

International Society for Nutritional Psychiatry Research
Practice Guidelines for Omega-3 Fatty Acids in the
Treatment of Major Depressive DisorderThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Psychother Psychosom. 2019 (Aug 11); 88 (5): 263–273 ~ FULL TEXT
Ta-Wei Guu, David Mischoulon, Jerome Sarris, Joseph Hibbeln,
Robert K. McNamara, Kei Hamazaki. Marlene P. Freeman, et/ al
Departments of Psychiatry and Mind-Body Interface Laboratory (MBI-Lab),
China Medical University Hospital,
Taichung, Taiwan.Major depressive disorder (MDD) is a complex mental illness with unmet therapeutic needs. The antidepressant effects of ω-3 polyunsaturated fatty acids (n-3 PUFAs) have been widely reported. The subcommittee of the International Society for Nutritional Psychiatry Research organized an expert panel and conducted a literature review and a Delphi process to develop a consensus-based practice guideline for clinical use of n-3 PUFAs in MDD. The guideline focuses on 5 thematic areas:
general concepts,
acute treatment strategy,
depression recurrence monitoring and prevention,
use in special populations, and
potential safety issues.The key practice guidelines contend that:
(1) clinicians and other practitioners are advised to conduct a clinical interview to validate clinical diagnoses, physical conditions, and measurement-based psychopathological assessments in the therapeutic settings when recommending n-3 PUFAs in depression treatment;
(2) with respect to formulation and dosage, both pure eicosapentaenoic acid (EPA) or an EPA/docosahexaenoic acid (DHA) combination of a ratio higher than 2 (EPA/DHA >2) are considered effective, and the recommended dosages should be 1-2 g of net EPA daily, from either pure EPA or an EPA/DHA (>2:1) formula;
(3) the quality of n-3 PUFAs may affect therapeutic activity; and
(4) potential adverse effects, such as gastrointestinal and dermatological conditions, should be monitored, as well as obtaining comprehensive metabolic panels.The expert consensus panel has agreed on using n-3 PUFAs in MDD treatment for pregnant women, children, and the elderly, and prevention in high-risk populations. Personalizing the clinical application of n-3 PUFAs in subgroups of MDD with a low Omega-3 Index or high levels of inflammatory markers might be regarded as areas that deserve future research.
Keywords Omega-3 polyunsaturated fatty acids · Docosahexaenoic acid · Eicosapentaenoic acid · Guideline · Major depressive disorder
From the FULL TEXT Article:
Introduction
Major depressive disorder (MDD) affects one tenth of the population and has been the world’s leading cause of disability. [1, 2] MDD is of heterogeneous etiology with multiple contributory biological mechanisms. Pharmacological treatments with the currently available antidepressants, although proven to be effective in treating moderate to severe symptoms in MDD, have only modest effect sizes but various adverse effects. [3] Therefore, to optimize the patients’ outcomes, clinicians need more efficacious and tolerable treatments supported by valid scientific evidence and reliable practice guidelines.
Omega-3 polyunsaturated fatty acids (n–3 PUFAs), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) have drawn clinical attention of medical specialties. [4–7] Several lines of evidence have suggested the efficacy of n–3 PUFAs as a preventive and treatment strategy in MDD, from epidemiological and case-controlled studies [8, 9] to randomized-controlled trials [10–20] and meta-analyses. [21–30] In addition to clinical studies that examine the efficacy [31, 32] and tolerability [33], the mechanisms of n–3 PUFAs’ antidepressant effects have also been rigorously studied. Several key mechanisms have been proposed, including neuronal cell plasticity and neurogenesis, neurotransmitter dysregulation, and neuro-inflammation. [6, 34, 35]
Despite the clinical and biological evidence, and empirical experience using n–3 PUFAs as an alternative or adjunctive treatment for MDD, there is a current lack of definitive clinical practice guidelines to assist clinicians in the prescriptive application of n–3 PUFAs for MDD. To address this, an advisory subcommittee from the International Society for Nutritional Psychiatry Research (ISNPR) was formed to provide international consensus-based practice guidelines for the evidence-based prescriptive use of n–3 PUFAs for the treatment of MDD.
Methodology
Overview
The format and content of this practice guideline for n–3 PUFAs were developed through 3 stages, including(1) conducting a literature review on major research findings of n–3 PUFAs in MDD treatment;
(2) generating a clinical guideline questionnaire and obtaining consensus through a 2–round, web-based modified mini-Delphi survey; and
(3) optimizing the guidelines from consensus meetings with international experts.
Literature Review and Search Strategy
We had the first preparatory meeting held by a subcommittee under the auspices of 7 key members from the ISNPR in November 2017. ISNPR is an international collaboration of academics advocating recognition of various nutrients as crucial determinants of both physical and mental health, and the positional statements had been published elsewhere. [36, 37]
A systematic review of published literature was conducted with an emphasis on randomized controlled trials (RCTs), systematic reviews and meta-analyses, focusing on the quality of evidence and the implications. Observational studies, physiological or preclinical studies in nonhuman subjects, and ongoing trials would also be reviewed as only supportive evidence.
The subsequent literature review was conducted via PubMed and from the Cochrane Database from inception to May 29, 2019, by the terms “omega-3 polyunsaturated fatty acids,” “n–3 PUFAs,” “major depressive disorder,” and “treatment.” Articles retrieved from these searches and relevant references cited in those articles were also reviewed. High-quality articles published in English, Chinese, and Japanese were included for preliminary review. The outline of the review was drafted by 4 core authors (T.G., D.M., J.S., and K.-P.S.), and then all the authors examined cross-referencing, identified missing important studies, revised the draft of the review, and discussed through subsequent online conferences.
The evidence was categorized using a modified format of the 2011 Levels of Evidence grading system developed by the Oxford Center for Evidence-Based Medicine. Level 1 evidence derives from meta-analyses and systematic reviews of narrow confidence interval (CI) or little conflicting results. Level 2 evidence includes appropriately designed RCTs. Smaller and lower-quality RCTs and nonrandomized controlled cohort/follow-up studies are considered level 3 evidence. Case reports and case series were considered and discussed in the expert consensus meeting to formulate level 4 evidence.
Guideline Questionnaire and Delphi Survey
Four core authors (T.G., D.M., J.S., and K.-P.S.) had an initial online meeting in September 2018 to confirm the evidence obtained from the review and to discuss the major themes and prescriptive issues that could be assessed using a survey (and codified in a resultant consensus guideline). Previous guidelines about n–3 PUFAs and MDD, including using n–3 PUFAs in the treatment of cardiovascular diseases by the American Heart Association, were included as references and discussed to facilitate the formation of the questionnaire. [38–40] After internal correspondences, the draft questionnaire consisted of 20 questions covering 5 major themes: (1) general concepts, (2) acute treatment strategy, (3) depression recurrence monitoring and prevention, (4) special populations, and (5) safety issues.
A Likert scale (0–10) was used for the 19 closed questions (0 = fully against, 10 = fully agree). Questions that scored a predefined consensus level (7.0/10) were included into the guidelines, questions that scored between 5.1 and 6.9 were discussed while questions with scores lower than 5.0 were allocated into a proposed second round Delphi survey with inverse questions. The questionnaire was then tabulated in a web-based survey platform (Survey Monkey) for online voting.
Consensus Meetings
There were 14 experts who participated in the Delphi survey conducted in October 2018. The panellists were selected mainly according to the h-index of the Web of Science database, under the topic of “depression and omega-3” with time span until the end of September 2018 and completed with purposive snowball sampling among active ISNPR members in this topic.
In the online consensus meetings, the panellists focused on confirming the affirmed statements for inclusion and discussing the 3 questions that did not reach the consensus level. After the meeting, the results from the literature review, together with recommendations and the feedback from the survey and meeting, were synthesized into the final version of the official practice guidelines
Results

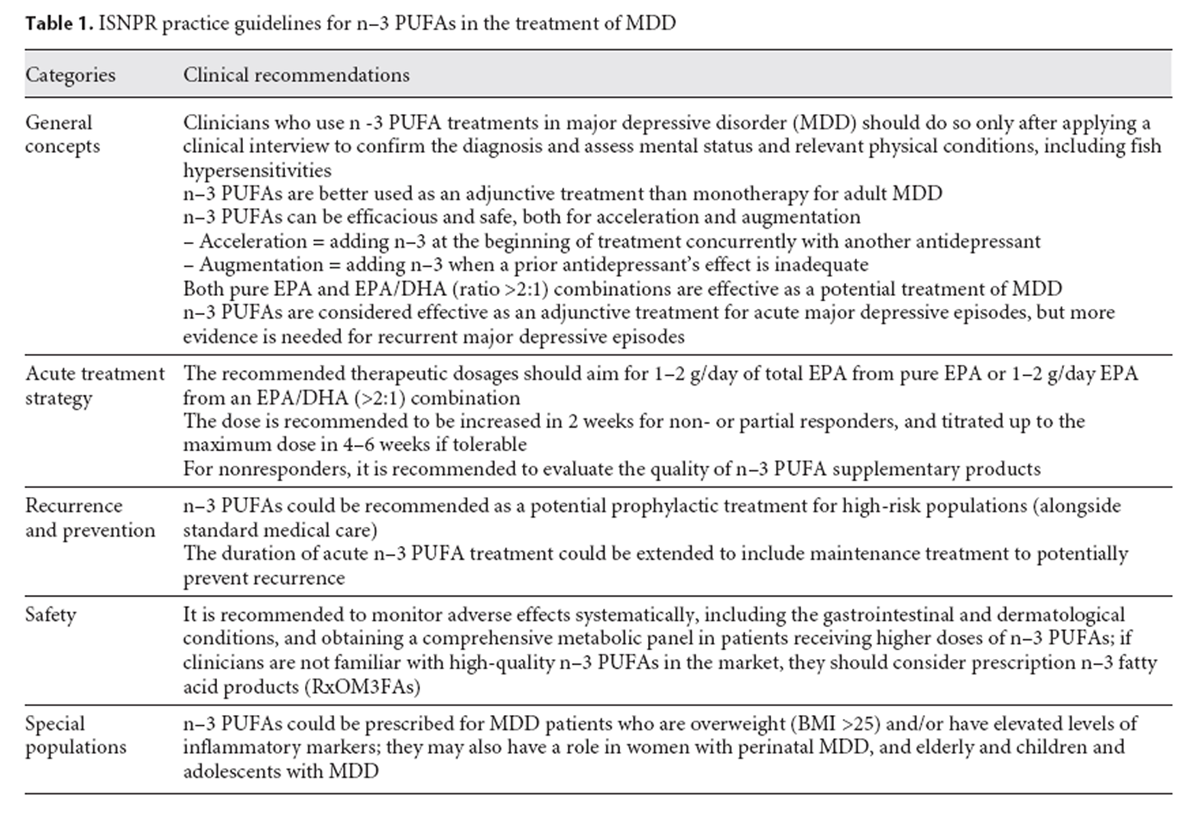
Table 1 The guideline is summarized in Table 1, and the background and evidence supporting the guideline are presented in the key domain sections below
Diagnosis and Measurement-Based Care
The panel consensus emphasizes the importance on diagnosis-based clinical interview and measurement-based depression assessments to validate the accurate diagnosis and psychopathology severity of MDD in the clinical setting. [41] Indeed, when the antidepressant efficacy of n–3 PUFAs is rigorously studied, the pooled effects favor n–3 PUFAs over placebo mainly in RCTs with clinician interview-based diagnosis, rather than in trials including subjects with subclinical depressive symptoms screened by questionnaire. [23, 29]
Disease StagesAcute Stage of MDD The efficacy of small to moderate effect sizes with good safety profiles has been reported in several well-designed RCTs with MDD patients in the acute stage. [10–12, 20] Further, the pooled results from the RCTs for MDD adults (nonpregnant and no-children populations) support the use of n–3 PUFAs for “adjunctive” treatment rather than n–3 PUFA monotherapy (level 1). [24, 25, 30, 42, 43]
Recurrent MDD and Maintenance Treatment Patients with MDD usually require maintenance treatment after the acute depressive episode. However, we identified no studies having enough follow-up duration to address the prevention effects for recurrent MDD. Therefore, current evidence is not adequate to either support or refute the prescription of n–3 PUFAs as longer-term maintenance therapy or for recurrent major depressive episodes. However, considering that most antidepressant medication might be associated with higher dropout rates as compared to placebo [3], the advantage of tolerability profiles of n–3 PUFAs might suggest its potential in maintenance treatment (level 2).
Treatment Strategy (Monotherapy, Augmentation, or Acceleration)
The panel endorses the application for augmentative therapy of n–3 PUFAs because cumulative evidence favors the efficacy of n–3 PUFAs over placebo with the enhanced antidepressant effects clearly shown in meta-analyses (level 1). [24, 25, 30, 42, 43] Furthermore, in one meta-analysis investigating the time points when n–3 PUFAs were added to antidepressants [42], the results showed beneficial effects in either adding n–3 PUFAs at the beginning of the treatment (as an accelerating agent) or adding them at the time when the standing antidepressant was inadequate (i.e., as an augmentative agent; level 1).
Our literature review revealed only a few studies assessing n–3 PUFAs as a monotherapy for MDD. Monotherapy with n–3 PUFAs may have therapeutic benefits in children [44] and pregnant women [14] with depression. However, Mischoulon et al. [45] revealed that neither EPA nor DHA monotherapy were superior to placebo in MDD adults. In another study, patients with postmyocardial infarction were treated with 460 mg EPA and 380 mg DHA for 12 months as monotherapy, and there was also no significant effect in favor of n–3 PUFAs. [46] Therefore, current evidence is inadequate overall of using n–3 PUFAs as monotherapy for MDD, and further RCTs are needed to provide support for or against the use of n–3 PUFAs as a monotherapy for adult MDD (nonpregnant and no-children) patients (level 2).
Dosing, Ratio, and Duration
The functional status of n–3 PUFAs in an individual can be influenced by many factors like dietary patterns, gender, age, and metabolic functions. Therefore, it is impossible to predict the absolute effects of a fixed dose n–3 PUFA supplementation in MDD individuals. In addition, there is no RCT investigating clinical dosing of n–3 PUFAs based on individual dietary or blood level differences.
According to the available RCT results, the panel advises that the starting dose should be at least 1 g of net EPA in a pure EPA form or in an EPA/DHA combination (ratio higher than 2). If well tolerated, the dose could be titrated up to at least 2 g of net EPA daily in 2–4 weeks for partial responsiveness (level 1). [21, 22, 24, 25, 27–30, 42, 43] The panel also reaches a unanimous consensus on the recommendation of EPA/DHA ratio of ≥2:1 to be crucial to n–3 PUFAs’ antidepressant effects (level 1). Indeed, this conclusion is supported by most of the meta-analyses that the higher ratio of EPA, the better the therapeutic outcome, while DHA as main component had no detectable pooled effects on the MDD symptoms. [21, 23–25, 29]
There was insufficient data to conclude the optimal duration of n–3 PUFA supplementation. The duration of most RCTs varies from 4 to 16 weeks. Due to the length of time needed for n–3 PUFAs to be incorporated into brains, and for the downstream neuroplastic effects and anti-inflammatory actions, the panel endorses a prescriptive guideline of at least 8 weeks. Clinicians are advised to check the quality of the n–3 PUFA prescription of nonresponders, and evaluate the response and the tolerability profiles for an optimal duration (level 2). [24, 25, 27]
Safety and Adverse Effects
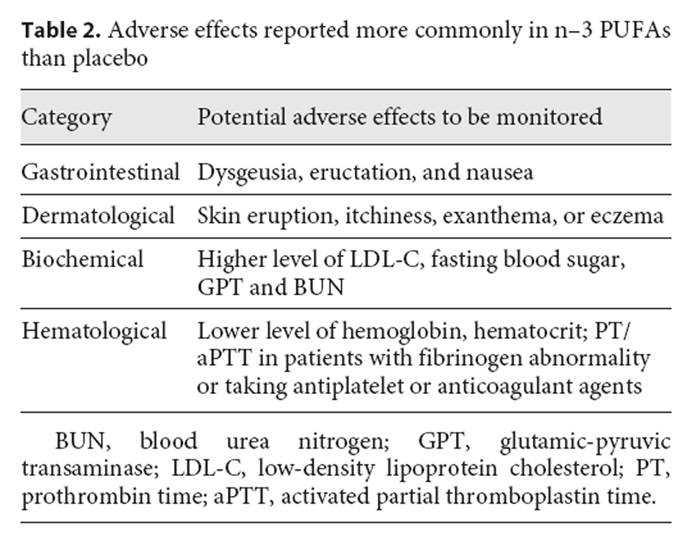
One recent meta-analysis comprehensively examined the adverse effects reported when using prescribed n–3 PUFA products in various clinical populations. n–3 PUFAs were found to be associated with higher rates of mild gastrointestinal symptoms (such as fishy taste, belching, and nausea), less in skin abnormalities (such as eruption and itchiness), and no serious adverse effects. [33] Another meta-analysis using adverse effects as one of the primary outcomes reported that, despite poor data quality, the numbers of individuals experiencing adverse events were similar in intervention and placebo groups and were negligible (level 1). [30] The risk of theoretical adverse effects of excessive bleeding did not exist, and current evidence suggests that under concurrent usage of antiplatelet or anticoagulant agents, doses up to 4 g of n–3 PUFAs daily are not associated with an increased risk of major bleeding. [47] Although both a recent meta-analysis focusing on pregnancy [48] and the other focusing on perioperative periods [49] support similar safety profiles compared with placebo in general and in bleeding-related adverse events, and most in vivo studies do not suggest that n–3 PUFAs would impact either platelet aggregation or adhesion in healthy subjects [50], we recommend shared decision-making discussions between patients and clinicians on bleeding-related hematological examinations, especially if the patient has underlying fibrinogen dysfunction or is taking antiplatelet or anticoagulant agents.
Table 2 Laboratory measurements have revealed that n–3 PUFAs (compared to placebo) may cause higher fasting blood sugar, glutamate pyruvate transaminase, low-density lipoprotein cholesterol and blood urea nitrogen, and lower hemoglobin and hematocrit levels. Although the mean differences were relatively small, and may have only statistical rather than clinical importance, the panel recommends that, when using higher doses, these biomarkers may need to be monitored (level 1). It is interesting to note that in this meta-analysis, combining EPA and DHA was associated with higher rates of the aforementioned adverse effects, compared with EPA alone. [33] The monitoring profiles are summarized in Table 2
Quality and Purity of Marine-Derived Preparations
The significant difference in efficacy observed in various conditions could be partly related to the concentration (purity) and quality (product preparation) of n–3 PUFA products, which lead to the discrepancy of bioavailability and pharmacodynamics. [51] Many countries advise adequate fish consumption under careful selection of the types and regions of farming and the species of fish to prevent overintake of methylmercury and other pollutants. However, these advices have been controversial and are not included in recommendations about n–3 PUFA supplementations. If clinicians are not familiar with high-quality n–3 PUFA products in the market, it is advised to consider the prescription n–3 PUFA products (RxOM3FAs; level 4). [52, 53] Due to the possibility of oxidation, with consequent loss of health benefits and formation of aldehydes, recommendations are to use fish oil or non-marine-derived n–3 PUFA products with antioxidants added (including vitamin E), store the products in airtight and dark containers to protect from light and to refrigerate n–3 PUFA products after opening. [54]
Special Consideration and PopulationsPerinatal Depression and Childhood Depression Pharmacotherapy for MDD in pregnant women and children is still a clinical dilemma. There are no RCTs for antidepressant drugs during pregnancy. To date, the US Food and Drug Administration approves no psychotropic drugs during pregnancy and even issues a black box warning of suicidal risk on antidepressant drugs for children. [32] So far, 3 double-blind, placebo-controlled RCTs of n–3 PUFAs have been published in perinatal women with MDD. [14, 55, 56] The first study using 2.2 g/day of EPA and 1.2 g/day of DHA successfully detected the therapeutic signal that n–3 PUFAs were significantly better than placebo to improve depressive symptoms and achieve treatment response. [14] The other 2 RCTs that failed to show the antidepressant efficacy of n–3 PUFA treatment both administered supplements rich in DHA rather than EPA. [55, 56]
A recent multicenter, double-blind, placebo-controlled RCT investigated the efficacy of n–3 PUFAs for depressive symptoms among pregnant women in Japan and Taiwan (the SYNCHRO trial). [57] One hundred and 8 pregnant women from 3 study sites took n–3 PUFAs (1,206 mg EPA and 609 mg DHA) or placebo for 12 weeks. The total HAMD score was not significantly different between the n–3 and placebo groups in the primary analysis. Prespecified subgroup analysis for study site, however, showed a significant antidepressant effect of lower Hamilton Depression Scale scores in the n–3 PUFA than in the placebo group at one site where the severest cases were included, with an effect size of 0.72. Thirty participants reported minor adverse events, but there were no significant differences in adverse events between the n–3 and placebo groups (27.3 vs. 28.3%, respectively).
The panel concludes that clinicians should interpret these positive results carefully and apply n–3 PUFAs cautiously during the perinatal-specific period in general because the data from rather small sample sizes are currently insufficient and inconsistent regarding the efficacy of n–3 PUFAs in perinatal MDD (level 2). n–3 PUFAs are important nutrients for pregnant women and young brains, and suboptimal levels of n–3 PUFAs are emerging as a potential risk factor for brain disorders in younger populations. [58] A small RCT recruiting 20 children aged between 8 and 12 years showed that daily supplementation of 380–400 mg of EPA and 180–200 mg of DHA was significantly better than placebo to improve depression symptomatology in a 16–week intervention. [44] Again, the sample size is too small to draw a solid conclusion. Therefore, we need evidence from more RCTs.
MDD with Low-Grade Inflammation or Comorbid Obesity Recent work has examined the interrelationship between certain inflammatory biomarkers and treatment response to n–3 PUFAs in MDD0. [18, 32] A clinical trial comparing EPA, DHA, and placebo found that individuals who had 4–5 elevated baseline inflammatory biomarkers (including high-sensitivity C-reactive protein, interleukin-6, interleukin-1 receptor antagonist, leptin) and decreased adiponectin were more likely to respond to EPA but not to DHA [18], echoing the notion that n–3 PUFAs may be more effective in depression associated with inflammation. [32] Furthermore, subjects with more than one elevated inflammatory marker were more likely to be overweight. The preliminary results support the use of n–3 PUFAs in depressed individuals who are overweight and/or have elevated inflammatory biomarkers. The above findings are currently being pursued in an ongoing clinical trial using EPA monotherapy in a sample of overweight patients with MDD and elevated CRP at baseline (NCT02553915).
Chronic inflammation is involved in the etiology of MDD. Of particular relevance to this context, Su et al. [59] have previously conducted a double-blind RCT to test the effects of n–3 PUFA supplementation in the prevention of interferon-α-induced depression, and found that incident rates of interferon-α-induced depression were significantly reduced in EPA-treated patients, but not DHA- or placebo-treated patients. This study further confirms the notion that n–3 PUFAs may be effective antidepressants in the context of depression associated with inflammation. [59] Of note, one recently published RCT that recruited prenatal subjects demonstrated that prenatal depression is significantly associated with lower DHA, EPA, total n–3 PUFA levels and higher tumor necrosis factor α. [60] This finding not only provides the rationale to investigate the inflammation mechanism underlying n–3 PUFA treatment for prenatal depression, but also encourages further consideration of n–3 PUFAs for pregnant women with mood disorders.
Gender and Age Differences and Other Considerations Epidemiological studies from various jurisdictions have consistently revealed that females are more prone to depression than male counterparts. [61] As reported by Yang et al. [43], a beneficial effect and good tolerability of the combination of EPA and DHA was found on depressed mood in women. No previous study has reported gender-specific differences (level 1).
Although MDD patients in different age groups may vary in their psychopathological presentation, one meta-analysis also reported that age of the studied cohorts did not significantly influence the efficacy of n–3 PUFAs (level 1). [24] There are also studies showing the potential benefit of n–3 PUFAs for anxiety symptoms [62], suggesting that future research to elucidate the true antidepressant and anxiolytic mechanisms of different n–3 PUFAs is warranted.
Chronic inflammation might also be involved in the etiology of many other medical conditions including heart disease, stroke, cancer, and metabolic syndrome. Since n–3 PUFAs, EPA in particular, may lower systemic inflammation, more recent studies are focusing on patients with a range of comorbidities. [46, 63–65] One recent meta-analysis, however, reported that studies involving comorbid populations showed no overall treatment effect. [42] Therefore, the panel advises avoiding overgeneralization of MDD patients with different physical comorbidities as “one category.” Instead, the clinical researchers are recommended to carefully monitor the response and adverse effects when applying n–3 PUFAs in MDD patients with specific physical illness.
Discussion
To our knowledge, this is the first international research society consensus-based practice guideline for clinical use of n–3 PUFAs in MDD. The guideline includes 12 clinical recommendations and is well summarized in Table 1 based on the items which reached consensus levels. In general, the recommendations focus on 5 thematic areas: general concepts, acute treatment strategy, recurrence and prevention, special populations, and safety. The guideline did not include, yet discussed in the previous section Results, the 3 items of our expert survey that did not reach consensus levels.
The panel emphasizes the importance of accurate clinical diagnosis and measurement-based psychopathological assessments practised in the therapeutic settings when recommending n–3 PUFAs in depression treatment. As cumulative evidence favors the efficacy of n–3 PUFAs as an adjunctive use on top of antidepressant medication, the attitude of prescribing n–3 PUFAs should not be based on antimedication.
As meta-analyses reveal only small but statistically significant effects, there are always critical debates on the benefits of n–3 PUFAs for MDD. The estimated effect sizes (standardized mean differences between n–3 PUFAs and placebo) range from 0.23 to 0.56 (with wide CI) in treating DSM-defined MDD patients in 3 recent meta-analyses. [24, 29, 30] However, small effect sizes are also reported for all kinds of antidepressant drugs compared to placebo, with the standardized mean differences between 0.30 and 0.47 (with narrower CI). [3, 66, 67] Till now, the scientific evidence and clinical opinions do not support any particular treatment based on efficacy differences. Although n–3 PUFAs would not be regarded as “a new antidepressant,” when the clinicians consider taking the differences in adverse events and patients’ preference into consideration, n–3 PUFAs would be potentially an applicable alternative choice of treatment. [68]
Three practical strategies could be considered for the unmet needs in depression treatment as every single recommended therapy only has small effects: “an open-minded attitude to integrative intervention,” “the application of personalized medicine,” and a “shared decision-making process based on balanced information to enhance treatment adherence.”
First, the integrative intervention is often criticized for overpromotion on efficacy and safety and for nonregulation of product quality and malpractice by trustworthy authorities. This panel consists of the most cited experts in the fields and aims to provide an evidence-based empirical practice guideline to help clinicians to have a more open-minded attitude to recommend n–3 PUFAs to depressed patients. For other “nonpatentable” interventions with sound clinical and preclinical evidence (e.g., exercise [69], mindfulness [70, 71], or acupuncture [72]), we need more well-established expert consensus and practice guidelines supported by trustworthy authorities for the same reasons.
The second important strategy to increase the treatment effects is subtyping patients into more homogeneous subgroups, as MDD populations can be extremely heterogenous based on current diagnostic systems. [73] Rapaport et al. [18] published an interesting RCT and demonstrated that EPA monotherapy was more effective than the placebo or DHA in patients with elevated markers of inflammation. Specifically, the overall treatment group differences were negligible (ES = –0.09 to –0.13) among MDD patients without stratifying. However, subjects classified with “high” inflammation improved more on EPA than placebo (ES = –0.39 to –1.11 from any one marker to 4–5 markers) or DHA (ES = –0.60 to –1.10 from any one marker to 4–5 markers). Furthermore, EPA-placebo separation increased with increasing numbers of markers of high inflammation. In other words, employing biomarkers of inflammation indeed facilitated identification of a more homogeneous cohort of subjects with MDD who would respond better to n–3 PUFA antidepressant treatment. [32] Therefore, this current practice guideline specifies subgroups of MDD for n–3 PUFAs, including perinatal depression, childhood depression, and MDD with low-grade inflammation or comorbid obesity.
Finally, it has been noted that a shared decision-making process may enhance patients’ adherence and satisfaction to treatment, especially in chronic illnesses. [74] As MDD is often a long-lasting, relapse-remitting illness, assessing the patient’s attitudes toward treatment, integrating information regarding responsiveness, vulnerability, comorbidity and important psychosocial and contextual factors, rather than providing a reductionistic view of treatment options, may allow the patients to actively participate in the therapeutic settings and subsequently improve the adherence and satisfaction toward the treatment. [75–78] In this guideline, we tried to address all the relevant clinical aspects when considering n–3 PUFAs for MDD patients, and it is important to emphasize that “the process” of discussing the information can be as important as the information itself.
Despite several meta-analyses and independent clinical trials which have shown that n–3 PUFAs were more effective than placebo, the meta-analyses from 2 groups failed to detect antidepressant effects of n–3 PUFAs. [22, 79] In fact, the main reasons of inconsistent results from meta-analyses in n–3 PUFA trials are due to common methodological flaws such as pooling heterogeneous clinical trials, applying nonstandardized diagnostic procedures and unreliable outcome measurements, and implementing improper intervention methods [29, 80], which are rarely found in high-quality clinical trials conducted by pharmaceutical companies. In the first meta-analysis with negative findings [22], the authors included a clinical trial [81] enrolling individuals according to self-rating scales, but not structured interview, and in nonclinical settings that weighted up to 31.7% of the whole pooled estimation. In another meta-analysis showing negative outcomes [78], one single 43.3%–weighted clinical trial was included [82], which not only applied no appropriate tools for clinical diagnoses or assessments, but also defined its n–3 PUFA intervention as “advising” subjects to “eat more fish.” Obviously, the methodological flaws undermined the possibility to detect the small signals in clinical trials for n–3 PUFAs’ antidepressant effects. And if the problematic RCTs were taken away, all the meta-analyses from independent groups with well-conducted designs showed positive results. [23–25, 27, 29, 83]
Some limitations need to be taken into account when applying this guideline in clinical settings. First, 3 items did not reach consensus levels: (1) “n–3 PUFAs are one of the potential monotherapies for adult MDD”; (2) “pure EPA is more recommended than EPA/DHA (>2) combination”; and (3) “n–3 PUFAs are considered similarly effective for recurrent MDD.” Therefore, we concluded that the evidence is inadequate overall of using n–3 PUFA prevention of MDD recurrence or as a monotherapy. In addition, the consensus describes that “the pure EPA form or the EPA/DHA combination could both be effective.” Second, we should be aware of the aggregated mild treatment effects in meta-analyses and the inconsistence in some of the RCTs. In addition to general methodological flaws mentioned previously, the other main reasons for inconsistent findings from several RCTs include insufficient statistic powers due to small sample sizes, poor quality of product preparations, and inadequate dosage or ratio of EPA in the n–3 PUFA supplementations. It is very important to note that the clinical trials using DHA-predominant formulations are consistently ineffective. [55, 56, 81, 84–87] Therefore, this guideline includes: “Both pure EPA and EPA/DHA (ratio >2:1) combinations are effective as a potential treatment of MDD (item 4).” Third, unlike medication, most n–3 PUFA supplementary products are not strictly regulated by government regulation. Therefore, this guideline recommends that “If clinicians are not familiar with high-quality n–3 PUFAs in the market, they should consider prescription omega-3 fatty acid products (item 11).” Finally, although the panel has a certain agreement about subtyping specific MDD populations, there are neither “Omega-3 Index” guidance nor pharmacogenomic research data to support personalized medicine for n–3 PUFA treatment.
To conclude, the ISNPR provides the first practice guideline of n–3 PUFAs in depression treatment and emphasizes the importance of accurate clinical diagnosis and measurement-based psychopathological assessments practised in the therapeutic settings. Pure EPA or a combination of EPA and DHA (with net EPA starting from at least 1 up to 2 g/day) for at least 8 weeks are recommended as adjunctive treatment. Monitoring of adverse effects is recommended. In MDD patients with different medical comorbidities, during the perinatal period, or for primary prevention of MDD in specialized populations, there were promising results with good tolerability profiles, but well-designed RCTs with larger sample sizes and longer duration are needed to confirm the efficacy of n–3 PUFAs.
Acknowledgments
The authors of this work received the following research grants related to this work: MOST 108-2320-B-039-048; 108-2314-B-039-016; MOST 107-2314-B-039-005; 106-2314-B-039-027-MY3; 106-2314-B-038-049; 106-2314-B-039-031; 106-2314-B-039-035; and 105-2918-I-039-001 from the Ministry of Science and Technology, Taiwan; NHRI-EX106-10528NI from the National Health Research Institutes, Taiwan; and CRS-106-063, DMR-107-202, DMR-107-204, DMR-107-091, DRM-107-097, DRM-108-091, CRS-108-048, and the Chinese Medicine Research Center from the China Medical University, Taiwan.
Disclosure Statement and Funding Sources
Prof. Carmine Pariante has received research funding from Johnson and Johnson as part of a program of research on depression and inflammation, and research funding from the Medical Research Council (UK) and the Wellcome Trust for research on depression and inflammation as part of 2 large consortia that also include Johnson and Johnson, GSK, and Lundbeck.
Prof. Jerome Sarris has received either presentation honoraria, travel support, clinical trial grants, book royalties, or independent consultancy payments from: Integria Healthcare and MediHerb, Pfizer, Scius Health, Key Pharmaceuticals, Taki Mai, FIT-BioCeuticals, Blackmores, Soho-Flordis, Healthworld, HealthEd, HealthMasters, Kantar Consulting, Research Reviews, Elsevier, Chaminade University, International Society for Affective Disorders, Complementary Medicines Australia, SPRIM, Terry White Chemists, ANS, Society for Medicinal Plant and Natural Product Research, Sanofi-Aventis, Omega-3 Centre, the National Health and Medical Research Council, CR Roper Fellowship.
Prof. Yutaka J. Matsuoka has received presentation honoraria from Morinaga Milk, Eli Lilly, and NTT Data and is conducting collaborative research with Morinaga Milk.
Dr. Marlene P. Freeman (past 12 months): investigator-initiated trials/research: JayMac, Sage; advisory boards: Otsuka, Alkermes, Sunovion; independent data safety and monitoring committee: Janssen (Johnson and Johnson). Dr. Marlene P. Freeman is an employee of Massachusetts General Hospital and works with the MGH National Pregnancy Registry (current registry sponsors: Teva [2018 to present], Alkermes Inc. [2016 to present]; Otsuka America Pharmaceutical Inc. [2008 to present]; Forest/Actavis [2016 to present], Sunovion Pharmaceuticals Inc. [2011 to present]). As an employee of MGH, Dr. Marlene P. Freeman works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH.
Prof. David Mischoulon has received research support from Nordic Naturals. He has provided unpaid consulting for Pharmavite LLC and Gnosis USA Inc. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy, Blackmores, and PeerPoint Medical Education Institute LLC. He has received royalties from Lippincott Williams and Wilkins for the published book Natural Medications for Psychiatric Disorders: Considering the Alternatives. He also works with the MGH Clinical Trials Network and Institute (CTNI), which has received research funding from multiple pharmaceutical companies and NIMH.
Prof. Felice Jacka has received grant/research support from the Brain and Behaviour Research Institute, the National Health and Medical Research Council (NHMRC), Australian Rotary Health, the Geelong Medical Research Foundation, the Ian Potter Foundation, Eli Lilly, Meat and Livestock Australia, the A2 Milk Company, BeFit Foods, Woolworths Ltd., Fernwood Foundation, the Wilson Foundation, and the University of Melbourne and has received speaker honoraria from Sanofi-Synthelabo, Janssen Cilag, Servier, Pfizer, HealthEd, Network Nutrition, Angelini Farmaceutica, Eli Lilly, and Metagenics. She is supported by an NHMRC Career Development Fellowship (2; #1108125). Felice Jacka is currently writing 2 books for commercial publication and has a personal belief that good diet quality is important for mental and brain health.
Dr. Robert K. McNamara has received research support from Martek Biosciences Inc., Royal DSM Nutritional Products, LLC, Inflammation Research Foundation, Ortho-McNeil Janssen, AstraZeneca, Eli Lilly, NARSAD, and the National Institutes of Health, and previously served on the scientific advisory board of the Inflammation Research Foundation.
References:
Belmaker RH, Agam G. Major depressive disorder. N Engl J Med. 2008 Jan;358(1):55–68.
Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997 May;349(9063):1436–42.
Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018 Apr;391(10128):1357–66.
Hibbeln JR, Nieminen LR, Blasbalg TL, Riggs JA, Lands WE. Healthy intakes of n-3 and n-6 fatty acids: estimations considering worldwide diversity. Am J Clin Nutr. 2006 Jun;83(6 Suppl):1483S–93S.
Connor WE. Importance of n-3 fatty acids in health and disease. Am J Clin Nutr. 2000 Jan;71(1 Suppl):171S–5S.
Su KP. Biological mechanism of antidepressant effect of omega-3 fatty acids: how does fish oil act as a ‘mind-body interface’? Neurosignals. 2009;17(2):144–52.
Su KP, Shen WW, Huang SY. Effects of polyunsaturated fatty acids on psychiatric disorders. Am J Clin Nutr. 2000 Nov;72(5):1241.
Lin PY, Huang SY, Su KP. A meta-analytic review of polyunsaturated fatty acid compositions in patients with depression. Biol Psychiatry. 2010 Jul;68(2):140–7.
Hibbeln JR. Fish consumption and major depression. Lancet. 1998 Apr;351(9110):1213.
Nemets B, Stahl Z, Belmaker RH. Addition of omega-3 fatty acid to maintenance medication treatment for recurrent unipolar depressive disorder. Am J Psychiatry. 2002 Mar;159(3):477–9.
Peet M, Horrobin DF. A dose-ranging study of the effects of ethyl-eicosapentaenoate in patients with ongoing depression despite apparently adequate treatment with standard drugs. Arch Gen Psychiatry. 2002 Oct;59(10):913–9.
Su KP, Huang SY, Chiu CC, Shen WW. Omega-3 fatty acids in major depressive disorder. A preliminary double-blind, placebo-controlled trial. Eur Neuropsychopharmacol. 2003 Aug;13(4):267–71.
Jazayeri S, Tehrani-Doost M, Keshavarz SA, Hosseini M, Djazayery A, Amini H, et al. Comparison of therapeutic effects of omega-3 fatty acid eicosapentaenoic acid and fluoxetine, separately and in combination, in major depressive disorder. Aust N Z J Psychiatry. 2008 Mar;42(3):192–8.
Su KP, Huang SY, Chiu TH, Huang KC, Huang CL, Chang HC, et al. Omega-3 fatty acids for major depressive disorder during pregnancy: results from a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2008 Apr;69(4):644–51.
Frangou S, Lewis M, McCrone P. Efficacy of ethyl-eicosapentaenoic acid in bipolar depression: randomised double-blind placebo-controlled study. Br J Psychiatry. 2006 Jan;188(1):46–50.
da Silva TM, Munhoz RP, Alvarez C, Naliwaiko K, Kiss A, Andreatini R, et al. Depression in Parkinson’s disease: a double-blind, randomized, placebo-controlled pilot study of omega-3 fatty-acid supplementation. J Affect Disord. 2008 Dec;111(2-3):351–9.
Mischoulon D, Papakostas GI, Dording CM, Farabaugh AH, Sonawalla SB, Agoston AM, et al. A double-blind, randomized controlled trial of ethyl-eicosapentaenoate for major depressive disorder. J Clin Psychiatry. 2009 Dec;70(12):1636–44.
Rapaport MH, Nierenberg AA, Schettler PJ, Kinkead B, Cardoos A, Walker R, et al. Inflammation as a predictive biomarker for response to omega-3 fatty acids in major depressive disorder: a proof-of-concept study. Mol Psychiatry. 2016 Jan;21(1):71–9.
Lespérance F, Frasure-Smith N, St-André E, Turecki G, Lespérance P, Wisniewski SR. The efficacy of omega-3 supplementation for major depression: a randomized controlled trial. J Clin Psychiatry. 2011 Aug;72(8):1054–62.
Gertsik L, Poland RE, Bresee C, Rapaport MH. Omega-3 fatty acid augmentation of citalopram treatment for patients with major depressive disorder. J Clin Psychopharmacol. 2012 Feb;32(1):61–4.
Martins JG. EPA but not DHA appears to be responsible for the efficacy of omega-3 long chain polyunsaturated fatty acid supplementation in depression: evidence from a meta-analysis of randomized controlled trials. J Am Coll Nutr. 2009 Oct;28(5):525–42.
Bloch MH, Hannestad J. Omega-3 fatty acids for the treatment of depression: systematic review and meta-analysis. Mol Psychiatry. 2012 Dec;17(12):1272–82.
Martins JG, Bentsen H, Puri BK. Eicosapentaenoic acid appears to be the key omega-3 fatty acid component associated with efficacy in major depressive disorder: a critique of Bloch and Hannestad and updated meta-analysis. Mol Psychiatry. 2012 Dec;17(12):1144–9.
Grosso G, Pajak A, Marventano S, Castellano S, Galvano F, Bucolo C, et al. Role of omega-3 fatty acids in the treatment of depressive disorders: a comprehensive meta-analysis of randomized clinical trials. PLoS One. 2014 May;9(5):e96905.
Mocking RJ, Harmsen I, Assies J, Koeter MW, Ruhé HG, Schene AH. Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Transl Psychiatry. 2016 Mar;6(3):e756.
Bai ZG, Bo A, Wu SJ, Gai QY, Chi I. Omega-3 polyunsaturated fatty acids and reduction of depressive symptoms in older adults: A systematic review and meta-analysis. J Affect Disord. 2018 Dec;241:241–8.
Hallahan B, Ryan T, Hibbeln JR, Murray IT, Glynn S, Ramsden CE, et al. Efficacy of omega-3 highly unsaturated fatty acids in the treatment of depression. Br J Psychiatry. 2016 Sep;209(3):192–201.
Lin PY, Su KP. A meta-analytic review of double-blind, placebo-controlled trials of antidepressant efficacy of omega-3 fatty acids. J Clin Psychiatry. 2007 Jul;68(7):1056–61.
Lin PY, Mischoulon D, Freeman MP, Matsuoka Y, Hibbeln J, Belmaker RH, et al. Are omega-3 fatty acids antidepressants or just mood-improving agents? The effect depends upon diagnosis, supplement preparation, and severity of depression. Mol Psychiatry. 2012 Dec;17(12):1161–3.
Appleton KM, Sallis HM, Perry R, Ness AR, Churchill R: Omega-3 fatty acids for depression in adults. Cochrane Database Syst Rev. 2015;Cd004692.
Su KP, Wang SM, Pae CU. Omega-3 polyunsaturated fatty acids for major depressive disorder. Expert Opin Investig Drugs. 2013 Dec;22(12):1519–34.
Su KP. Personalized medicine with Omega-3 fatty acids for depression in children and pregnant women and depression associated with inflammation. J Clin Psychiatry. 2015 Nov;76(11):e1476–7.
Chang CH, Tseng PT, Chen NY, Lin PC, Lin PY, Chang JP, et al. Safety and tolerability of prescription omega-3 fatty acids: A systematic review and meta-analysis of randomized controlled trials. Prostaglandins Leukot Essent Fatty Acids. 2018 Feb;129:1–12.
Su KP. Nutrition, psychoneuroimmunology and depression: the therapeutic implications of omega-3 fatty acids in interferon-α-induced depression. Biomedicine (Taipei). 2015 Dec;5(4):21.
Song C, Shieh CH, Wu YS, Kalueff A, Gaikwad S, Su KP. The role of omega-3 polyunsaturated fatty acids eicosapentaenoic and docosahexaenoic acids in the treatment of major depression and Alzheimer’s disease: acting separately or synergistically? Prog Lipid Res. 2016 Apr;62:41–54.
Sarris J, Logan AC, Akbaraly TN, Amminger GP, Balanzá-Martínez V, Freeman MP, et al.; International Society for Nutritional Psychiatry Research. Nutritional medicine as mainstream in psychiatry. Lancet Psychiatry. 2015 Mar;2(3):271–4.
Sarris J, Logan AC, Akbaraly TN, Paul Amminger G, Balanzá-Martínez V, Freeman MP, et al. International Society for Nutritional Psychiatry Research consensus position statement: nutritional medicine in modern psychiatry. World Psychiatry. 2015 Oct;14(3):370–1.
McIntyre RS, Suppes T, Tandon R, Ostacher M. Florida Best Practice Psychotherapeutic Medication Guidelines for Adults With Major Depressive Disorder. J Clin Psychiatry. 2017 Jun;78(6):703–13.
Ravindran AV, Balneaves LG, Faulkner G, Ortiz A, McIntosh D, Morehouse RL, et al.; CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 5. Complementary and Alternative Medicine Treatments. Can J Psychiatry. 2016 Sep;61(9):576–87.
Siscovick DS, Barringer TA, Fretts AM, Wu JH, Lichtenstein AH, Costello RB, et al.; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and the Prevention of Clinical Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation. 2017 Apr;135(15):e867–84.
Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al.; STAR*D Study Team. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006 Jan;163(1):28–40.
Schefft C, Kilarski LL, Bschor T, Köhler S. Efficacy of adding nutritional supplements in unipolar depression: A systematic review and meta-analysis. Eur Neuropsychopharmacol. 2017 Nov;27(11):1090–109.
Yang JR, Han D, Qiao ZX, Tian X, Qi D, Qiu XH. Combined application of eicosapentaenoic acid and docosahexaenoic acid on depression in women: a meta-analysis of double-blind randomized controlled trials. Neuropsychiatr Dis Treat. 2015 Aug;11:2055–61.
Nemets H, Nemets B, Apter A, Bracha Z, Belmaker RH. Omega-3 treatment of childhood depression: a controlled, double-blind pilot study. Am J Psychiatry. 2006 Jun;163(6):1098–100.
Mischoulon D, Nierenberg AA, Schettler PJ, Kinkead BL, Fehling K, Martinson MA, et al. A double-blind, randomized controlled clinical trial comparing eicosapentaenoic acid versus docosahexaenoic acid for depression. J Clin Psychiatry. 2015 Jan;76(1):54–61.
Zimmer R, Riemer T, Rauch B, Schneider S, Schiele R, Gohlke H, et al.; OMEGA-Study Group. Effects of 1-year treatment with highly purified omega-3 fatty acids on depression after myocardial infarction: results from the OMEGA trial. J Clin Psychiatry. 2013 Nov;74(11):e1037–45.
Mori TA. Omega-3 fatty acids and cardiovascular disease: epidemiology and effects on cardiometabolic risk factors. Food Funct. 2014 Sep;5(9):2004–19.
Middleton P, Gomersall JC, Gould JF, et al.: Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst Rev 2018;11:Cd003402
Akintoye E, Sethi P, Harris WS, Thompson PA, Marchioli R, Tavazzi L, et al. Fish Oil and Perioperative Bleeding. Circ Cardiovasc Qual Outcomes. 2018 Nov;11(11):e004584.
Bagge A, Schött U, Kander T. High-dose omega-3 fatty acids have no effect on platelet aggregation or coagulation measured with static and flow-based aggregation instruments and Sonoclot; an observational study in healthy volunteers. Scand J Clin Lab Invest. 2018 Nov - Dec;78(7-8):539–45.
Cicero AF, Morbini M, Borghi C. Do we need ‘new’ omega-3 polyunsaturated fatty acids formulations? Expert Opin Pharmacother. 2015 Feb;16(3):285–8.
Ginsberg GL, Toal BF. Quantitative approach for incorporating methylmercury risks and omega-3 fatty acid benefits in developing species-specific fish consumption advice. Environ Health Perspect. 2009 Feb;117(2):267–75.
Wu PW. A review on the analysis of ingredients with health care effects in health food in Taiwan. Yao Wu Shi Pin Fen Xi. 2015 Sep;23(3):343–50.
Heller M, Gemming L, Tung C, Grant R. Oxidation of fish oil supplements in Australia. Int J Food Sci Nutr. 2019 Aug;70(5):540–50.
Rees AM, Austin MP, Parker GB. Omega-3 fatty acids as a treatment for perinatal depression: randomized double-blind placebo-controlled trial. Aust N Z J Psychiatry. 2008 Mar;42(3):199–205.
Freeman MP, Davis M, Sinha P, Wisner KL, Hibbeln JR, Gelenberg AJ. Omega-3 fatty acids and supportive psychotherapy for perinatal depression: a randomized placebo-controlled study. J Affect Disord. 2008 Sep;110(1-2):142–8.
Nishi D, Su KP, Usuda K, Pei-Chen Chang J, Chiang YJ, Chen HT, et al. The Efficacy of Omega-3 Fatty Acids for Depressive Symptoms among Pregnant Women in Japan and Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial (SYNCHRO; NCT01948596). Psychother Psychosom. 2019;88(2):122–4.
Chang JP, Su KP, Mondelli V, Pariante CM. Omega-3 Polyunsaturated Fatty Acids in Youths with Attention Deficit Hyperactivity Disorder: a Systematic Review and Meta-Analysis of Clinical Trials and Biological Studies. Neuropsychopharmacology. 2018 Feb;43(3):534–45.
Su KP, Lai HC, Yang HT, Su WP, Peng CY, Chang JP, et al. Omega-3 fatty acids in the prevention of interferon-alpha-induced depression: results from a randomized, controlled trial. Biol Psychiatry. 2014 Oct;76(7):559–66.
Chang JP, Lin CY, Lin PY, Shih YH, Chiu TH, Ho M, et al. Polyunsaturated fatty acids and inflammatory markers in major depressive episodes during pregnancy. Prog Neuropsychopharmacol Biol Psychiatry. 2018 Jan;80(Pt C):273–8.
Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al.; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003 Jun;289(23):3095–105.
Su KP, Tseng PT, Lin PY, Okubo R, Chen TY, Chen YW, et al. Association of Use of Omega-3 Polyunsaturated Fatty Acids With Changes in Severity of Anxiety Symptoms: A Systematic Review and Meta-analysis. JAMA Netw Open. 2018 Sep;1(5):e182327.
Dashti-Khavidaki S, Gharekhani A, Khatami MR, Miri ES, Khalili H, Razeghi E, et al. Effects of omega-3 fatty acids on depression and quality of life in maintenance hemodialysis patients. Am J Ther. 2014 Jul-Aug;21(4):275–87.
Ravi S, Khalili H, Abbasian L, Arbabi M, Ghaeli P. Effect of Omega-3 Fatty Acids on Depressive Symptoms in HIV-Positive Individuals: A Randomized, Placebo-Controlled Clinical Trial. Ann Pharmacother. 2016 Oct;50(10):797–807.
Chang JP, Chang SS, Yang HT, Chen HT, Chien YC, Yang B, et al. Omega-3 polyunsaturated fatty acids in cardiovascular diseases comorbid major depressive disorder - Results from a randomized controlled trial. Brain Behav Immun. 2019 Mar;S0889-1591(18)31188-7.
Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam JD, Shelton RC, et al. Antidepressant drug effects and depression severity: a patient-level meta-analysis. JAMA. 2010 Jan;303(1):47–53.
Kirsch I, Deacon BJ, Huedo-Medina TB, Scoboria A, Moore TJ, Johnson BT. Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med. 2008 Feb;5(2):e45.
Dubovsky SL. What Is New about New Antidepressants? Psychother Psychosom. 2018;87(3):129–39.
Gordon BR, McDowell CP, Hallgren M, Meyer JD, Lyons M, Herring MP. Association of Efficacy of Resistance Exercise Training With Depressive Symptoms: Meta-analysis and Meta-regression Analysis of Randomized Clinical Trials. JAMA Psychiatry. 2018 Jun;75(6):566–76.
Chi X, Bo A, Liu T, Zhang P, Chi I. Effects of Mindfulness-Based Stress Reduction on Depression in Adolescents and Young Adults: A Systematic Review and Meta-Analysis. Front Psychol. 2018 Jun;9:1034.
Goyal M, Singh S, Sibinga EM, Gould NF, Rowland-Seymour A, Sharma R, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014 Mar;174(3):357–68.
Chan YY, Lo WY, Yang SN, Chen YH, Lin JG. The benefit of combined acupuncture and antidepressant medication for depression: A systematic review and meta-analysis. J Affect Disord. 2015 May;176:106–17.
Lichtenberg P, Belmaker RH. Subtyping major depressive disorder. Psychother Psychosom. 2010;79(3):131–5.
Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219–26.
De Las Cuevas C, de Leon J. Reviving Research on Medication Attitudes for Improving Pharmacotherapy: focusing on Adherence. Psychother Psychosom. 2017;86(2):73–9.
Fava GA, Guidi J, Rafanelli C, Sonino N. The clinical inadequacy of evidence-based medicine and the need for a conceptual framework based on clinical judgment. Psychother Psychosom. 2015;84(1):1–3.
Fava GA, Guidi J, Rafanelli C, Rickels K. The Clinical Inadequacy of the Placebo Model and the Development of an Alternative Conceptual Framework. Psychother Psychosom. 2017;86(6):332–40.
Horwitz RI, Hayes-Conroy A, Singer BH. Biology, Social Environment, and Personalized Medicine. Psychother Psychosom. 2017;86(1):5–10.
Appleton KM, Rogers PJ, Ness AR. Updated systematic review and meta-analysis of the effects of n-3 long-chain polyunsaturated fatty acids on depressed mood. Am J Clin Nutr. 2010 Mar;91(3):757–70.
Senthil Kumaran S, Shih YH, Su KP. Detecting the modest signals of omega-3 fatty acids' antidepressant effects by homogenizing depressed patient groups. Lipid Technol. 2016;28:86–7.
Rogers PJ, Appleton KM, Kessler D, Peters TJ, Gunnell D, Hayward RC, et al. No effect of n-3 long-chain polyunsaturated fatty acid (EPA and DHA) supplementation on depressed mood and cognitive function: a randomised controlled trial. Br J Nutr. 2008 Feb;99(2):421–31.
Ness AR, Gallacher JE, Bennett PD, Gunnell DJ, Rogers PJ, Kessler D, et al. Advice to eat fish and mood: a randomised controlled trial in men with angina. Nutr Neurosci. 2003 Feb;6(1):63–5.
Sublette ME, Ellis SP, Geant AL, Mann JJ. Meta-analysis of the effects of eicosapentaenoic acid (EPA) in clinical trials in depression. J Clin Psychiatry. 2011 Dec;72(12):1577–84.
Grenyer BF, Crowe T, Meyer B, Owen AJ, Grigonis-Deane EM, Caputi P, et al. Fish oil supplementation in the treatment of major depression: a randomised double-blind placebo-controlled trial. Prog Neuropsychopharmacol Biol Psychiatry. 2007 Oct;31(7):1393–6.
Marangell LB, Martinez JM, Zboyan HA, Kertz B, Kim HF, Puryear LJ. A double-blind, placebo-controlled study of the omega-3 fatty acid docosahexaenoic acid in the treatment of major depression. Am J Psychiatry. 2003 May;160(5):996–8.
Mozaffari-Khosravi H, Yassini-Ardakani M, Karamati M, Shariati-Bafghi SE. Eicosapentaenoic acid versus docosahexaenoic acid in mild-to-moderate depression: a randomized, double-blind, placebo-controlled trial. Eur Neuropsychopharmacol. 2013 Jul;23(7):636–44.
Silvers KM, Woolley CC, Hamilton FC, Watts PM, Watson RA. Randomised double-blind placebo-controlled trial of fish oil in the treatment of depression. Prostaglandins Leukot Essent Fatty Acids. 2005 Mar;72(3):211–8.

Return to OMEGA-3 FATTY ACIDS
Since 10-05-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |