

Patterns of Use, Expenditures, and Perceived Efficacy of
Complementary and Alternative Therapies
in HIV-Infected PatientsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Archives of Internal Medicine 1998 (Nov 9); 158 (20): 257–2264 ~ FULL TEXT
OPEN ACCESS Kathleen M. Fairfield, MD; David M. Eisenberg, MD; Roger B. Davis, ScD; et al
Beth Israel Deaconess Medical Center,
and Harvard Medical School,
Boston, Mass 02215, USA.BACKGROUND: Complementary and alternative medicine (CAM) use is common in the general population, accounting for substantial expenditures. Among patients with human immunodeficiency virus (HIV) infection, few data are available on the prevalence, costs, and patterns of alternative therapy use.
METHODS: We carried out detailed telephone surveys and medical chart reviews for 289 active patients with HIV in a general medicine practice at a university-based teaching hospital in Boston, Mass. Data were collected on prevalence and patterns of CAM use, out-of-pocket expenditures, associated outcomes, and correlates of CAM use.
RESULTS: Of 180 patients who agreed to be interviewed, 122 (67.8%) used herbs, vitamins, or dietary supplements, 81 (45.0%) visited a CAM provider, and 43 (23.9%) reported using marijuana for medicinal purposes in the previous year. Patients who saw CAM providers made a median of 12 visits per year to these providers compared with 7 visits per year to their primary care physician and nurse practitioner. Mean yearly out-of-pocket expenditures for CAM users totaled $938 for all therapies. For the main reason CAM was used, respondents found therapies "extremely" or "quite a bit" helpful in 81 (81.0%) of 100 reports of supplement use, in 76 (65.5%) of 116 reports of CAM provider use, and in 27 (87%) of 31 reports of marijuana use. In multivariable models, college education (odds ratio [OR]=3.7, 95% confidence interval [CI]=1.9–7.1) and fatigue (OR=2.7, 95% CI=1.4–5.2) were associated with CAM provider use; memory loss (OR=2.3, 95% CI=1.1–4.8) and fatigue (OR=0.4, 95% CI=0.2–0.9) were associated with supplement use; and weight loss (OR=2.6, 95% CI=1.2–5.6) was associated with marijuana use.
CONCLUSIONS: Patients with HIV infection use CAM, including marijuana, at a high rate; make frequent visits to CAM providers; incur substantial expenditures; and report considerable improvement with these treatments. Clinical trials of frequently used CAMs are needed to inform physicians and patients about therapies that may have measurable benefit or measurable risk.
From the FULL TEXT Article:
Background
Complementary or alternative medical therapies, defined as those treatments that have not generally been promoted and taught in Western medical schools and that have not generally been available at Western hospitals and clinics, [1–4] have been the focus of increasing interest by patients, clinicians, and researchers. A nationwide telephone survey in 1990 found that 34% of those surveyed used at least 1 complementary or alternative medical therapy to treat a serious or bothersome problem within the previous year. Based on data collected in that survey, the authors estimated that in 1990, 60 million US citizens used these therapies and spent an estimated $14 billion, of which $10.5 billion was spent "out-of-pocket." [1]
Use of complementary or alternative medicine (CAM) may be substantially more prevalent among patients with human immunodeficiency virus (HIV) than among the general population. A small study [5] of 2 groups of HIV-infected patients in northern California from 1988 to 1990 found that 70% had used CAM at some point. According to results from a Boston, Mass, survey, Cohen et al [6] reported in 1990 that 73% of patients used CAM. This study showed that those patients with higher education levels and lower helper T cells were more likely to use CAM. These studies were performed before the availability of protease inhibitors, which may have affected CAM use. In addition, few data are available on the specific therapeutic goals or symptoms that patients with HIV may attempt to treat with CAM, their associated outcomes, and expenditures for CAM by HIV-infected patients.
Among patients cared for in a primary care practice, we sought to determine patterns of use, associated expenditures, and perceived efficacy of CAM use among patients with HIV. We hypothesized that prevalence and expenditures for CAM would be high in this population, that patients with more advanced disease would use CAM to a greater degree, and that patients would generally perceive CAM to be efficacious.
Patients and methods
Study population
The study included a telephone survey and detailed medical chart review of all known HIV-infected patients at a primary care internal medicine practice at Beth Israel Deaconess Medical Center, Boston. This practice includes approximately 30 faculty, 100 house officers, and 10 nurse practitioners. The medical records for the practice are completely computerized, including all notes, medications, and problem lists. [7] The practice provides more than 50,000 patient visits annually. Approximately 30% of patients are covered by Medicaid or by a hospital system of free care.
In December 1996, we identified all known HIV-positive patients in our practice. We contacted the primary care physician for each patient by mail in January 1997 and asked for permission to include their patients in a study of CAM use. If permission was given, we contacted patients by mail with a letter sent jointly by their primary care physician and the study's principal investigator. Patients had the opportunity to request that they not be contacted for interview either by sending back a refusal card included with the letter or by calling within 2 weeks. To preserve patient confidentiality, neither the initial letter nor the card included any mention of HIV infection as a criterion for study eligibility. Also, the letter did not specifically mention CAM in an attempt to avoid enriching our sample for patients interested in describing CAM use. After 2 weeks, we attempted to contact by telephone those patients who had not refused to participate. We obtained informed consent verbally at the beginning of the telephone survey after informing patients that they were confidentially identified as HIV positive for research purposes. We informed patients that researchers at Beth Israel Deaconess Medical Center were carrying out the study to investigate types of therapies people may use for health problems. At no point during the interview did we use the term "alternative therapy" or an equivalent term to avoid value judgments about what therapies might be "alternative." The Beth Israel Deaconess Medical Center Committee on Clinical Investigations approved the consent process and study design.
As of December 1996, there were 289 active patients with HIV who received primary care in the practice. We excluded 14 hospital employees, 4 non–English-speaking or deaf patients, 3 patients with no working telephone, and 23 patients whose households were never reached by telephone despite numerous attempts during the study. Primary care physicians excluded 7 patients for reasons including severe psychiatric disease, difficult social situations, and extreme physical illness. Of 238 patients who remained eligible, 59 refused the telephone interview. We completed 180 interviews, yielding a response rate of 75.6%.
Data collectionTelephone Survey We interviewed all patients by telephone between April 22 and June 30, 1997, using professional interviewers. The interviews averaged 22 minutes. We asked patients whether they had experienced specific symptoms in the past year that were bothersome enough to keep them from their usual activities. These symptoms included pain, fatigue, weight loss and anorexia, and memory impairment or difficulty concentrating. Within each of these symptom categories, patients were queried about conventional therapies a physician may have prescribed for each problem and the perceived efficacy of those therapies. We then asked about the use of vitamins, herbal therapies, dietary supplements, marijuana for medicinal purposes, off-label prescription medications, and any other supplements in the past year using open-ended questions. Off-label prescription medications were described as medications that were generally available only by prescription but that the patient was able to obtain in another manner. We asked patients specifically if they had visited an acupuncturist, chiropractor, herbalist, homeopath, massage therapist, or other provider in the past year. We then asked open-ended questions about use of other therapies not already discussed or visits to other practitioners not specifically queried earlier. For those who use CAM providers or dietary supplements such as herbs or vitamins, we asked the respondent to identify the 3 most helpful therapies they used and then asked a series of specific questions about these 3 therapies.
Specific questions about each therapy included whether the patient was currently using the therapy, duration of use, frequency of use, and expenditures (total and out-of-pocket). We defined total expenditures as all expenditures by the patient and any other payer and out-of-pocket expenditures as those not covered by insurance or some other payer. Patients were queried about whether they had ever stopped using prescription medicines or specific CAM therapies because of the cost. We then asked if there was a specific main reason the patient sought the alternative therapy. Patients who reported a main reason for using a therapy were asked what that reason was and were queried about perceived efficacy of the therapy for that main reason. All patients, including those who did not report a main reason, were asked if there were any other reasons they used the therapy. Patients could report as many other reasons as applied. We also asked if their primary care physician was aware that they used the therapy and whether they started using the therapy before finding out they were HIV positive.
We collected demographic information, including level of education, race, and years of known HIV infection, as well as current employment status and income. Patients were queried about their sources of information about alternative therapies and their preferences for sources of information in the future.
Medical Chart Review We abstracted clinical data from the computerized medical record for the 2–year period between July 1, 1995, and June 30, 1997. Demographic data were collected, including age, sex, insurance type, HIV risk factors, and duration of HIV infection. We abstracted clinical information, including all prescription medications, HIV-related complications, CD4 cell counts and viral load measurements, clinic visits and hospital admissions, history of anxiety and depression, outpatient psychiatric care, and history of painful syndromes (eg, neuropathy and back pain). We also noted whether there was documentation of alternative therapy use in the medical record. Because of concern that patients might choose alternative therapies in place of conventional therapies, we searched text of notes and problem lists for evidence that this had occurred.Statistical analyses
We used descriptive statistics (SAS Institute Inc, Cary, NC) to characterize our study population. Nonrespondents and respondents were compared using logistic regression models with a single covariate, with P<.05 as a criterion for statistical significance. We calculated yearly expenditures on supplements and marijuana by multiplying reported monthly expenditures by 12. For CAM providers, we calculated yearly expenditures by multiplying reported costs per visit by the average number of visits per year. We used descriptive statistics to examine most common self-reported indications for therapies, perceived efficacy of specific therapies, and current vs ideal sources of information for patients.

Table 1 Our outcomes of interest included use of CAM providers, herbs, vitamins, other supplements, and marijuana and any other CAM use. We sought to identify all correlates of CAM use for each major category of CAM. Because of inadequate statistical power, we present only descriptive statistics (Table 1) for CAM not included in these major categories. Using bivariable logistic regression, we identified all unadjusted predictors of CAM use. The best multivariable model for each type of CAM use was then selected by carrying out forward logistic regression with stepwise checks and elimination of any previously selected variables with the smallest nonsignificant partial F statistic.8 Variables that were eliminated were examined as potential confounders using a change in the variable estimate of 10% as the criterion for confounding.9 We searched for significant interaction terms based on clinical judgment and statistical associations. Final models were created for each type of CAM using the best models from stepwise regression with the addition of confounders. We report relative risks with 95% confidence intervals as measures of association.
The number of visits and costs of CAM nationwide were extrapolated by multiplying the number of known adult and adolescent HIV-positive persons in the United States [10] by the percentage who would be expected to use any CAM (for costs) or CAM provider (for visits) from our estimates of CAM use. We used the consumer price indexes for medical care between 1991 and 1997 to estimate costs of conventional medical care for persons with HIV in 1997 using cost data from 1990. [11]
Results
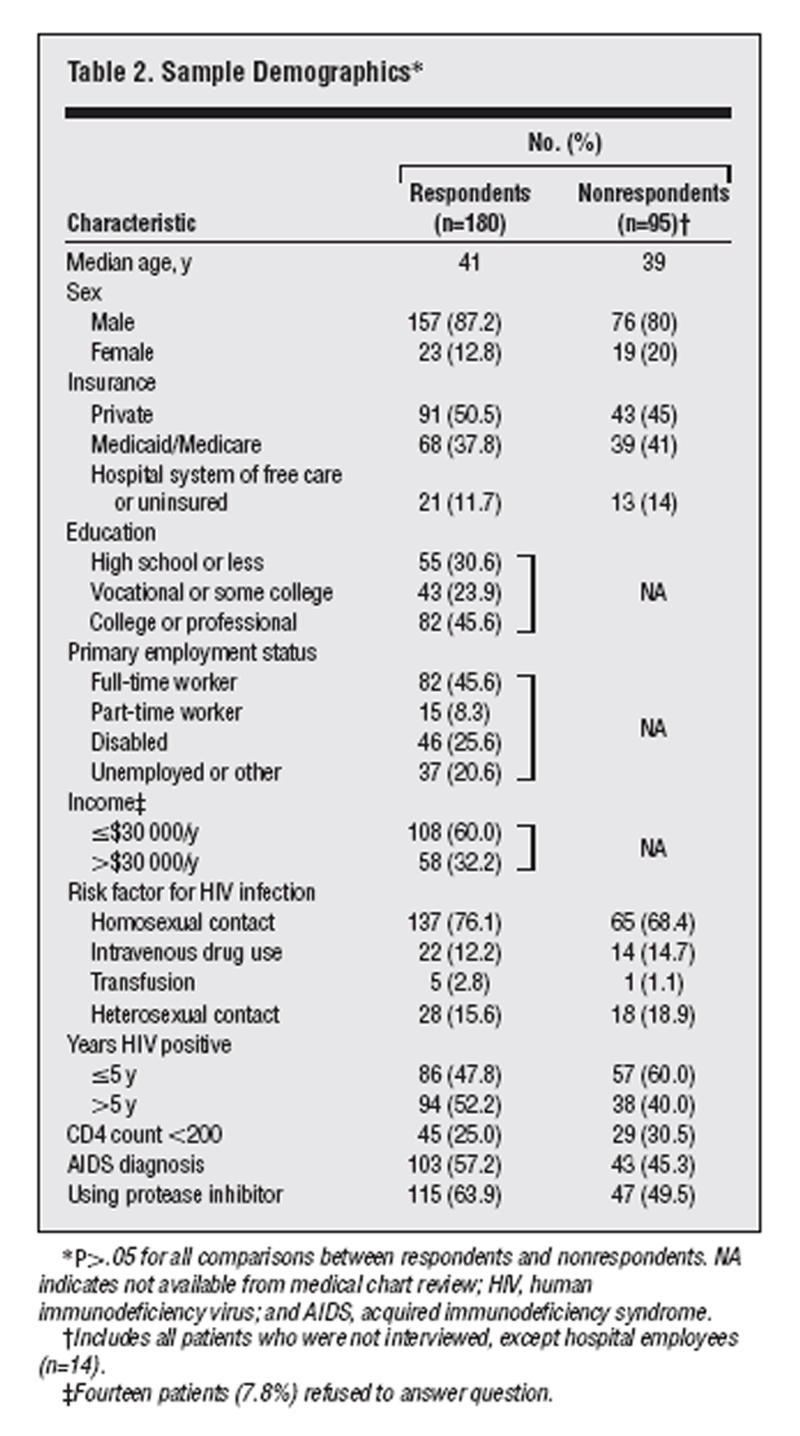
Table 2 Table 2 provides a comparison of demographic data for respondents vs nonrespondents (including refusals and ineligibles). Respondents and nonrespondents did not differ significantly with regard to age, sex, insurance status, HIV risk factors, years of HIV infection, percentage of patients with CD4 cell counts less than 0.20 × 109/L (200 cells/µL), acquired immunodeficiency syndrome diagnosis, or protease inhibitor use. We report data on years of HIV infection from the medical chart review instead of the interview because we have chart data on all participants, and concordance between duration of HIV infection by patient reports and medical chart review was excellent. Because educational attainment, income, and employment status were assessed with the survey, we do not have data on nonrespondents. Both respondents and nonrespondents used a median of 16 prescription medications.
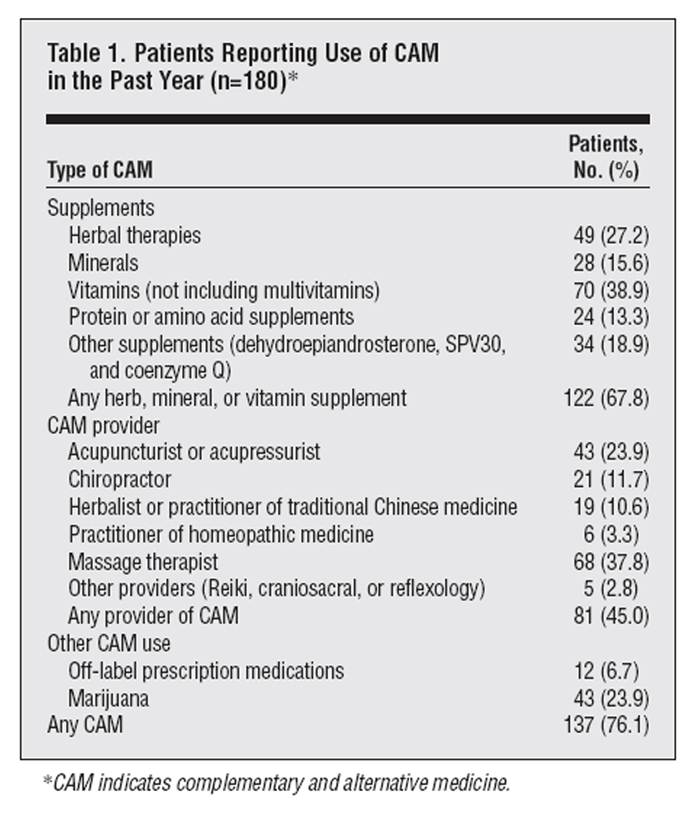
Table 1 describes the prevalence of CAM use in the study population, excluding users of multivitamins or commonly prescribed energy supplements. The most common dietary supplements were vitamins and herbal therapies. Massage therapists and acupuncture and acupressure providers were the most commonly reported CAM providers visited. Twenty-four percent of patients reported using marijuana for medicinal purposes. Forty-seven (38.5%) of 122 respondents who used supplements used more than 3 types of supplements, whereas 14 (17%) of 81 respondents who used CAM providers used more than 3 types of providers.
For respondents who used CAM, mean total (and out-of-pocket) annual expenditures were $815 ($620) for herbs, vitamins, and supplements; $510 ($340) for marijuana; and $652 ($495) for CAM providers. Mean total (and out-of-pocket) annual expenditures for all CAMs were $1,159 ($939) per year. These data represent reported expenditures for the 3 most helpful CAMs in each category for a respondent. Sixteen percent of patients reported discontinuing use of prescription medications at some point because of cost. For respondents who used CAM, 20% stopped using supplements, 49% stopped seeing CAM providers, and 49% stopped using marijuana at some point because of cost.
Overall, for patients who saw CAM providers, the median visit frequency was 12 visits per year. Respondents who saw massage therapists (n=68) and acupuncturists (n=43) made a median of 10 visits per year to each of those providers; respondents who saw chiropractors (n=21) made a median of 24 visits per year; respondents who saw herbalists (n=19) made a median of 12 visits per year; and respondents who saw practitioners of homeopathic medicine (n=6) made a median of 6 visits per year. The median frequency of visits to all other CAM providers (n=5, including Reiki, craniosacral therapy, and reflexology) was 20 visits per year. In comparison, patients who saw CAM providers made a median of 7 visits per year to their primary care physicians and nurse practitioners combined. Respondents who used supplements did so frequently during an average month, reporting that 86% of the time they used supplements more than 10 days per month.
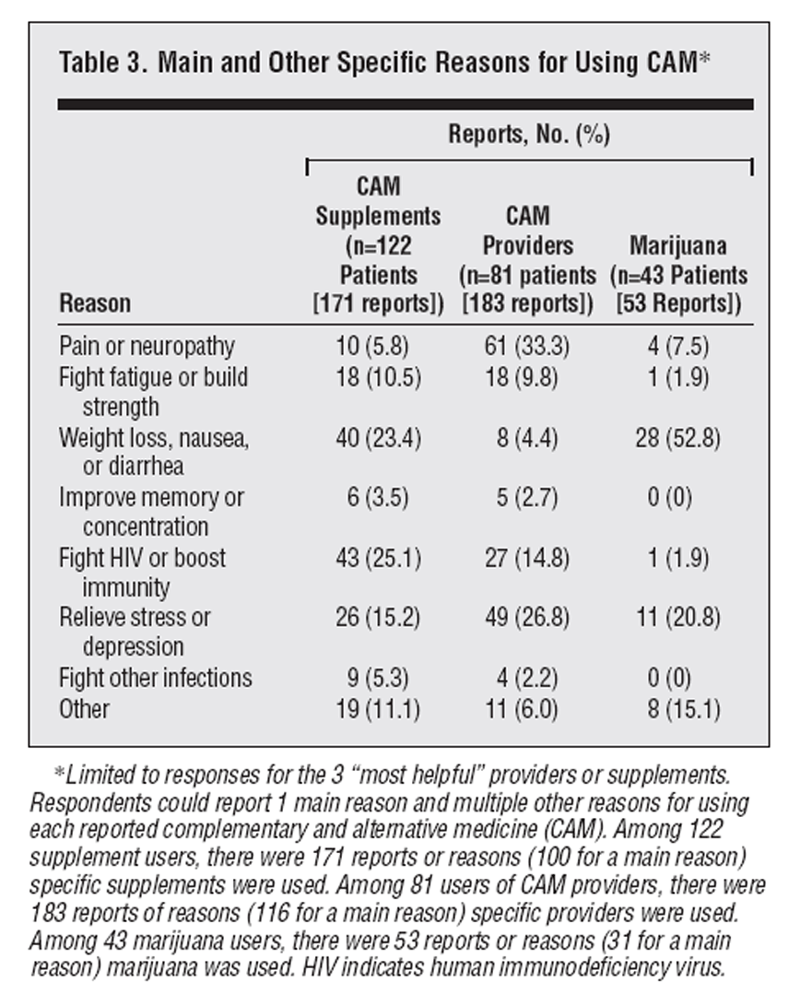
Table 3 Table 3 demonstrates main and other reasons for using CAM. The most commonly reported reasons for using herbs, vitamins, and supplements were to fight infections or boost immunity (25%) and to treat weight loss, nausea, and diarrhea (23%). The most commonly reported reasons for visiting CAM providers were pain relief or neuropathy (33%) and to reduce stress and depression (27%). For the main reason supplements were used, those who used supplements (n=122) found them "extremely" or "quite a bit" helpful in 81 (81%) of 100 reports of use. For the main reason CAM providers were used, those who used CAM providers (n=81) found them "extremely" or "quite a bit" helpful in 76 (65.5%) of 116 reports of use.
Of those patients using marijuana (n=43), 44% reported using marijuana more than 10 days per month. The most commonly reported reason for using marijuana was nausea or weight loss (53%). For the main reason marijuana was used, those who used marijuana (n=43) found it "extremely" or "quite a bit" helpful in 27 (87%) of 31 reports of use.
In response to questions about bothersome symptoms in the past year, 30.6% (55/180) of patients experienced unintentional weight loss, 31.1% (56/180) of patients experienced memory or concentration problems, and 37.8% (68/180) of patients experienced bodily pain; 47.8% (86/180) of respondents experienced fatigue.
Among patients reporting fatigue as the main reason for using CAM (15 reports), 67% found the therapy "extremely" or "quite a bit" helpful. When primarily used to improve pain (57 reports), 58% found the therapy "extremely" or "quite a bit" helpful. When primarily used to reduce stress or depression (32 reports), 57% reported finding the therapy "extremely" or "quite a bit" helpful. Among patients reporting nausea or weight loss as the main reason for using CAM (32 reports), 60% found it "extremely" or "quite a bit" helpful. Few patients received either medical or CAM treatment for memory and concentration problems.

Figure 1 Of patients with fatigue (Figure 1), 22 (26%) of 86 had received treatment from a physician for fatigue; of those 22 patients, 17 (77%) found the medication at least moderately helpful. Only 5 of 22 patients found medical therapy "slightly" or "not at all" helpful for fatigue, and none of those sought CAM for fatigue. Of 17 patients who found medical therapy helpful, 15 (88%) also used CAM specifically for fatigue, and 14 (93%) of 15 patients found CAM at least moderately helpful. Of 64 patients who complained of fatigue but did not receive medical therapy, 8 used CAM for fatigue, and 7 (88%) of 8 patients found CAM at least moderately helpful. We found similar patterns for use of conventional medical therapy and CAM for pain and weight loss or anorexia.
Most patients started visiting alternative providers (72.7%) and using supplements (70.9%) after learning that they were HIV positive. Users of acupuncture (87.8%) and supplements other than herbs, vitamins, and minerals (95.8%) were most likely to begin use after learning that they were HIV positive. In contrast, only 30.2% of patients reporting marijuana use began using it after learning about their HIV status. Slightly more than 67% of patients reported that their primary care physician was aware that they saw CAM providers, while 65.6% of supplement users and 69.8% of marijuana users reported that their primary physician was aware of their CAM use. For most respondents (64%) who reported that their primary care physician knew about their CAM use, we found supporting documentation in the medical record.
Respondents reported receiving information about CAM from newsletters for patients with HIV (62.2% [112/180]), friends or family members (51.1% [92/180]), physicians (47.2% [85/180]), and practitioners other than physicians (32.8% [59/180]). We queried patients about their 2 most favored sources of information on CAM. Patients reported preferring to receive CAM information from physicians (62.2% [112/180]), a consultation service at the hospital (52.2% [94/180]), and newsletters for patients with HIV (32.2% [58/180]).
We identified 3 patients (1.7%) by medical chart review who chose alternative therapies instead of conventional therapies. All 3 patients were taking other prescription medications but were not undergoing antiretroviral drug therapy. All 3 eventually accepted protease inhibitors after having a rise in their viral load. We found no documentation of patients refusing treatment or prophylaxis against opportunistic infections in favor of CAM.
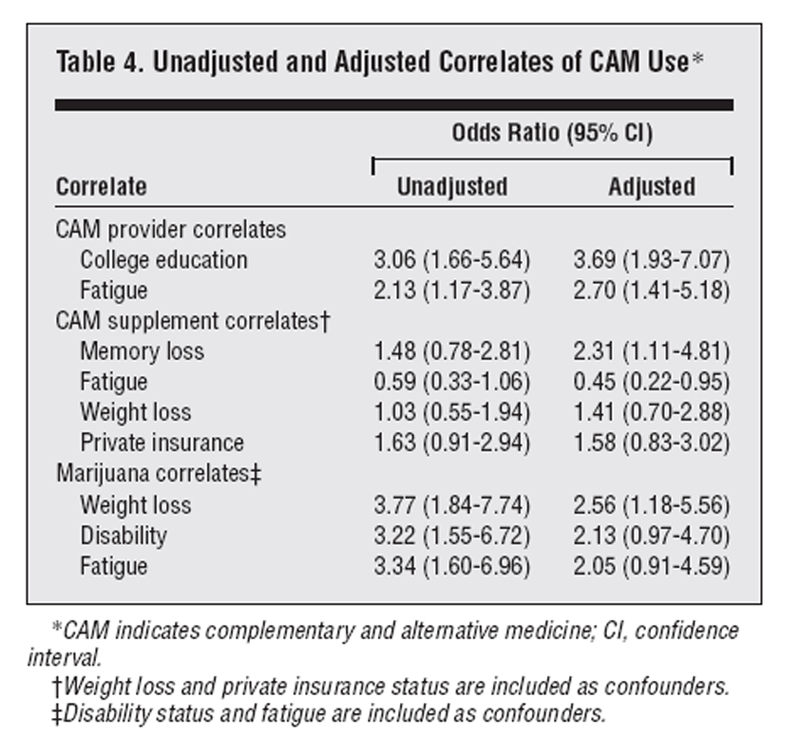
Table 4 Table 4 shows the unadjusted and adjusted odds ratios for the significant predictors of CAM use. In multivariable models, history of college education and fatigue were positively associated with CAM provider use. For patients taking supplements, history of memory loss was positively associated with use, but patients with fatigue were less likely to use supplements. History of weight loss was positively associated with marijuana use. We did not identify any significant interaction terms. A diagnosis of acquired immunodeficiency syndrome, CD4 cell count, number of HIV-related complications, duration of HIV infection, history of depression, HIV risk factors, frequency of clinic visits, and race were not statistically associated with CAM use in bivariable or multivariable models.
Comment
We found a high rate of CAM use among HIV-infected patients in our population, and most often these patients were using conventional therapy as well. However, patients who used CAM providers made more visits to these providers than to their physicians and nurses combined. Patients reported substantial benefit from the use of CAM, whether they used it alone or in combination with conventional treatment.
There are few previous data on expenditures for CAM among the HIV-infected population, a group known to experience economic hardship because of changes in employment from their debilitating disease. [12, 13] In our study, costs for these visits were variable, with several patients reporting that they receive services free of charge. Several clinics in the Boston area now offer these services at low or no cost to patients with HIV and acquired immunodeficiency syndrome. Despite this availability, the mean out-of-pocket yearly expenditure was more than $900 for all alternative therapies for those using any CAM. The observation that nearly half the respondents stopped using a therapy at some point because of cost suggests that some patients may seek alternative therapies to the point of financial hardship.
There has been an intense increase in media coverage on the issue of medicinal use of marijuana in the recent past. One quarter of our population uses marijuana for medicinal purposes. To our knowledge, no recent survey has assessed prevalence of marijuana use among patients with HIV. Patients seem to be aware of the purported benefits of marijuana, using it primarily for symptoms of nausea and weight loss. We also found high perceived efficacy of marijuana, with 87% finding it "extremely" or "quite a bit" helpful regardless of the problem for which it was used. Total and out-of-pocket expenditures on marijuana were nearly as high as expenditures on CAM providers. It is unclear why some patients reported out-of-pocket costs for marijuana that differed from total costs and whether some patients were receiving subsidies for marijuana purchases.
Our findings are consistent with those of earlier studies in Boston6 and California [5] of HIV-infected patients showing high rates for using CAM. Our findings differ from those of Greenblatt et al [14] and Anderson et al, [15] who found that only 29% to 40% of patients attending conventional medical care sites were also using CAM. These studies may have underestimated CAM use because they referred to therapies as "unorthodox" or "alternative" or because they only assessed therapies taken by mouth. [14] Because we collected our data after protease inhibitors became widely available, it seems that the availability of efficacious antiviral drugs has not diminished CAM use. Others have reported comparably high rates of CAM use in patients with long-term disease other than HIV infection, including cancer [16, 17] and arthritis. [18] Our findings suggest that HIV-infected patients, like those with other long-term illness, may use CAM to a much greater degree than the general population.
Patients with HIV seem to use CAM for a variety of reasons, most importantly to relieve pain or neuropathy, to relieve stress or depression, to fight other infections, and to treat weight loss and nausea. In contrast to findings by Anderson et al [15] suggesting that many patients sought cure or antiviral effects from CAM, we found that few respondents used CAM to fight HIV specifically. This difference may be because of the availability of more potent antiviral drugs (ie, protease inhibitors) than were available to patients studied by Anderson et al in 1993. Perceived efficacy for CAM was high overall among our study patients. Patients often use CAM for a specific problem even if they received medical treatment for the same problem and had perceived the conventional therapy to be efficacious. These data are consistent with findings from previous works1,6 demonstrating that most CAM users also sought conventional therapy for medical problems treated with CAM. Therefore, patients infected with HIV who receive care in a conventional setting seem to use CAM with conventional medical therapies in an integrative fashion.
We found a high rate of disclosure regarding CAM use between patients and physicians. Patient reports of disclosure were supported by medical record documentation in most cases. These data are in contrast to the findings by Eisenberg et al1 in 1990, who found that 72% did not inform their physician about CAM use. The reasons for higher disclosure rates are unclear but may reflect secular trends, a change in the receptivity of physicians to discussing CAM use, or the possibility that individuals with long-term or life-threatening illness are more apt to discuss CAM with their conventional caregivers.
We estimated that mean total and out-of-pocket annual expenditures for all CAM were $1.159 and $939, respectively, for users of CAM. Comparison with expenditures on conventional medical care is difficult because reliable data on out-of-pocket expenditures for medical care of patients with HIV are limited. The Boston Health Study [19] reported mean out-of-pocket expenditures of $429 per person with acquired immunodeficiency syndrome for 4 months in 1990 ($1,287 annually). They reported mean total expenditures of $9,093 ($27,279 annually). When adjusted for the consumer price index, [11] the comparable 1997 estimates would be $1,801 out-of-pocket and $38,165 total expenditures. Current out-of-pocket expenditures may vary from this estimate because of changes in outpatient drug therapy for HIV and hospitalization rates. We estimate that 2% of total costs and 24% of out-of-pocket costs of medical care for HIV-infected patients are attributable to CAM. Given that approximately 600,000 adults and adolescents are known to be HIV-infected in the United States, [10] extrapolation to the US HIV population (assuming that 76% use CAM) would place total expenditures on CAM at approximately $529 million per year and the total number of annual visits for CAM providers (assuming 45% utilization) at 3.2 million nationwide.
Our study has several limitations. Because the study population consists primarily of homosexual males and is limited geographically to the metropolitan Boston area, our findings may not be generalizable to the entire US population. However, given that CAM use seems to be higher in the western United States, it is likely to underestimate utilization rates in the HIV population nationwide. Our small sample size may result in low statistical power to detect differences between respondents and nonrespondents. Also, we queried only patients who had already chosen to receive care in a conventional setting, making it difficult to extrapolate conclusions about the integrative nature of CAM use among all people with HIV infection. However, this is also likely to underestimate CAM use because people with HIV who reject conventional care may be expected to use CAM to a greater degree. There is potential for selection bias if patients who used CAM were more likely to complete the interview. However, we did not inform patients of the study's purpose during the recruitment process.
An additional limitation is that small numbers of users of certain types of CAM make it difficult for us to comment on perceived efficacy for specific therapies. Our data with regard to perceived efficacy may be biased because our study is cross-sectional in nature. Respondents may have ceased using therapies perceived as less helpful in the past. In addition, for patients who used several alternative therapies, we asked detailed questions about expenditures and perceived efficacy only for the 3 they believed were most helpful. This may have biased our results toward those therapies used most frequently and therefore increased our estimates for visit frequency as well as perceived efficacy. Also, patients may be more likely to perceive therapies as efficacious if they made an active choice to obtain them. In addition, our study can comment on perceived efficacy only and not on efficacy of CAM for specific problems. However, data on perceived efficacy may guide randomized controlled trials in the future. Our cost data are incomplete because we only inquired about cost for a limited number of CAMs. However, this may have resulted in an underestimation of total visits and costs because many patients used several types of CAM. In addition, our relatively small sample may not be representative of the HIV population in the United States for the reasons discussed above, so the extrapolation of our cost data should be viewed with caution.
Another potential limitation of our study is our choice of definition of CAM. We included massage and vitamins (but not daily multivitamins), which may be considered mainstream therapy by some providers of conventional medicine. These inclusions would tend to overestimate prevalence and costs of CAM use. Nonetheless, use of high-dosage vitamins and massage can be distinguished from such activities as weight training and day-spas as having specific therapeutic (if not "medicinal") goals for most patients who use them (eg, immune boosting or stress reduction). However, use of high-dosage vitamins and massage are not generally believed to be therapeutic maneuvers by conventional physicians, and massage techniques are not taught at conventional medical schools. Although data on therapeutic efficacy for some therapies (such as acupuncture for neuropathic pain) are being collected, we may have to be flexible about definitions of CAM for purposes of descriptive studies.
In this study, we did not collect data on potential adverse effects of CAM. There are several reports in the medical literature that suggest potential for harm with certain CAM therapies. [20–23] Little is known about the biologic activity of most CAM therapies, and there seems to be potential for "drug-drug" (or "drug-herb or supplement") interaction for CAM therapies that are ingested. This may be particularly problematic when patients involved in clinical trials also use CAM therapies. [24] Several groups nationally and internationally have called for regulation of CAM and prospective monitoring for adverse events. [25–28] Future studies should place emphasis on careful collection of data on adverse events.
In summary, we demonstrated a high prevalence of CAM use among patients with HIV, with high yearly visit rates and expenditures. Patients involved in conventional care use CAM to complement conventional therapies for specific symptoms or problems rather than to the exclusion of conventional care. In general, perceived efficacy of CAM is high. Clinicians are often queried about CAM and have limited information to offer patients. Until more information is available from randomized trials, perceived efficacy of therapies may be a useful way to guide patients toward therapies that seem to provide relief from refractory symptoms. Research funds should be directed toward conducting outcomes research and randomized controlled trials of specific therapies in those patient subgroups who seem to derive the most benefit. For example, studies of the antiemetic effect of marijuana and the analgesic effects of acupuncture and chiropractic might be given higher priority. These trials should include patients who are undergoing intensive pharmacological therapy for HIV to provide data on potential interactions or adverse effects.
This study was supported by National Research Service Award PE11001-09 (Dr Fairfield). Partial funding for this project was provided by the Center for Alternative Medicine Research; grant U24 AR3441 from the National Institutes of Health, Bethesda, Md; The John E. Fetzer Institute, Kalamazoo, Mich; the Friends of Beth Israel Deaconess Medical Center, Boston, Mass; the Kenneth J. Germeshausen Foundation, Boston; and the J. E. and Z. B. Butler Foundation, New York, NY.
We thank the patients of Beth Israel Deaconess Medical Center who gave their time for this study.
Corresponding author: Kathleen M. Fairfield, MD, Division of General Medicine and Primary Care, Beth Israel Deaconess Medical Center, Libby 330, 330 Brookline Ave, Boston, MA 02215.
References:
Eisenberg DM, Kessler RC, Foster C, Morlock FE, Calkins DR, Delbanco TL.
Unconventional Medicine in the United States: Prevalence, Costs, and Patterns of Use
New England Journal of Medicine 1993 (Jan 28); 328 (4): 246–252Gevitz N
Alternative medicine and the Orthodox Canon.
Mt Sinai J Med. 1995;62127- 131Delbanco TL
Bitter herbs: mainstream, magic, and menace.
Ann Intern Med. 1994;121803- 804urray RHRubel AJ
Physicians and healers: unwitting partners in health care.
N Engl J Med. 1992;32661- 64Dwyer JTSalvato-Schille AMCoulston ACasey VACooper WCSelles WD
The use of unconventional remedies among HIV-positive men living in California.
J Assoc Nurses AIDS Care. 1995;617- 28Cohen CJMayer KHEisenberg DMOrav EJDelbanco TL
Determinants of nonconventional treatment use among HIV-infected individuals.
International Conference on AIDS. 1990;6285Abstract SD781.Safran CRury CRind DMTaylor WC
A computer-based outpatient medical record for a teaching hospital.
MD Comput. 1991;8291- 299Kleinbaum DGKupper LLMuller KE
Applied Regression Analysis and Other Multivariable Methods.
Belmont, Calif Duxbury Press1988;Mickey RMGreenland S
The impact of confounder selection criteria on effect estimation.
Am J Epidemiol. 1989;129125- 137 10.Centers for Disease Control and Prevention,
HIV/AIDS Surveillance Report. 1997;9 ((No. 1)) Available at:
http://cdcnpin.org. Accessed January 22, 1998.US Department of Labor, Bureau of Labor Statistics,
Consumer Price Index Web site. Available at:
http://stats.bls.gov/cpihome.htm. Accessed March 2, 1998.Massagli MPWeissman JSSeage GR IIIEpstein AM
Correlates of employment after AIDS diagnosis in the Boston Health Study.
Am J Public Health. 1994;841976- 1981Kass NEMunoz AChen B et al.
Changes in employment, insurance, and income in relation to HIV status and disease progression.
J Acquir Immune Defic Syndr. 1994;786- 91Greenblatt RMHollander HMcMaster JRHenk CJ
Polypharmacy among patients attending an AIDS clinic: the utilization of prescribed, unorthodox,
and investigational treatments.
J Acquir Immune Defic Syndr. 1991;4136- 143Anderson WO'Connor BBMacGregor RRSchwartz JS
Patient use and assessment of conventional and alternative therapies for HIV infection and AIDS.
AIDS. 1993;7561- 566Cassileth BRLusk EJStrouse TBBodenheimer BJ
Contemporary unorthodox treatments in cancer medicine.
Ann Intern Med. 1984;101105- 112US Congress, Office of Technology Assessment,
Unconventional Cancer Treatments.
Washington, DC Government Printing Office1990;Publication OTA-H-405.Cronan TAKaplan RMPosner LBlumberg EKozin F
Prevalence of the use of unconventional remedies for arthritis in a metropolitan community.
Arthritis Rheum. 1989;321604- 1607Epstein AMSeage GWeissman JS et al.
Costs of medical care and out-of-pocket expenditures for persons with AIDS in the Boston Health Study.
Inquiry. 1995;32211- 221Curt GAKatterhagen GMahaney FX Jr
Immunoaugmentative therapy: a primer on the perils of unproved treatments.
JAMA. 1986;255505- 507Woolf GMPetrovic LMRojter SE et al.
Acute hepatitis associated with the Chinese herbal product Jin Bu Huan.
Ann Intern Med. 1994;121729- 735Hirschtick REDyrda SEPeterson LC
Death from an unconventional therapy for AIDS [letter].
Ann Intern Med. 1994;120694eely DRQuigley SMLangman AW
Ear candles: safety and efficacy.
Laryngoscope. 1996;1061226- 1229Fogelman ILim LBassett R et al.
Prevalence and patterns of use of concomitant medications among participants in three multicenter
human immunodeficiency virus type I clinical trials.
J Acquir Immune Defic Syndr. 1994;71057- 1063Marwick C
Growing use of medicinal botanicals forces assessment by drug regulators.
JAMA. 1995;273607- 609 ArticleDe Smet PA
Should herbal medicine–like products be licensed as medicines [editorial]?
BMJ. 1995;3101023- 1024Vautier GSpiller RC
Safety of complementary medicines should be monitored [letter].
BMJ. 1995;311633Drew AKMyers SP
Safety issues in herbal medicine: implications for the health professions.
Med J Aust. 1997;166538- 541
Return to EISENBERG's CAM ARTICLES
Since 3-21-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |