

Is It Time To Stop Functional Pre-manipulation
Testing of the Cervical Spine?This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Manual Therapy 2005 (May); 10 (2): 154–158 ~ FULL TEXT
Haymo Thiel, George Rix
Anglo-European College of Chiropractic,
13-15 Parkwood Road,
Bournemouth BH5 2DF, UK.
hthiel@aecc.ac.uk
The combined extended and rotated cervical spine position has been postulated to affect vertebral artery blood flow by primarily causing a narrowing of the vessel lumen, usually within the artery contralateral to the side of head rotation. The production of brainstem symptoms during the manoeuvre has generally been considered to be a positive test result. As a consequence, functional pre-manipulation testing of the cervical spine has been part of clinical screening undertaken by chiropractors and other manual practitioners to rule out the risk of possible injury to the vertebral artery. To date, these testing procedures are taught to students and carried out in daily clinical practice, despite the considerable controversy that exists about their validity.
This paper considers and discusses the usefulness of functional pre-manipulation testing for clinical scenarios, involving dissection, spasm or stenosis of the vertebral artery, and makes the following recommendations:(1) Practitioners must assess the patient thoroughly, through careful history taking and physical examination, for the possibility of vertebral artery dissection. It is important to note that vertebral artery dissection (VAD) may present as pain only, and may not be associated with symptoms and signs of brainstem ischaemia.
(2) If there is a strong likelihood of VAD, provocative pre-manipulation tests should not be performed, and the patient must be referred appropriately.
(3) In the patient presenting with symptoms of brainstem ischaemia due to non-dissection stenotic vertebral artery pathologies, provocative testing is very unlikely to provide any useful additional diagnostic information.
(4) In the patient with unapparent vertebral artery pathology, where spinal manipulative therapy (SMT) is considered as the treatment of choice, provocative testing is very unlikely to provide any useful information in assessing the probability of manipulation induced vertebral artery injury.
From the FULL TEXT Article:
Introduction
Functional pre-manipulation testing of the cervical spine has been part of clinical screening undertaken by practitioners of spinal manipulative therapy (SMT) for many years, and various protocols have been adapted to rule out the risk of possible injury to the vertebral artery (Carey, 1995; Rivett, 1995; Grant, 1996; Barker et al., 2000). Since first reported in the literature in 1927 by DeKleyn and Nieuwenhuyse (DeKleyn and Nieuwenhuyse, 1927), the combined extended and rotated cervical spine position has been postulated to affect vertebral artery blood flow by primarily causing a narrowing of the vessel lumen, usually within the artery contralateral to the side of head rotation. The production of brainstem symptoms during the manoeuvre has generally been considered to be a positive test result. To date, these testing procedures are continued to be taught to students and carried out in daily clinical practice, despite the considerable controversy that exists about their validity (Kunnasmaa and Thiel, 1994; Thiel et al., 1994; Cote et al., 1996; Rivett et al., 1998; Licht et al., 2000; Westaway et al., 2003). This may be partially based on the belief that performance of these screening tests, and a negative result, could offer the practitioner some form of medico-legal or clinical negligence protection, or that these tests may afford, both the practitioner and the patient, a lesser risk of postmanipulation stroke.

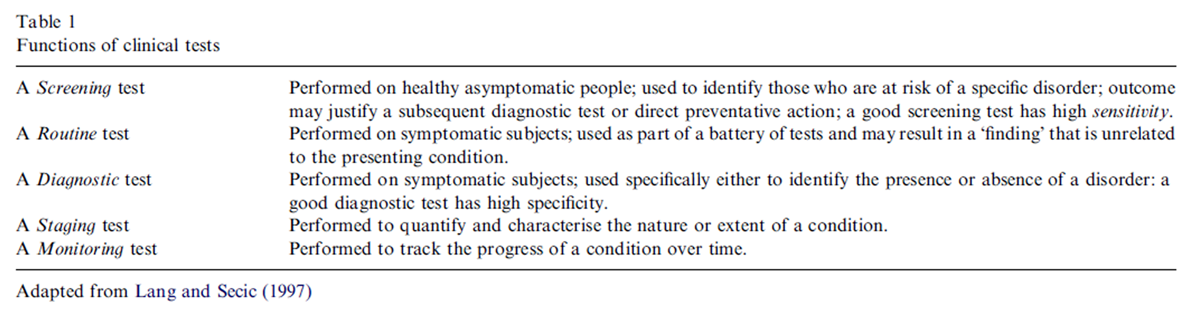
Table 1
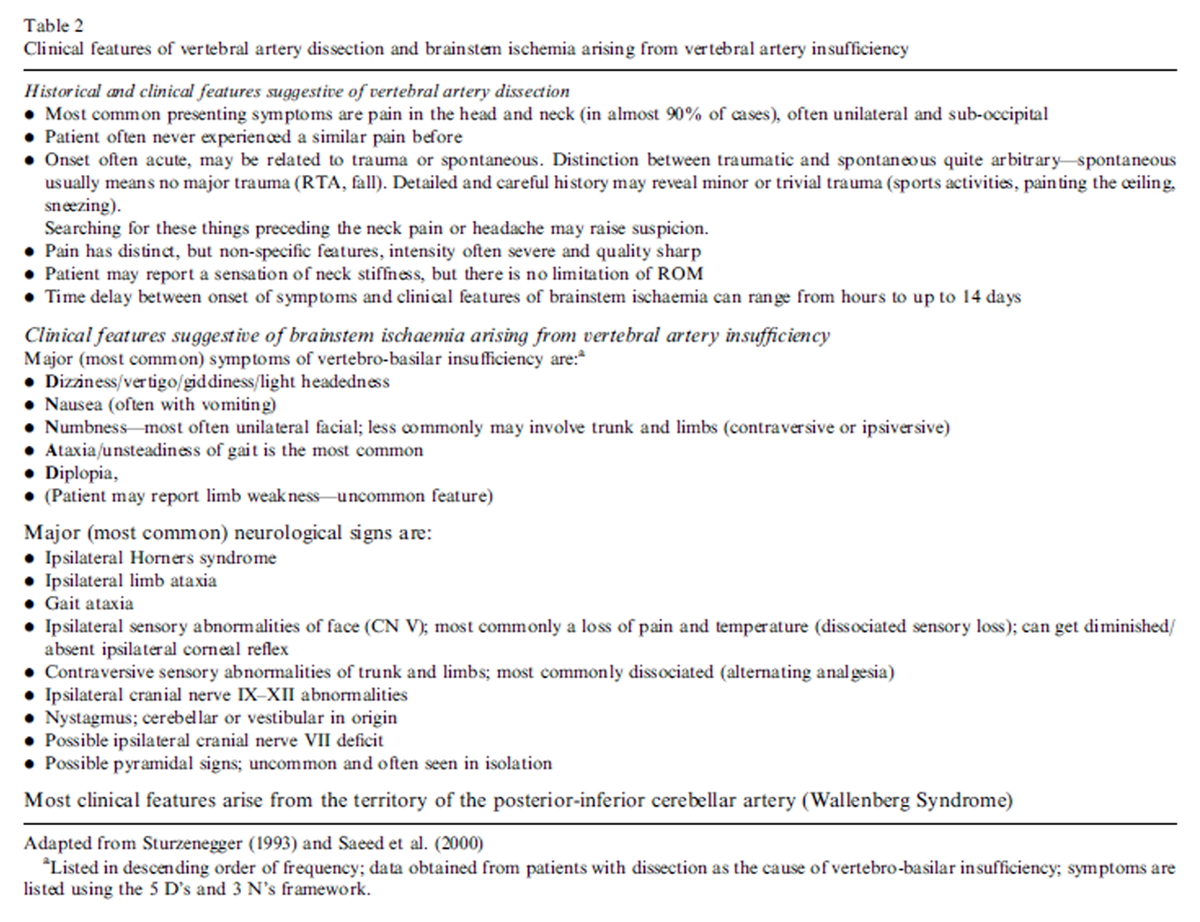
Table 2 Clinical tests may have one or more of five functions (Table 1). Provocative or functional vertebral artery insufficiency tests are most commonly used for diagnostic or screening purposes. This commentary focuses on the role of functional vertebral artery insufficiency testing as a pre-manipulation screening tool. Clinical tests are used to perform a specific function for a specific condition, or risk factors for that condition, in a specific population (Lang and Secic, 1997). In this sense, the provocative or functional vertebral artery insufficiency tests are considered to be a screen for otherwise unapparent vertebral artery pathology that may represent a pre-manipulation risk, in a situation where SMT of the cervical spine is considered to be the treatment of choice. By ‘unapparent’ we mean the absence of historical or other clinical features suggestive of vessel pathology such as dissection, and/or brainstem ischaemia (Table 2). This scenario reflects the clinical situation that practitioners of SMT most commonly face with respect to pre-manipulation screening in their daily practice.
In assessing the usefulness of a screening procedure, a prerequisite must be to define the pre-symptomatic condition that it is aimed at detecting. Although the exact pathophysiological mechanisms underlying stroke and SMT are still unclear, the most commonly accepted one is that of vertebral artery dissection (Frisoni and Anzola, 1991). If this dissection or other sequelae related to vessel wall injury was to be due to a pre-symptomatic congenital or acquired weakness of the vessel wall, it is hard to see how positional tests, aimed at assessing the haemodynamics of that still patent vessel, will afford any useful clinical information regarding the possible risk of injury. Furthermore, in this scenario, performing these tests alone may possibly put the patient at a higher risk due to the potential stretching forces exerted on an already weakened vessel wall. While obviously not in vivo, studies on human cadavers have shown that strain values exerted onto the vertebral artery during a premanipulation test are higher than those observed during a typical cervical SMT procedure (Symons et al., 2002). Although there are no documented cases of dissection following pre-manipulation testing alone, the literature cites many examples of non-manipulation positional manoeuvres of the head and neck that have been associated with cerebrovascular injury (Thiel, 1991; Rosner, 2003).
Vessel spasm is another pathophysiological process that has been hypothesised by some to lead to vertebral artery occlusion following SMT (Easton and Sherman, 1977; Schmitt, 1991). This may occur with or without arterial wall damage. Again, and for the same reason as for dissection, it is hard to see how on biologically plausible grounds, a positional pre-manipulation test could assess for the possibility of an impending vasospasm. In summary, the construct validity of the tests with these pathologies in mind is poor.
A less commonly accepted link between SMT and stroke is embolisation from a pre-existing thrombus formation in the vertebral artery. In the absence of endothelial injury, this pathological process is most commonly associated with atherosclerosis. The atheroma alone may result in an asymptomatic partial stenosis of the arterial lumen. Hypothetically, the addition of a test, which may further occlude the vessel, could result in sufficient alteration in arterial flow characteristics to produce ischaemic brainstem symptoms. On the other hand, it is also conceivable that the test may dislodge the embolus resulting in stroke.
Hypoplasia of the vertebral arteries (p2 mm) has been considered another stenotic factor related to postmanipulation stroke (Mann and Refshauge, 2001). There is no evidence to suggest that a hypoplastic vessel has a greater predisposition to dissection. However, some reports suggest that in the event of vessel injury, a contralateral hypoplastic artery may not be able to provide sufficient collateral circulation to prevent ischaemia and possible infarction (Henderson and Cassidy, 1998; Mann and Refshauge, 2001).
So what is the usefulness of the provocative or functional vertebral artery insufficiency tests in detecting lumenal stenosis due to thrombus or hypoplasia? In attempting to address this question only in vivo Doppler ultrasound studies of vertebral artery flow in human subjects have been reviewed. As mentioned previously, it is generally assumed that pre-manipulation positional manoeuvres measure the degree of lumenal patency, or absence thereof, via the production of transient brain-stem ischaemic symptoms. In other words, the test is believed to be an indirect measure of vertebral artery haemodynamics. However, a review of the literature on vertebral artery flow studies clearly shows conflicting results with regard to the effects of sustained premanipulation positional manoeuvres. Doppler studies attempting to measure the volume, velocity, or resistance to contralateral vertebral artery flow, have inconsistently indicated either a decrease or disappearance in some of these flow parameters (Stevens, 1984, 1991; Refshauge, 1994; Haynes 1995, 1996, 2000, 2002; Licht et al., 1998; Rivett et al., 1999; Yi-Kai et al., 1999; Mitchell, 2003), or an insignificant or no change at all (Weingart and Bischoff, 1992; Thiel et al., 1994; Cote et al., 1996; Lantz et al., 1996; Licht et al., 1999; Zaina et al., 2003) when applying a variety of functional premanipulation tests. Further, there have been reports of patients who had either known vertebral artery hypoplasia or complete lumenal occlusion on neck rotation but did not experience any symptoms during the premanipulation manoeuvres (Bolton et al., 1989; Rivett et al., 1998; Westaway et al., 2003). Of particular interest are the Doppler studies by Licht and his co-workers which seem to indicate that flow velocity in the vertebral artery is neither significantly affected shortly after SMT of the neck in asymptomatic subjects (Licht, 1998), nor in subjects who had tested positive on performing premanipulation tests (Licht et al., 2000).
Even if one accepts that to an extent, the significant disparity of the results of the various studies on vertebral artery flow during functional pre-manipulation testing, is dependent upon a variety of methodological factors, the weight of the evidence seems to strongly suggest that these screening tests lack the necessary sensitivity in order to be valid and dependable predictors of risk. As such, a negative test result cannot determine the safety of cervical SMT. The lack of sensitivity of the pre-manipulation tests as a valid screening procedure is further supported by some of the findings of Haldeman et al. in their review of 64 medicolegal cases of cerebrovascular accidents associated with SMT of the cervical spine (Haldeman et al., 2002). In 27 of the cases, the practitioner had described the use of a pre-manipulation provocative screening manoeuvre, however, none of these patients had shown any adverse responses to this screening test before the manipulation.
In view of these arguments, we would like to make the following observations and recommendations:1. Practitioners must assess the patient thoroughly, through careful history taking and physical examination,for the possibility of vertebral artery dissection. It is important to note that VAD may present as pain only, and may not be associated with symptoms and signs of brainstem ischaemia (Table 2).
2. If there is a strong likelihood of VAD, provocative pre-manipulation tests should not be performed, and the patient must be referred appropriately.
3. In the patient presenting with symptoms of brainstem ischaemia due to non-dissection stenotic vertebral artery pathologies, provocative testing is very unlikely to provide any useful additional diagnostic information.
4. In the patient with unapparent vertebral artery pathology, where SMT is considered as the treatment of choice, provocative testing is very unlikely to provide any useful information in assessing the probability of manipulation induced vertebral artery injury.
5. Practitioners might well now consider whether provocative testing provides any real benefit to any of these patient populations.
REFERENCES:
Barker S, Kesson M, Ashmore J, Turner G, Conway J, Stevens D.
Guidance for pre-manipulative testing of the cervical spine.
Manual Therapy 2000;5:37–40.Bolton P, Stick P, Lord R.
Failure of clinical tests to predict cerebral ischemia before neck manipulation.
Journal of Manipulative and Physiological Therapeutics 1989;12:304–7.Carey P.
A suggested protocol for the examination and treatment of the cervical spine: managing the risk.
Journal of the Canadian Chiropractice Association 1995;39:35–9.Cote P, Kreitz B, Cassidy D, Thiel H.
The validity of the extensionrotation test as a clinical screening procedure
before neck manipulation: a secondary analysis.
Journal of Manipulative and Physiological Therapeutics 1996;19:159–64.DeKleyn A, Nieuwenhuyse P. Schwindelanfaelle und nystagmus beieiner bestimmten stellung des kopfes.
Acta Otolaryngologica 1927;11:155–7.Easton J, Sherman D.
Cervical manipulation and stroke.
Stroke 1977;8:594–7.Frisoni G, Anzola G.
Vertebrobasilar ischemia after neck motion.
Stroke 1991;22:1452–60.Grant R.
Vertebral artery testing—the Australian Physiotherapy Association protocol after 6 years.
Manual Therapy 1996;1: 149–53.Haldeman S, Kohlbeck FJ, McGregor M.
Unpredictability of Cerebrovascular Ischemia Associated with Cervical
Spine Manipulation Therapy: A Review of Sixty-four Cases
After Cervical Spine Manipulation
Spine (Phila Pa 1976) 2002 (Jan 1); 27 (1): 49–55Haynes M.
Cervical rotational effects on vertebral artery flow.
Chiropractice Journal of Australia 1995;25:73–6.Haynes M.
Doppler studies comparing the effects of cervical rotation and lateral flexion
on vertebral artery blood flow.
Journal of Manipulative Physiological Therapeutics 1996;19:378–84.Haynes M.
Vertebral arteries and neck rotation: Doppler velocimeter and duplex results compared.
Ultrasound in Medicine and Biology 2000;26:57–62.Haynes M.
Vertebral arteries and cervical movement: Doppler ultrasound velocimetry
for screening before manipulation.
Journal of Manipulative Physiological Therapeutics 2002;25:556–7.Henderson D, Cassidy D.
Vertebral artery syndrome. Part A: vertebrobasilar vascular accidents
associated with cervical manipulation.
In: Vernon H editor. Upper cervical syndrome.
Baltimore: Williams & Wilkins; 1998. p. 194–206.Kunnasmaa K, Thiel H.
Vertebral artery syndrome: a review of the literature.
Journal of Orthomolecular Medicine 1994;16: 17–20.Lang TA, Secic M.
How to report statistics in medicine.
Philadelphia: American College of Physicians; 1997.Lantz C, Bivius M, Pretorius D.
The effect of extreme head positions on vertebral artery velocity.
Bournemouth, UK: International Conference on Spinal Manipulation; 1996 p 197–19.Licht P.
Vertebral artery flow and spinal manipulation: A randomized, controlled
and observer-blinded study.
Journal of Manipulative Physiological Therapeutics 1998;21:141–3.Licht P, Christensen H, Hoilund-Carlsen P.
Vertebral artery volume flow in human beings.
Journal of Manipulative Physiological Therapeutics 1999;22:363–7.Licht P, Christensen H, Hoilund-Carlsen P.
Is there a role for premanipulative testing before cervical manipulation?
Journal of Manipulative and Physiological Therapeutics 2000;23:175–9.Licht P, Christensen H, Hojgaard P, Hoilund-Carlsen P.
Triplex ultrasound of vertebral artery flow during cervical rotation.
Journal of Manipulative Physiological Therapeutics 1998;21:27–31.Mann T, Refshauge K.
Causes of complications from cervical spine manipulation.
Australian Journal of Physiotherapy 2001;2001:255–66.Mitchell J.
Changes in vertebral artery blood flow following normal rotation of the cervical spine.
Journal of Manipulative Physiological Therapeutics 2003;26:347–51.Refshauge K.
Rotation: a valid premanipulative dizziness test? Does it predict safe manipulation?
Journal of Manipulative Physiological Therapeutics 1994;17:15–9.Rivett D.
The pre-manipulative vertebral artery testing protocol: a brief review.
New Zealand Journal of Physiotherapy 1995: 9–12.Rivett D, Milburn P, Chapple C.
Negative pre-manipulative vertebral artery testing despite complete occlusion: a case of false negativity?
Manual Therapy 1998;3:102–7.Rivett D, Sharples K, Milburn P.
Effect of premanipulative tests on vertebral artery and internal carotid artery blood flow: a pilot study.
Journal of Manipulative Physiological Therapeutics 1999;22:368–75.Rosner A.
Risks of cerebrovascular accidents in perspective.
Manuelle Medizin 2003;41:1–9.Schmitt H.
Anatomical structure of the cervical spine with reference to pathology of manipulation complications.
Manual Medicine 1991;6:93–101.Stevens A.
Doppler sonography and neck rotation.
Journal of Manual Medicine 1984;1:49–53.Stevens A.
Functional Doppler sonography of the vertebral artery and some considerations
about manual techniques.
Journal of Manual Medicine 1991;6:102–5.Symons, B., Leonard, T.R., Herzog, W., 2002.
Internal Forces Sustained by the Vertebral Artery
During Spinal Manipulative Therapy
J Manipulative Physiol Ther 2002 (Oct); 25 (8): 504–510Thiel H.
Gross morphology and pathoanatomy of the vertebral arteries.
Journal of Manipulative Physiological Therapeutics 1991;14:133–41.Thiel H, Wallace K, Donat J, Yong-Hing K. Effect of various head and neck positions on vertebral artery blood flow.
Clinical Biomechanics 1994:105–10.Weingart J, Bischoff H.
Doppler sonography of the vertebral artery with regard to head positions appropriate to manual medicine.
Journal of Manual Medicine 1992;6:62–5.Westaway M, Stratford P, Symons B.
False-negative extension/rotation pre-manipulative screening test on a patient with
an atretic and hypoplastic vertebral artery.
Manual Therapy 2003;8:120–7.Yi-Kai L, Yun-Kun Z, Cai-Mo L, Shi-Zen Z.
Changes and implications of blood flow velocity of the vertebral artery during
rotation and extension of the head.
Journal of Manipulative Physiological Therapies 1999;22:91–5.Zaina C, Grant R, Johnson C, Dansie J, Taylor P, Spyropolous P.
The effect of cervical rotation on blood flow in the contralateral vertebral artery.
Manual Therapy 2003;8: 103–9.
Return to STROKE AND CHIROPRACTIC
Since 6-14-2005
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |