

Diagnostic and Treatment Methods Used by
Chiropractors: A Random Sample Survey
of Canada's English-speaking ProvincesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc. 2015 (Sep); 59 (3): 279–287 ~ FULL TEXT
OPEN ACCESS Aaron A. Puhl, MSc, DC, Christine J Reinhart, PhD, DC, and H. Stephen Injeyan, PhD, DC
Department of Pathology and Microbiology,
Canadian Memorial Chiropractic College,
Toronto, ON, M2H 3J1.
OBJECTIVE: It is important to understand how chiropractors practice beyond their formal education. The objective of this analysis was to assess the diagnostic and treatment methods used by chiropractors in English-speaking Canadian provinces.
METHODS: A questionnaire was created that examined practice patterns amongst chiropractors. This was sent by mail to 749 chiropractors, randomly selected and stratified proportionally across the nine English-speaking Canadian provinces. Participation was voluntary and anonymous. Data were entered into an Excel spreadsheet, and descriptive statistics were calculated.
RESULTS: The response rate was 68.0%. Almost all (95.1%) of respondents reported performing differential diagnosis procedures with their new patients; most commonly orthopaedic testing, palpation, history taking, range of motion testing and neurological examination. Palpation and painful joint findings were the most commonly used methods to determine the appropriate joint to apply manipulation. The most common treatment methods were manual joint manipulation/mobilization, stretching and exercise, posture/ergonomic advice and soft-tissue therapies.
CONCLUSIONS: Differential diagnosis is a standard part of the assessment of new chiropractic patients in English-speaking Canadian provinces and the most common methods used to determine the site to apply manipulation are consistent with current scientific literature. Patients are treated with a combination of manual and/or manipulative interventions directed towards the joints and/or soft-tissues, as well as exercise instruction and postural/ergonomic advice.
There are more articles like this @ our:
CHIROPRACTIC SUBLUXATION PageKEYWORDS: chiropractic; diagnostic testing; differential diagnosis; survey; treatment methods
From the FULL TEXT Article:
Introduction
Doctors of Chiropractic (DC) focus on the evaluation and management of disorders of the musculoskeletal system [1] and there is a movement towards adopting a role as primary spine care providers. [2, 3] The appropriate management of a patient requires the DC to diagnose the complaint, determine the best course of treatment and finally, provide that treatment, or refer to another healthcare provider for appropriate care. DCs are taught numerous diagnostic and therapeutic procedures during their undergraduate education and clinical internships and perhaps just as important, they are also able to obtain certifications through seminars and continuing education courses to employ a diversity of assessment and treatment techniques that may not be introduced within the context of their formal educational settings. It is imperative that we understand how Canadian DCs diagnose and treat their patients in order to guide research, guide the undergraduate, post-graduate and continuing educational chiropractic curricula, as well as to inform all stakeholders, including the public, insurance companies and government agencies about chiropractic practice.
While previous studies have investigated similar topics among Canadian DCs [4-7], those previous examinations are limited by the age of the analysis [4], limited sampling [5-7], or poor response rates [6, 7], resulting in poor reliability and generalizability. Moreover, no previous study has specifically investigated what methods Canadian DCs are using in clinical practice to decide where to apply joint manipulation, which is the most notable treatment method used by chiropractors. [8] The objectives of this descriptive analysis of DCs in English-speaking Canadian provinces were to1) determine if DCs are performing differential diagnosis procedures and describe the methods used for this purpose;
2) describe the tests/procedures used to determine the site of joint manipulation and the frequency of their use; and
3) describe the treatment methods used and the frequency of their use.
Methods
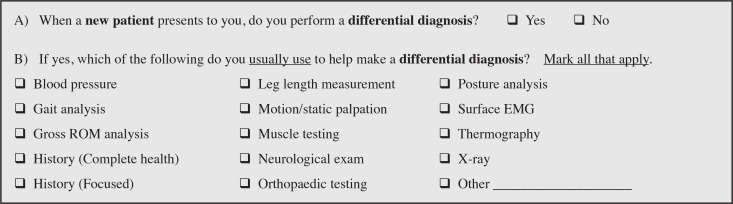
Figure 1
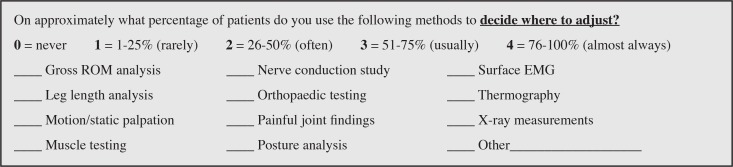
Figure 2
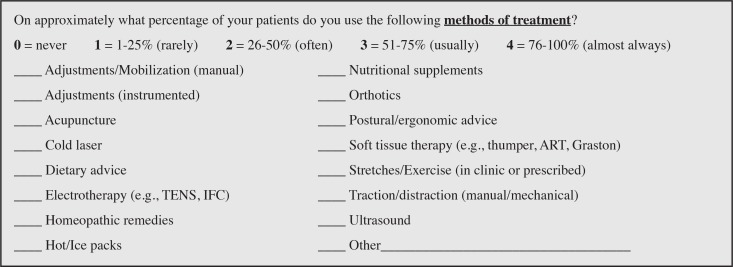
Figure 3 Survey development and administration have been detailed in previous works. [9, 10] In short, a 16 item survey instrument was developed by the authors that included topics ranging from practice techniques to practice philosophy. This paper reports on the data from three questions (Figures 1–3), which specifically addressed approaches to diagnosis and treatment. The survey instrument was tested by ten DCs and revisions were made to the survey instrument after interviewing the test subjects to identify any problems. A list of all currently licensed DCs for each of the nine English-speaking Canadian provinces was developed from the online directories of the provincial chiropractic licensing bodies.
A random sample was selected from each provincial list using a computerized random number generator; the final sample included 749 DCs (12% of eligible DCs), stratified proportionally across the English-speaking Canadian provinces. The survey was administered by mail from August 2010 to December 2010 and used postage-paid, return addressed envelopes and two follow-up mailings to maximize response rates. [11] Surveys were mailed with a personalized letter briefly explaining the purpose of the study, guaranteeing anonymity and providing a means of avoiding future mailings if they did not wish to participate; informed consent was implied by participation. The CMCC Research Ethics Board approved the study protocol (REB Approval # 1006X02) and the CMCC Research Division provided all funding.
In order to determine the use of various diagnostic procedures by DCs for the purposes of differential diagnosis, subjects were asked to document, from alphabetized lists of tests/procedures, which procedures they commonly used (Figure 1). With regard to determining where to apply joint manipulation, subjects were asked to document, from an alphabetized list of diagnostic procedures, which tests/procedures they used and also to indicate the percentage of patients on whom they used each procedure (Figure 2). To determine which treatment methods are being employed, participants were asked to document, from an alphabetized list, which treatment modalities they used and the frequency with which they are used (Figure 3).
All survey data were entered into an electronic spreadsheet by two authors using the double data entry method to control for errors. Descriptive statistics were used to report the data.
Results

Table 1
Table 2
Table 3
Table 4 Of 740 deliverable surveys, 503 were returned, a response rate of 68.0%; seven respondents returned the cover page only, indicating they did not wish to participate; nine surveys were undeliverable. The majority of respondents were male (68.4%); had attained a Bachelor’s degree prior to attending chiropractic college (76.2%); and had attended chiropractic college at CMCC (62.6%). The average number of years in practice was 14.9 (standard deviation ±11.0). Table 1 contains the response rates and demographic information of respondents by province.
The vast majority (470/494; 95.1%) of respondents reported performing differential diagnosis procedures when a new patient presents to them for the first time. The prevalence of use of common diagnostic tests/procedures for the purpose of differential diagnosis is detailed in Table 2. The most commonly used diagnostic tests/procedures were orthopaedic testing (88.8%), palpation (88.0%), history taking (83.5%), range of motion (80.0%) and neurological examination (79.9%); each of which were used by at least 80% of respondents. With regard to determining where to apply joint manipulation procedures, the prevalence of use of common diagnostic tests/procedures and the proportion of patients on which they are used is detailed in Table 3. The most commonly used tests/procedures for determining where to apply spine manipulation were palpation (98.4%) and painful joint findings (89.8%); both used by at least 90% of respondents and used on the majority of their patients. Also commonly used was analysis of posture, range of motion and leg length, as well as orthopaedic testing (each used by at least 80% of respondents).
The prevalence of use of specific treatment methods by respondents is detailed in Table 4. The most commonly used methods of treatment were manual joint manipulation and/or mobilization (99.0%), stretching and/or exercises (96.0%), posture and/or ergonomic advice (90.8%) and soft-tissue therapies (85.4%). These were each used by greater than 85% of respondents and used on the majority of their patients. Also used by a significant majority (>80%) of respondents, but used on only small proportion of their patients, were orthotics and dietary advice.
Discussion
While at least 65% of chiropractic patients have been shown to present for back pain [12], several medical conditions, such as cancer, infections, and visceral disease, are known to mimic non-specific, low back pain conditions. [13-15] As such, appropriate and skilled examinations are imperative for the delivery of optimal patient care. Indeed, the Canadian Chiropractic Association suggests that the chiropractic profession adheres to a patient-centred, biopsychosocial approach to health care that encompasses examination, diagnosis and treatment [16] and clinical practice guidelines suggest that the accurate diagnosis of patient conditions is key to effective management and treatment. [17] DCs are taught numerous diagnostic procedures during their undergraduate education and clinical internships and analyses conducted by the National Board of Chiropractic Examiners in the United States (US) have suggested that US DCs develop differential diagnoses on a daily basis. [18]
However, to our knowledge only one recent investigation has assessed the use of diagnostic tests/procedures by Canadian DCs. [7] While the aforementioned study attempted a more specific assessment of the individual diagnostic tests and therapeutic procedures used by Canadian DCs than our current study, it had a number of limitations, including a very low response rate and a pseudo-randomized sampling method, which reduces both the reliability and generalizability of the findings. The present study suggests that nearly all (95%) DCs in English-speaking provinces are performing some form of differential diagnosis procedures with their new patients. The vast majority of respondents indicated using diagnostic methods consistent with standard assessment of musculoskeletal conditions [19]; that is, history taking, orthopedic testing, palpation, range of motion testing and neurological exams.
Notable is the fact that only a minority (28.5%) of DCs surveyed indicated using blood-pressure assessment as a common diagnostic test with new patients. Blood-pressure measurement can aid in the identification of cardiovascular, or pulmonary problems that might affect prognosis and intervention, or require referral to another practitioner. Indeed, it has been argued that blood-pressure measurements can prove to be an appropriate objective test for assessment prior to manual therapy interventions and provide direction for risk assessment and/or the management of patients. [20] That only a minority of respondents indicated assessing new patient’s blood-pressure makes us question whether they are aware of the relevance of hypertension to the clinical reasoning necessary for the optimal management of musculoskeletal patient populations.
In addition to the standard tests involved with the diagnosis of a musculoskeletal complaint, DCs and other professionals who use joint manipulation will often perform supplementary physical examinations to determine whether dysfunctional joints are present that may be contributing to a patient’s condition. If dysfunctional joints are present and no contraindications are found, manipulative procedures are often applied with the intent of improving joint biomechanics and function, which in turn may explain the efficacy of manipulative therapy for improving mobility and reducing pain. However, numerous reviews examining the validity and reliability of common examination methods intended to identify dysfunctional spinal joint segments have, to date, suggested that many tests are relatively unreliable and/or invalid. [21-26] Scientific investigation seems most supportive of direct, mechanical methods of assessing and identifying the site of care, such as maneuvers that replicate the patient’s familiar pain. [26]
There is also some evidence suggesting that palpation and leg-length analysis may be useful for some applications and orthopedic maneuvers may help narrow the region where treatment may be applied. On the other hand, the evidence is not supportive of less direct methods such as manual muscle testing for non-pathological states, radiographic measurements, thermography and surface electromyography. [26]
The present study thus suggests that DCs in English-speaking Canadian provinces are practicing consistently with the current scientific literature, as “palpation” and “painful joint findings” were the most commonly used methods for identifying spinal segments that could benefit from joint manipulation, used by nearly every respondent, on nearly every patient. Moreover, methods that are currently not supported by the scientific literature, such as radiographic measurements, thermography and surface electromyography, were the least-commonly used procedures. Nevertheless, it is a concern that there is a notable minority of DCs that reported regularly using methods not shown to be valid or reliable. Our data also suggests that DCs in Canada’s English-speaking provinces use a combination of examination findings to identify spinal segments that could benefit from joint manipulation. While many clinical tests are of questionable diagnostic value, it has been suggested in the literature that improved diagnostic accuracy can be achieved by using combinations of clinical examination findings, as compared with individual physical examination tests. [27] As such, the use of examination methods with only low to moderate reliability and validity may add some clinical value when used in conjunction with pain provocation; to our knowledge, no analysis has examined the use of combination tests for identifying levels of segmental dysfunction in the spine.
In addition to the joint manipulation procedures commonly associated with care from a DC, nutritional and postural advice, lifestyle counselling and prescription of exercises have long been associated with chiropractic practice and are often considered as important hallmarks of the profession. In 1997, the Canadian Chiropractic Research Databank reported that the treatment techniques used by greater than 80% of chiropractors were joint manipulation, patient education and exercise. [4] Although our current data suggests that similar treatment modalities are still being used by most DCs, there was a notable increase in the use of soft-tissue therapies. In 1997, only 71.9% of Canadian DCs reported using soft-tissue therapies, whereas this survey saw 85.4% of respondents indicating the use of soft-tissue therapies. This finding is consistent with the previously suggested trend towards the use of proprietary soft tissue therapies (e.g., Active Release Therapy, Graston technique, etc.) for patient care. [6, 28] Our data suggest that the majority of chiropractors in English-speaking Canadian provinces today use a combination of manual and/or manipulative interventions directed towards the joints and soft-tissues, as well as exercise instruction and postural/ergonomic advice when they treat their patients.
Our study has some important strengths and limitations. The relatively high response rate (68%) may be considered a strength that increases the validity of the findings, however we do recognize that this was a select sample, and the chiropractors surveyed may not be representative of all Canadian DCs. The exclusion of French-speaking Canadian provinces and the Canadian territories means that our data might not be generalizable to those regions, but was necessary to avoid confounds related to language and regulatory differences. Respondents may have been influenced by social-desirability bias. The survey did not provide an operational definition for the term ‘differential diagnosis’, thus it is possible that some respondents misinterpreted the meaning of this term. We acknowledge that although the survey items were constructed using examples from the existing literature, the survey instrument used in this study was not previously tested or validated.
Conclusion
Differential diagnosis is a standard part of the assessment of new chiropractic patients in English-speaking Canadian provinces and this is most commonly done using orthopaedic tests, palpation, history-taking, range of motion testing and neurological examination. The clinical tests/procedures used most commonly by these DCs to determine where to apply joint manipulation are palpation and painful joint findings. These methods are consistent with the current scientific literature. Chiropractic patients in Canada’s English-speaking provinces are treated with a combination of manual joint manipulation/mobilization, exercise, posture/ergonomic advice and soft-tissue therapies. These treatment methods are consistent with earlier analyses of Canadian DCs, but the data do suggest that chiropractors in Canada are increasingly using soft-tissue therapies as part of their therapeutic regimen.
Funding Support:
CMCC’s Research Division provided all funding.
REFERENCES:
Coulter ID, Hurwitz EL, Adams AH, Genovese BJ, Hays R, Shekelle PG.
Patients Using Chiropractors in North America:
Who Are They, and Why Are They in Chiropractic Care?
Spine (Phila Pa 1976) 2002 (Feb 1); 27 (3): 291–298Nelson, C., Lawrence, D., Triano, J., Bronfort, G., Perle, S., Metz, R. D., et al.
Chiropractic As Spine Care: A Model For The Profession
Chiropractic & Osteopathy 2005 (Jul 6); 13: 9Erwin WM, Korpela AP, Jones RC.
Chiropractors as Primary Spine Care Providers:
Precedents and Essential Measures
J Can Chiropr Assoc. 2013 (Dec); 57 (4): 285–291Kopansky-Giles D, Papadopoulos C.
Canadian Chiropractic Resources Databank (CCRD): a profile of Canadian chiropractors.
J Can Chiropr Assoc. 1997;41(3):155–191.Waalen JK, Mior SA.
Practice patterns of 692 Ontario chiropractors (2000–2001)
J Can Chiropr Assoc. 2005;49(1):21–31Gleberzon B, Stuber K.
Frequency of Use of Diagnostic and Manual Therapeutic Procedures of the Spine Taught at
the Canadian Memorial Chiropractic College: A Preliminary Survey of Ontario Chiropractors.
Part 1 - Practice Characteristics and Demographic Profiles
J Can Chiropr Assoc. 2013 (Jun); 57 (2): 165–175Gleberzon B, Stuber K.
Frequency of Use of Diagnostic and Manual Therapeutic Procedures of the Spine Currently Taught at
the Canadian Memorial Chiropractic College: A Preliminary Survey of Ontario Chiropractors.
Part 2 - Procedure Usage Rates
J Can Chiropr Assoc. 2013 (Jun); 57 (2): 165–175Kaptchuk TJ, Eisenberg DM.
Chiropractic Origins, Controversies, and Contributions
Arch Intern Med 1998 (Nov 9); 158 (20): 2215-2224McGregor M, Puhl AA, Reinhart C, Injeyan HS, Soave D.
Differentiating intraprofessional attitudes toward paradigms in health care delivery among chiropractic factions:
results from a randomly sampled survey.
BMC Complement Altern Med. 2014;14:51Puhl AA, Reinhart CJ, Doan JB, McGregor M, Injeyan HS.
Relationship between chiropractic teaching institutions and practice characteristics among Canadian doctors
of chiropractic: a random sample survey.
J Manipulative Physiol Ther. 2014;37(9):709–718Russell ML, Verhoef MJ, Injeyan HS, McMorland DG.
Response rates for surveys of chiropractors.
J Manipulative Physiol Ther. 2004;27(1):43–48Hurwitz EL, Coulter ID, Adams AH, Genovese BJ, Shekelle PG.
Use of chiropractic services from 1985 through 1991 in the United States and Canada.
Am J Public Health. 1998;88(5):771–775Boissonnault WG, Bass C.
Pathological origins of trunk and neck pain: Part 1—Pelvic and abdominal visceral disorders.
J Orthop Sports Phys Ther. 1990;12:192–202Deyo RA, Rainville J, Kent DL.
What can the history and physical examination tell us about low back pain?
JAMA. 1992;268:760–765Patel AT, Ogle AA.
Diagnosis and management of acute low back pain.
Am Fam Phys. 2000;61(6):1779–1786Canadian Chiropractic Association Position Statements:
The Chiropractic Profession Within the Health Care Framework. Accessed 07/13.
http://www.chiropractic.ca/about-cca/code-of-ethics/chiropractic-profession-within-health-care-framework/Bryans R, Descarreaux M, Duranleau M, Marcoux H, Potter B, Ruegg R, Shaw L, Watkin R, White E.
Evidence-Based Guidelines For The Chiropractic Treatment Of Adults With Headache
J Manipulative Physiol Ther. 2011 (Jun); 34 (5): 274–289Christenson M, Kerkhoff D, Kollasch MW, et al.
A project report, survey analysis and summary of practice of chiropractic within the United States.
Greely, USA: National Board of Chiropractic Examiners;
The 1993 National Board of Chiropractic Examiners.
Job Analysis of Chiropractic 1993; p. 84.Souza T.
Differential Diagnosis and Management for the Chiropractor: Protocols and Algorithms.
Jones & Bartlett Publishers; Mississauga, ON: 2009.Taylor AJ, Kerry R.
Vascular profiling: should manual therapists take blood pressure?
Man Ther. 2013;18(4):351–353Walker BF.
The reliability of chiropractic methods used for the detection of spinal subluxation.
An overview of the literature.
Australas Chiropr Osteopathy. 1996;5(1):12–22Najm WI, Seffinger MA, Mishra SI, et al.
Content validity of manual spinal palpatory exams – a systematic review.
BMC Complement Altern Med. 2003;3:1Haneline MT, Young M.
A review of intraexaminer and interexaminer reliability of static spinal palpation:
a literature synthesis.
J Manipulative Physiol Ther. 2009;32(5):379–386Seffinger MA, Najm WI, Mishra SI, Adams A, Dickerson VM, Murphy LS, Reinsch S.
Reliability of spinal palpation for diagnosis of back and neck pain: a systematic review of the literature.
Spine (Phila Pa 1976) 2004;29(19):E413–E425Laslett M.
Evidence-based diagnosis and treatment of the painful sacroiliac joint.
J Man Manip Ther. 2008;16(3):142–152Triano J, Budgell B, Bagnulo A, Roffey B, Bergmann T, Cooperstein R.
Review of Methods Used by Chiropractors to Determine
the Site for Applying Manipulation
Chiropractic & Manual Therapies 2013 (Oct 21); 21 (1): 36Miller KJ, Sittler MD, Corricelli DM, DiMura DN, Comerford JS.
Combination testing in orthopedic and neurologic physical examination: a proposed model.
J Chiropr Med. 2007;6(4):163–171Mykietiuk C, Wambolt J, Pilipow T, Mallay C, Gleberzon BJ.
Technique systems used by post-1980 graduates of the Canadian Memorial Chiropractic College
practicing in five Canadian provinces: A preliminary survey.
J Can Chiro Assoc. 2009;53(1):32–39
Return to LOCATING SUBLUXATIONS
Since 1-14-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |