

Transforming the Veterans Affairs to a Whole Health
System of Care: Time for Action and ResearchThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Medical Care 2020 (Apr); 58 (4): 295–300 ~ FULL TEXT
OPEN ACCESS Barbara G. Bokhour, PhD • Jolie N. Haun, PhD • Justeen Hyde, PhD
Martin Charns, DBA • Benjamin Kligler, MD, MPH
Center for Healthcare Organization and Implementation Research,
Edith Nourse Rogers Memorial Veterans Affairs Medical Center,
VA New England Healthcare System, Bedford, MA 01730
FROM: Transforming the Veterans Affairs (Medical Care 2020)From the Full-Text Article:
Introduction
As part of the national movement towards value-based and accountable care, health care systems are working to incorporate patient-centered approaches to improve patients’ wellness and increase engagement in self-care. [1, 2] In 2001, the Institute of Medicine identified patient-centered care as one of the 6 pillars of quality of care, and defined it as “providing care that is respectful of and responsive to individual preferences, needs, and values and ensuring that patient values guide all clinical decisions.” [3] Patient-centered care shifts away from a disease-focused care model, and changes the conversation from “What is the matter with you?” to “What matters to you?”
For the past 6 years, the US Department of Veterans Affairs (VA) has been promoting patient-centered care through the implementation of a Whole Health approach. Whole Health is defined as an approach to health care that empowers and equips people to take charge of their health and well-being and live their life to the fullest.
The goals of the Whole Health approach go beyond patient-centered care; it focuses on understanding the patient’s life meaning, aspiration, and purpose (ie, what matters most to the patient) as the foundation for health care delivery. Whole Health integrates allopathic and complementary and integrative health (CIH) care where patients’ goals and priorities are incorporated into health care decisions, with peer-led support, personalized health planning, Whole Health coaches, and well-being classes.
The system-wide implementation of the Whole Health approach to care truly began in 2015–2016, with the identification of 25 “design sites,” VA medical centers that received dedicated funding to explore best practices for operationalizing the Whole Health vision. Spurred by a Congressional mandate in the Comprehensive Addiction and Recovery Act, [4] the Whole Health System of Care (WHS) was further formalized in 2017 when each Veterans Integrated Service Network — VA’s 18 regional networks — identified and funded a flagship medical center to implement the full WHS. A Veterans Health Administration Policy Directive, published in May 2017 mandating system-wide coverage of the evidence-based CIH approaches as part of VA standard medical benefits provided further momentum. [5]
In response to these impetuses, the Office of Patient Centered Care and Cultural Transformation (VA National Office), developed a bundle of implementation strategies to support Flagship and other sites in their system transformation efforts. This wide-ranging natural experiment provides an opportunity to examine the impact of the WHS on Veterans, employees, and the VA health care system.
If the hypothesized improvement in patient outcomes and satisfaction resulting from Whole Health is borne out and implementation of the WHS is shown to be cost-neutral or cost-effective, this system could become a model for value-based care for Accountable Care Organizations across the country searching for ways to transition from disease-based to population and value-based care.
Preliminary data from flagship sites are promising, with evidence indicating Veterans utilizing Whole Health services are reporting increases in patient engagement and satisfaction and decreases in perceived stress and opioid utilization (Bokhour BG, unpublished white paper, Veterans Affairs Office of Patient Centered Care and Cultural Transformation, December 2019).
Components of the Whole Health System of Care
There are 3 major components of the WHS:(1) The Pathway;
(2) Well-Being Programs; and
(3) Whole Health Clinical Care.Together these components illustrate a system of care that begins with the patients and their goals, then designs a personalized health plan to facilitate the achievement of those goals.
The Pathway introduces Veterans to the concepts of Whole Health and facilitates their identification of personal life and health goals and the development of a personal health plan. Ideally, the Pathway is introduced by a peer, rather than a licensed medical professional.
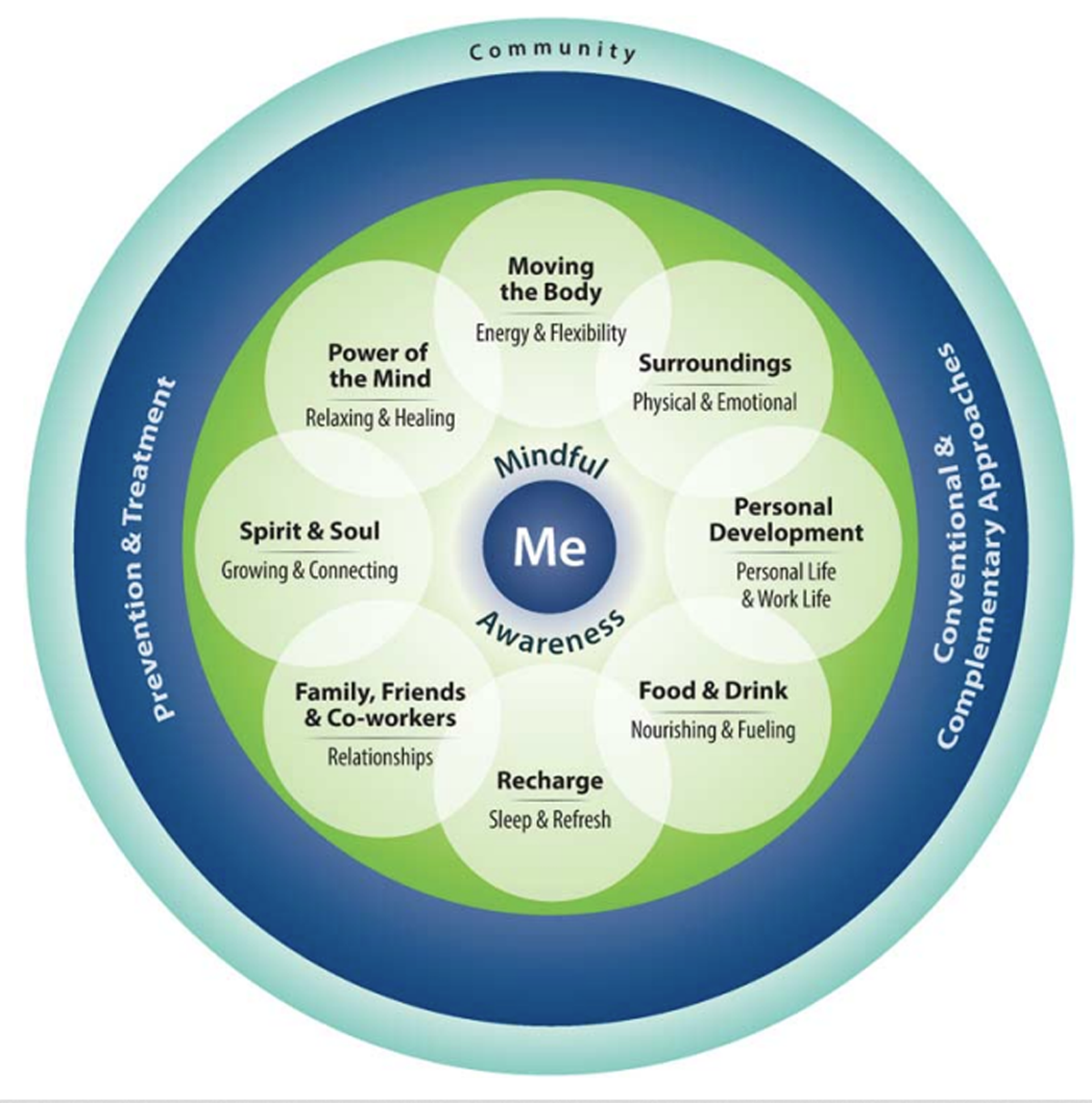
Figure 1 Through the Pathway, Veterans are introduced to the Components of Proactive Health & Well-Being — using the Wheel of Health (Figure 1) and encouraged to explore their mission, aspiration, and purpose through the completion of a Personal Health Inventory, leading to the development of a personal health plan.
Well-Being Programs include a combination of CIH services, health coaching, and support, and 9 self-care and skill-building groups aligned with the 8 components of the Wheel of Health (Figure 1).
All VA medical centers are now mandated to provide, either in-house or through contracted services outside the VA, nine different CIH modalities:
acupuncture, chiropractic, meditation, massage therapy, biofeedback, clinical hypnosis, guided imagery, yoga, and Tai Chi.
Whole Health Clinical Care includes the use of a Whole Health paradigm for providing care in both allopathic and CIH settings. Providers throughout the system are trained to provide Whole Health care, focusing on patients’ personal health plans and goals aligned with their meaning, aspiration and purpose as a foundation for treatment recommendations. Providers engage in health coaching and joint problem solving with patients to provide care in a way that is most aligned with the patients’ goals.
Care is optimized when these somewhat discrete components work synergistically, forming a WHS which aims to improve Veterans’ health and well-being by changing the culture of health care delivery such that Veterans are engaged as partners in their health care.
Supplementing the current expert-clinician model that focuses on targeted clinical or disease-specific goals, this model is grounded in the recognition that most of an individual’s health outcomes are related to factors outside of clinic walls, including their environment, personal behaviors, relationships, and income.
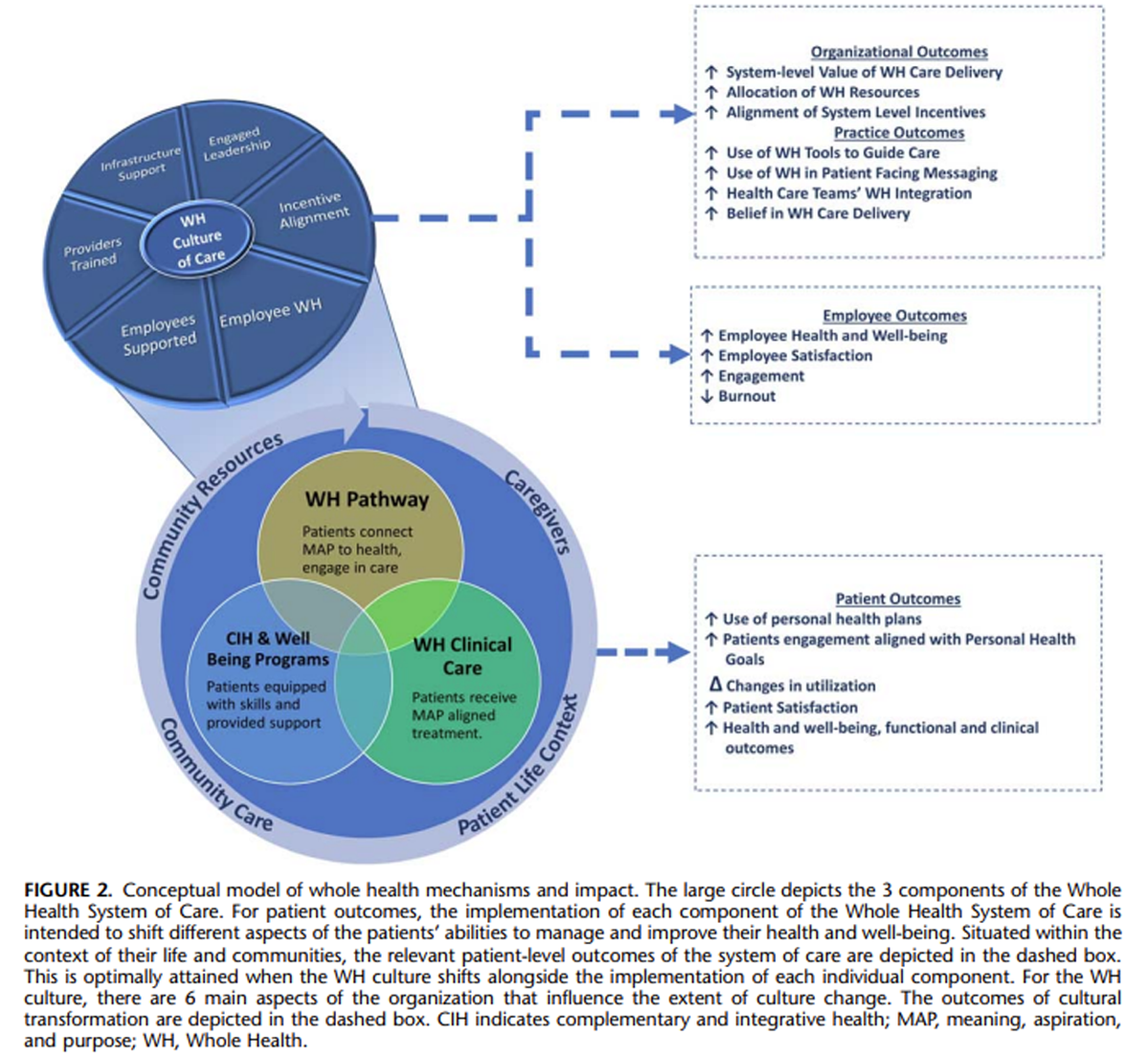
Figure 2 The WHS shifts the burden of health care towards a partnership model, with clinicians and Veterans bringing their expertise to the encounter and collaborating to identify the best course of care. The WHS conceptual model (Figure 2) provides a framework for understanding the intended outcomes of each component as well as the WHS. This model constitutes a conceptual shift regarding the relevant outcomes for the health care system from the absence of disease to improved well-being.
Research Directions for the Components of Whole Health
The evidence to date supporting the WHS as an effective integrated care delivery model is limited. Prior research supports some of the individual components; however, the integration of these components into a single system of care has yet to be thoroughly studied. In October 2018, VA Health Services Research & Development (HSR&D) convened a meeting of leading experts in patient-centered care and Whole Health with the goal of developing a research agenda to advance the science and implementation of Whole Health as a care delivery model within the VA. The following section summarizes the outcomes of that meeting.
Whole Health Pathway
There is little published literature examining health or wellness outcomes associated with exploration of one’s meaning, aspiration, and purpose or peer-based, non–disease-specific facilitation [6, 7]; there is a modest body of research on the role of peer-led groups and peer interventions, which focus more on disease-specific support. [8–11] Evidence is needed regarding the impact of giving patients opportunities to reflect on what matters most in their lives on patient engagement and self-efficacy to manage their health. Further, does having these activities led by Veterans, for Veterans makes a difference in process? We also need to know more about how variation in how often and in what format peers lead this exploration may impact outcomes.
Complementary and Integrative Health and Well-being Programs
There is a significant evidence base for the use of individual CIH modalities targeting specific health conditions, [12–14] as well as specifically for Veterans. These studies have demonstrated the effectiveness of CIH approaches such as acupuncture, chiropractic, meditation and mindfulness, yoga, and Tai Chi for managing symptoms of conditions including low back pain, chronic pain, post-traumatic stress disorder, and depression. [15–18]
Further research is needed to be focused on building knowledge about CIH by examining:(1) efficacy and use among Veterans;
(2) dosing, tailoring and sequencing of CIH and non-CIH approaches
(eg, cognitive behavioral therapy);
(3) delivery models;
(4) use of multimodality care on specific Veteran populations,
such as those with mental health and substance use;
(5) effective implementation strategies and barriers; and
(6) dissemination strategies. [19]Questions also remain about the effectiveness of the provision of CIH as standalone services as opposed to providing CIH within the context of the WHS.
Whole Health Coaching
Whole Health coaching in the WHS focuses on supporting Veterans to develop and attain their personal health goals. While there is a growing body of literature focused on health coaching, most studies conducted to date have examined coaching as a strategy to change the behavior associated with specific diseases, including mental health conditions, substance use, diabetes, weight management, and hypertension. [20–22]
Notably, substantial variation exists in the content of health coaching, the orientation of the coaches and the general theoretical framework guiding the coaching model. [23] There is some evidence that peer coaches can produce positive outcomes for specific conditions of focus. However, to date, there have not been rigorous studies examining the extent to which there are different outcomes associated with health coaching based on the clinical or nonclinical training of coaches.
Critical questions remain regarding the effectiveness of a coaching approach focusing on broader health goals aligned with the wheel of health. Should health coaching be in the context of ongoing regular care from clinically trained providers or from trained peer health coaches? What type of training is necessary to provide health coaching? How can health coaching be most effectively integrated into the health care team?
Whole Health Clinical Care
Using the Whole Health approach, the nature of the clinical conversation shifts away from one that starts with disease prevention, diagnosis, and treatment, to one that starts with the patients’ goals and priorities. Critical to this is incorporating what matters most to the patient to collaboratively develop shared goals for health and well-being and link interventions to the patient’s personal health plan.
There is a substantial body of work on the value of patient-centered communication and approaches to provider education for improving care and outcomes in many populations. There is however, insufficient knowledge about how creating this shift in the clinical conversation affects care in a broader-based health care system.
There are several gaps in Whole Health research relevant to clinical care. First is how to shift the orientation of experienced clinicians towards this patient-driven Whole Health approach to clinical conversations. We do not know what types of trainings, tools, or implementation strategies would be effective in achieving this goal.
For the conversation to shift, we must also shift the orientation of patients to what to expect in the clinical encounter. How do we engage patients in this endeavor to focus more on what matters to them and then engage them in making choices with their clinician that will result in most benefit? Finally, we need to know more about the structural, organizational barriers to engaging in these changed conversations.
Measuring Impact
One of the critical questions in implementing the WHS is the impact on Veterans’ health and well-being. Selecting measures that assess more than disease-specific clinical outcomes is critical. Measures must focus on the extent to which care provided helps patients engage in health care and selfcare and reach their own goals. This requires a conceptual shift about the goal of health care—from treating disease only, to treating disease and also fostering well-being. Health care systems need valid, reliable, and relevant measures for measuring this “new” dimension of their work. The Whole Health research agenda must include studies to identify key metrics for the outcomes of the WHS, studies examining patient outcomes of each component of the system, as well as patient and provider-level outcomes of implementing the WHS as a whole.
Organizational Change/Cultural Transformation
While each of the components described above offers concrete, discrete interventions to provide Whole Health care, there remain many challenges in implementing such a broad scale organizational change. We need to understand more about the organizational structures and requirements that facilitate or hinder the implementation of the model as intended.
Implementation science frameworks offer useful guidance for developing effective strategies to implement WHS components. Yet, without true organizational cultural transformation, the system of care will remain driven by a disease-based model of health care. [24, 25]
Cultural change must include shifting assumptions and values about the effectiveness and importance of Whole Health and the incorporation of norms of behavior aligned with Whole Health. It must also include an examination of how current organizational incentives, protocols and procedures align with Whole Health approaches. There is little research to date on patient-centered care [26] or Whole Health cultural transformation, yet we can learn from other studies and theories about other types of transformation (ie, safety culture, the culture of improvement). Studies in these areas have demonstrated that values are transformed through social networks and opinion leaders. [27]
Questions remain about how best to enculturate staff and providers to embrace a Whole Health approach. Who are the relevant opinion leaders for Whole Health transformation? What role do different social networks play for a Whole Health cultural shift? And how does Whole Health impact employees throughout the system? Moreover, how do we know when a system has succeeded in cultural transformation? There is a need to develop methods and metrics for assessing the experience of cultural change at the patient, caregiver, provider and staff level.
The Organization Transformation Model [27] offers one framework for understanding such large-scale cultural transformations. This model identifies 5 drivers of change:(1) leadership;
(2) alignment of organizational strategy (goals, resources, rewards);
(3) integration across internal organizational boundaries;
(4) impetus for change; and
(5) improvement initiatives.Through these drivers, change is achieved in individual behaviors, processes, and values; collectively, the changes in values in the social network is a change in organizational culture.
Conclusions
Creating a system of care that is truly patient-centered, focused on providing care that is aligned with individual patients’ goals, is of the highest priority. A Whole Health approach to care may have impacts on many levels — patients’ perception of their experiences, engagement in health care and self-care, and ultimately improved health and well-being. The Whole Health approach may also improve the lives of the health care system’s employees as they embrace the Whole Health approach for patients and for their own lives.
This is an ideal time for research to take advantage of the natural experiment of the WHS implementation. The flagship sites are embarking on their third year of funding. National expansion of the WHS continues, with 37 new medical centers selected by Veterans Integrated Service Network directors to participate in the next Whole Health learning collaborative to implement components of the WHS in 2020.
All 143 VA medical centers are advancing the Whole Health approach at varying levels. Studying implementation strategies for integrating Whole Health throughout the current system of care is essential to further the spread of Whole Health. A full research agenda that takes advantage of VA’s ongoing natural experiment of sites rolling out the WHS is necessary for understanding how a Whole Health approach can improve the health and wellbeing of our nation’s Veterans.
References:
Shortell SM, Poon BY, Ramsay PP, et al.
A multilevel analysis of patient engagement and patient-reported outcomes in primary care practices of accountable care organizations.
J Gen Intern Med. 2017; 32:640–647.Hacker K, Walker DK.
Achieving population health in accountable care organizations.
Am J Public Health. 2013;103:1163–1167.Institute of Medicine (US) Committee on Quality of Health Care in America.
Crossing the Quality Chasm: A New Health System for the 21st Century
Washington, DC: National Academies Press (US); 2001.United States Congress.
Joint Explanatory Statement of the Committee of Conference on S 524,
the Comprehensive Addiction and Recovery Act (CARA)
Washington, DC: US Government; 2016.Veterans Health Administration.
VHA Directive 1137: Provision of Complementary and Integrative Health
Washington, DC: Department of Veterans Affairs; 2017.Collins DA, Shamblen SR, Atwood KA, et al.
Evaluation of a health coaching course for providers and staff in Veterans Health Affairs medical facilities.
J Prim Care Community Health. 2015; 6: 250–255.Collins DA, Thompson K, Atwood KA, et al.
Integration of health coaching concepts and skills into clinical practice among VHA providers: a qualitative study.
Glob Adv Health Med. 2018;7:2164957X18757463.Tudor-Locke C, Lauzon N, Myers AM, et al.
Effectiveness of the First step Program delivered by professionals versus peers.
J Phys Act Health. 2009; 6: 456–462.Qi L, Liu Q, Qi X, et al.
Effectiveness of peer support for improving glycaemic control in patients with type 2 diabetes: a meta-analysis of randomized controlled trials.
BMC Public Health. 2015; 15: 471.Eisen SV, Schultz MR, Mueller LN, et al.
Outcome of a randomized study of a mental health peer education and support group in the VA.
Psychiatr Serv. 2012;63:1243–1246.Ashing-Giwa K, Tapp C, Rosales M, et al.
Peer-based models of supportive care: the impact of peer support groups in African American breast cancer survivors.
Oncol Nurs Forum. 2012; 39: 585–591.Strauss JL, Coeytaux R, McDuffie J, et al.
Efficacy of Complementary and Alternative Medicine Therapies
for Posttraumatic Stress Disorder (VA ESP Project #09-010)
Washington, DC: US Department of Veterans Affairs; 2011.Peterson K, Anderson J, Ferguson L, et al.
Evidence Brief: The Comparative Effectiveness of Selected
Complementary and Integrative Health (CIH) Interventions
for Preventing or Reducing Opioid Use in Adults With
Chronic Neck, Low Back, and Large Joint Pain
(VA ESP Project #09-199)
Washington, DC: US Department of Veterans Affairs; 2016.Elwy AR, Groessl EJ, Eisen SV, et al.
A systematic scoping review of yoga intervention components and study quality.
Am J Prev Med. 2014; 47: 220–232.Hempel S, Taylor SL, Solloway MR, et al.
Evidence Map of Acupuncture (VA ESP Project #05-226)
Washington, DC: US Department of Veterans Affairs; 2014.Hempel S, Taylor SL, Solloway MR, et al.
Evidence Map of Tai Chi (VA ESP Project #05-226)
Washington, DC: Department of Veterans Affairs; 2014.Miake-Lye I, Lee J, Lugar T, et al.
Massage for Pain: An Evidence Map (VA ESP Project #05-226)
Washington, DC: US Department of Veterans Affairs; 2016.Coeytaux RR, McDuffie J, Goode A, et al.
Evidence Map of Yoga for High-Impact Conditions
Affecting Veterans (VA ESP Project #09-010)
Washington, DC: US Department of Veterans Affairs; 2014.Kligler B, Bair MJ, Banerjea R, et al.
Clinical policy recommendations from the VHA State-of-the-Art Conference on non-pharmacological approaches to chronic musculoskeletal pain.
J Gen Intern Med. 2018; 33: 16–23.Boehmer KR, Barakat S, Ahn S, et al.
Health coaching interventions for persons with chronic conditions: a systematic review and meta-analysis protocol.
Syst Rev. 2016; 5: 146.Wolever RQ, Simmons LA, Sforzo GA, et al.
A systematic review of the literature on health and wellness coaching: defining a key behavioral intervention in healthcare.
Glob Adv Health Med. 2013; 2: 38–57.Edelman D, Oddone EZ, Liebowitz RS, et al.
A multidimensional integrative medicine intervention to improve cardiovascular risk.
J Gen Intern Med. 2006; 21: 728–734.Gierisch JM, Hughes JM, Edelman D, et al.
The Effectiveness of Health Coaching (VA ESP Project #09-010)
Washington, DC: US Department of Veterans Affairs; 2017.Lee SY, Weiner BJ, Harrison MI, et al.
Organizational transformation: a systematic review of empirical research in health care and other industries.
Med Care Res Rev. 2013; 70: 115–142.Willis CD, Saul J, Bevan H, et al.
Sustaining organizational culture change in health systems.
J Health Organ Manag. 2016; 30: 2–30.Bokhour BG, Fix GM, Mueller NM, et al.
How can healthcare organizations implement patient-centered care? Examining a large-scale cultural transformation.
BMC Health Serv Res. 2018; 18: 168.Lukas CV, Holmes SK, Cohen AB, et al.
Transformational change in health care systems: an organizational model.
Health Care Manage Rev. 2007; 32: 309–320.
Return to OPIOID EPIDEMIC
Return to ALT-MED/CAM ABSTRACTS
Return to CHIROPRACTIC CARE FOR VETERANS
Since 6-20-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |