

Long-Term Trends in the Use of Complementary
and Alternative Medical Therapies
in the United StatesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Annals of Internal Medicine 2001 (Aug 21); 135 (4): 262–268 ~ FULL TEXT
You may also enjoy this Dynamic Chiropractic extended review of this article
Ronald C. Kessler, PhD; Roger B. Davis, ScD; David F. Foster, MD;
Maria I. Van Rompay, BA; Ellen E. Walters, MS; Sonja A. Wilkey, BA;
Ted J. Kaptchuk, OMD; and David M. Eisenberg, MDBACKGROUND: Although recent research has shown that many people in the United States use complementary and alternative medical (CAM) therapies, little is known about time trends in use.
OBJECTIVE: To present data on time trends in CAM therapy use in the United States over the past half-century.
DESIGN: Nationally representative telephone survey of 2055 respondents that obtained information on current use, lifetime use, and age at first use for 20 CAM therapies.
SETTING: The 48 contiguous U.S. states.
PARTICIPANTS: Household residents 18 years of age and older.
MEASUREMENT: Retrospective self-reports of age at first use for each of 20 CAM therapies.
RESULTS: Previously reported analyses of these data showed that more than one third of the U.S. population was currently using CAM therapy in the year of the interview (1997). Subsequent analyses of lifetime use and age at onset showed that 67.6% of respondents had used at least one CAM therapy in their lifetime. Lifetime use steadily increased with age across three age cohorts: Approximately 3 of every 10 respondents in the pre–baby boom cohort, 5 of 10 in the baby boom cohort, and 7 of 10 in the post–baby boom cohort reported using some type of CAM therapy by age 33 years. Of respondents who ever used a CAM therapy, nearly half continued to use many years later. A wide range of individual CAM therapies increased in use over time, and the growth was similar across all major sociodemographic sectors of the study sample.
CONCLUSIONS: Use of CAM therapies by a large proportion of the study sample is the result of a secular trend that began at least a half century ago. This trend suggests a continuing demand for CAM therapies that will affect health care delivery for the foreseeable future.
From the FULL TEXT Article:
Background
Community surveys done over the past decade have documented that a substantial proportion of Americans use complementary and alternative medical (CAM) therapies [1-4], which have been defined as “interventions neither taught widely in medical schools nor generally available in U.S. hospitals”. [1] Many managed care organizations have responded to this evidence by providing insurance coverage for some CAM therapies. [5] Furthermore, most U.S. medical schools have begun offering courses on CAM therapies. [6]
These responses imply that CAM therapies are perceived to be a force to be reckoned with for some time to come. Yet, little is known about the likelihood that this will be the case. The prevailing assumption is that CAM therapies were used by a fairly narrow segment of the population until the 1970s, at which time the ideology associated with the youth counterculture led to a rapid dissemination and use of CAM therapies that has persisted through the present. [7] However, lack of rigorous trend data from epidemiologic surveys have precluded evaluating this assumption rigorously or projecting the future growth of CAM therapies on the basis of evidence of past trends.
In the current report, we present nationally representative trend data of this sort from a prevalence study. The data came from retrospective self-reports of a nationally representative sample of the U.S. general population in a 1997–1998 telephone survey [4] about age at first use of 20 representative CAM therapies. In our analysis, we studied trends by examining betweencohort differences in rates of initiation of CAM therapy use. [8] In the absence of prospective data, which do not exist, our results represent, to our knowledge, the most accurate information currently available on U.S. trends in CAM therapy use over the past half-century.
METHODS
Sample
The telephone survey was conducted between November 1997 and February 1998 in a nationally representative household sample. Random-digit dialing was used to select households, and a random-selection method was used to select one respondent 18 years of age or older for interview in each sample household. Eligibility was limited to English speakers without cognitive or physical impairment that would prevent interview completion. The average administration time was 30 minutes. A $20 financial incentive for participation was offered. The Beth Israel Deaconess Committee on Clinical Investigations, Boston, Massachusetts, approved the survey methods.
Of the initial sample of 9750 telephone numbers, 26% did not work, 17% were not assigned to households, and 9% were unavailable despite six attempted follow-up contacts. Of the remaining households, 481 were ineligible because of language barrier or cognitive or physical incapacity. Of the 4,167 total eligible respondents, 1,720 (41.3%) completed the interview on initial request. Of a random subsample of 1066 persons who initially declined and were offered an increased stipend ($50), 335 agreed to participate. In all, 2,055 interviews were completed. After we extrapolated the conversion rate to all persons who had initially declined and weighted the data for the undersampling of those who participated after initially declining, the weighted overall response rate among eligible respondents was 60%.
The data were weighted for three factors: 1) probability of selection within household as well as geographic variation in cooperation (by region of the country and urbanicity [local population density]), 2) nonresponse, and 3) post-stratification for aggregate discrepancies between the sample distributions and Census population distributions on a variety of sociodemographic variables. [9, 10] More details on the sample design have been presented elsewhere. [4] Age data were missing for 6 respondents; our analyses are limited to the remaining 2,049 respondents.
Measures
The interview was described to respondents as a survey by investigators from Harvard Medical School about the health care practices of Americans. Interviewers made no mention of CAM therapies. The first substantive questions concerned perceived health, functional impairment due to health problems, interactions with physicians, and history of chronic medical conditions. Interviewers then queried respondents about their lifetime and recent use of 20 CAM therapies—acupuncture, aromatherapy, biofeedback, chiropractic care, commercial diet programs, energy healing (for example, laying on of hands), folk remedy, herbal medicine, homeopathy, hypnosis, imagery, lifestyle diet (such as vegetarianism or macrobiotics), massage, megavitamin therapy, naturopathy, osteopathy, relaxation techniques, self-help group, spiritual healing by others, and yoga. Users of each therapy were asked their age at first use as well as details about the conditions for which the therapy was initiated. The final set of questions dealt with sociodemographic issues.
Cohorts were aggregated into three subsamples: prebaby boom (respondents $54 years of age at interview, born before 1945); baby boom (34 to 53 years of age at interview, born 1945–1964); and post– baby boom (18 to 33 years of age at interview, born 1965–1979). For sociodemographic variables, we used two categories for sex (male or female), four for race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, or other), four for education (less than high school, high school graduate, some college, or college graduate), four for U.S. region (northeast, midwest, south, or west), and four for urbanicity (residence in a large city, small city, suburb, town/rural).
Statistical Analysis
All analyses were performed with weighted data by using SAS statistical software. [11] To assess differences in trends among cohorts, the Kaplan–Meier [12] method was used to generate a graphic representation of the cumulative lifetime prevalences of CAM therapy use according to cohort. The significance of historical changes in lifetime use was estimated by using discretetime survival analysis [13], a method of survival analysis appropriate for data in which events are recorded only at discrete time points (for example, in yearly increments). Discrete-time survival analysis was operationalized as a logistic regression with person-year as the unit of analysis and first use of CAM therapy as the outcome variable. The predictors of primary interest were a series of dummy variables for decades of historical time, and covariates included sociodemographic and dummy variables adjusted for the baseline hazard rate of each year of a person’s life. This model results in an intercept for each time period, and the odds ratios (ORs) can be interpreted as the relative risk for the annual risk for use of alternative therapy. Subsample models were estimated to study sociodemographic variation in trends. Disaggregated models were estimated to study trends in the use of particular CAM therapies.
To adjust for the design effects introduced by weighting of the data, the method of jackknife repeated replications [14] was used to estimate standard errors (SEs). For this method, we used user-written macros in SAS statistical software. For this process, 50 random primary sampling units were created with two random half-samples in each unit for a total of 100 random replicates. Jackknife repeated replication is a method that uses simulations of coefficient distributions in subsamples to generate empirical estimates of SEs and significance tests. The ratios of the coefficients to these adjusted SEs are used to compute the 95% CIs of the ORs. Tests for the significance of sets of predictors taken together were computed by using the Wald chisquare test from coefficient variance– covariance matrices based on the jackknife repeated replications simulations.
RESULTS
Differences in Aggregate Use Trends among Cohorts

Figure 1 At the time of interview, 67.6% of all respondents had used at least one CAM therapy at some time in their lives. Figure 1 presents Kaplan–Meier age-of-onset curves showing trends in each cohort in the cumulative probabilities of use according to age. Of note are the dramatic differences in use among cohorts. This is seen most clearly by focusing on cumulative probabilities of use for age 33 years, the oldest age represented in all three cohorts. Approximately 3 of every 10 respondents in the pre– baby boom cohort used some type of CAM therapy by the age of 33 years compared with 5 of 10 in the baby boom cohort and 7 of 10 in the post– baby boom cohort.
Historical Trends in Aggregate Use

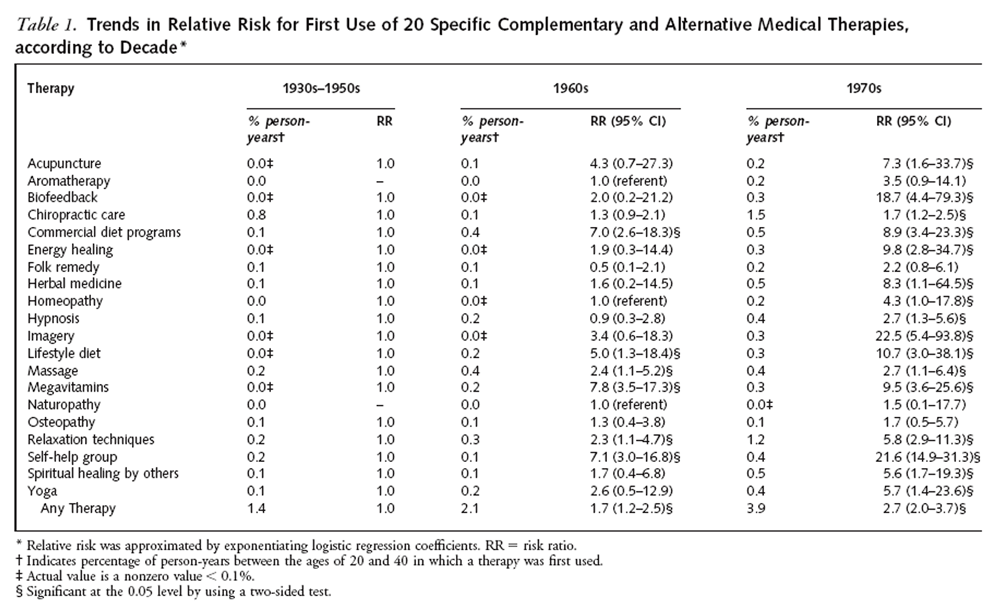
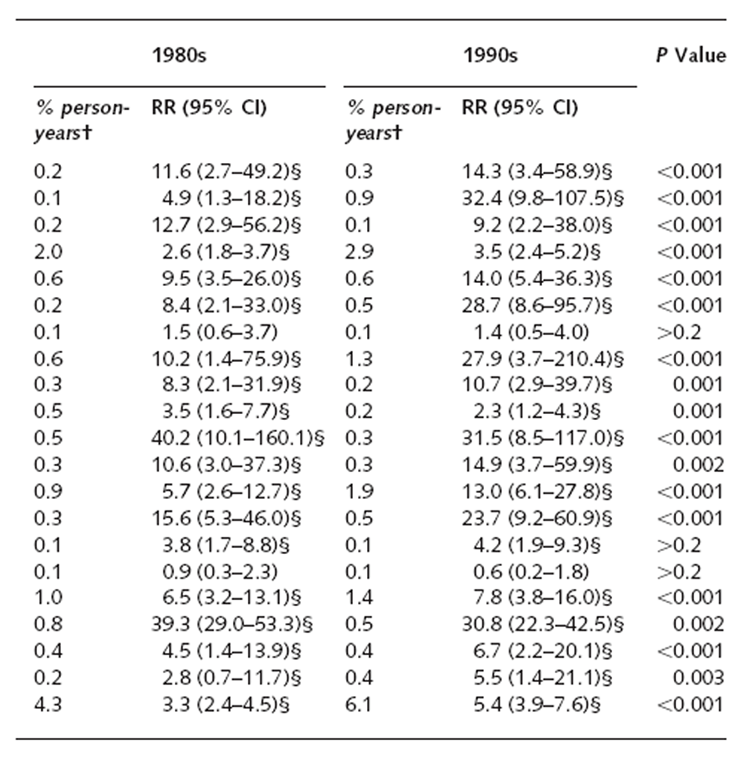
Table 1A
Table 1B The aggregate data in the Figure are presented in a different format in the bottom row of Table 1, where the risk ratios are shown from a discrete-time survival model that estimated the effects of historical time in predicting age at first use of CAM therapy among respondents after adjustment for person-year and sociodemographic variables. The contrast category is first use before 1960. Consistent with the pattern in the Figure, the results of the model for the outcome of any therapy show monotonically increasing risk ratios in each decade from the 1960s through the 1990s.
Possible demographic subsample differences in time trends were examined by estimating separate subsample models that were identical to the discrete-time survival model for any therapy and by evaluating the statistical significance of differences in trends across subsamples. No statistically significant (0.05 level in two-sided tests) differences in trends were found for sex, race/ethnicity, education level, region of the country, or urbanicity.
Trends in the Use of Specific Therapies
Table 1 also shows the risk ratios to estimate first use of each of the 20 CAM therapies assessed. All trends are statistically significant except for those for folk remedy, naturopathy, and osteopathy; thus, in the United States over the past half-century, use of most kinds of CAM therapy has grown.
The data in Table 1 can be transformed to yield information on changes over historical periods of time rather than across cohorts. Data resulting from this transformation (results not shown) yield interesting insights into variations in the timing of societal adoption of the different therapies. Use of all but 4 of the therapies increased in the 1960s compared with pre-1960, and the increase was with a risk ratio of 2.0 or greater for 11 of these therapies. In the 1960s, growth in the use of 4 therapies increased markedly—commercial diet programs, lifestyle diet therapy, megavitamin therapy, and self-help groups. Increased use of all 4 of these therapies is consistent with the largely increased national interest that was seen at that time in fitness and health as a result of a fitness campaign initiated by President Kennedy in the early 1960s. [15]
Our analysis also shows markedly increased growth in the use of alternative therapies in the 1970s as well; use of all the therapies increased in this decade compared with use in the 1960s, and this increase was substantial for 4 of the therapies (biofeedback, energy healing, herbal medicine, and imagery). In addition, 8 of the 20 assessed therapies had their largest rate of growth during the transition from the 1960s to the 1970s (biofeedback, energy healing, folk remedy, herbal medicine, homeopathy, hypnosis, imagery, and spiritual healing by others).
The 1980s saw more modest growth in the use of CAM therapies. Use of 14 of the therapies increased compared with the 1970s, but only 2 (massage and naturopathy) had risk ratios that were markedly greater than in the 1970s. Only yoga became significantly less popular over this time period. Overall, a modest level of growth continued in the 1990s, with 16 therapies having increased use compared with the 1980s, but only 5 of these had markedly greater risk ratios than in the 1980s (aromatherapy, energy healing, herbal medicine, massage, and yoga). Aromatherapy had the most dramatic growth during this period. Although the risk ratios for use of some of the therapies during the 1990s were lower than in the 1980s, none of these declines was statistically significant.
Next, we examined the hypothesis that observed differences in trends among cohorts were primarily due to increased use of selected CAM therapies considered mainstream (as opposed to alternative). To test this hypothesis, we repeated our cohort analyses by fitting the Kaplan-Meier age-of-onset curves to two additional definitions of alternative therapy that excluded possibly mainstream therapies. The intermediate definition excluded biofeedback, commercial diet programs, hypnosis, lifestyle diet, massage, osteopathy, and relaxation techniques from the definitions used in this report; the narrow definition also excluded imagery and megavitamin therapy. The differences in trends between cohorts remained significant (P , 0.001) for all definitions.
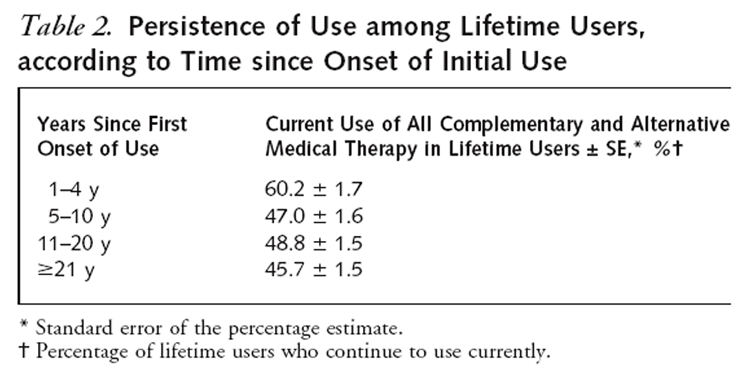
Persistence of Use
Table 2 Table 2 presents data on the percentage of therapies used in the past 12 months by lifetime users, who were classified according to the number of years since first use. The unit of analysis for this table is persontherapies. Of the 2,049 survey respondents, 1,386 reported lifetime use of at least 1 CAM therapy, with an average of 3.03 therapies used by users, for a total of 4,199 person-therapies. Continued use of a specific therapy in the 12 months before the interview was 47% among therapies begun 5 to 10 years before the interview, 48.8% for therapies begun 11 to 20 years previously, and 45.7% for therapies begun more than 20 years earlier. The lack of significant difference among prevalence rates suggests that slightly fewer than half of lifetime users continued to use CAM therapies in any given year throughout their life course.
DISCUSSION
The results reported here suggest that the lifetime prevalence of CAM therapy use in the United States has increased steadily since the 1950s. This increase appears not to be concentrated in a single population sector or decade. Furthermore, the trend is seen for several therapies, although variation can be seen in the timing of the introduction of different therapies between the 1960s and 1990s. We also found powerful cohort effects that are substantial and consistent across cohorts. The post– baby boom respondents had a higher rate of lifetime use by age 33 years than the pre– baby boom respondents had by age 79 years.
These consistent and pervasive results should dispel any suggestion [16] that use has increased for only singular complementary or alternative modalities or that the use of CAM therapies is a passing fad associated with one particular generation or fringe segment of the population. On the basis of the plausible assumption that demand for CAM therapies, similar to that for conventional health care, is sensitive to how much patients must pay out of pocket [17], it seems likely that the proportion of people using CAM therapies will increase as insurance coverage for these treatments expands in the future.
Although limitations in our data do not allow examination of persistence of use over time, we found that 50% of all CAM therapy use that had been initiated at least 5 years before the interview had persisted at the time of the interview. This finding is consistent with the finding of a previous report [18] that most CAM therapies are used, at least in part, to prevent future illness or to maintain health and vitality as part of lifestyle choices linked to the perceived value of disease prevention and health promotion. It seems reasonable to assume that individuals’ interest in prevention will probably persist throughout their lifetime, and this factor may help explain the high rate of persistent use documented in Table 2.
Our results are limited by the restriction of the sampling frame to people who spoke English and who lived in households with telephones, as well as by the relatively low response rate (60%) and the use of a financial incentive. [4] Furthermore, we have no data on the accuracy of self-reports on recollection of lifetime use or age at first use of a therapy. Recall bias is a possibility, and the degree of bias might be related to respondent age. Although we could not correct for these limitations, such adjustments might have made the estimated trends less pronounced.
A second potential confounding element of this study is the constant flux in the labels for and the very existence of particular CAM therapies. These may not necessarily have remained stable throughout the examined periods. For example, some unconventional medical professions, such as “drugless practitioners” and “sanipractors,” which were licensed in some states in the 1930s, have since disappeared. [19]
Our finding of a pervasive increase in the use of 20 CAM therapies over the past half-century warrants reflection on these trends in a historical context. History does not work statistically, and the role of chance makes prediction even more difficult. Specific historic events (such as the invention of the polio vaccination or the discovery of a link between acupuncture and endorphins) and general secular trends (such as confidence in medical progress) are all likely to influence the use or abandonment of CAM therapies. In the future, episodes of conventional or CAM practices associated with dramatic positive developments or adverse events may tip prevalence patterns in one direction or another. Also, from a historical perspective, our data may not represent a consistent trend of increased use of CAM therapies but rather a distinct peak in a longer trend of constant fluctuation in CAM therapy use. For example, survey data from the 1920s and 1930s have revealed high rates of unconventional therapy use [20], and government statistics from 1900 document large numbers of registered unconventional practitioners. [21] Our data may, in fact, be demonstrating a resurgence in CAM use after a period of diminished use during the 1940s and 1950s.
The trend of increased CAM therapy use across all cohorts since 1950, coupled with the strong persistence of use, suggests a continuing increased demand for CAM therapies that will affect all facets of health care delivery over the next 25 years. Evaluations of efficacy and effectiveness by medical researchers and treating physicians’ discussions with patients hold the promise of minimizing adverse effects and maximizing the usefulness of those CAM therapies that prove effective.
Acknowledgment:
The authors thank the staff of DataStat, Inc., Ann Arbor, Michigan, for assistance with telephone data collection.
Grant Support:
In part by the National Institutes of Health (grants U24 AR43441 and K05 MH00507), the John E. Fetzer Institute, the American Society of Actuaries, the Friends of Beth Israel Deaconess Medical Center, the Kenneth J. Germeshausen Foundation, and the J.E. and Z.B. Butler Foundation.
References:
Eisenberg DM, Kessler RC, Foster C, Morlock FE, Calkins DR, Delbanco TL.
Unconventional Medicine in the United States: Prevalence, Costs, and Patterns of Use
New England Journal of Medicine 1993 (Jan 28); 328 (4): 246–252Paramore LC.
Use of alternative therapies: estimates from the 1994 Robert Wood Johnson Foundation National Access to Care Survey.
J Pain Symptom Manage. 1997;13:83-9Druss BG, Rosenheck RA.
Association between use of unconventional therapies and conventional medical services.
JAMA. 1999;282:651-6Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Pelletier KR, Marie A, Krasner M. et al.
Current Trends in the Integration and Reimbursement of Complementary and
Alternative Medicine by Managed Care, Insurance Carriers, and Hospital Providers
Am J Health Promot 1997 (Nov); 12 (2): 112–122Wetzel MS, Eisenberg DM, Kaptchuk TJ.
Courses Involving Complementary and Alternative Medicine at US Medical Schools
JAMA 1998 (Sep 2); 280 (9): 784-787Berliner HS, Salmon JW.
The holistic alternative to scientific medicine: history and analysis.
Int J Health Serv. 1980;10:133-47Shyrock HS, Siegel JS.
The Methods and Materials of Demography. vols. 1, 2.
Washington, DC: U.S. Bureau of the Census; 1971.Holt D, Smith TM.
Post stratification.
Journal of the Royal Statistical Society. 1979;142(Series A):33-46.U.S. Bureau of the Census.
United States Population Estimates, by Age, Sex, Race, and Hispanic Origin, 1990 to 1997.
Available at
www.census.gov/population/estimates/nation/intfile2-1.txt
Accessed 10 June 2001.SAS Institute.
SAS Users Guide, Release 6.12.
Cary, NC: SAS Institute; 1996.Clayton D, Hills M.
Statistical Models in Epidemiology.
Oxford: Oxford Univ Pr; 1993:31-7.Willett JB, Singer JD.
Investigating onset, cessation, relapse, and recovery: why you should, and how you can, use discrete-time survival analysis to examine event occurrence.
J Consult Clin Psychol. 1993;61:952-65Lee ES, Forthofer RN, Lorimer RJ.
Analyzing complex survey data.
In: Lewis-Beck MS, ed.
Newbury Park, CA: Sage Publications; 1989.Goldstein MS.
The Health Movement: Promoting Fitness in America.
New York: Twayne Publishers; 1992.Delbanco T.
A piece of my mind. Leeches, spiders, and astrology: predilections and predictions.
JAMA. 1998;280:1560-2Shekelle PG, Rogers WH, Newhouse JP.
The effect of cost sharing on the use of chiropractic services.
Med Care. 1996;34:863-72Astin JA.
Why patients use alternative medicine: results of a national study.
JAMA. 1998;279:1548-53Whorton JC.
Drugless healing in the 1920s: the therapeutic cult of sanipractic.
Pharmacy in History. 1986;28:14-25Reed LS.
The Healing Cults. A Study of Sectarian Medical Practice:
Its Extent, Causes and Control.
Chicago: Univ Chicago Pr; 1932.Rothstein WG.
American Physicians in the Nineteenth Century; From Sects to Science.
Baltimore: Johns Hopkins Univ Pr; 1985.
Return to EISENBERG's CAM ARTICLES
Since 10-31-2001
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |