

Spinal Manipulation and Clinician-Supported Self-Management
for Preventing Chronic Low Back Pain Impact:
The PACBACK Randomized Clinical TrialThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: JAMA Intern Med 2026 (Jun 1): e261893 ~ FULL TEXT
OPEN ACCESS Gert Bronfort, PhD, DC • Eric N. Meier, MS • Brent Leininger, PhD, DC, MS • Michael Schneider, PhD, DC • Roni Evans, PhD, DC, MS1 • Carol Greco, PhD • Linda Hanson, DC, MS • Christine McFarland, BS, BA • Roger Chou, MD • John Connett, PhD • Anthony Delitto, PhD, PT • Steven Z. George, PhD, PT • Ronald M. Glick, MD • Francis Keefe, PhD • John Licciardone, DO, MS, MBA • Craig Schulz, DC, MS • Dennis Turk, PhD • Bryan A. Comstock, MS • Ana Gabriela Vasconcelos, MS • Patrick J. Heagerty, PhD, MS
Integrative Health and Wellbeing Research Program,
Earl E. Bakken Center for Spirituality & Healing,
University of Minnesota, Minneapolis.
Importance: Acute and subacute low back pain (LBP) often progresses to a chronic impactful back problem in patients with elevated risk. The most effective way to prevent this progression is unknown.
Objective: To determine the effectiveness of spinal manipulation and clinician-supported biopsychosocial self-management vs medical care for preventing chronic impactful LBP.
Design, setting, and participants: This 2 × 2 factorial randomized clinical trial was conducted in research clinics at the University of Minnesota and the University of Pittsburgh, Pennsylvania, from November 2018 to May 2023, with follow-up concluding in June 2024. Adults with acute or subacute LBP with a moderate to high risk of chronicity were included.
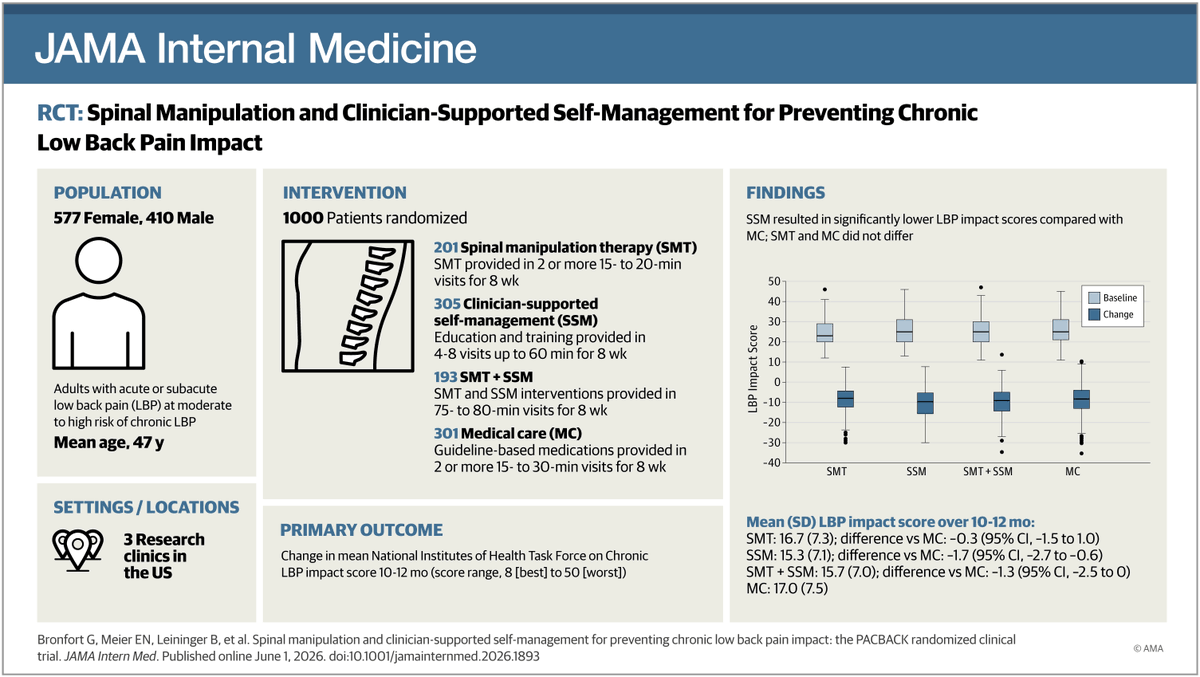
Interventions: Four interventions were applied for 8 weeks: spinal manipulation therapy; supported self-management; combined spinal manipulation therapy and supported self-management; and guideline-based medical care. Spinal manipulation and supported self-management were provided by physical therapists and chiropractors.
Main outcomes and measures: Mean LBP impact score per the US National Institutes of Health Task Force on Chronic LBP scale (8 [best] to 50 [worst]) during 10 to 12 months, responder analyses of group differences in the proportion of participants with at least 50% reductions. A reduction of 30% was considered the minimal clinically important within-patient difference. Secondary outcomes included measures of chronicity and LBP burden (ie, health care and medication use, productivity), important patient-reported outcomes (eg, improvement, satisfaction), biopsychosocial measures (eg, Patient-Reported Outcomes Measurement Information System), and potential mediating psychosocial measures (eg, self-efficacy, kinesiophobia, pain catastrophizing).
Results: Of the 1000 participants (mean [SD] age, 47 [16] years; 577 females [58%]) randomized, 928 (93%) completed the trial. An omnibus test of the primary outcome was statistically significant (P = .006). Group differences in mean LBP impact scores were small but statistically significant: supported self-management vs medical care, -1.7 (95% CI, -2.7 to -0.6); combined self-management and spinal manipulation vs medical care, -1.3 (95% CI, -2.5 to 0). Spinal manipulation therapy and medical care did not differ: -0.3 (95% CI, -1.5 to 1.0). Adding spinal manipulation to supported self-management did not provide additional benefit. The supported self-management group had a significantly higher proportion with at least 50% reduction in LBP impact vs medical care (64% vs 55%). Supported self-management also performed better on most secondary outcomes compared to medical care, including 12% fewer reporting chronic pain that frequently interfered with regular activities. Mediation analyses showed changes in psychosocial factors at 6 months and explained 76% of supported self-management effects at 1 year.
Conclusions and relevance: This randomized clinical trial found that for patients with acute or subacute LBP at increased risk of chronic impactful LBP, clinician-supported biopsychosocial self-management resulted in a lower mean LBP impact score at 10 to 12 months vs medical care; spinal manipulation and medical care did not differ. While the LBP impact difference was small, the consistent results of the responder analyses and most secondary outcomes suggest differences between clinician-supported self-management and medical care are clinically relevant.
Registration: Trial ClinicalTrials.gov Identifier: NCT03581123.
Key Points
Question: Are spinal manipulation therapy and clinician-supported biopsychosocial self-management provided by physical therapists or chiropractors more effective than guideline-based medical care for preventing chronic impactful low back pain (LBP) at 1 year?
Findings: In this randomized clinical trial including 1000 adults, supported self-management resulted in a small reduction in LBP impact score at 1 year with a higher proportion of responders with at least a 50% reduction compared to medical care. Reductions in LBP impact scores did not differ between spinal manipulation and medical care, and supported self-management performed better on most secondary outcomes compared to medical care.
Meaning: Given the reductions in LBP impact score and consistent results of the responder analyses and multiple measures of chronic LBP burden, the effects of clinician-supported biopsychosocial self-management compared with guideline-based medical care appear to be clinically relevant.
From the FULL TEXT Article:
Supplementary Material
References:

Return to LOW BACK PAIN
Since 6-10-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |