

An Electronic Parent Reported Infant Outcome Measure
in Chiropractic Clinics: A Feasibility StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2017 (Sep); 16 (1): 1355–1361 ~ FULL TEXT
OPEN ACCESS Heather Anne Hanson DC, MSc and Joyce Elaine Miller BS, DC, PhD
AECC University College,
Bournemouth, United KingdomBackground: The United Kingdom Infant Questionnaire (UKIQ) is a validated and reliable parent reported outcome measure based on common public health issues and presenting complaints of infancy. The UKIQ is proposed as a pragmatic tool for research purposes and an electronic version might be advantageous for large-scale data collection in chiropractic clinics.
Study objectives: The primary objective of this study was to test the feasibility of an electronic version of an infant outcomes instrument. To this end, feasibility benchmarks were set based on technical performance and acceptance of the tool by its users, chiropractic offices and mothers.
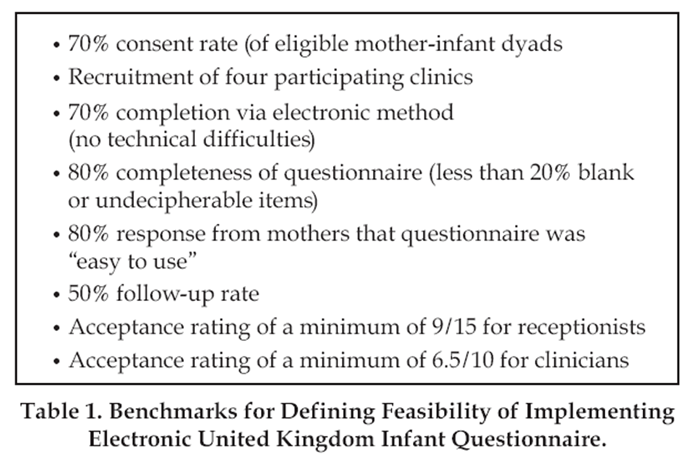
Materials and methods: In this prospective, multi-center observational study, mothers of infants (0-12 months) were asked to complete the electronic UKIQ at initial presentation and at follow-up in chiropractic clinics in the United Kingdom. Technical issues encountered and rates of non-consent were tracked during the study period. Feasibility benchmarks included the following: recruitment of four participating clinics, a minimum of 70% maternal consent to participation, 80% completeness of data, 80% response from mothers that the questionnaire was “easy to use” and a follow-up rate of 50%. Participating chiropractors and receptionists were asked for feedback and ratings of their experience with the tool. Additionally, clinics who showed interest in participating but did not participate were asked to provide feedback in order to elucidate barriers to implementation.
Results: During the testing period, 100 intake and 46 follow-up forms were completed. All feasibility benchmarks were achieved, except for follow-up rate (46%) and lower than anticipated participation of recruited clinics (n=2). No technical difficulties prevented mothers from completing the form and collected data had a high rate of completeness with <0.03% missing data for standard questions and no undecipherable answers. No incidents of maternal non-consent occurred and 98.9% of mothers found the tool easy to use. Clinicians and receptionists rated their experience with the tool highly (mean 5/5 for clinician perception of clinical utility and likelihood of continued use and mean 4.5/5 for receptionist’s ease of administering and 5/5 for receptionist perception of willingness of mothers to complete and ease with which mothers completed the questionnaire).
Conclusions: This tool is technically capable of large-scale data collection and well-accepted by users. However, implementation of the instrument in private chiropractic clinics was lower than anticipated. Future research must investigate methods to improve uptake of key outcomes instruments in chiropractic practices.
From the FULL TEXT Article:
Introduction
Recently, a parent-reported outcome measure based on common public health issues and features of infant life has been developed and found to be valid and reliable. [1] This questionnaire is referred to as the United Kingdom Infant Questionnaire (UKIQ), and was designed to capture information about an infant’s complaints and maternal concerns across various domains including maternal impressions of feeding, sleeping and crying behaviors, comfort in the supine position, cervical range of motion and “tummy time.” [1] Additionally, it enquires about the mother’s mental state, which may be of relevance clinically due to its recognized impact on infant health outcomes. [2, 3]
Historically, patient-reported outcome measures (PROMs) have mainly been implemented for research purposes. [4] However, their application in clinical practice is becoming more common for monitoring patient progress and quantifying response to treatment. Additionally, PROMs have become recognized as tools for improving communication between clinicians and patients and aiding shared decision making. [5] The use of PROMs in infant care has lagged behind, not least because the infant cannot complete their own questionnaires.
Though infants are disproportionately frequent users of chiropractic care [6-8] the chiropractic profession has been the object of criticism for a lack of high quality research supporting its treatment of this population. [9-11] A valid and reliable outcome measure is a key requirement for conducting high quality clinical research and the UKIQ could meet the need for a patient-centered tool for research of chiropractic care for infants. [1]
An electronic version of such a measure might be particularly useful. Some evidence suggests that patients prefer electronic methods for collecting information to paper methods [12] particularly in younger populations [13] and that use of electronic methods may improve completion rates when using PROMs. [14, 15] An electronic version of this tool could circumvent the substantial logistic and administrative challenges involved in paper-based collection of PROMs. [16]
The use of electronic PR0Ms for adult patients in chiropractic clinical practice has been shown to be feasible. [17] An electronic version of the UKIQ seems theoretically well-suited to the collection of data from large populations. However, it would need to be adopted by chiropractors in practice in order for it to be effectively used for this purpose and it is possible that certain factors might impede widespread adoption. In particular, clinician perception of an outcome measure’s clinical value and ease of use have been suggested as important factors for the successful routine implementation of outcome measures in addition to good organizational and administrative support. [16, 18]
This study’s primary objective was the investigation of the feasibility of using an electronic version of the previously validated UKIQ widely across chiropractic care.
Methods
This was a prospective, multi-center observational study conducted during October and November, 2016, in the United Kingdom. The infant clinic within the Anglo-European College of Chiropractic and four other private chiropractic clinics were recruited for participation. Ethical approval was granted by the Anglo-European College of Chiropractic Research Ethics Sub-Committee.

Table 1 Feasibility benchmarks were set a priori (Table 1). While arbitrarily determined, these benchmarks were thought to be realistic indicators of user acceptance and the technical feasibility of widespread use of this tool.
Participating clinics were required to have access to their own hand-held device for completion of the questionnaire. All mothers presenting their infant (0-12 months) for treatment and/or examination for the first time were eligible for inclusion. Exclusion criteria included mothers presenting a child over one year of age, who did not speak English or were intellectually incapable of providing consent to participation and infants being presented by someone other than the mother. Mothers younger than 16 years of age were also ineligible for inclusion. Clinics were asked to track instances in which mothers did not consent to participation or were unable to provide consent.
The electronic UKIQ was completed during patient registration in the reception area to prevent interaction with the clinician from influencing responses. The questionnaire was completed in a web browser and data was subsequently entered into an Excel™ worksheet on a web server in encrypted form using SSL technology. All data was password protected. Formstack® provided the services for this project. A follow-up questionnaire was completed in a similar fashion at the fourth visit or when deemed clinically appropriate by the treating chiropractor. Chiropractors were allowed to use their discretion in determining appropriate timing of follow-up, but were given the guidance that this should take place when they thought that clinically significant change (improvement or worsening) had occurred. In cases where patients were discharged or parents decided to discontinue care, the questionnaire was provided at the last visit even if this was prior to the fourth visit. No follow-up was pursued in cases that were referred to another professional without treatment given at the first visit or in cases where care was discontinued without the follow-up being completed at the last visit.
All data were collected anonymously and analyzed in pooled form. Infant gender and age in weeks were collected due to their clinical relevance, but no other identifying data were obtained.
Clinics were encouraged to contact the lead researcher with any problems encountered and to log any occurrence of technical issues preventing online completion. Additionally, clinics that did not actually implement the electronic UKIQ during the study period despite initial enrolment were contacted for their feedback, specifically regarding any barriers to implementation. At the close of the study, one chiropractor and one receptionist from each participating clinic were asked to complete a questionnaire in order to rate their experience in using the electronic UKIQ.
Results
100 intake questionnaires and 46 follow-up questionnaires were completed during the study period. The follow-up rate of 46% (46/100) therefore did not meet the predetermined feasibility benchmark. There were no cases of maternal refusal to participate, maternal inability to consent or an infant being presented by someone other than the mother.
No incidents of a logistic or technical issue preventing online completion of the questionnaire were noted. Data were incomplete for 0.1% of standard questions on the intake questionnaire and 0.9% of standard questions on the follow-up questionnaire, representing a rate of less than 0.3% for all standard questions. For items that could be answered with “other,” 2.6% (13/500) were left unspecified by the mothers on the intake. Therefore, the feasibility benchmark of more than 80% completeness of data was achieved. One incident was recorded in which the “submit” button was not hit and some loss of data occurred, but there was no indication that his had occurred more often.
All mothers consented to participation and most responded that they found the questionnaire easy to use (97/98=98.9%), indicating a satisfactory level of maternal acceptance of the tool.
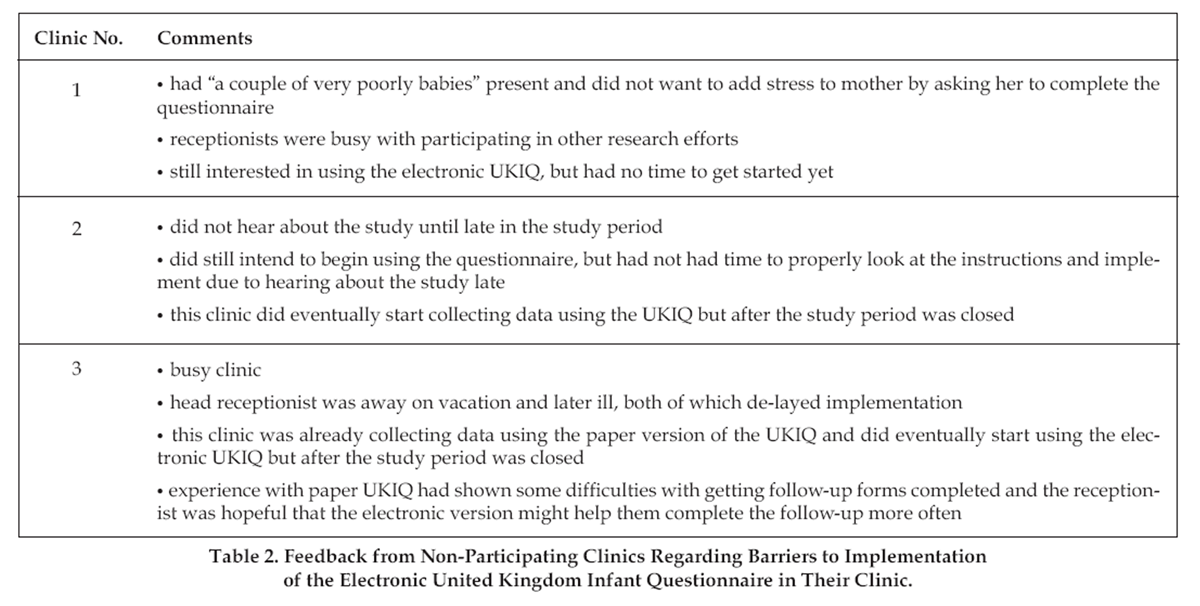
Table 2 Five clinics initially enrolled in the study, but only two of these implemented the electronic UKIQ during the study period. Feedback from non-participating clinics is summarized in Table 2, but all clinics indicated time constraints as an issue in implementing the electronic questionnaire. Two of these clinics began using the questionnaire after the study period was complete.
Participating chiropractors and administrative staff rated their acceptance of the questionnaire highly. Clinical usefulness and likelihood of continued use were both rated at 5/5 by clinicians. Administrative staff provided the following mean ratings: 4.5/5 for ease of administering using a hand-held device, 5/5 for willingness of mothers to complete and 5/5 for perceived ease with which the mothers completed the online questionnaire.
Discussion
All feasibility benchmarks were met, with the exception of lower than anticipated clinic participation and follow-up rate. These findings indicate that this electronic tool possesses the technical features necessary for widespread implementation and that it is well-accepted by its users: mothers, chiropractors and administrative staff.
The low follow-up rate may be partially attributable to the short study period, as it is possible that some infants were not far enough in the treatment process to warrant completion of a follow-up questionnaire at the close of the study. However, this finding brings to light an area that warrants attention in future studies using the UKIQ.
The main barriers to widespread implementation encountered during this feasibility study appear to be related to shortage of time and high workload of clinicians and administrative staff. The low follow-up rate is likely also a reflection of these issues. This is unsurprising, as workload is commonly cited in the literature as an impediment to the implementation of routine use of PROMs [16, 19] and the initial phase of implementation of such outcome measures is recognized as being particularly problematic. [20] The short study period likely served to highlight this issue.
Utilization of PROMs in research on chiropractic care of infants is congruent with the current trend in growing use of PROMs by governments and government agencies in evaluating and attempting to improve healthcare and therefore, it seems that endeavors to overcome barriers to implementation are worthwhile. Future research efforts using the electronic UKIQ might consider ways in which additional support can be offered during the implementation phase and a longer study period.
Evidence suggests that clinician perception that PROM use leads to improved patient care will foster clinician acceptance and utilization, while perception that a PROM is only useful for research purposes tends to hinder clinician acceptance. [16] While clinical utility and likelihood of future use was rated highly by the participating chiropractors, recruitment efforts focused mainly on the need for better quality research in the area of pediatric chiropractic care. Shifting the focus towards the clinical utility of this tool and the known benefits of PROMs in improving patient satisfaction with care and even patient outcomes [5, 21] might boost future efforts at recruiting participating chiropractors.
Chiropractors working in private practice generally do not receive compensation for non-clinical activities like research. Even in settings like academic hospitals, where research efforts are given priority, a need to support and provide incentive for clinicians to participate in research has been noted in the literature. [22] Overcoming this lack of incentives will continue to be challenging when attempting research involving private chiropractic clinics.
Conclusion
Most feasibility benchmarks were met during the study period, suggesting that the electronic UKIQ possesses the necessary technical features for widespread use. However, lower than expected clinic participation and completion of follow-up were encountered. Future research efforts might look to the identified barriers in attempts to improve participation rates.
References:
Miller AS, Huizinga B, Pinkster M, Telford ACJ, ten Heggeler JM, Miller JE.
Development and Testing of a Multidimensional Parent Reported Outcome Measure
for Common Presenting Complaints of Infancy: The UK Infant Questionnaire
Journal of Clinical Chiropractic Pediatrics 2016; 15(3):1292-1300Fallon V, Groves R, Halford JCG, Bennett KM, Harrold JA.
Postpartum Anxiety and Infant-Feeding Outcomes: A Systematic Review.
J Human Lact 2016; 32(4):740-758.Ni PK, Siew Lin SK.
The role of family and friends in providing social support towards enhancing the wellbeing of
postpartum women: a comprehensive systematic review.
JBI Libr Sys Rev 2011;9(10):313-370.Black N, Burke L, Forrest CB, Sieberer UHR, Ahmed S, Valderas JM, Bartlett SJ, Alonso J.
Patient-reported outcomes: pathways to better health, better services, and better societies.
Qual Life Res 2016; 25(5):1103-111.Valderas JM, Kotzeva A, Espallargues M, Guyatt G, Ferrans CE, Halyard MD, Revicki DA, Symonds ET.
The impact of measuring patient-reported outcomes in clinical practice:
a systematic review of the literature.
Qual Life Res 2008; 17(1):179-193.Hestbaek L, Jřrgensen A, Hartvigsen J.
A Description of Children and Adolescents in Danish Chiropractic Practice:
Results from a Nationwide Survey
J Manipulative Physiol Ther. 2009 (Oct); 32 (8): 607–615Miller J.
Demographic Survey of Pediatric Patients Presenting to
a Chiropractic Teaching Clinic
Chiropractic & Osteopathy 2010 (Dec 15); 18: 33Allen-Unhammer A, Willson FJH, Hestbaek L.
Children and adolescents presenting to chiropractors in Norway:
National Health Insurance data and a detailed survey.
Chiropr Man Therap 2016; 24;29-38.Ernst E.
Chiropractic spinal manipulation for infant colic: a systematic review of randomised clinical trials.
Int J Clin Pract 2009; 63 (9):1351-1353.Gotlib, A and Rupert, R.
Chiropractic Manipulation in Pediatric Health Conditions - An Updated Systematic Review
Chiropractic & Osteopathy 2008 (Sep 12); 16: 11Bronfort G, Haas M, Evans R, Leiniger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Kania-Richmond A, Weeks L, Scholten J, Reney M.
Evaluating the feasibility of using online software to collect patient information in a
chiropractic practice-based research network.
J Can Chiropr Assoc 2016; 60(1):93-105.Suzuki E, Mackenzie C, Sanson-Fischer R, Carey M, D’Este C, Asada H, Toi M.
Acceptability of a Touch Screen Tablet Psychosocial Survey Administered to Radiation Therapy Patients in Japan.
Int J Behav Med 2016; 23(4):485-491.Roberts N, Bradley B, Williams D.
Use of SMS and tablet computer improves the electronic collection of elective orthopaedic
Patient Reported Outcome Measures.
Ann Roy Coll of Surg Eng 2014; 96:348-351.Malhotra K, Buraimoh O, Thornton J, Cullen N, Singh D, Goldberg AJ.
Electronic capture of patient-reported and clinician-reported outcome measures in an elective
orthopaedic setting: a retrospective cohort analysis.
BMJ Open 2016; 6:e011975.Boyce MB, Browne JP.
Does providing feedback on patient-reported outcomes to healthcare professionals result in better
outcomes for patients? A systematic review.
Qual Life Res 2013; 22(9):2265-2278.Newell D, Diment E, Bolton, J.
An Electronic Patient-Reported Outcome Measures System in UK Chiropractic Practices:
A Feasibility Study of Outcomes and Costs.
J Manipulative Physiol Ther 2016; 39(1);31-41.Duncan AS, Murray J.
The barriers and facilitators to routine outcome measurement by allied health professionals
in practice: a systematic review.
BMC Health Serv Res 2012; 12:96.Hughes R, Aspinal F, Addington JM, Dunckley M, Faull C, Higginson I.
It just didn’t work: the realities of quality assessment in the English health care context.
Int J Nurs Stud 2004; 41:(7)704-712.Dunckley M, Aspinal F, Addington-Hall J, Hughes R, Higginson I.
A research study to identify facilitators and barriers to outcome measure implementation.
Int J of Palliat Nurs 2005; 11(5):218-225.Boyce MB, Browne JP.
Does providing feedback on patient-reported outcomes to healthcare professionals result in
better outcomes for patients?
A systematic review. Qual Life Res 2013; 22:2265-2278.Embi PJ, Tsevat J.
The Relative Research Unit: Providing Incentives for Clinician Participation in Research Activities.
Acad Med 2012; 87(1):11-14.
Return to PEDIATRICS
Since 7-03-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |