect. 2023; 26:2453-2460Esteve, R. Lopez-Martinez, A.E. Ruiz-Parraga, G.T.
Pain acceptance and pain-related disability predict healthcare utilization and medication intake in patients with non-specific chronic spinal pain
Int J Environ Res Public Health. 2020; 17Fahrni, M.L. Saman, K.M. Alkhoshaiban, A.S.
Patient-reported outcome measures to detect intentional, mixed, or unintentional non-adherence to medication: a systematic review
BMJ Open. 2022; 12, e057868Ferreira, M.L. Machado, G. Latimer, J.
Factors defining care-seeking in low back pain--a meta-analysis of population based surveys
Eur. J. Pain. 2010; 14:747 e1-7Fors, M. Oberg, B. Enthoven, P.
The association between patients' illness perceptions and longitudinal clinical outcome in patients with low back pain
Pain Rep. 2022; 7:e1004Foster, N.E. Bishop, A. Thomas, E.
Illness perceptions of low back pain patients in primary care: what are they, do they change and are they associated with outcome?
Pain. 2008; 136:177-187Frostholm, L. Fink, P. Christensen, K.S.
The patients' illness perceptions and the use of primary health care
Psychosom. Med. 2005; 67:997-1005Ginnerup-Nielsen, E. Bandak, E. Bartholdy, C.
Validity of the Brief Illness Perception Questionnaire in people with knee pain: a Rasch analysis
Scand. J. Rheumatol. 2024; 53:63-71Ginnerup-Nielsen, E. Harreby, M. Christensen, R.
The correlation between illness perception, pain intensity and quality of life in elderly with low back pain in Denmark: a cross-sectional study
PeerJ. 2022; 10, e14129Glattacker, M. Heyduck, K. Meffert, C.
Illness beliefs and treatment beliefs as predictors of short-term and medium-term outcome in chronic back pain
J. Rehabil. Med. 2013; 45:268-276Gron, S. Jensen, R.K. Jensen, T.S.
Back beliefs in patients with low back pain: a primary care cohort study
BMC Musculoskelet. Disord. 2019; 20:578Hagger, M.S. Koch, S. Chatzisarantis, N.L.D.
The common sense model of self-regulation: Meta-analysis and test of a process model
Psychol. Bull. 2017; 143:1117-1154Hall, A.M. Aubrey-Bassler, K. Thorne, B.
Do not routinely offer imaging for uncomplicated low back pain
BMJ. 2021; 372:n291Hallegraeff, J.M. van Trijffel, E. Kan, R.W.
Illness perceptions as an independent predictor of chronic low back pain and pain-related disability: a prospective cohort study
Physiotherapy. 2021; 112:72-77Harris, P.A. Taylor, R. Thielke, R.
Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support
J Biomed Inform. 2009; 42:377-381Haslam-Larmer, L. Norman, K.E. Patey, A.M.
"It's hard to trust an individual, it's easier to trust an image"-patients with low back pain want imaging as a means of coping with uncertainty
BMC Prim. Care. 2025; 26:332Hayden, J.A. Wilson, M.N. Riley, R.D.
Individual recovery expectations and prognosis of outcomes in non-specific low back pain: prognostic factor review
Cochrane Database Syst. Rev. 2019; 2019Huysmans, E. Leemans, L. Beckwee, D.
The relationship between cognitive and emotional factors and healthcare and medication use in people experiencing pain: a systematic review
J. Clin. Med. 2020; 9Jenkins, H.J. Kongsted, A. French, S.D.
Patients with low back pain presenting for chiropractic care who want diagnostic imaging are more likely to receive referral for imaging: a cross-sectional study
Chiropr. Man. Therap. 2022; 30:16Kjelle, E. Brandsaeter, I.O. Andersen, E.R.
Cost of low-value imaging worldwide: a systematic review
Appl Health Econ Health Policy. 2024; 22:485-501Kragting, M. Pool-Goudzwaard, A.L. Coppieters, M.W.
Illness perceptions in people with chronic and disabling non-specific neck pain seeking primary healthcare: a qualitative study
BMC Musculoskelet. Disord. 2024; 25:179Lauridsen, H.H. Hartvigsen, J. Manniche, C.
Danish version of the Oswestry Disability Index for patients with low back pain. Part 1: Cross-cultural adaptation, reliability and validity in two different populations
Eur. Spine J. 2006; 15:1705-1716Leventhal, H. Phillips, L.A. Burns, E.
The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management
J. Behav. Med. 2016; 39:935-946Illness perceptions explain the variance in functional disability, but not habitual physical activity, in patients with chronic low back pain: a cross-sectional Study
Pain Pract. 2018; 18:523-531Lim, Y.Z. Chou, L. Au, R.T.
People with low back pain want clear, consistent and personalised information on prognosis, treatment options and self-management strategies: a systematic review
J. Physiother. 2019; 65:124-135Lullo, G. Giannotta, G. Tamborrino, A.
"Do I need an imaging?" exploring why patients with non-specific chronic low back pain request diagnostic instrumental evaluation: a phenomenological qualitative study
Musculoskelet Sci Pract. 2025; 80, 103416Manniche, C. Asmussen, K. Lauritsen, B.
Low Back Pain Rating scale: validation of a tool for assessment of low back pain
Pain. 1994; 57:317-326Morton, L. de Bruin, M. Krajewska, M.
Beliefs about back pain and pain management behaviours, and their associations in the general population: a systematic review
Eur. J. Pain. 2019; 23:15-30Morton, L. de Bruin, M. Macfarlane, G.J.
Illness perceptions and illness behaviours in back pain: a cross-sectional cluster analysis
Eur. J. Pain. 2021; 25:1948-1958Otero-Ketterer, E. Penacoba-Puente, C. Ferreira Pinheiro-Araujo, C.
Biopsychosocial factors for chronicity in individuals with non-specific low back pain: an umbrella review
Int J Environ Res Public Health. 2022; 19Petrie, K.J. Jago, L.A. Devcich, D.A.
The role of illness perceptions in patients with medical conditions
Curr Opin Psychiatry. 2007; 20:163-167Robinson, C.A. Gosdin, M.M. Cipri, C.S.
Facilitators and barriers to deferring imaging for acute low back pain: a qualitative study
BMC Prim. Care. 2025; 26:204Sharma, S. Traeger, A.C. Reed, B.
Clinician and patient beliefs about diagnostic imaging for low back pain: a systematic qualitative evidence synthesis
BMJ Open. 2020; 10, e037820Traeger, A.C. Hubscher, M. Henschke, N.
Effect of primary care-based education on reassurance in patients with acute low back pain: systematic review and meta-analysis
JAMA Intern. Med. 2015; 175:733-743Unal, O. Akyol, Y. Tander, B.
The relationship of illness perceptions with demographic features, pain severity, functional capacity, disability, depression, and quality of life in patients with chronic low back pain
Turk J Phys Med Rehabil. 2019; 65:301-308WHO Guidelines on the Management of Chronic Primary
Low Back Pain in Adults
World Health Organization, Geneva, 2023
Return to LOW BACK PAIN
Since 7-01-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |