

A Survey of Parent Satisfaction with
Chiropractic Care of the Pediatric PatientThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2014 (Nov); 14 (3): 1167–1171 ~ FULL TEXT
OPEN ACCESS By Ida Marie Navrud, DC, Joyce Miller, BSc, DC, DABCO, PhD,
Maja Eidsmo Bjřrnli, DC, Cathrine Hjelle Feier, DC, Tale Haugse, DC
Private practice, NorwayIntroduction: Chiropractic is a common parental choice as a therapeutic intervention for numerous pediatric conditions. No studies investigating parent satisfaction with pediatric chiropractic care have been published to date.
Method: All infants aged 0–36 weeks and presenting to a chiropractic teaching clinic on the south coast of England between January 2011 and October 2013 were eligible for inclusion. Parents completed questionnaires, which rated their own and their infant’s characteristics prior to, and at the end of, a course of chiropractic care. Non-parametric tests were used to analyze before and after care scores.
Results: A total of 395 results were collected in this study. Satisfaction scores of 10/10 (“completely satisfied”) were reported by 75.1% (n=295) of the parents. There was a significant improvement in parental distress (Median=5.0 before care, Median=2.0 after care, Z=–13.7, p<.001, r =–.49) and infants’ sleep quality (Median=5.0 before care, Median=3.0 after care, Z=–10.5, p<.001, r =–.38). Satisfaction scores were found to have a small correlation with sleep quality (rs =–.21) after care, as well as a moderate correlation with distress (rs =–.31) and improvement scores (rs =.42), p<.01.
Conclusion: The parents in this study appear to be satisfied with the care their infant received. However, the satisfaction scores and improvement scores are only moderately correlated, which indicates that there are other factors influencing the level of satisfaction.
MeSH terms: chiropractic, complementary therapies, infants, pediatrics
Key words: pediatric, satisfaction, parent, chiropractic, complementary alternative medicine
From the Full-Text Article:
Introduction
Satisfaction with chiropractic care for pediatric patients is currently an unexplored area in the literature. Measuring outcomes of care is essential in evidence-based healthcare, and satisfaction is a key concept in assessing patients’ perception of care. Studies of satisfaction can be useful in determining how well patients’ hopes and expectations are met when they receive a form of treatment. [1, 2] There is substantial agreement in the literature about satisfaction measures being valid in assessing quality of care. They allow patients to express their personal evaluation of health care services and practitioners. [3–7]
The concept of satisfaction is difficult to grasp, and even harder to define. The literature does not provide one clear definition, but some general components can be identified. It is often an emotional or cognitive response; pertaining to a particular focus or goal. [8, 9] Satisfaction has been described as the fulfillment of expectations, needs, or desires. [6] Ygge and Arnetz investigated parent satisfaction with hospital care for the pediatric patient. They found that parents were most satisfied with staff attitudes, care processes, and medical treatment. Accessibility and staff work environment received the lowest satisfaction scores. [10] It has been suggested that patient satisfaction is dependent on the patient feeling empowered, in control of one’s life, and the establishment of an empathetic therapeutic relationship. Hope, communication, respect, and trust were the four main themes associated with the therapeutic relationship. [12] Good Communication stands out as a consistent determinant of overall satisfaction in several studies. [1, 6, 11–16]
However, in the care of the pediatric patient, the patient has no say in the matter, only the parent or guardian. Hence, satisfaction may take on a unique character in this domain. We hypothesize that parents might be most satisfied with improvement in the child’s condition. A survey was developed to test this theory, and investigate parental rating of satisfaction and other factors in patient care.
Methods
A cohort of parents presenting their infant to a chiropractic teaching clinic, located on the south coast of England, were followed through the course of care for their infant. All infants between the age of one day up to 36 weeks who presented between January 2011 and October 2013 were eligible for inclusion if the parents had completed both pre- and post-treatment questionnaires. No further exclusion criteria were used. A total of 395 valid results were collected and analyzed for this study.
Data were collected using two, practitioner-administered, questionnaires. The first was done prior to initiation of care, and the second on the day of discharge. In the first questionnaire, parents were asked to rate their level of distress due to the infant’s behavior. These metrics were measured using a 10–point scale, with 1 being the most positive (e.g. not at all distressed) and 10 being the most negative response (e.g. extremely distressed). The parents were asked to indicate the numerical value that best represented their perception of the questions asked. On the day of discharge, the parents were asked the same questions using the same methods. In addition, they were asked to rate the degree of improvement in their infant’s condition, and their satisfaction with the care received. The scale ranged from 1 (not at all) to 10 (completely better). Data on age, gender, number of treatments, and time frame of treatment (in weeks) were also collected.
All statistical analyses were conducted in IBM SPSS Statistics 20. [17] Measures of central tendency were calculated. Kolmogorov-Smirnov and Shapiro-Wilks tests were used to test the data for normality. Non-parametric tests were used as the data were not normally distributed, but also to account for the ordinal nature of the majority of the data. The Mann-Whitney U test was performed to assess for differences between two independent groups. Wilcoxon’s signedrank test was used to compare scores before and after care. Spearman’s rank correlation coefficient (Spearman’s rho) was calculated to assess the relationship between variables. According to Cohen, a correlation coefficient of 0.1–0.3 is defined as small, moderate if 0.3–0.5, and high if greater than 0.5. [18]
The Anglo European College of Chiropractic (AECC) ethics panel approved the study, and data from all patients were anonymous.
Results

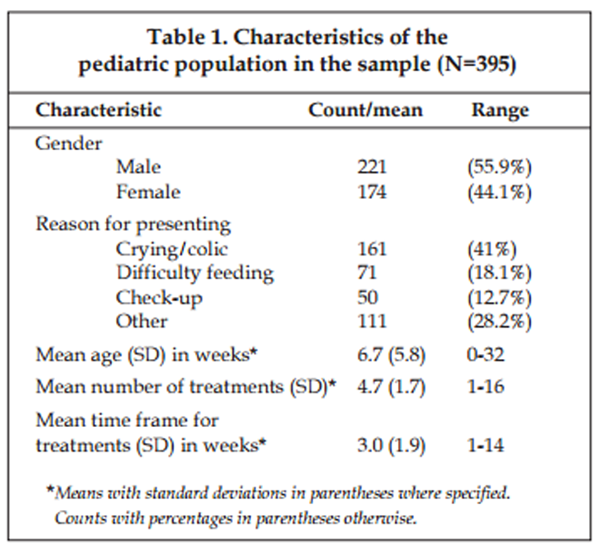
Table 1 A summary of the sample characteristics can be found in Table 1. The sample consisted of 11.8% (n=47) more males than females. Mann-Whitney U tests were performed to assess for differences between genders, but no significant differences were detected.
The main reasons for presenting to the clinic were“crying/colic” (41%)
“difficulty feeding” (18.1%) and
“check up” (12.7%).Reasons mentioned under “other” included:
“birth trauma” (5.1%)
“will not lie supine with comfort” (5.3%)
“cannot turn head equally” (5.1%)
“positional head deformity” (3.8%)
“sleep” (3.6%)
“axial musculoskeletal” (2.5%) and
“appendicular musculoskeletal”(.3%).
Table 2 Participating parents were asked to rate their level of distress on a 1–10 scale, with 1 being “not at all” and 10 being “extremely distressed”, before and after care (Table 2). Distress scores of 5 and below were reported by 56.0% before care, and 92.6% after care. This was further investigated through a Wilcoxon signed-rank test, and there was a significant decrease in distress from before care (Median=5.0) to after care (Median=2.0), Z=–13.7, p<.001, r =–.49.
Sleep quality before and after care was assessed on a 1–10 scale, with 1 representing “sleeps deeply and restfully most of the time” and 10 representing “restless, difficult to settle or stay asleep or does not sleep deeply.” Scores of 5 or lower were reported by 50.6% before care, and 78.6% after care. Wilcoxon’s signed-rank test revealed a significant improvement in sleep scores from before care (Median=5.0) to after care (Median=3.0), Z=–10.5, p<.001, r =–.38.
The amount of over-all improvement was investigated through a 1–10 scale, where 1 represented “infant’s condition is worsened” and 10 represented “completely better.” The lowest score reported was 2, indicating “no change,” and 8.7% reported scores of 5 and lower. Scores from 8 to 10 (indicating good or total recovery) were reported by 69.1%. Parents were also asked to rate their level of satisfaction with the care on a scale from 1–10, with 1 being “not at all” and 10 being “completely satisfied.” Scores below 7 were reported by 1.3%, and a total of 75.1% responded that they were completely satisfied (Table 2).
Table 3 All correlations between improvement, satisfaction, distress after care, and sleep quality after care were statistically significant at the .01 level (Table 3). The positive correlations indicate that high scores in one group are associated with high scores in the other group, and that low scores in one group are associated with low scores in the other group. The negative correlations, however, indicate that high scores in one group are associated with low scores in the other group. Distress and sleep quality scores are better the lower they are, whereas satisfaction and improvement scores are better the higher they are.
The Spearman’s rho revealed a small negative correlation between satisfaction and sleep quality after care (–.21). A moderate positive correlation was found between satisfaction and improvement scores (.42). Moderate negative correlations were found between improvement and sleep quality after care (–.37), between improvement and distress after care (–.39), as well as between satisfaction and distress after care (–.31). Furthermore, a high positive correlation was revealed between distress after care and sleep quality after care (.53).
Discussion
Table 4 The parents in this study reported high levels of satisfaction, and improvement of the presenting condition. Parents reported a decrease in their distress levels, and an improvement in the infant’s sleep quality after an episode of care. For example, lower levels of parental distress correlate with higher parental satisfaction. Analysis of the data revealed a moderate positive correlation between satisfaction and improvement scores. A moderate negative correlation was found between satisfaction scores and parents’ level of distress. Satisfaction and sleep quality after care demonstrated a small negative correlation. This is suggestive of high improvement scores, improved sleep quality, and lower levels of parental distress being associated with high levels of satisfaction (Table 4). However, these correlations were not strong enough to account for the high satisfaction levels reported in this study. This suggests that other factors, not investigated in this study must influence parent satisfaction. The literature suggests that satisfaction is a multidimensional concept, and thus other possible factors should be investigated. Suggestions of such factors include practitioner’s communication skills and interpersonal manner, time spent with the patient, and time allowed for questions. In addition, sociodemographics and treatment cost could play a role. [14, 15] It should be noted that parents pay for care at this clinic, whereas medical care is free in the UK.
According to Jackson et al., satisfaction levels obtained at the end of the treatment course provide more information on treatment success than those obtained early in the course of treatment. [19] Satisfaction scores obtained early on are thought to provide an evaluation of factors such as the clinician, the clinic, and patient-practitioner interaction. Clinical outcome and satisfaction have been found to be positively linked. [20] However, a study by Williams et al. suggests that high satisfaction rates do not necessarily mean high quality of care; it could also be that no situations leading to dissatisfaction were encountered. [21] It appears that while efficacious therapeutic techniques are important, other variables may have a greater impact on reported satisfaction. These include communication, practitioner’s technical skills and interpersonal manner, time spent with practitioner, accessibility and availability of services, and the financial aspects through the course of treatment. [8, 15, 19–21]
While satisfaction studies can be an effective tool in gathering patients’ perceptions of health care environments, they are challenging to execute. Satisfaction is a multidimensional concept, making it difficult to measure accurately. [22] Satisfaction studies have been criticized for demonstrating a lack of standardization, low reliability, and uncertain validity of results due to generally high reported satisfaction levels and lack of variability in responses. This caused Haggerty to question whether satisfaction is a flawed way of evaluating practice performance. [23] It has been suggested that dissatisfaction might be a more valuable concept. Negative findings will give feedback of areas requiring improvement, and it is thought to give a greater understanding of what patients expect from their treatment. [2, 5, 21]
The questionnaires utilized in this study were presented to the parents in the treatment room, and placed in the chart upon completion. Interviewer–administered questionnaires tend to yield responses in a socially desirable direction. [24] The parents might have felt embarrassed to give a low score, which may have resulted in unrealistically high satisfaction scores. The validity of a survey depends on subjects’ honesty in their responses. [24] Additionally, some evidence suggests that non–responders tend to be less satisfied than responders. [25]
An unknown number of pediatric patients seen at the clinic may never have been included in this study. There can be various reasons for this; their practitioner did not provide the questionnaire for completion, the parents were not willing to submit it, or the patient never returned to complete the care regime. One can only speculate if these outstanding responses, which leave an unfilled gap in the results, could be due to dissatisfaction regarding their experience. Handling paper questionnaires versus electronic is a time and resource consuming process. The data were entered manually, which is associated with data entry errors, although 10% were checked for accuracy. It also results in very slow feedback, thus delaying the actions on problems identified. [26]
Although no studies have been published on the topic of parent satisfaction with chiropractic pediatric care, a pilot study was carried out at a private clinic in France in 2012. This was a much smaller study than the one carried out at the UK clinic, but the results were similar, showing high levels of satisfaction with care. [27]
Conclusion
This study showed that parents generally were very satisfied with chiropractic care of their child. Correlations between high satisfaction and improvement of the infant’s presenting complaint, improved sleep quality, and lower levels of parental distress were observed. As these correlations were not strong enough to account for the high satisfaction levels reported, additional research is needed to identify other factors influencing parent satisfaction with pediatric chiropractic care.
References:
Conner JM, Nelson EC.
Neonatal intensive care: satisfaction measured from a parent’s perspective.
Pediatrics 1999; 103, 336-349.Sofaer S, Firminger K.
Patient perceptions of the quality of health services.
Annu Rev Public Health 2005; 26, 513-59.Crow R, Gage H, Hampsom S, Hart J, Kimber A, Storey L, Thomas H.
The measurement of satisfaction within healthcare: implications for practice from a systematic review of the literature.
Core Research 2002Hall JA, Dornan MC.
Patient sociodemographic characteristics as predictors of satisfaction with medical care: a meta-analysis.
Social Science & Medicine 1990; 30 (7), 811-818.Sawyer C, Kassak K.
Patient Satisfaction With Chiropractic Care
J Manipulative Physiol Ther 1993 (Jan); 16 (1): 25–32Sitzia J, Wood N.
Patient satisfaction: a review of issues and concepts.
Social Science & Medicine 1997; 45 (12), 1829-1843.Ware Jr JE, Snyder MK, Wright WR, Davies AR.
Defining and measuring patient satisfaction with medical care.
Evaluation and Program Planning 1983; 6 (3), 247-263.Oliver RL.
Satisfaction: A behavioral perspective on the consumer. 2nd ed.
New York: ME Sharpe Inc; 2010.Giese JL, Cote JA.
Defining consumer satisfaction.
Academy of Marketing Science Review 2000; 1 (1), 1-22.Ygge B-M, Arnetz JE.
Quality of paediatric care: application and validation of an instrument for measuring parent satisfaction with hospital care.
International Journal for Quality in Health Care 2001;13 (1), 33-43.Halfon N, Inkelas M, Mistry R, Olson LM.
Satisfaction with health care for young children.
Pediatrics 2004; 113, 1965-72.Hong SS, Murphy SO, Connolly PM.
Parental satisfaction with nurses’ communication and pain management in a pediatric unit.
Pediatric Nursing 2008; 34 (4), 229-289.Maisels MJ, Kring EA.
A simple approach to improving patient satisfaction.
Clinical Pediatrics 2005; 44 (9), 797-800.Strutt R, Shaw Q, Leach J.
Patients’ perceptions and satisfaction with treatment in a UK osteopathic training clinic.
Manual Therapy 2008;13 (5), 456-467.Gaumer G.
Factors Associated With Patient Satisfaction With Chiropractic Care:
Survey and Review of the Literature
J Manipulative Physiol Ther 2006 (Jul); 29 (6): 455–462Breen A. and Breen R.
Back Pain and Satisfaction with Chiropractic Treatment:
What Role Does the Physical Outcome Play?
The Clinical Journal of Pain 2003 (Jul); 19 (4): 263–268IBM Corp.
IBM SPSS Statistics for Windows, Version 20.0.
Armonk, NY: IBM Corp; 2011.Cohen J.
Statistical power analysis for the behavioural sciences.
Hillsdale, NJ: Erlbaum Associates; 1998.Jackson JL, Chamberlin J, Kroenke K.
Predictors of patient satisfaction.
Social Science & Medicine 2001; 52 (4), 609-620.Pascoe GC.
Patient satisfaction in primary health care: a literature review and analysis.
Evaluation and Program Planning 1983; 6 (3), 185-210.Williams B, Coyle J, Healy D.
The meaning of patient satisfaction: an explanation of high reported levels.
Social science & medicine 1998; 47(9)1351-1359.Larsson G, Larsson BW.
Quality improvement measures based on patient data: Some psychometric issues.
International Journal of Nursing Practice 2003; 9 (5), 294-299.Haggerty, J. L.
Are measures of patient satisfaction hopelessly flawed.
BMJ 2010; 341, c4783Kreuter F, Presser S, Tourangeau R.
Social Desirability Bias in CATI, IVR, and Web Surveys The Effects of Mode and Question Sensitivity.
Public Opinion Quarterly 2008; 72(5), 847-865.Sitzia J, Wood N.
Response rate in patient satisfaction research: an analysis of 210 published studies.
Int J Qual Health Care 1998;10 (4), 311-317Ammentorp J, Rasmussen A M, Nřrgaard B, Kirketerp E, Kofoed P.
Electronic questionnaires for measuring parent satisfaction and as a basis for quality improvement.
International Journal of Quality in Health Care 2007; 19(2): 120-124Klingelschmitt-Brachet V.
Survey on parent’s satisfaction for paediatric care of children aged to 0 to 10 years in a private chiropractic clinic.
UK: Anglo-European College of Chiropractic
Return to PEDIATRICS
Return to PATIENT SATISFACTION
Since 2-03-2016



| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |