

Older Adults Who Use Vitamin/Mineral Supplements Differ
from Nonusers in Nutrient Intake Adequacy and Dietary AttitudesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Am Diet Assoc. 2007 (Aug); 107 (8): 1322–1332 ~ FULL TEXT
Rhonda S. Sebastian, MA, Linda E. Cleveland, MS, RD,
Joseph D. Goldman, MA, Alanna J. Moshfegh, MS, RD
US Department of Agriculture,
Agricultural Research Service,
Food Surveys Research Group,
Beltsville, MD 20705, USA.
Rhonda.Sebastian@ars.usda.govOBJECTIVE: To measure nutrient intake adequacy of vitamin/mineral supplement users and nonusers aged 51 years and older, determine the efficacy of supplement practices in compensating for dietary deficits, and identify predictors of supplement use.
DESIGN: Analyses of two 24-hour recalls, demographic variables, and attitude questions collected during the Continuing Survey of Food Intakes by Individuals and Diet and Health Knowledge Survey in 1994 to 1996. Data were weighted to be representative of older Americans.
SUBJECTS: Four thousand three hundred eighty-four adults aged 51 years and older (1,777 daily supplement users, 428 infrequent users, and 2,179 nonusers) residing in households in the United States.
STATISTICAL ANALYSES: Usual nutrient intake distributions were estimated using the Iowa State University method. The Estimated Average Requirement (EAR) cutpoint method was applied to determine the proportion of older adults not meeting requirements before and after accounting for nutrient intake from supplements. Student t tests were used to assess differences between users and nonusers. Logistic regression was used to determine sociodemographic and attitudinal predictors of supplement use.
RESULTS: For one or more of the sex-age groups studied, a significantly smaller proportion of supplement users than nonusers had intakes from food alone below the EAR for vitamins A, B-6, and C; folate; zinc; and magnesium. Even so, less than 50% of both users and nonusers met the EAR for folate, vitamin E, and magnesium from food sources alone. Overall, supplements improved the nutrient intake of older adults. After accounting for the contribution of supplements, 80% or more of users met the EAR for vitamins A, B-6, B-12, C, and E; folate; iron; and zinc, but not magnesium. However, some supplement users, particularly men, exceeded Tolerable Upper Intake Levels for iron and zinc and a small percentage of women exceeded the Tolerable Upper Intake Level for vitamin A. Significant sociodemographic factors related to supplement use for older men were age group, metropolitan area, and educational status. Race, region, smoking status, and vegetarian status were significant factors for women. Attitude about the importance of following a healthful diet was a consistent predictor of supplement use for both men and women.
CONCLUSIONS: A large proportion of older adults do not consume sufficient amounts of many nutrients from foods alone. Supplements compensate to some extent, but only an estimated half of this population uses them daily. These widespread inadequacies should be considered when developing recommendations for supplement use for clients in this age group. Modifying dietary attitudes may result in a higher rate of supplement use in this at-risk population.
From the FULL TEXT Article:
Background
Analyses of nationwide survey data have shown that a large percentage of older adults do not receive recommended amounts of many nutrients from food alone [1–11]. Other measures, such as the Healthy Eating Index, also indicate that the diets of older adults need improvement and may leave them susceptible to nutrition-related problems [12, 13]. This is of particular concern because conditions prevalent in this population, including chronic diseases and absorption problems, can compromise nutritional status [14–16]. At the same time, a growing proportion of older adults are using vitamin and mineral supplements, which can substantially increase nutrient intake and counter some of these shortfalls [17–19]. Little is known about the effectiveness of vitamin/mineral supplements in appropriately compensating for dietary deficits.
With the introduction of the Dietary Reference Intakes (DRIs), new standards are available for the assessment of nutrient intakes. The establishment of Estimated Average Requirements (EARs) makes it possible, for the first time, to estimate the prevalence of nutritional inadequacy in population groups. Additionally, the Tolerable Upper Intake Levels (ULs) provide cutpoints for estimating the percentage of the population of interest that is at potential risk of adverse effects due to overconsumption of a nutrient [20]. These two components of the DRIs provide new opportunities for assessing nutrient intake and evaluating the influence of supplement use on dietary status.
Although supplement use provides potential benefits in increasing nutrient intakes, there are potential drawbacks [21–25]. The extensive use of supplements by older adults increases the possibility for overconsumption of nutrients. The American Dietetic Association’s position paper on food fortification and dietary supplements [26] notes that documented cases of toxicity are often caused by supplementation. In fact, the ULs were developed largely in response to the growing use of supplements and fortified foods [20].
Considering the potential for both positive and negative effects on overall nutrient intake, an important question to ask is what factors influence supplement use. Characteristics associated with taking supplements are well documented. Users generally consume more nutrient- dense diets and vary significantly from nonusers in many sociodemographic factors, including age, sex, race, education status, and income level [17, 27–45]. Research is more limited on the effect of more modifiable factors, such as attitudes about diet and health, on supplement use. The Diet and Health Knowledge Survey, a component of the US Department of Agriculture’s Continuing Survey of Food Intakes by Individuals (CSFII), was designed to provide information about people’s attitudes and knowledge on topics that could affect their dietary intake [46]. Currently, the Diet and Health Knowledge Survey offers the only national survey data that links attitudes about diet and health with dietary behavior, including supplement use.
The purpose of this study was to examine the effects of supplement use on nutrient intake and dietary adequacy for adults aged 51 years and older, and to identify determinants of supplement use. Objectives were to compare the nutrient intake adequacy of older adults who consumed vitamin/mineral supplements daily to those who did not, to estimate the contribution of supplements to total nutrient intake and the associated reduction in nutritional inadequacy, to determine if supplement use creates nutrient intake excesses among older adults, and to identify sociodemographic and attitudinal factors that are predictive of supplement use.
METHODS
Data Source and Sample
Data for this study were drawn from US Department of Agriculture’s 1994–96 CSFII and Diet and Health Knowledge Survey. The CSFII- Diet and Health Knowledge Survey is a nationally representative survey of noninstitutionalized individuals in all 50 states and Washington, DC. A complex multistage, area probability sample design was used to select persons within households. Individuals aged 51 years and older were oversampled. Details of the sample design and methods have been enumerated elsewhere [46]. Dietary intake data were collected using two in-person, interviewer-administered 24–hour recalls conducted 3 to 10 days apart. The Diet and Health Knowledge Survey was administered by telephone to one adult sample person in the household 3 weeks after the second intake interview.
Supplement information was collected through a series of questions following the first 24–hour recall. Two handcards were used to query respondents on the types of vitamin/mineral supplements taken (ie, multivitamin, multivitamin with iron, combination of vitamin C and iron, and single vitamins and/or minerals); and if indicated, what specific types of single vitamins/minerals were consumed (eg, vitamin A, vitamin C, calcium, and iron). The frequency of consumption (taken daily or less often) was also obtained, but not the specific quantity. The amount of each nutrient in the supplement (the formulation) and the brand name were not collected.
Data from the CSFII sample were used to determine nutrient intake adequacy of supplement users and nonusers. Data from the smaller Diet and Health Knowledge Survey sample were used to identify attitudinal and sociodemographic predictors of supplement use. A total of 4,384 respondents aged 51 and older provided two complete 24–hour recalls in the CSFII. Supplement users were defined as individuals who took any kind of vitamin or mineral supplement every day. Almost 10% of the sample (M = 428) was classified as infrequent supplement users and excluded from the analysis. These individuals reported that they took vitamin or mineral supplements “every so often.” The remaining sample of 3,956 supplement users and nonusers was used in assessments of nutrient intake adequacy. The infrequent users were then added back to the sample, and information from the 2,571 respondents aged 51 years and older providing complete responses to the Diet and Health Knowledge Survey attitude questions were used in the analysis to identify predictors of supplement use.
Calculating Nutrient Intake from Foods and Supplements Foods.
Some nutrients required conversion to standardized measurement units before comparison of dietary intakes to the DRIs could be made. Vitamin A had to be converted to retinol activity equivalents, vitamin E to milligrams αtocopherol, and folate to dietary folate equivalents. For vitamins A and E, a special database developed by the US Department of Agriculture, which translated intake estimates of dietary vitamin A from retinol equivalents into retinol activity equivalents and dietary vitamin E from αtocopherol equivalents into milligrams αtocopherol was employed [47]. For folate, the food composition database did not distinguish between the naturally occurring form and the synthetic form (folic acid), so all contributions to folate intake by food were assumed to be the less bioavailable folate form. One microgram converted directly to 1 µg dietary folate equivalent. Because the dietary data for this study were from 1994 through 1996 and widespread fortification of enriched cereal-grain foods with folic acid was not completed until 1998, the underestimation of total folate intake is not as great as it would be if folate fortification had been in place [48–51]. Nonetheless, dietary inadequacy for folate is overestimated to some immeasurable degree.
Supplements. Because brand names and formulations of supplements were not collected in CSFII, assignment of nutritive values for both single nutrient and multivitamin- mineral supplements was based on the nutrient profile of the most frequently reported supplement of that type in the 1999–2000 National Health and Nutrition Examination Survey (NHANES). This is following the procedure used in NHANES when brand and/or formulation were not available [52]. The source of the nutrient values for the supplements was the NHANES Dietary Supplement Database [52]. Before conversions to standardized units could be made for vitamins A and E, and folate, assumptions concerning the form of the nutrient in the supplement were required. Vitamin A in multivitamin- mineral supplements was assumed to be comprised of 60% retinol and 40% beta-carotene, which was the formulation most commonly seen in supplements recorded in the NHANES Dietary Supplement Database. Dietary vitamin A measured in international units was multiplied by 0.30 and beta-carotene by 0.15 to convert to retinol activity equivalents [53]. For vitamin E, the factor of .45 for all-racemic αtocopherols was used for all supplemental sources to convert to milligram αtocopherol units [54]. All supplemental folate was considered to be folic acid, and intake in micrograms was multiplied by 1.7 to convert to dietary folate equivalents [55, 56].
Method for Comparing Intakes to DRIs
To assess the nutrient intake adequacy of groups using the DRIs, an estimate of the usual or long-term intake distribution is needed [20]. For this study, the Iowa State University method, implemented with C-Side software (version 1.02, 1997, Department of Statistics, Iowa State University, Ames), was used to estimate the usual nutrient intake distributions and apply the EAR cutpoint method [57, 58]. Estimates were generated for percentages of individuals below the EAR and above the UL. The proportion of older adults considered to be inadequate for each nutrient was estimated as the percentage whose usual intake fell below the EAR for that nutrient [57].
To account for contributions to nutrient intake from all sources, nutrient values assigned to each type of supplement reported were added to the nutrient intake contributed by food. Because supplement users were defined as those who took supplements every day, the contribution from supplements was applied to both of the dietary intake days. The DRIs used in these analyses were taken from reports of the National Academy of Sciences on vitamin A, iron, and zinc [53]; vitamin C and vitamin E [54]; calcium and magnesium [59]; and vitamin B-6, folate, and vitamin B-12 [55].
Identification of Factors Related to Supplement Use
Sociodemographic variables for this analysis included variables shown in previous studies to be related to supplement use, including sex, age, race, poverty status, and education level [17, 27–31, 33–40, 42, 44]. In addition, two attitude scales, composed of 11 questions each, were derived from Diet and Health Knowledge Survey data. The first scale was developed from questions on perceived adequacy of the respondent’s own diet. Respondents indicated if they believed their diets were too low, too high, or about right in each of 11 nutrients. Higher scores indicated a more favorable assessment of the healthfulness of one’s daily food intake. The second scale measured the importance the respondent placed on following the 1990 Dietary Guidelines for Americans—the most recent government recommendations at the time of CSFII- Diet and Health Knowledge Survey data collection [60]. Higher scores indicated a greater importance placed on incorporating the recommendations into one’s own diet.
Statistical Analyses
The SUDAAN program (version 9.0, 2005, Research Triangle Institute, Research Triangle Park, NC) and SAS (release 8.2, 2001, SAS Institute Inc, Cary, NC) were used for all statistical calculations. Student t tests were conducted to measure for significant differences between supplement users and nonusers in proportions below the EAR for each analyzed nutrient. Dietary intakes of nonusers were tested against the dietary (food only) intake of supplement users; and the total intake of users, including the supplement contribution. A P level of 0.001 was applied to account for the large number of comparisons made.
χ2 analyses were conducted to determine if there were differences in supplement use between men and women, and between age groups.
Logistic regression was performed using the Diet and Health Knowledge Survey sample to identify sociodemographic variables and attitudes associated with the decision to use supplements. Contrasts were done when a variable was significant in the model and the variable had more than two response choices.
RESULTS

Table 1
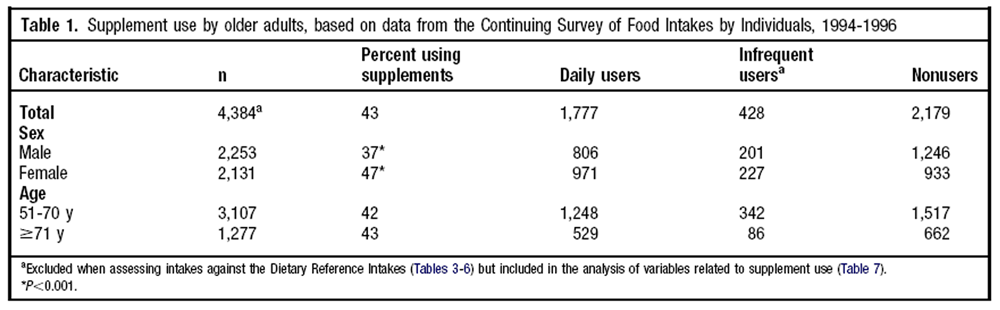
Table 2 Table 1 shows that supplement use was widespread among older adults. In CSFII, 37% of men and 47% of women consumed at least one type of supplement every day. Significant differences were noted between men and women, but not between age groups.
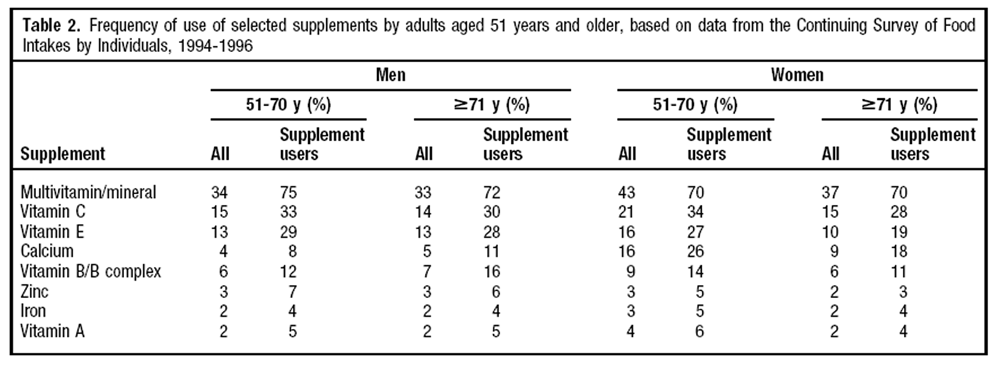
Overall, multivitamin-multimineral supplements were the most frequently reported supplement type for both men and women (Table 2) with 34% of all older men and 41% of all older women taking one. Among all supplement users, 74% of men and 70% of women aged 51 years and older took this type. Vitamin C and vitamin E were the most commonly mentioned single vitamin or mineral supplements with 19% to 34% of respondents reporting use. Calcium supplements were popular among older women; 26% of users aged 51 to 70 years and 18% of users aged 71 years and older took them.
Comparison of Nutrient Adequacy from Food between Users and Nonusers
Table 3
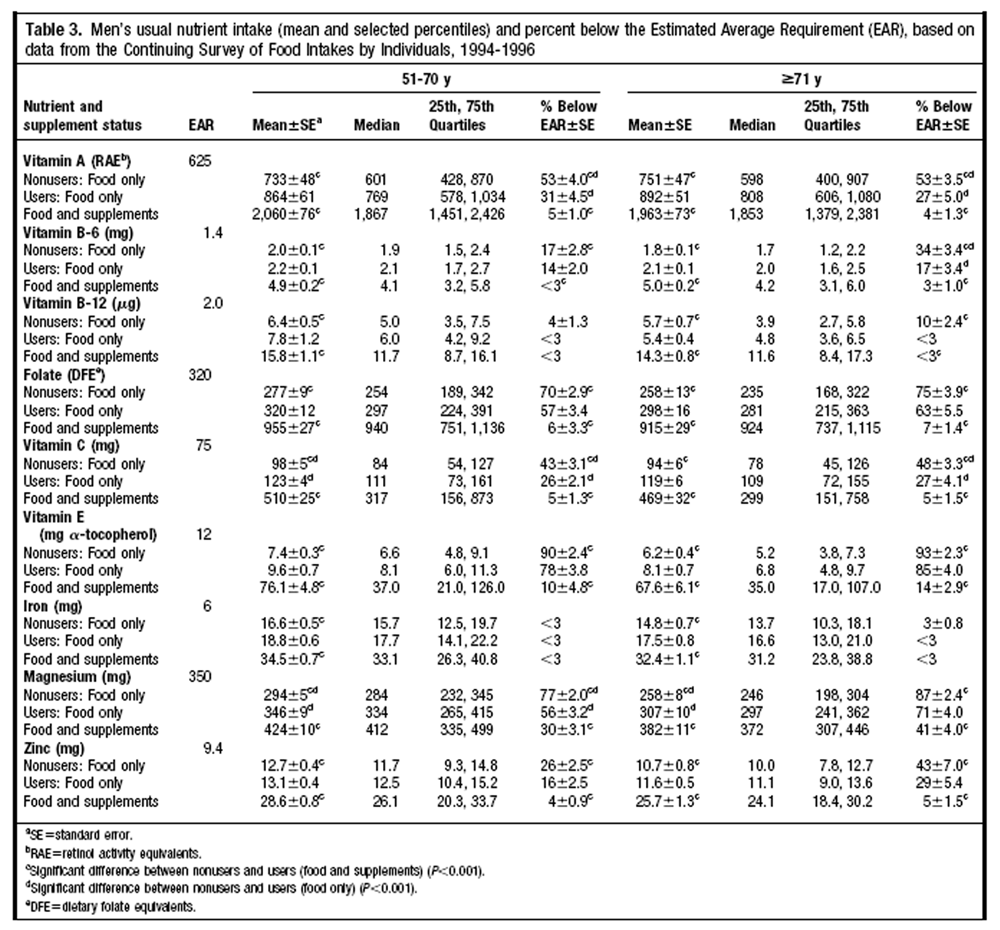
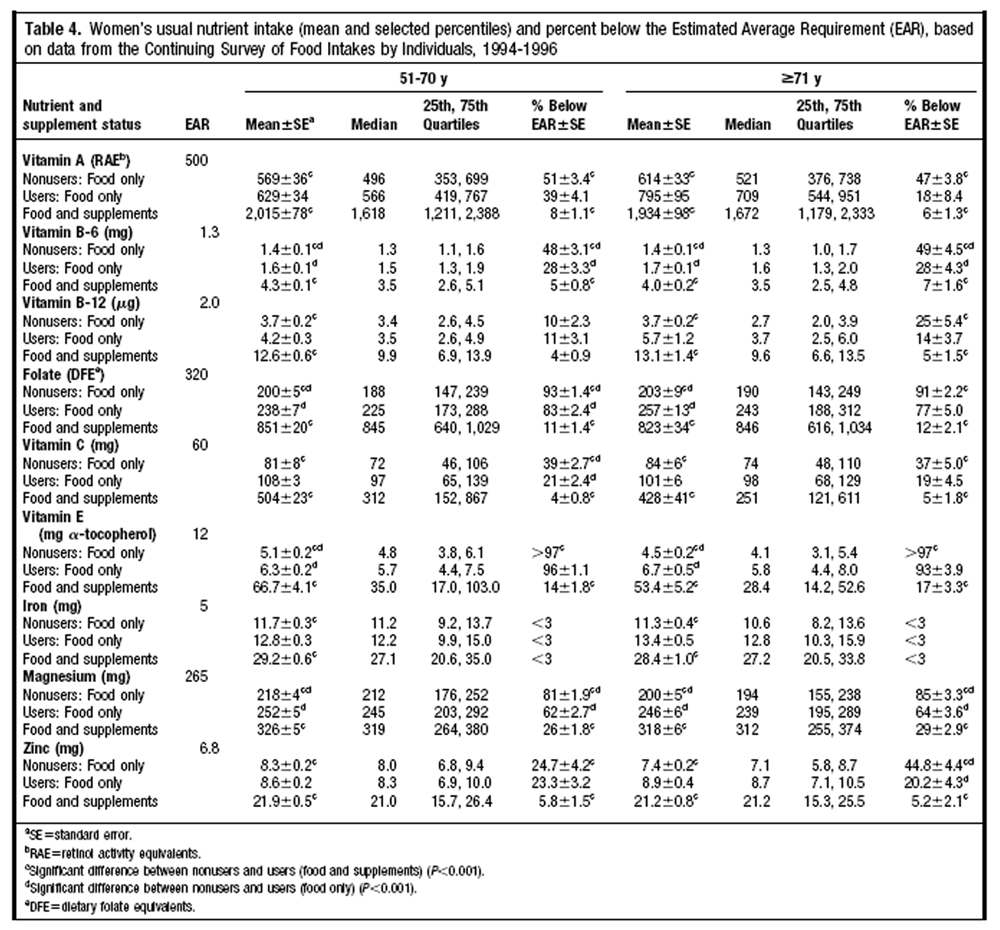
Table 4 Tables 3 and 4 present the mean usual daily nutrient intake and intake at the 25th, 50th, and 75th percentiles for supplement users and nonusers. For supplement users, estimates are presented for intake from food sources only and for the combined intake from both food and supplements. Also shown are percentages of the population with intakes below the EAR (ie, percentages with inadequate intakes). Data are shown separately for men (Table 3) and women (Table 4).
When considering nutrient intake from food sources alone, generally smaller proportions of supplement users than nonusers had inadequate intakes. Intakes of vitamins A and C were significantly higher for users than nonusers in both age groups of men. Vitamin B-6 and magnesium were significantly higher for users as compared to nonusers in both age groups of women. More than 50% of both supplement users and nonusers had inadequate intakes of folate, vitamin E, and magnesium from food. In addition, for most of the sex/age groups studied, more than 25% had inadequate intakes of vitamins A, B-6, and C from food. Iron was the only nutrient studied for which the prevalence of inadequate intakes among older adults was consistently low; 3% or fewer older adults had intakes below the EAR.
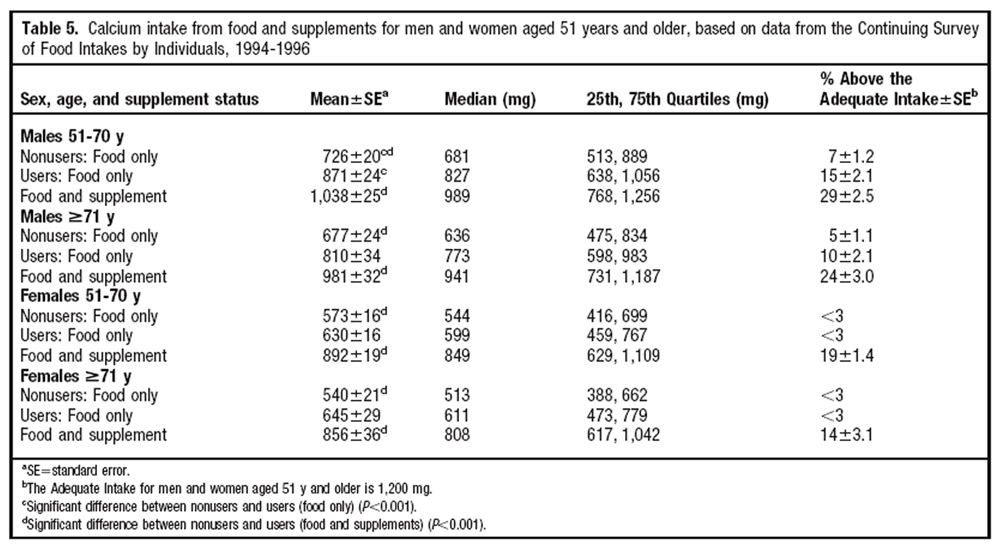
Table 5 It was not possible to determine proportions of the population with inadequate calcium intakes because the DRI is expressed as an Adequate Intake and not as an EAR. Although mean intakes from food alone were higher among supplement users than nonusers (Table 5), the only statistical difference between users and nonusers was among men aged 51 to 70 years. The nutrient intake from food alone was not sufficient to exceed the ULs for any of the nutrients in this analysis. This was true for men and women in both age groups, regardless of supplement use.
Contribution of Supplements to Nutrient Intake
Regular supplement use, in effect, reduced the percentage of older adults with inadequate intakes by at least three fourths for most nutrients (Table 3 and 4). Folate and vitamin E intakes were particularly improved by supplements. Food-only intakes of these nutrients were inadequate for 57% to 96% of supplement users. After accounting for supplements, only 6% to 17% were classified as inadequate.
When the nutrient contribution of supplements was considered, significant differences were found between users and nonusers in percentages with inadequate intakes for nearly all the nutrients studied. Mean intakes of vitamin B-12 and iron were boosted by supplements, but the percent of this population with inadequate intakes was largely unaffected, because most older adults met the EAR from food intake alone. An exception was that significantly more nonuser women aged 71 years and older had inadequate intakes of vitamin B-12 compared to the total intake of supplement users in this sex/age group. Although for the most part the percent meeting the EAR was not significantly increased for vitamin B-12 and iron, supplements did affect intake. Mean intakes from food and supplements for users were significantly different from total intake of nonusers. Supplements more than doubled vitamin B-12 intake for men and women, and this may be of benefit because the absorption of naturally occurring vitamin B-12 may be problematic in older adults [55].
Older men and women who consumed supplements had significantly higher total calcium intakes than nonusers of these products (Table 5). The proportion reaching or exceeding the Adequate Intake increased from 15% to 29% for men aged 51 to 70 years. Large improvements were also found for older women and men aged 71 years and older.
Supplements and Overconsumption of Nutrients
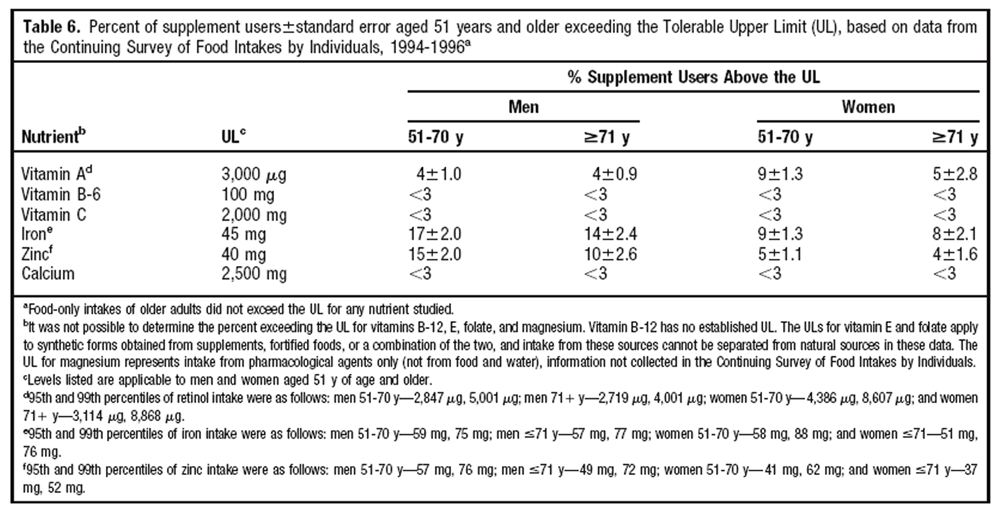
Table 6 Fewer than 3% of men in both age groups had total intakes that exceeded the UL for vitamins B-6, and C, and calcium, indicating that risk of adverse effects from excesses of these nutrients is low in this population group (Table 6). Supplement use did, however, result in intakes that exceeded the ULs for iron and zinc for 10% or more of older men.
Women in both age groups exceeded the UL for iron and zinc, but they did so in smaller proportions than the men. Unique to the women was that a higher proportion (5% to 9%) exceeded the UL for vitamin A than the proportion of men (4%) who did so.
Demographic and Attitudinal Predictors of Supplement Use
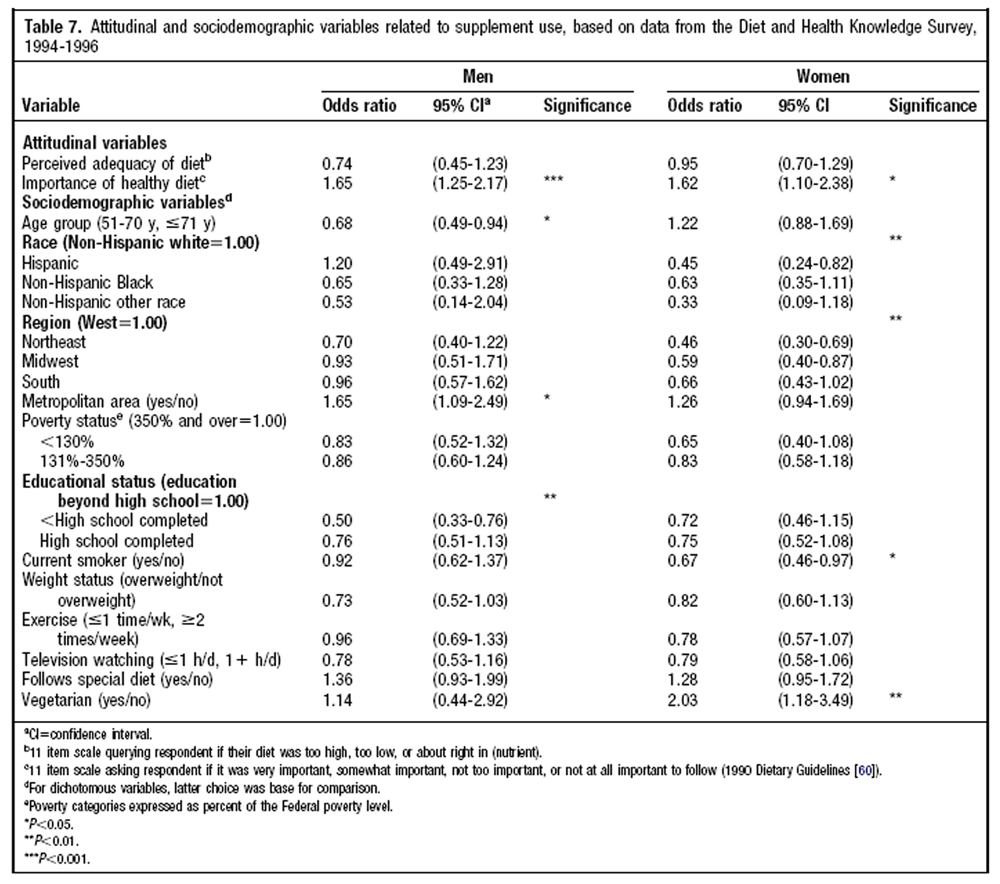
Table 7 Predictors of supplement use were different for older men than for older women (Table 7). Men aged 71 years and older and those living in metropolitan areas were significantly more likely to consume supplements compared to men in the 51– to 70–year age group and those in nonmetropolitan areas, respectively. Education status was also a predictor of supplement use for men. Contrasts showed that significant differences were found between the least educated men (less than high school completion attained) and those with either a high school education or formal education beyond high school. No differences were noted between the two higher education categories. For the women, race, region, smoking status, and vegetarian status were significant predictors of supplement use. White women were more likely to take supplements than all other racial groups combined, and were twice as likely to take supplements as Hispanic women. Residence in the western region of the United States indicated greater prevalence of supplement use than in all other regions together; those in the northeast and midwest were about half as likely to be users. Women who were nonsmokers were more likely to consume supplements than women who smoked, and the small percentage of older women who were vegetarians (4%) were twice as likely to be supplement users as their nonvegetarian counterparts.
Of the two attitude variables included in the logistic regression model, the personal importance of consuming a diet consistent with Dietary Guidelines recommendations was a significant predictor of supplement use. Interestingly, it was also the only factor that was significant for both men and women. Attitudes related to the perception of the adequacy of one’s own diet were not related to supplement use.
DISCUSSION
This study provides estimates of the prevalence of nutrient inadequacies and excesses among older adults, and compares intakes of supplement users and nonusers. The estimates cover total nutrient intake from both foods and supplements. To our knowledge, this is the first study to use DRIs in combination with estimates of usual total nutrient intake to evaluate intakes in this population.
The results are consistent with those from previous studies [27, 32, 38, 40, 41, 43–45] in showing that, generally, supplement users consume more nutritious diets than nonusers. We found that supplement users were more likely to have adequate nutrient intakes from food alone than nonusers for many of the nutrients studied. However, both supplement users and nonusers had large shortfalls in intake from food alone for several nutrients, most notably folate, vitamin E, and magnesium. Supplementation was most beneficial in improving intakes for these nutrients. Nutrients for which little benefit from supplementation was observed were vitamin B-12 (assuming adequate absorption) and iron because most older adults met the EARs from foods alone. Among users, 80% or more met EARs with their total intake for all nutrients studied except magnesium.
The folate estimates here underestimate current intakes because the US Food and Drug Administration did not mandate fortification of grain products until 1998, after data for this study were collected; however, they provide a benchmark for comparison to post-fortification levels. Fortification was expected to add 70 to 130 µg to the daily diet, but subsequent studies have shown that intakes have been increased by 200 µg or more [48, 49, 61, 62]. Based on our study, most older adults would meet adequacy standards if diets provided a net increase of 200 µg/day. Nevertheless, recent analyses using NHANES 2001–2002 data and the accompanying US Department of Agriculture’s Food and Nutrient Database for Dietary Studies 1.0, which accounts for current fortification levels found that depending on the sex/age category, 7% to 21% of older adults still had inadequate intakes from food alone [63]. Further study is needed to determine if folate taken as a dietary supplement should be recommended for this population to improve intake and achieve dietary adequacy.
Most older adults appear to obtain adequate amounts of vitamin B-12 from dietary sources. However, the Institute of Medicine has advised that individuals aged 50 years and older obtain vitamin B-12 from supplemental sources because 10% to 30% of older adults may not be able to absorb the naturally occurring form found in foods [55]. With databases available for these analyses, it was not possible to differentiate between the naturally occurring form and the synthetic form added to fortified foods for estimating intake. In the future, with such a database, research can determine if supplemental vitamin B-12 is needed to meet EARs in addition to the vitamin B-12 typically provided by the food supply.
Supplements boosted total intakes of iron and zinc so that a considerable proportion of older adults, particularly men, exceeded the UL. Due to the adverse effects associated with iron overload and the possibility of its association with coronary heart disease, the Institute of Medicine has recommended that men and postmenopausal women avoid iron supplements and highly fortified foods [53]. Data from this study support those recommendations. In contrast, zinc intake inadequacy before supplementation affected 20% or more of the population. This finding is consistent with other research that has found that older adults, particularly those aged 71 years and older, are the population at greatest risk of zinc intake inadequacy [4, 6, 7, 11, 64, 65]. At the same time, data from this study indicate that approximately 15% of men aged 51 to 70 years and 10% of men aged 71 years and older who are supplement users are exceeding the UL for zinc. Excess consumption of zinc is associated with a risk of reduced copper status, impaired immune response, and lowered plasma high-density lipoprotein cholesterol levels [53]. Supplementation of zinc appears to be needed by a sizable proportion of older men and women, but should be undertaken prudently.
The UL for vitamin A was exceeded by 9% of women aged 51 to 70 years and by 5% of women aged 71 years and older who took supplements. This finding is of concern because long-term vitamin A intake ≥3,000 µg per day has been associated with hip fractures in postmenopausal women [66–68]. Most of the supplemental vitamin A was consumed in a multivitamin/multimineral supplement. An imputed retinol:beta-carotene ratio was used for estimating intake based on the most commonly reported supplement of that type in NHANES 1999–2000. The percentage of women actually consuming vitamin A in levels above the UL, and therefore at risk of adverse effects, may be higher or lower if the particular brands of supplements consumed have a different ratio. Further investigation with more precise data is needed to identify if excess vitamin A intake by supplementation is an issue affecting large numbers of older women.
A secondary objective of the study was to identify characteristics associated with supplement use with particular emphasis on more modifiable factors like attitudes. Whereas sociodemographic factors related to supplement use varied by sex, attitudes about the importance of following a healthful diet consistent with expert recommendations was a significant predictor for both men and women. Those respondents most concerned about their diets and dietary recommendations were more likely to take supplements. These findings suggest that encouraging positive attitudes about a healthful diet in combination with nutrition guidance and appropriate supplement information may result in promoting advantageous use of supplements by this at-risk population.
The fact that the CSFII 1994–1996 is more than 10 years old raises questions as to the applicability of these findings to current dietary adequacy of older adults. However, nutrient intakes from food in this study are comparable to those reported in assessments using the NHANES 2001–2002 data, suggesting that there has been little change in nutrient intake from food during this time period [63]. Using approximate t tests, we investigated changes from 1994 to 1996 to 2001 to 2002 in the percent of the older adult population meeting the EAR for the nutrients included in this study. Except for folate and calcium, no differences were found. Folate intake dramatically increased by more than 200 µg in all of the age/sex groups due to changes in fortification regulations implemented after the data for this study were collected. The mean calcium intake from food increased significantly for men aged 51 to 70 years (611 mg±12 to 874 mg±30) and women aged 51 to 70 years (589 mg±17 to 701 mg±19). Results concerning the other eight nutrients we analyzed should apply now as they do to a decade ago.
Methodologic limitations demand caution be taken in interpreting results from this research. Supplement use was not tied to a specific day of intake, and the validity of applying quantitative intake assessment to frequency data has been questioned [69]. If the supplement information had been collected to match the days of the 24– hour food recalls, it would be better suited to the statistical requirements for intake assessment [69]. Another methodologic limitation is the need for assumptions due to the lack of specificity of the available supplement data. Because brand name information was not collected, estimates were derived using formularies reflecting the composition of the most commonly reported supplement of that type in NHANES 1999–2000. If a respondent did not take the most frequently used product of that type, this imputation may not accurately reflect what nutrients were actually consumed. Moreover, formulations of supplements are changed frequently, and a specific supplement manufactured in 1994 through 1996 may not be identical to the 1999 through 2000 product. In addition, whereas frequency information on supplement use was collected (ie, every day/infrequently/not at all), the quantity of supplements taken was not obtained. Last, supplement use is subject to misreporting. Respondents may not remember any or all the supplements they take or how often they take them. Because of these limitations, the proportions of supplement users meeting EARs and exceeding ULs may be higher or lower than reported in this study. Also absent from these intake data is information on supplements such as antacids and medicinal products that may have been taken and would contribute nutrients. Older adults are heavy consumers of these products [17, 19, 27, 28, 33, 70]. Calcium intake in particular may be underestimated due to lack of data on intake of antacids, which are promoted as calcium supplements and popular among the older population [71].
CONCLUSIONS
Supplements had a positive influence on nutrient adequacy for men and women aged 51 years and older. Whereas dietary modifications to improve intake are paramount, the use of supplements by older adults appears beneficial to attain nutrient adequacy. To avoid exceeding the UL, this population should avoid the routine supplemental intake of certain nutrients including vitamin A in the form of retinol and iron.
The link between dietary attitudes and subsequent behavior, including supplement use, needs further research. Currently there is no attitude data collected in conjunction with dietary information on a nationwide scale [72, 73]. Comprehensive attitude data related to dietary issues needs to be obtained to investigate possible avenues for intervention to encourage healthful behavior.
REFERENCES
US Department of Agriculture.
Table Set 10: Results from USDA’s 1994–96 Continuing Survey of Food Intakes
by Individuals and 1994–96 Diet and Health Knowledge SurveyFord ES, Mokdad AH.
Dietary magnesium intake in a national sample of US adults.
J Nutr. 2003;133:2879-2882.Bell RA, Quandt SA, Spangler JG, Case LD.
Dietary calcium intake and supplement use among older African American, white and Native American women in a rural southeastern community.
J Am Diet Assoc. 2002;102:844-847.Ervin RB, Kennedy-Stephenson J.
Mineral intakes of elderly adult supplement and non-supplement users in the Third National Health and Nutrition Examination Survey.
J Nutr. 2002;32:3422-3427.Fletcher RH, Fairfield KM.
Vitamins for chronic disease prevention in adults: Clinical applications.
JAMA. 2002;287:3127-3129.Briefel RR, Bialostosky K, Kennedy-Stephenson J, McDowell MA, Ervin RB, Wright JD.
Zinc intake of the US population: Findings from the third National Health and Nutrition Examination Survey, 1988- 94.
J Nutr. 2000;130(suppl):1367S-1373S.Cid-Ruzafa J, Caulfield LE, Barron Y, West SK.
Nutrient intakes and adequacy among an older population on the eastern shore of Maryland: The Salisbury Eye Evaluation.
J Am Diet Assoc. 1999;9:564-571.Enns CW, Goldman JD, Cook A.
Trends in food and nutrient intakes by adults: NFCS 1977-78, CSFII 1989-91, and CSFII 1994-95.
Fam Econ Nutr Rev. 1997;10:16-31.Dietary Intake of Vitamins, Minerals, and Fiber of Persons Ages 2 Months and Over in the United States:
Third National Health and Nutrition Examination Survey, Phase 1, 1988-91.
Hyattsville, MD: National Center for Health Statistics; 1994.
Advance data from Vital and Health Statistics, No. 258.Bialostosky K, Wright J. Kennedy-Stephens J, McDowell M, Johnson C.
Dietary intake of macronutrients, micronutrients and other dietary constituents: United States 1988-94.
Vital Health Stat 11. 2002;245: 1-158.Hallfrisch J, Muller DC.
Does diet provide adequate amounts of calcium, iron, magnesium, and zinc in a well-educated population?
Exp Gerontol. 1993;28:473-483.Juan WY, Lino M, Basiotis PP.
Quality of Diets of Older Americans. Alexandria, VA: Center for Nutrition Policy and Promotion; 2004.
Nutrition Insight 29.Finke MS, Huston SJ.
Healthy Eating Index scores and the elderly.
Fam Econ Nutr Rev. 2003;15:67-73.Chandra RK.
Impact of nutritional status and nutrient supplements on immune responses and incidence of infection in older individuals.
Ageing Res Rev. 2004;3:91-104.Fairfield KM, Fletcher RH.
Vitamins for chronic disease prevention in adults: Scientific review.
JAMA. 2002;287:3116-126.Russell RM.
Factors in aging that effect the bioavailability of nutrients.
J Nutr. 2001;131(suppl 4):S1359-S1361.Millen AE, Dodd KW, Subar AF.
Use of vitamin, mineral, nonvitamin, and nonmineral supplements in the United States:
The 1987, 1992, and 2000 National Health Interview Survey Results.
J Am Diet Assoc. 2004;104:942-950.Briefel RR, Johnson CL.
Secular trends in dietary intake in the United States.
Annu Rev Nutr. 2004;24:401-431.Messerer M, Johanasson SE, Wolk A.
Use of dietary supplements and natural remedies increased dramatically during the 1990s.
J Intern Med. 2001;250:160-166.Institute of Medicine, Food and Nutrition Board.
Dietary Reference Intakes: Applications in Dietary Assessment.
Washington, DC: National Academies Press; 2000.Bjelakovic G, Nikolova D, Simonetti RG, Gluud C.
Antioxidant supplements for prevention of gastrointestinal cancers: A systematic review and meta-analysis.
Lancet. 2004;364:1219-1228.Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, Keogh JP.
Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease.
N Engl J Med. 1996; 334:1150-1155.Herbert V, Shaw S. Jayatilleke E, Stopler-Kasdan T.
Most free-radical injury is iron-related: It is promoted by iron, hemin, holoferritin and vitamin C, and inhibited by deferoxamine and apoferritin.
Stem Cells. 1994;12:289-303.Nelson RL, Davis FG, Sutter E, Sobin LH, Kikendall JW, Bowen P.
Body iron stores and risk of colonic neoplasia.
J Natl Cancer Inst. 1994;86:455-460.Cook JD, Dassenko SA, Whittaker P.
Calcium supplementation: Effect on iron absorption.
Am J Clin Nutr. 1991;53:106-111.Position of The American Dietetic Association:
Food fortification and dietary supplements.
J Am Diet Assoc. 2001;101:115-125.Archer SJ, Stamler J, Moag-Stahlberg A, Van Horn L, Garside D, Chan Q.
Association of dietary supplement use with specific micronutrient intakes among middle-aged American men and women: The INTERMAP Study.
J Am Diet Assoc. 2005;105: 1106-1114.Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF.
Dietary supplement use by US adults: Data from the National Health and Nutrition Examination Survey, 1999-2000.
Am J Epidemiol. 2004;160:339-349.De Jong N.
Demographic and lifestyle characteristics of functional food consumers and dietary supplement users.
Br J Nutr. 2003;89: 273-281.Foote JA, Murphy SP, Wilkens LR, Hankin JH, Henderson BE, Kolonel LN.
Factors associated with dietary supplement use among healthy adults of five ethnicities: The Multiethnic Cohort Study.
Am J Epidemiol. 2003;157:888-897.Satia-Abouta J, Kristal AR, Patterson RE, Littman AJ, Stratton KL, White E.
Dietary supplement use and medical conditions: the VITAL study.
Am J Prev Med. 2003;24:43-51.Beitz R, Mensink GB, Fischer B, Thamm M.
Vitamins—Dietary intake and intake from dietary supplements in Germany.
Eur J Clin Nutr. 2002;56:539-545.Troppmann L, Johns T, Gray-Donald K.
Natural health product use in Canada.
Can J Pub Health. 2002;93:426-430.Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE.
Americans’ views on the use and regulation of dietary supplements.
Arch Intern Med. 2001;161:805-810.Balluz LS, Kieszak SM, Philen RM, Julinare J.
Vitamin and supplement use in the United States: Results from the third National Health and Nutrition Examination Survey.
Arch Fam Med. 2000;9:258-262.Messerer M, Johansson SE, Wolk A.
Sociodemographic and health behaviour factors among dietary supplement and natural remedy users.
Eur J Clin Nutr. 2000;55:1104-1110.Ervin RB, Wright JD, Kennedy-Stephenson J.
Use of dietary supplements in the United States, 1988-94.
Vital Health Stat 11. 1999;244: i-iii, 1-14.Kirk SF, Cade, JE, Barrett JH, Conner M.
Diet and lifestyle characteristics associated with dietary supplement use in women.
Public Health Nutr. 1999;2:69-73.Nayga RM, Reed DB.
Factors associated with the intake of dietary supplements.
Fam Econ Nutr Rev. 1999;12:43-48.Lyle BJ, Mares-Perlman JA, Klein BE, Klein R, Greger JL.
Supplement users differ from nonusers in demographic, lifestyle, dietary and health characteristics.
J Nutr. 1998;128:2355-2362.Patterson RE, Neuhouser ML, White E, Hunt JR, Kristal AR.
Cancer related behavior of vitamin supplement users.
Cancer Epidemiol Biomarkers Prev. 1998;7:79-81.Eliason BC.
Dietary supplement users: Demographics, product use, and medical system interaction.
J Am Board Fam Pract. 1997;10:265-271.Houston DK, Johnson MA, Daniel TD, Poon LW.
Health and dietary characteristics of supplement users in an elderly population.
Int J Vitam Nutr Res. 1997;67:183-191.Slesinski MJ, Subar AF, Kahle LL.
Dietary intake of fat, fiber and other nutrients is related to the use of vitamin and mineral supplements in the United States: The 1992 National Health Interview Survey.
J Nutr. 1996;126:3001-3008.Looker A, Sempos, CT, Johnson C, Yetley EA.
Vitamin-mineral supplement use: Association with dietary intake and iron status of adults.
J Am Diet Assoc. 1988;88:808-814.Tippett KS, Cypel, YS, eds.
Design and Operation: The Continuing Survey of Food Intakes by Individuals
and the Diet and Health Knowledge Survey, 1994-96.
Beltsville, MD: US Department of Agriculture,
Agriculture Research Service; 1988. Nationwide Food Surveys Report No. 96-1.USDA Database of Vitamin A (mcg RAE) and Vitamin E (mg AT) for National Health and Nutrition Examination Survey 1999-2000.
Beltsville, MD: Agricultural Research Service, Food Surveys Research Group; 2006.Quinlivan EP, Gregory JF.
Effect of food fortification on folic acid intake in the United States.
Am J Clin Nutr. 2003;77:221-225.Lewis CJ, Crane NT, Wilson DB, Yetley EA.
Estimated folate intakes: Data updated to reflect food fortification, increased bioavailability, and dietary supplement use.
Am J Clin Nutr. 1999;70:198-207.Food standards; amendment of standards of identity for enriched grain products to require addition of folic acid, final rule. 61
Federal Register 8781-8897 (1996).Food additives permitted for direct addition to food for human consumption; folic acid (folacin), final rule. 61
Federal Register 8797-8807 (1996).National Center for Health Statistics.
National Health and Nutrition Examination Survey 1999-2000 Dietary Supplement Data Release.
http://www.cdc.gov/nchs/about/major/nhanes/quest99_00.htmInstitute of Medicine, Food and Nutrition Board.
Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc.
Washington, DC: National Academies Press; 2001.Institute of Medicine, Food and Nutrition Board.
Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids.
Washington, DC: National Academies Press; 2000.Institute of Medicine, Food and Nutrition Board.
Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline.
Washington, DC: National Academies Press; 2000.Suitor CW, Bailey LB.
Dietary folate equivalents: Interpretation and application.
J Am Diet Assoc. 2000;100:88-94.Carriquiry AL.
Assessing the prevalence of nutrient inadequacy.
Public Health Nutr. 1999;2:23-33.Nusser SM, Carriquiry AL, Dodd KW, Fuller WA.
A semiparametric transformation approach to estimating usual daily intake distributions.
J Am Stat Assoc. 1996;91:1440-1449.Institute of Medicine, Food and Nutrition Board.
Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride.
Washington, DC: National Academies Press; 1997.US Department of Agriculture, US Department of Health and Human Services.
Nutrition and Your Health: Dietary Guidelines for Americans. 3rd ed. 1990.
ashington, DC: Home and Garden Bulletin No. 232.Choumenkovitch SF, Selhhub J, Wilson PWF, Rader JI, Rosenberg IH, Jacques PF.
Folic acid intake from fortification in United States exceeds predictions.
J Nutr. 2002;132:2792-2798.Honein MA, Paulozzi LJ, Mathews TJ, Erickson JD, Wong LC.
Impact of folic acid fortification of the US food supply on the occurrence of neural tube defects.
JAMA. 2001;285:2981-2986.Moshfegh AM, Goldman JD, Cleveland L.
What We Eat in America, NHANES 2001-2002:
Usual Nutrient Intake from Food Compared to Dietary Reference Intakes.
Washington, DC: US Department of Agriculture, Agricultural Research Service; 2005.Ma J, Betts NM.
Zinc and copper intakes and their major food sources for older adults in the 1994-96 Continuing Survey of Food Intakes by Individuals (CSFII).
J Nutr. 2000;133:2838-2843.Bales CW, DiSilvestro RA, Currie KL, Plaisted CS, Joung H, Galanos AN, Lin PH.
Marginal zinc deficiency in older adults: Responsiveness of zinc status indicators.
J Am Coll Nutr. 1994;13:455-462.Feskanich D, Singh V, Willett WC, Colditz GA.
Vitamin A intake and hip fractures among postmenopausal women.
JAMA. 2002;287:47-54.Promislow JHE, Goodman-Gruen D, Slymen DJ, Barrett-Connor E.
Retinol intake and bone mineral density in the elderly: The Rancho Bernardo study.
J Bone Miner Res. 2002;17:1349-1358.Melhus H, Michaelsson, K, Kindmark A, Bergstrom R, Holmberg L, Mallmin H, Wolk A, Ljunghall S.
Excessive dietary intake of vitamin A is associated with reduced bone mineral density and increased risk of hip fracture.
Ann Intern Med. 1998;129:770-778.Carriquiry AL.
Estimation of usual intake distributions of nutrients and foods.
J Nutr. 2003;133(suppl):601S-608S.Wold RS, Lopez ST, Yau L, Butler LM, Pareo-Tubbeh SL, Water DL, Garry PJ, Baumgartner RN.
Increasing trends in elderly persons’ use of nonvitamin, nonmineral dietary supplements and concurrent use of medications.
J Am Diet Assoc. 2005;105:54-63.Radimer KL, Subar AF, Thompson FE.
Nonvitamin, nonmineral dietary supplements: Issues and findings from NHANES III.
J Am Diet Assoc. 2000;100:447-454.Murphy, SP.
Collection and analysis of intake data from the intergrated survey.
J Nutr. 2003;133(suppl):585S-589S.Dwyer J, Picciano MF, Raiten DJ, Members of the Steering Committee, National Health and Nutrition Examination Survey.
Collection of food and dietary supplement intake data: What We Eat in America - NHANES.
J Nutr. 2003;133(suppl):590S-600S.
Return to NUTRITION
Return to SENIOR CARE
Since 8–01–2017
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |