

Low Back and Pelvic Girdle Pain of Pregnancy:
Recommendations for Diagnosis
and Clinical ManagementThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2010 (Dec); 11 (2): 775—779 ~ FULL TEXT
OPEN ACCESS Maria C. Browning, BSc, DC, MSc
Clinical tutor,
Anglo-European College of Chiropractic, UK.Introduction: Low back and pelvic girdle pain are common and disabling conditions during pregnancy. Chiropractors are in a unique position to diagnose various pain syndromes with reliable clinical tests and offer a variety of treatments that are safe for both mother and fetus.
Objective: This paper explores the current evidence base on low back and pelvic girdle pain of pregnancy with recommendations for diagnosis and clinical management.
Discussion: Clinical tests used by chiropractors are reliable and a number of treatment techniques are available for the different low back and pelvic girdle pain syndromes of pregnancy.
Conclusion: Treating the pregnant patient can be challenging and it is realistic for the goal to be supportive care and keeping quality of life static due the constantly changing dynamics of pregnancy.
Key words: chiropractic, pelvic girdle pain, low back pain, symphysis pubis dysfunction
Introduction
Pregnancy should be a joyful time but can quickly turn into a miserable experience for women who have back or pelvic girdle pain and their quality of life can be seriously affected. This article will explore the validity of clinical tests, manual therapy techniques and exercises for low back pain (LBP) and pelvic girdle pain (PGP) in pregnancy in order to maintain optimal function.
Discussion
LBP is usually defined by pain between the 12th rib and the gluteal fold, whilst pelvic girdle pain is defined as pain experienced between the posterior iliac crest and the gluteal fold, particularly in the vicinity of the sacroiliac joints. The pain may radiate in the posterior thigh and can also occur in conjunction with or separately in the symphysis. The incidence of pelvic girdle pain in pregnancy is about 20%. [1, 2] If low back pain is included, this figure rises to 84%. [3] Pelvic girdle pain can be further subdivided into pelvic girdle syndrome (daily pain in all three pelvic girdle joints) which affects 29.7% of pregnant women with pelvic girdle pain, symphysis pubis pain which affects 11.6%, one-sided sacroiliac pain which affects 27.3% and bilateral sacroiliac pain which affects 31.4%. [1] Significant risk factors for developing low back pain or pelvic girdle pain in pregnancy are previous low back pain or pelvic girdle pain and/or previous trauma to the pelvis. [1, 2] Predictors for having persistent pelvic girdle pain or combined pain after delivery are low endurance of back flexors, older age, combined pain in early pregnancy and work dissatisfaction. [4] Pelvic girdle pain during pregnancy has a significant effect on quality of life as the endurance capacity for standing, walking, and sitting is diminished. This is particularly so in the third trimester when the disability rating index (DRI) is significantly higher compared with pregnant women with low back pain only and pregnant women without pain. The highest DRI is found in women with bilateral posterior pelvic pain plus symphysis pubis pain Women with pelvic pain in more than one location report more frequent use of crutches. [5]
Why do so many women experience low back or pelvic girdle pain during pregnancy? There has been much discussion in the literature on the role of relaxin, previously thought to be involved in the etiology of pregnancy-related PGP. Early studies concluded that an increased concentration of serum relaxin was a risk factor. [6] However, this correlation has not been confirmed by subsequent studies. [7, 8] The anatomy of the sacroiliac joint leads to the highest coefficient of friction of diarthrodial human joints. This friction can be altered according to the loading situation along with nutation of the sacrum, resulting in functional adaptations to stabilize the pelvic girdle. [2] Therefore, it is likely that the postural adaptations of pregnancy result in increased friction and loading on the sacroiliac joints.
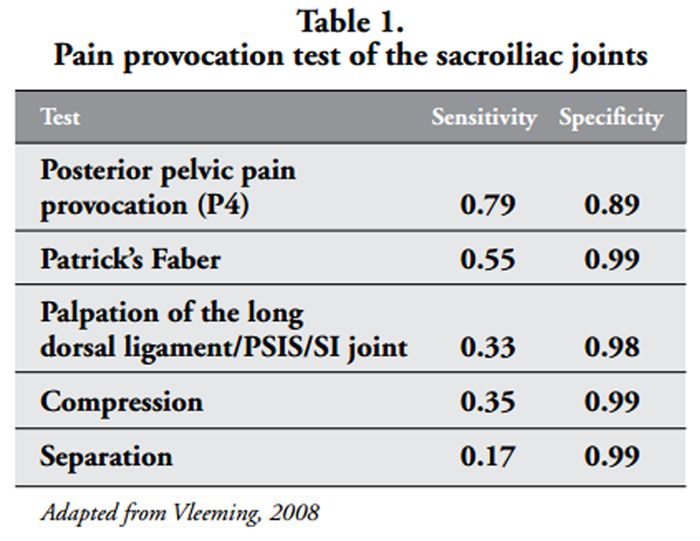
Chiropractors have a range of clinical tests to assess low back and pelvic girdle pain. Which tests are most optimal for evaluating the various low back and pelvic girdle pain syndromes of pregnancy? The following tests are recommended by the European guidelines for the diagnosis of pelvic girdle pain. [2] A description of these tests can be found in Appendix 1.
The most reliable tests to identify pain originating from the sacroiliac joints are:
- the posterior pelvic pain test (thigh thrust or P4),
- Patrick Faber test,
- tenderness on palpation of the long dorsal sacroiliac ligament
- Gaenslens test.
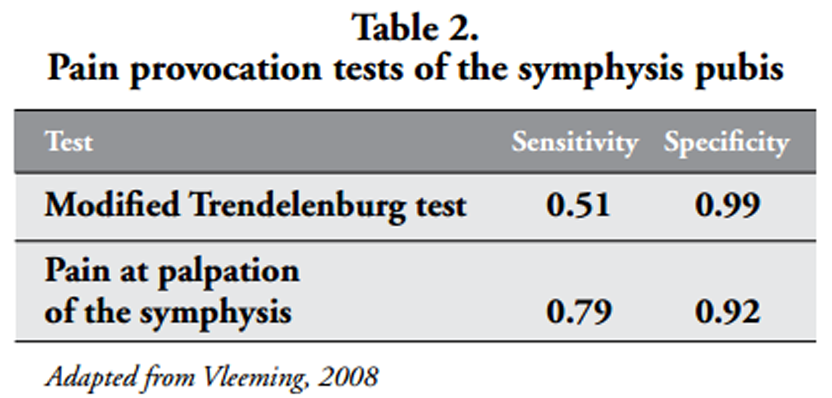
The most reliable tests to identify pain originating from the symphysis pubis are:
- tenderness on palpation of the symphysis pubis
- modified Trendelenberg test.
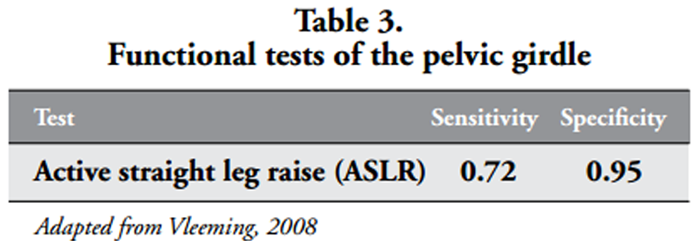
A reliable test for pelvic function and stability is the active straight leg raise (ASLR). Women with pregnancy-related low back and pelvic girdle pain use significantly more effort during ASLR than pregnant women without pain. At both 0cm and 20cm leg raise height they have less hip flexion force and develop more muscle activity. Therefore, the ASLR demonstrates disturbed load across the sacroiliac joints in pregnant women with pregnancy-related low back and pelvic girdle pain. [9]

Table 1
Table 2
Table 3 The sensitivity and specificity of these tests are depicted in Tables 1, 2 and 3. Worthy of note is that a bilateral positive P4 corresponds to a higher DRI than a unilateral or negative P4. Additionally, there is a significantly higher DRI if the ASLR is more than 0. [5]
What is the most effective treatment for reducing pain and disability in pregnant patients with low back or pelvic girdle pain? The following management techniques are recommended by the European Guidelines for the treatment of pelvic girdle pain. [2]
Manual therapy
The use of spinal manipulative therapy during pregnancy to reduce back pain and other related symptoms is supported by limited evidence. [10] A systematic review of 6 studies concluded that chiropractic care is associated with improved outcomes in pregnancy-related low back pain and pelvic girdle pain. [11]
Specific stabilizing exercises
There is evidence that specific muscle strengthening exercises (focusing specifically on stabilizing exercises for control and stability), with advice on activities of daily living, result in a significant reduction in pain. However, use of a rigid or non-rigid pelvic support belt does not add to the effects provided by exercise and advice. [12]
Water aerobics
There is limited evidence that water aerobics diminishes pregnancy related low back pain and sick leave due to pregnancy-related low back pain more than a land-based physical exercise program. [13] Nonetheless, regular water aerobics can result in significantly fewer requests for analgesia during labor and is a low risk exercise during pregnancy. However, there is no influence on maternal cardiovascular capacity, duration of labor or type of delivery. [14]
Acupuncture
There is some evidence that acupuncture, combined with stabilizing exercises, results in less pelvic girdle pain and may be a useful addition to a combined management program. [15] However, it should be noted that although no serious adverse events have been reported with the use of acupuncture during pregnancy, there is a risk of mild adverse events (painful treatment, headache and drowsiness, rash, nausea with feeling faint, sweating and dizziness) on the day of the treatment. [16]
CHIROPRACTIC MANAGEMENT
Chiropractic care is safe during pregnancy although there are some suggested modifications. Adjustments should be low-force (remember that relaxin is present from the first trimester to 3 months postpartum.) The patient should experience no abdominal pressure. The practitioner should make sure that the uterus is supported when the patient is side-lying and flex the hip less than usual when doing side posture techniques.
The author uses the following techniques with a good rate of success in reducing pain and restoring optimal function for the pregnant patient so that she can continue her activities of daily living in comfort. However, it is realistic for the goal to be supportive care and keeping quality of life static due to the constantly shifting dynamics of pregnancy.
Treatment of Symphysis Pubis Dysfunction (SPD)
This can occur from the first trimester and ranges from mildly to severely disabling. Some women have extreme difficulty walking and need to use crutches. It can have a detrimental effect on most activities of daily living. Chiropractors can manage the pain but it often does not resolve completely until after the birth. There are direct and indirect treatment methods for SPD that the chiropractor can utilise. Direct treatment includes use of the activator on the inferior or superior pubic ramus. Indirect treatment includes correction of any sacroiliac joint restrictions, symphysis pubis mobilization and myofascial techniques.
The sacroiliac joints can be adjusted either in side posture or with a prone drop whilst lying on a pregnancy pillow. However, the author has found that utilizing the drop piece with the patient supine and contacting the ASIS gives good results too. It is also less alarming for the patient. The patient is supine with knees bent and feet flat on the couch. The chiropractor is at the foot of the table on the side of SIJ restriction. Reassure the patient that no pressure will be exerted on the baby but only on the side of the pelvis and that this is a safe and gentle technique. Contact the ASIS with the thenar eminence and the indifferent hand contacts the patient’s posterior thigh on the same side. Lift the hip into slight flexion and apply a drop over the ASIS in an anterior to posterior with slight inferior to superior direction. Repeat a further 1-2 times.
Symphysis pubis mobilization is as follows. The patient is supine with both knees flexed and feet flat on the couch. The chiropractor tests whether resisted hip abduction or adduction causes pain over the symphysis pubis. If adduction is the less painful of the two, the chiropractor places the palms of both hands on the medial knees and asks the patient to push her knees together against mild resistance. The chiropractor then releases their hands. If abduction is the less painful of the two, the chiropractor places the palms of both hands on the lateral knees and asks the patient to push her knees apart against mild resistance. The chiropractor then releases their hands. The author has found that abduction is more often the most painful.
Myofascial techniques should include the round ligament, the long dorsal sacroiliac ligament, sacrotuberous ligament, gluteal muscles and piriformis. The long dorsal sacroiliac ligament has close anatomical relations with the erector spinae muscle, the posterior layer of the thoracolumbar fascia, and a specific part of the sacrotuberous ligament. Functionally, it is an important link between legs, spine, and arms. The ligament is tensed when the sacroiliac joints are counternutated and slackened when nutated. Slackening of the long dorsal sacroiliac ligament can be counterbalanced by both the sacrotuberous ligament and the erector muscle. [17]
Treatment of coccydynia
A couple of useful techniques for the chiropractor are the gluteal squeeze and coccygeal pump. For the gluteal squeeze, the patient lays prone and squeezes her buttocks together tightly. The chiropractor resists by pushing outwards with their hands in a cross-bilateral position then suddenly releasing. This can also be given as a home exercise with the patient using their own hands to resist. The coccygeal pump is done in the same way as the sacral pump but the middle finger of the contact hand lies along the coccyx to encourage flexion and extension.
For correction of coccygeal laterality, contact (with activator or thumb) immediately lateral to the base of the coccyx. The line of drive is lateral and superior. Avoid direct contact with the coccygeal apex as it is exquisitely painful.
Round ligament syndrome
This is characterised by a sudden, sharp pain in the abdomen and/or groin. It occurs from sit to stand and with hip extension. After the 5th month of pregnancy the round ligament is palpable and is released by holding it as a trigger point. Always check the SIJ’s and correct any restrictions.
Other techniques used by the author for pelvic girdle pain include the Webster technique, side-lying position, standing sacral release and orthopedic blocking.
The Webster technique was developed by a chiropractor particularly for the pregnant patient with a breech presentation and to address intrauterine constraint. [18, 19] A practice-based study in the USA reported that the Webster technique is 69% effective with the greatest changes observed in frank breech presentations. [20] It is a useful technique but not in isolation. More satisfying results are obtained when it is used in combination with other techniques.
Most pregnant patients find the side-lying position very comfortable as a general stretching technique for the pelvic girdle. The chiropractor stands in front of the patient with legs against the couch at the level of the patient’s belly. Contact over the lateral pelvis. Ask the patient to drop the top leg off the bed and support the pelvis to resist any forward roll of the body. Apply gentle pressure in a lateral to medial direction.
The standing sacral release is indicated for the nutated sacrum. The patient stands with both hands against the wall as if they are going to be “frisked”. The chiropractor supports the belly with the indifferent hand and slides the heel of the other hand down the sacrum from superior to inferior. If the sacrum is not nutated, the hand slides smoothly down to towards the apex. However, if the hand ‘catches’ then the sacrum is in pronation. Apply a light pressure in a superior to inferior and posterior to anterior direction until the hand slides smoothly down the sacrum.
How often should the chiropractor treat a pregnant patient? The author finds that twice a week for three weeks then once a week for two to three weeks works well. It depends on the gestation week on initial consultation and whether they have pain in more than one location. Once they reach 30 weeks, they are seen once or twice a week to maintain optimal function until the birth.
Conclusion
There is evidence that low back and pelvic girdle pain can be assessed with reliable clinical tests and treated with a combination of manual therapy and specific exercises to reduce pain and disability during pregnancy.
Appendix 1: Adapted from the European guidelines for the
diagnosis and treatment of pelvic girdle pain. 2
Active straight leg raise test The patient lies supine with straight legs and the feet 20 cm apart. The test is performed after the instruction: “Try to raise your legs, one after the other, above the couch for 20 cm without bending the knee”. The patient is asked to score any feeling of impairment (on both sides separately) on a 6-point scale: not difficult at all = 0; minimally difficult = 1; somewhat difficult = 2; fairly difficult = 3; very difficult = 4; unable to do = 5. The scores on both sides are added so that the sum score can range from 0 to 10.
Gaenslen’s test The patient, lying supine, flexes the hip/knee and draws it towards the chest by clasping the flexed knee with both hands. The patient is then shifted to the side of the examination table so that the opposite leg extends over the edge while the other leg remains flexed. The examiner uses this manoeuvre to gently stress both sacroiliac joints simultaneously. The test is positive if the patient experiences pain (either local or referred) on the provoked side.
Long dorsal sacroiliac ligament (LDL) test The patient lies on her side with slight flexion in both hip and knee joints. If the palpation causes pain that persists for more than 5 seconds after removal of the examiner’s hand it is recorded as pain. If the pain disappears within 5 seconds it is recorded as tenderness.
Modified Trendelenburg’s test The patient stands on one leg and flexes the hip and knee at 90 degrees. If pain is experienced in the symphysis the test is considered positive.
Patrick’s Faber test The patient lies supine: one leg is flexed, abducted, and externally rotated so that the heel rests on the opposite knee. The examiner presses gently on the superior aspect of the tested knee joint. If pain is felt in the sacroiliac joints or in the symphysis the test is considered positive.
Posterior pelvic pain provocation test The test is performed supine and the patient’s hip flexed to an angle of 90 degrees on the side to be examined: light manual pressure is applied to the patient’s flexed knee along the longitudinal axis of the femur while the pelvis is stabilized by the examiner’s other hand resting on the patients contralateral superior anterior iliac spine. The test is positive when the patient feels a familiar well localized pain deep in the gluteal area on the provoked side.
A similar test is described as the posterior shear or “thigh thrust” test.
Symphysis pain palpation test The patient lies supine. The entire front side of the pubic symphysis is palpated gently. If the palpation causes pain that persists for more than 5 seconds after removal of the examiner’s hand, it is recorded as pain. If the pain disappears within 5 seconds it is recorded as tenderness.
REFERENCES:
Albert H, Godskesen M, Westergaard J.
Incidence of four syndromes of pregnancy-related pelvic joint pain.
Spine 2002;27(24):2831-2834Vleeming A, Albert H, Ostgaard HC, Sturesson B, Stuge B.
European guidelines for the diagnosis and treatment of pelvic girdle pain.
Eur Spine J 2008;17:794-819Bastiaanssen JM, de Bie RA, Bastiaenen CH,
Heuts A, Kroese ME, et al.
Etiology and prognosis of pregnancy-related pelvic girdle pain; design of a longitudinal study.
BMC Public Health 2005;5:1Gutke A, Ostgaard HC, Oberg B.
Predicting persistent pregnancy-related low back pain.
Spine 2008;33;12:E386-E393Robinson HS, Mengshoel AM, Bjelland EK, Vollestad N.
Pelvic girdle pain, clinical tests and disability in late pregnancy.
Man Ther 2010;15:280-285Kristiansson P, Svardsudd K, von Schoultz B.
Serum relaxin, symphyseal pain, and back pain during pregnancy.
Am J Obstet Gynecol 1996;175(5):1342-7Hansen A, Jensen DV, Larsen E,
Wilken-Jensen C, Pedersen LK
Relaxin is not related to symptom-giving pelvic girdle relaxation in pregnant women.
Acta Obstet Gynecol Scand 1996;75:245-249Albert H, Godskesen M, Westergaard JG, Chard T, Gunn L .
Circulating levels of relaxin are normal in pregnant women with pelvic pain.
Eur J Obstet Gynecol Reprod Bio 1997; 74:19-22de Groot M, Pool-Goudzwaard AL, Spoor CW, Snijders CJ.
The active straight leg raising test (ASLR) in pregnant women: Differences in muscle activity and force between patients and healthy subjects.
Man Ther 2008;13:68-74Khorsan R, Hawk C, Lisi AJ, Kizhakkeveettil A
Manipulative Therapy for Pregnancy and Related Conditions: A Systematic Review
Obstet Gynecol Surv 2009 (Jun); 64 (6): 416–427Stuber KJ, Smith DL.
Chiropractic treatment of pregnancyrelated low back pain: a systematic review of the evidence.
JMPT 2008;31(6):447-54Depledge J, McNair PJ, Keal-Smith C, Williams M.
Management of symphysis pubis dysfunction during pregnancy using exercise support belts.
Phys Ther 2005;85(12):1290-1300Granath AB, Hellgren MS, Gunnarsson RK.
Water aerobics reduces sick leave due to low back pain during pregnancy.
JOGNN 2006;35(4):465-71Baciuk EP, Pereira RI, Cecatti JG, Braga AF, Cavalcante SR
Water aerobics in pregnancy: cardiovascular response, labor andneonatal outcomes.
Reprod Health 2008; 5:10Elden H, Ladfors L, Olsen MF, Ostgaard HC, Hagberg H.
Effects of acupuncture and stabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdle pain: randomised single blind controlled trial.
BMJ 2005;330(7494):761Elden H, Ostgaard HC, Fagevik-Olsen MF, Ladfors L, Hagberg H.
Treatments of pelvic girdle pain in pregnant women: adverse effects of standard treatment, acupuncture and stabilising exercises on the pregnancy, mother, delivery and the fetus/neonate.
BMC Comp Altern Med 2008;8:34Vleeming A, Pool-Goudzwaard AL, Hammudoghlu D,
Stoeckart R, Snijders CJ, Mens J M.
The Function of the Long Dorsal Sacroiliac Ligament: Its Implication for Understanding Low Back Pain.
Spine 1996;21(5)556-562Kunau PL.
Application of the Webster in-utero constraint technique: a case series.
J Clin Chiro Ped 1998;3:211-6Pistolese RA.
The Webster Technique: A Chiropractic Technique With Obstetric Implications
J Manipulative Physiol Ther 2002 (Jul); 26 (6): E1—9Alcantara J, Ohm J.
“The Webster Technique: Results from a chiropractic practice-based research program”;
accepted for poster presentation at the
ACNM annual meeting in Boston, May 2008
Return to PEDIATRICS
Since 12-24-2015
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |