

Is Chiropractic a CAM Therapy
or is it a Separate Profession?This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2005 (Sep); 49 (3): 133-136 ~ FULL TEXT
OPEN ACCESS Lon Morgan, DC, DABCO
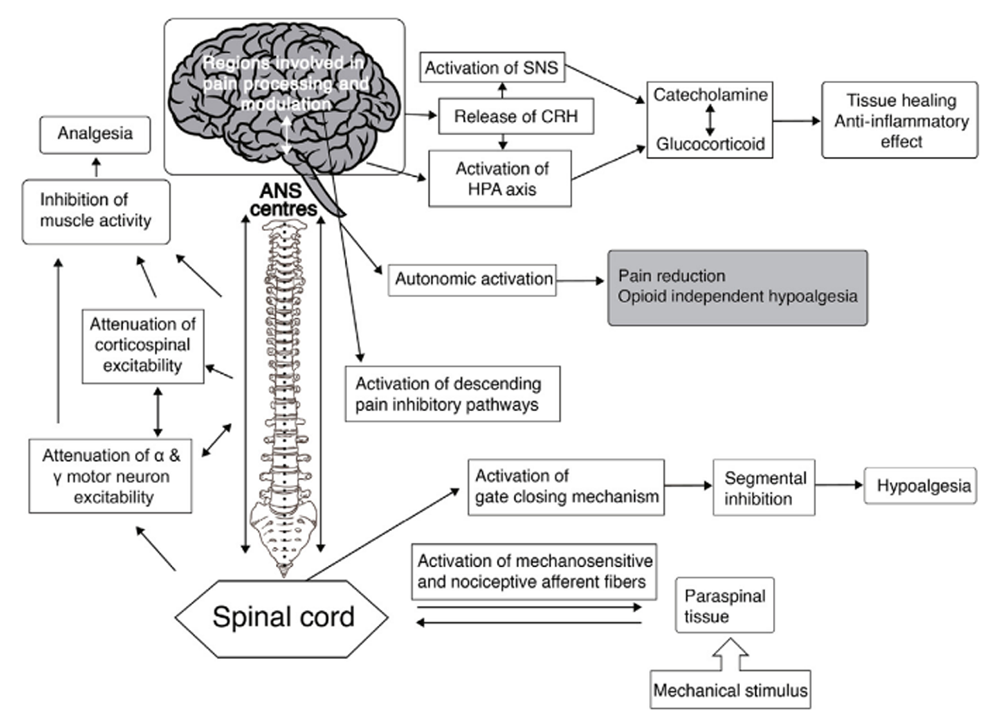
Neurophysiological effects of spinal manipulation
FROM: J Integrative Medicine 2019
As buzzwords go CAM (Complementary or Alternative Medicine) has attracted considerable public attention. CAM is a loose term encompassing a wide range of therapies, basically anything that is not medical regardless of its established merit. One common definition in the U.S. medical literature is “those practices neither taught widely in United States medical schools nor generally available in United States hospitals.” [1] This paper will explore whether chiropractic should be a part of the CAM phenomenon.
From the Full-Text Article:
CAM usage
The origins of CAM are lost in antiquity, being passed down to us from ancient shamans, spiritual healers, witch doctors, and hakeems in the form of rituals, rites, potions, lotions, and ceremonies. Today CAM includes, but is not limited to, treatments as diverse as aromatherapy, prayer, crystal healing, feng shui, homeopathy, radionics, and by some the practice of chiropractic.
CAM popularity is worldwide and growing, and is used for a wide range of human ailments including Inflammatory Bowel Disease (IBD), [2] pediatric care, [3] inflammatory eye disease, [4] haematological malignancies, [5] herbs for rheumatology, [6] nausea in pregnancy, [7] etc. In other words there is really no human ailment that is not treatable in one form or another by some form of CAM. The proven effectiveness of these treatments is, however, decidedly controversial.
Many outside observers: social scientists, epidemiologists, researchers, authors, editors, etc., lump chiropractic in with the rest of the CAM alphabet soup. Many in chiropractic have reveled in the CAM identity despite the fact most CAM approaches conflict with chiropractic “philosophy”. To much of the outside world there is little perceived difference between naturopaths, homeopaths, aroma therapists, herbalists, energy healers, crystal channelers, and chiropractors. The ready willingness of many chiropractors to identify with CAM adds to this perception. Most of these CAM approaches are incompatible with each other, have conflicting notions of the causes of disease, and differ radically on how to treat a patient. These marked differences in CAM philosophical and treatment approaches are rarely given consideration. Each camp, however, has their enthusiastic devotees proclaiming the superiority of their particular approach. The only real commonality these groups are apt to share is an “Us vs. Them” (CAM vs. medicine) mentality.
This leads to the candid observation that despite recent attempts to better research CAM the results to date are at best equivocal and narrowly applicable. If there is one description that can be applied to CAM practitioners in general it is that they are often poorly credentialed, poorly educated, their methodologies poorly researched, their claims riddled with observer bias, and they have a poor understanding of scientific methodology in general. In addition, CAM practitioners are often loath to consider placebo effects or the natural course of disease in their claims, or to admit possible adverse side effects of their treatments. This is not to say CAM might not have effective uses, but how is one to know?
We have in effect attempted to have the best of both worlds with one foot in CAM and one toe dabbling in health science. This schizophrenic approach to a chiropractic identity serves no one. In most areas anyone can simply hang out a shingle and claim to be CAM provider. All it takes to be a homeopath, a naturopath, a psychic healer, or an aroma therapist requires nothing more than a sign in the window. Does it benefit chiropractic’s claim to legitimacy to be identified with this crowd? Is association with the CAM movement really in the best interests of chiropractic?
The downside of CAM for chiropractic
David M Eisenberg, MD of the Harvard Medical School has extensively researched the CAM phenomenon in a number of published articles. In a 1998 JAMA study Eisenberg noted the increased popularity of CAM in general in the U.S. While chiropractic was noted as the largest CAM supplier many other CAM groups had shown substantial increases in usage. Of particular interest is that in 1997 chiropractic’s share of the market (11%) remained largely stagnant compared to an earlier 1990 survey (10.1%). By contrast herbal remedies, herbal medicine, massage, spiritual healing, and other forms of CAM experienced substantial increases. [8]
From its 1997 peak chiropractic utilization has changed for the worse in recent years. The most recent 2005 survey by Eisenberg et al shows changes important to chiropractors. Eisenberg notes:“The greatest relative increase in CAM use between 1997 and 2002 was seen for herbal medicine (12.1% vs.18.6%, respectively), and yoga (3.7% vs. 5.1%, respectively), while the largest relative decrease occurred for chiropractic (9.9% to 7.4%, respectively).” [9] (Emp. added)
Chiropractic success in the U.S. in prior decades was built largely on enhanced insurance coverage. This trend has now reversed with very substantial cutbacks in insurance coverage of chiropractic services. Chiropractic is now largely excluded from Worker’s Compensation claims. Private insurance companies have raised deductibles and copays and installed medical doctor gatekeepers and payment caps. Medicare coverage for the elderly severely limits chiropractic participation in that program. The net result of these actions has been a substantial decline in average individual chiropractic income. Canada has also experienced a similar adverse event with the recent delisting of chiropractic services in the province of Ontario.
If the writing is not on the wall it is at least apparent in the data. While it is more difficult to obtain reliable chiropractic income information a survey conducted by the ACA noted a decline in net chiropractic income from $101,000 in 1989 to $86,000 in 1997, a dramatic 15% drop in income. [10] This in stark contrast with medical incomes which continue to rise substantially. [11] Possibly related to declining chiropractic prosperity has been a marked decline in chiropractic college enrollment in the U.S.:
According to data published by the National Center for Education Statistics, fall enrollments for sixteen U.S. chiropractic programs fell 39.9% from 16,500 in 1996 to 9,921 in 2002. [12]
At this point one has to wonder whether chiropractic, under the CAM umbrella, has passed its peak.
Foundering on founding myths
In the founding myths of Roman mythology Mars, the God of War, sires the twins Romulus and Remus. By some accounts the twins were nursed by a wolf under a fig tree, and upon reaching adulthood founded the ancient city of Rome.
Chiropractic’s involvement with CAM is fostered by its own founding myths: i.e., that an entity known as “subluxation” exists which blocks another myth, “innate”, from flowing, which in turns causes another myth, human “disease”, to occur. After 110 years of attempting to promulgate these myths chiropractic has utterly failed to convince leading authorities and institutions of the legitimacy of these “philosophical” notions. This should not come as a surprise. In a 1998 article I questioned the validity of so-called “Innate Intelligence”, referring to it as “... an untestable enigma that isolates chiropractic and impedes its acceptance as a legitimate health science.” [13] Events in the interim have only served to confirm that assessment.
Even worse, chiropractic’s fixation on the mythical “subluxation” has eroded a massive professional sinkhole. Consider this: we claim “subluxation” to be an articular phenomenon that may/may not be clinically significant, may/may not be palpable, may/may not be visible on x-ray, may/may not cause disease and may/may not be correctable by a near infinite number of hopelessly conflicting treatment theories. Nelson accurately describes “subluxation” as “... a concept so amorphous and ambiguous as to be unintelligible.” [14]
A concept as ambiguous as “subluxation” means anyone can make it up as they go along. It can be squeezed to fit any patient assessment or treatment approach however bizarre. Anything this vague, anything that can be all things to all people, is ultimately nothing to anyone.
Considering a new path
Benjamin Franklin defined Insanity as “continuing to do the same things over and over and expecting a different result.” We can now say, based on results, what does not work and what would be insane to continue doing. What does not work is aligning with CAM and continuing to cling to an archaic “philosophy” that isolates us from the core health delivery system in North America. Our founding myths keep us sidelined to the point where we are considered in many circles no longer even complementary, more optional, if that. If chiropractic is to be guaranteed any kind of long-term, viable position in future health care delivery systems it will come only after some major reassessments on our part. These reassessments must include tough and troublesome decisions as to what must be excluded in order to obtain this position.
The osteopathic example
It is important to recognize that chiropractic does have other choices. It is another one of chiropractic’s myths that osteopathy was “swallowed up” by medicine and no longer exists as a separate profession. It is rather humorous that no one has informed the osteopaths of this development. In their view they are doing just fine, thank you very much. The number of osteopathic schools has grown to twenty with three new ones recently added. Osteopaths can specialize in every recognized area of medicine, from pediatrics to neurosurgery. In the process they retain their own degree (D.O.) and identity. Along the way osteopathy had the intelligence to modify their misguided “rule of the artery” notion to recognize the multi-component nature of health care which can include spinal manipulation. In so doing osteopaths are prospering under their own identity, have hospital privileges and community respect and acceptance. One measure of osteopathy’s success is the U.S. government’s guaranteed student loan default rate: as of July, 2005 a total of only 28 osteopathic students were in default, versus 712 chiropractic students. [15]
A chiropractic course
If osteopaths are capable of changing course chiropractors can do the same. We must decide: how addicted to our insanity do we wish to be? Any decision to kick our insanity habit means giving up the chiropractic version of Methamphetamine: our addiction to pseudo-“philosophy” and all that goes with it. Doing so will leave some chiropractors with the feeling they have nothing left to live for. There is a false perception among some that holding to our “principles” is all that separates us from physical therapists. Some will feel vulnerable, that not having the innate/subluxation crutch to lean on will remove their raison d’ętre, their reason for being. To which one must simply ask:
What does it say about the chiropractic profession if it
must cling to unverifiable myths to justify its existence?
In a most remarkable recent paper authors Craig Nelson, Dana Lawrence, John Triano and others have set out a path of core values for chiropractic, a professional model that would encompass the following:
Spinal care as the defining clinical purpose of chiropractic.
Chiropractic as a portal-of-entry provider.
The acceptance and promotion of Evidence Based Health Care (EBHC).
A conservative clinical approach. Chiropractic as an integrated part of the healthcare mainstream.
The rigorous implementation of accepted standards of professional ethics. [16]
This model eschews any association with CAM, or with classical “philosophical” notions of “subluxation” and “innate”, or with medical antagonism. It would take chiropractic out of the realm of a pseudo-theology. Chiropractic would no longer promote untenable “Big Ideas”, practice building tactics, and “techniques du jour” of dubious integrity.
Whatever the future course of CAM, whether portions of it gain more credibility or whether it languishes as a passing fad, is largely irrelevant to chiropractic. The bottom line is we are not prospering under the CAM label and thus should have no further association with it. The challenge for chiropractic is to exhibit the foresight, the professional integrity, and the courage, to do what is necessary.
Chiropractic must give up its “rule of the nerve” and embrace evidence based health care in its entirety. It must do so as a profession separate from CAM and simultaneously seek alignment with established health care systems. Chiropractic must face the challenge of defining a credible role for itself devoid of “philosophical” trappings. Such a course will not be easy, but it provides the only option for re-inventing chiropractic as a credible, viable, sustainable, and separate profession.
References:
Flaherty J, Takahashi R.
The use of complementary and alternative medical therapies
among older persons around the world.
Clin Geriatr Med. 2004;20(2):179–200Hilsden R, Verhoef M, Best A, Pocobelli G.
Complementary and alternative medicine use by Canadian patients
with inflammatory bowel disease: results from a national survey.
Am J Gastroenterol. 2003;98(7):1563–1568Moher D, Soeken K, Sampson M, Ben-Porat L, Berman B.
Assessing the quality of reports of randomized trials
in pediatric complementary and alternative medicine.
BMC Pediatr. 2002;2(1):2Smith J, Spurrier N, Martin J, Rosenbaum J.
Prevalent use of complementary and alternative medicine
by patients with inflammatory eye disease.
Ocul Immunol Inflamm. 2004;12(3):203–214Molassiotis A, et al.
Complementary and alternative medicine use in patients
with haematological malignancies in Europe.
Complement Ther Clin Prac. 2005;11(2):105–110Setty A, Sigal L.
Herbal medications commonly used in the practice of rheumatology:
mechanisms of action, efficacy, and side effects.
Semin Arthritis Rheum. 2005;34(6):773–784Hollyer T, Boon H, Georgousis A, Smith M, Einarson A.
The use of CAM by women suffering from nausea and vomiting during pregnancy.
BMC Complement Altern Med. 2002;2(1):5Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Tindle H, Davis R, Phillips R, Eisenberg D.
Trends in use of complementary and alternative medicine by US adults: 1997–2002.
Altern Ther Health Med. 2005;11(1):42–49http://www.chiroweb.com/archives/17/12/01.html
http://www.deltamedcon.com/MHC/
http://www.chiroweb.com/archives/17/12/01.html
Morgan L.
Innate Intelligence: its origins and problems.
J Can Chiropr Assoc. 1998;42(1):35–41Nelson C.
The subluxation question.
Chiropractic Humanities. 7:46–55http://www.defaulteddocs.dhhs.gov/discipline.asp
Nelson, C., Lawrence, D., Triano, J., Bronfort, G., Perle, S., Metz, R. D., et al.
Chiropractic As Spine Care: A Model For The Profession
Chiropractic & Osteopathy 2005 (Jul 6); 13: 9
Return to THE NAYSAYERS CORNER
Since 4-24-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |