

Effects of Cervical Joint Manipulation
on Joint Position Sense of Normal AdultsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Phys Ther Sci 2013 (Jun); 25 (6): 721–723 ~ FULL TEXT
OPEN ACCESS Wontae Gong
Department of Physical Therapy,
Korea Nazarene University.
[Purpose] The purpose of this study was to identify the effects of cervical joint manipulation on joint position sense (JPS) of normal adults.
[Subjects] Thirty normal adults were divided into a test group of 15 subjects and a control group of 15 subjects.
[Methods] The test group was treated with cervical joint manipulation and massage, whereas the control group received only massage. Both groups were evaluated in terms of joint position error (JPE) using a digital dual clinometer before and after the interventions.
[Results] The comparision of the pre- and post-test results revealed the test group exhibited statistically significant changes in flexion, extension, left lateral flexion, right lateral flexion, left rotation, and right rotation. On the other hand, the control group showed no statistically significant changes in any of the variables.
[Conclusion] Cervical joint manipulation reduced JPE and improved joint position sence. Therefore, we consider its application to the treatment of patients with cervical problems in clinical practice is desirable.
From the Full-Text Article:
INTRODUCTION
Neck pain is a frequent and disabling complaint in the general population, and joint position sense (JPS) is an important function of the human body, recognizing the location of joints, and an essential element in the maintenance of balance or kinesthetic sense). [1] In a previous study, flexion, extension, left lateral flexion (LLF) right lateral flexion (RLF), left rotation (LR), right rotation (RR), and range of motion (ROM) of female office workers with neck pain were measured. That study reported that their neck mobility had declined in all directions and that altered muscle recruitment strategies were employed. Moreover, to help the office workers manage their neck pain, exercise programs including motor re-education were considered necessary). [2]
Therefore, reduction in cervical ROM may decrease JPS and alter muscle recruitment strategy. There are various methods of increasing cervical ROM, but research has demonstrated that spinal manipulative therapy has particularly beneficial effects). [3] In the literature of JPS-related studies, one study reported that conventional proprioceptive training improved JPS). [4] Another identified relations between JPS and dizziness. However, most JPS-related studies have focused on patients with persistent neck pain or whiplash injuries, and JPS was improved JPS through exercises. The present study aimed to identify whether an increase in the ROM of the cervical joint, resulting from manipulation techniques for joint mobility, improved cervical JPS.
SUBJECTS AND METHODS
The study subjects were 30 students attending N University in Chungcheongnam-do, Korea. The subjects were divided into a test group of 15 subjects (1 male and 14 females) and a control group of 15 subjects (1 male and 14 females). The test group was aged 21.9±0.2 years, 163.3±5.8 cm in height, and 55.2±7.0 kg in weight. The control group was aged 21.0±0.3, 162.2±5.9 cm in height, and 53.1±7.5 kg in weight. The two groups showed no statistically significant differences in their general characteristics. Subjects who had undergone surgery, were undergoing hospital treatment, or had a ruptured cervical disk were excluded from this study. All the subjects were given an explanation about the purpose of this study and the entire process of the experiment and submitted their voluntary written consent before participation.
The test group received cervical joint manipulation and massage for 25 minutes in a single session. In the cervical joint manipulation for the rotation correction, the therapist placed his thumb on the posterior articula pilla in the segment intended for rotation, applied rotational pressure against the y-axis in the horizontal plane, and then applied a short and quick thrust at the end range of rotation. For the correction of lateral flexion (LF), the therapist placed his index finger on the exterior of the segment intended for correction, generated LF against the z-axis in the coronal plane, and then applied a short and quick thrust at the end range of LF. To increase the extension ROM, Gong’s mobilization was used). [5]
The sternocleidomastoid, upper trapezius, levator scapulae, and posterior cervical muscles were massaged. After each subject lay supine on a table, the therapist sat down at the side of the subject’s head. The therapist supported the patient’s head with the hand closest to the patient and placed the other hand below the subject’s neck and massaged the posterior cervical muscles along the muscle fibers. Thereafter, the therapist turned the subject’s head in the opposite direction to the intended massaging direction, and then massaged the sternocleidomastoid, upper trapezius, and levator scapulae muscles). [6] The control group received only a single session of massage for 15 minutes.
JPS was evaluated through JPE, with a greater JPE denoting a lower JPS. The JPE was measured using a digital dual clinometer (Dualer IQ, JTECH Medical, U.S.A.). To measure the JPE, the subjects were shown twice how to adopt the exact positions of 35° flexion, 35° extension, 30° LLF, 30° RLF, 45° LR, and 45° RR with passive cervical movements in a neutral position under the measurer’s instructions. Afterward, the subjects had to adopt these six positions using their own active cervical movements without the measurer’s instructions. During the test, the difference between each position’s measured and correct values was recorded. The joint position was measured three times before and after the intervention, and the averages were used for the evaluation.
The experimental results were statistically analyzed using SPSS 12.0 KO (SPSS, Chicago, IL, U.S.A.). After the general characteristics of the subjects were determined, the paired t-test wsa used to compare the changes in the flexion, extension, LLF, RLF, LR, and RR between pre-test and post-test in each group. The differences between the two groups were tested using the independent t-test. The statistical significance level was chosen as α=0.05.

Table 1
Table 2 RESULTS
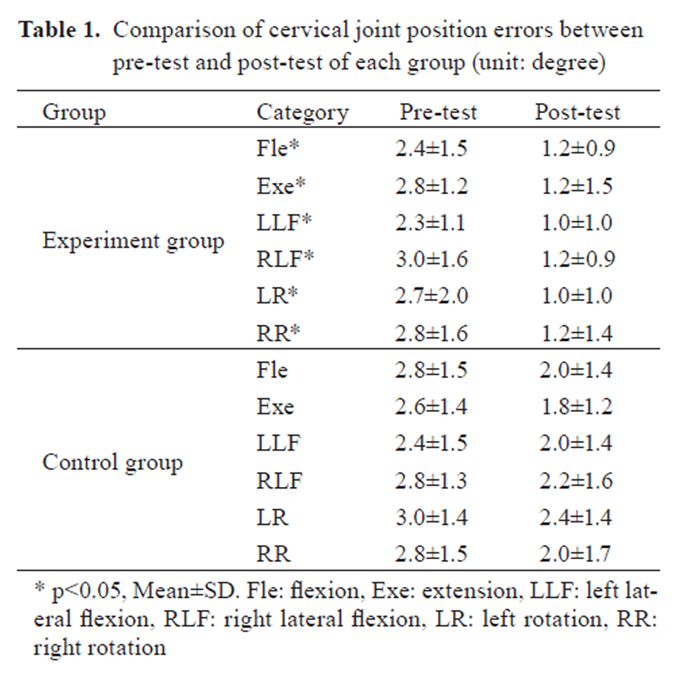
The comparison of the pre- and post-test results of the test group revealed statistically significant differences in flexion, extension, LLF, RLF, LR, and RR (p<0.05). On the other hand, the control group showed no statistical significant differences in any of the variables (p>0.05) (Table 1).
Based on the results of the independent t-test for the two groups before and after the test, only the differences between the pre- and post-test values of LLF and LR were statistically significant (p<0.05). All the other variables showed no statistically significant differences (p>0.05) (Table 2).
DISCUSSION
In a similar study related to cervical functions, Jull et al. reported that cranio-cervical flexion training increased deep cervical flexor electromyographic amplitudes and decreased sternocleidomastoid and anterior scalene electromyographic amplitudes across all stages of cranio-cervical flexion training). [7] In a study related to JPS, Treleaven et al. measured JPE in 102 subjects with dizziness and unsteadiness following whiplash injuries and in 44 normal adults. They reported that compared to normal adults, those with dizziness and unsteadiness following whiplash injuries showed larger declines in JPS. They further noted that cervical mechanoreceptor dysfunction can give rise to dizziness in patients with whiplash injuries). [8]
Jull et al. implemented conventional proprioceptive training and craniocervical flexion training for 64 female subjects with a history of chronic neck pain of either idiopathic (n=39) or traumatic (n=25) origin over a 6-month period. After the training, they measured JPE in cervical extension and rotation. They reported that while both groups exhibited declines in JPE, the proprioceptive training group showed a larger decline. In their study, the degree of JPE decreased from 4–5° before the intervention to 2–3° after the intervention. In the present study, the degree of JPE declined from 2.5–3.0° before the intervention to 1.0–1.2° after the intervention). [4] This difference is likely due to the present study having only included normal subjects.
In this study, the test group was treated with both cervical joint manipulation and massage, and displayed larger declines in JPE than the massage-only control group. Although no previous studies have reported an improvement in JPS through joint manipulation, mobility in the present study was likely to have been generated in each segment through joint mobilization, which, in turn, would have activated the proprioceptors in the joint capsules and deep muscles, eventually leading to improvement in JPS. However, in the comparison of the two group’s of differences between the pre- and post-test values of flexion, extension, LLF, RLF, LR, and RR, only LLF and LR exhibited statistical significance.
This suggests that while increase in cervical ROM leads to reduced JPE and improved JPS, JPE can also be reduced and JPS can be improved through massage. However, the differences between the two treatments were not statistically significant. In other words, while a single session of massage can reduce JPE and improve JPS, the combined treatment of massage and cervical joint manipulation was much more effective at increasing the ROM. Therefore, we recommend that when treating patients with reduced JPS due to decreased ROM, persistent neck pain, or whiplash injuries, the combined application of cervical joint manipulation and massage is used.
References:
Treleaven J, Jull G, LowChoy N:
The relationship of cervical joint position error to balance and eye movement
disturbances in persistent whiplash.
Man Ther, 2006, 11: 99–106Johnston V, Jull G, Souvlis T, et al. :
Neck movement and muscle activity characteristics in female office workers with neck pain.
Spine, 2008, 33: 555–563Terrett AC, Vernon H:
Manipulation and pain tolerance: a controlled study of the effect of
spinal manipulation on paraspinal cutaneous pain tolerance levels.
Am J Phys Med, 1984, 63: 217–225Jull G, Falla D, Treleaven J, et al. :
Retraining cervical joint position sense: the effect of two exercise regimes.
J Orthop Res, 2007, 25: 404–412Gong WT, HwangBo G, Lee YM:
The effects of Gong’s mobilization on cervical lordosis, forward head posture, and cervical ROM
in abnormal posture of the cervical spine of college students.
J Phys Ther Sci, 2011, 23: 531–534 [PMC free article]Clay JH, Pounds DM:
Basic Clinical Massage Therapy: Intergrating anatomy and treatment.
Philadelphia: Lippincott Williams & Wilkins press, 2006, pp 92–110.Jull GA, Falla D, Vicenzino B, et al. :
The effect of therapeutic exercise on activation of the deep cervical flexor muscles
in people with chronic neck pain.
Man Ther, 2009, 14: 696–701Treleaven J, Jull G, Sterling M:
Dizziness and Unsteadiness Following Whiplash Injury: Characteristic Features
and Relationship with Cervical Joint Position Error
J Rehabil Med 2003 (Jan); 35 (1): 36–43
Return to SUBLUXATION
Since 2-07-2021

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |