

The Pediatric Elbow:
A Review of FracturesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Dynamic Chiropractic (June 3, 2011)
By Deborah Pate, DC, DACBR
The elbow fracture is one of the most common fractures in children. Assessing the elbow for fracture can be difficult because of the changing anatomy of the growing skeleton and the subtlety of some of these fractures.
It's important to be aware of the radiographic signs of fracture in the elbow, along with knowing the appearance and fusion of the ossification centers in the pediatric patient, to avoid confusing an ossification center with a fracture fragment. Of course, alignment and radiographic positioning are also extremely important in making a diagnostic assessment.
When reviewing an X-ray study for trauma, it's best to have a methodical way of viewing the study. Perform (at the very least) two views of the elbow at 90° to each other, AP and lateral. Positioning is very important, particularly in the growing skeleton. Alignment of the joint cannot be assessed unless the positioning is accurate.
The two most common errors in positioning are: 1) elbow is lower than the shoulder, which projects the capitellum onto the ulna; and 2) elbow is higher than the wrist, which will make the capitellum and the head of the radius appear anterior, and the epicondyle appear posterior, making it difficult to assess the alignment. In a true lateral view, the elbow and the shoulder should be in the same plane and the wrist should be higher than the elbow to compensate for the normal valgus position of the elbow. The thumb should be up to keep the radius from rotating.
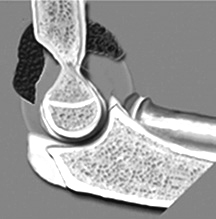
Diagram of a distended
joint capsule with the
fat pads displaced.
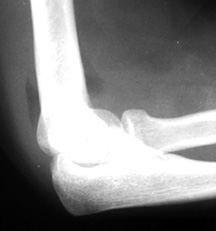
X-ray demonstrating
positive fat pad sign.Once X-rays are taken, it's a matter of reviewing the films methodically. Four questions should be kept in mind when reviewing pediatric trauma cases (when in doubt, have the films reviewed by a radiologist):
- Is there a sign of joint effusion?
- Are the bones in normal alignment?
Are the ossification centers normal? (In an adult, the question would be whether the joint spaces are maintained.)
Is there a subtle fracture? In children, rule out elbow fractures by paying particular attention to the following: supracondylar fracture with minimal displacement; lateral condyle fracture; slipped radial epiphysis; radial dislocation; and position of the medial epicondyle.
Is There Joint Effusion?
The way to evaluate joint effusion in the elbow is to look for a positive fat pad sign. Normally, when the elbow is flexed to 90°, the anterior fat pad may be seen just anterior to the joint; the posterior fat pad is not seen because it is located in the intercondylar fossa. With joint distention, the fat pads are displaced away from the joint in the anterior aspect; the fat pad will be elevated away from the joint and the posterior fat pad will be visible.
If a positive fat pad sign is not present in a child, significant intra-articular injury is considered unlikely; but on the other hand, if a visible fat pad sign is demonstrated without the appearance of a fracture, the patient should be treated as having a non-displaced fracture and should be splinted for two weeks and then re-evaluated. It is generally agreed that in the case of trauma, a displaced posterior fat pad is virtually pathognomonic of the presence of a fracture.
Assessing alignment:
The radiocapitellar line.Is the Alignment Normal?
There are two important lines that help in the assessment of normal alignment of the elbow. These are the radiocapitellar line and the anterior humeral line.
The radiocapitellar line is drawn through the center of the radial neck and should pass through the center of the capitellum. Even if the positioning isn't optimal, the capitellum should always be in alignment with the radius, since they articulate with each other. This should be true in both the AP and the lateral views. If not, there is a dislocation of the radius and one should look for other signs of fracture.
The anterior humeral line is drawn on a lateral view along the anterior surface of the humerus; it should pass through the middle third of the capitellum. In cases of supracondylar fracture, the anterior humeral line usually passes through the anterior third of the capitellum or in front of the capitellum, due to posterior bending of the distal humeral fragment.
Assessing alignment:
The anterior
humeral line.Are the Ossification Centers Normal?
There are six ossification centers around the elbow joint. They appear and fuse to the adjacent bones at different ages. The order of appearance is as follows: capitellum, radius, medial epicondyle, trochlea, olecranon and lateral epicondyle. This order never varies, but the ages at when they appear is variable and differs between individuals. In general, the capitellum appears at 1-3 years, medial epicondyle at 3-5 years, trochlea at 5-7 years, olecranon at 7-9 years and lateral epicondyle at 9-11 years. The age of appearance isn't nearly as important as is the order of appearance, because this never varies. (Mnemonic is Cover My Truck Of Love; no, I didn't make it up.)
Fractures by Type
Supracondylar fractures make up 60 percent of all fractures involving the elbow in children. There are two types of supracondylar fractures based on the mechanism of injury: 96 percent are extension-type fractures and 4 percent are flexion-type fractures.
The extension-type fracture is caused by a fall on the outstretched hand with the elbow hyperextended. The distal fragment of the humerus will angulate and displace posteriorly, depending on the severity of the trauma. There is a relatively high risk of nerve injury (approximately 10 percent of fractures) associated with this injury.
When there is nerve injury, the radial nerve is most commonly involved, followed by the median nerve and then the ulnar nerve. Radiological evaluation of these fractures can be difficult depending on the amount of displacement. The fat pad sign is very helpful. Also use the anterior humeral line, which normally intersects the middle third of the capitellum; in supracondylar fractures, the line often intersects the anterior third of the capitellum or beyond.
Lateral condyle fractures are the second most common fracture, accounting for about 15 percent of elbow fractures. Two mechanisms of injury have been proposed. First, the injury may result from a fall on the outstretched hand with the forearm supinated, which transmits a force through the forearm extensor musculature to its attachment on the lateral condyle. Second, these fractures may also occur with a force directed to the outstretched hand with the elbow flexed. The fracture can be easily identified radiographically if the capitellum is well-ossified and displaced. In more difficult cases, oblique radiographs may be helpful.
radiocapitellar line Assessing alignment: The radiocapitellar line. Medial epicondyle fractures are the third most common fracture, accounting for approximately 10 percent of elbow fractures. These are typically seen in an older age group, most commonly adolescent males. This injury results from a valgus force combined with contraction of the forearm flexor muscles. If the valgus force is great enough, elbow dislocation can result, in addition to avulsion of the medial epicondyle.
Radiographic diagnosis is not difficult in displaced fractures. In non-displaced fractures, the apophysis of the medial epicondyle may appear wider than normal. Comparison with the contralateral side will often be helpful in these situations.
anterior humeral line Assessing alignment: the anterior humeral line. Proximal radius fractures are the most common fracture of the elbow in adults, but only account for about 8 percent of fractures in the pediatric population. These fractures also differ from those seen in adults because they usually involve the radial neck and physis, rather than the radial head, as in adults. These injuries can result from a fall on the outstretched hand with the elbow extended. In the skeletally immature, the force is transmitted through the head, which is mostly cartilage, and directed to the physis and metaphysis. These fractures may also occur in association with posterior dislocation of the elbow.
Displaced fractures are usually easily diagnosed via radiographs. However, non-displaced fractures can be difficult to visualize radiographically. Oblique views of the radius may be helpful.
To perform oblique views, simply place the elbow in an AP position and then externally rotate the arm 45°; this profiles the anterior and anterolateral aspect of the radial head and neck, and the articular surface of the capitellum. If the arm is internally rotated 45°, this will profile the tip of the coronoid process and the margin of the trochlea.
One other common elbow injury that occurs rather frequently in children less than 5 years old is displacement of the annular ligament; commonly referred to as nursemaid's elbow. When the forearm is pulled or jerked up, as in lifting a child up onto a step or pulling them up from a seated position, the radial head moves distally and the annular ligament slips over the radial head, becoming trapped within the joint. This is because the annular ligament that binds the radial head to the ulna is loosely attached to the radial neck. This problem can be resolved by supination of the forearm, if you are clever enough to distract the child to perform the maneuver.
Deborah Pate is a licensed chiropractor and a diplomate of the American Chiropractic Board of Radiology. A 1982 graduate of National College of Chiropractic, she was the first chiropractor accepted into a fellowship in osteoradiology at the medical center of the University of California, at San Diego. Dr. Pate served as a research associate in the radiology department at the VA hospital from 1984 to 1986, and as chiropractic director of the American Chiropractic Network (now American Specialty Health Plans), both in San Diego, California, for several years. Still a consultant for several insurance companies, she has practiced as a clinician and radiology consultant since 1984, and maintains a radiology consulting practice. Dr. Pate is also a state-appointed qualified medical examiner and a certified disability evaluator. She has taught postgraduate courses at Parker College of Chiropractic, Los Angeles College of Chiropractic, the University of California at San Diego, and other respected institutions.

Return to RADIOLOGY
Return to PEDIATRICS
Since 12-20-2001
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |