

A Commentary on the Use of Mixed Methods
in Chiropractic Research: Part 1:
Overview of Mixed Methods EesearchThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2024 (Apr); 68 (1): 8–15 ~ FULL TEXT
OPEN ACCESS Peter C. Emary, DC, PhD • Kent J. Stuber, DC, PhD
Michael G. DeGroote Institute for Pain Research and Care,
McMaster University,
Hamilton, Ontario
We recently each completed doctoral programs where the major focus of our work was in mixed methods research. In the first part of this three-part commentary, we present an overview of mixed methods research. In the second part, we present a summary of our primary and secondary research findings from our doctoral work involving mixed methods. In a third paper, we will discuss integrating qualitative research with randomized controlled trials and how this mixed methods study design can be applied to research within the chiropractic profession.
Our aim with these papers is to increase awareness amongst the chiropractic community of the value (and challenges) of using this unique methodology. We also make recommendations for improving the quality of reporting and conduct of future chiropractic mixed methods studies. Further dissemination of this work will occur through online webinars and conference presentations.
Keywords: Chiropractic; Methodological Quality; Mixed Methods Research.
From the FULL TEXT Article:
Introduction
We recently each completed a Doctorate in Philosophy (PhD) degree in which we received extensive training in, and our respective thesis dissertations focused on, mixed methods research. The use of mixed methods designs (i.e., the combination of quantitative and qualitative methods) in research studies involving the chiropractic profession and other health-related fields has become increasingly common in recent years. [1–3] The explicit integration of methods within mixed methods research is distinct from “multi-method” research where investigators use quantitative and qualitative methods in a single study (e.g., a survey with follow-up interviews) but do not link or integrate the two components. [4–6] This distinction of mixed methods, that is, as an approach to research beyond simply using quantitative and qualitative methods as separate and distinct components in a single study, formally emerged within the mixed methods literature during the late 1980s and early 1990s. [5] Subsequently, the intentional and explicit integration of quantitative and qualitative methods is now recognized as a central tenet of mixed methods research. [4–6]
As part of our doctoral work, we reviewed the literature to assess the reporting and methodological quality of mixed methods studies involving chiropractic research and found that most (≈ 96%) studies had important omissions. [1–3] We applied these results to optimize methodologic reporting in three mixed methods studies we conducted, one on patient-centredness in chiropractic care, [7, 8] and two on the association between chiropractic care and opioid prescribing. [9–11]
Objective
The purpose of part 1 in this three-part commentary is to present an overview of mixed methods research for chiropractic clinicians and researchers. In part 2, we will summarize the findings from the aforementioned studies from our doctoral work involving mixed methods research. In doing so, our aim with these papers is to increase awareness amongst the chiropractic community of the value, and challenges, of using this unique methodology. We also make recommendations for improving the quality of reporting and conduct of future chiropractic mixed methods studies. In a third paper, we will discuss integrating qualitative research with randomized controlled trials and how this mixed methods study design can be applied to research within the chiropractic profession.
To inform this series of commentaries, we relied on mixed methods literature retrieved from previous searches in the MEDLINE, Embase, CINAHL, and the Index to Chiropractic Literature databases. [1–3] Additional mixed methods articles and textbooks not identified in our initial database searches that were pertinent to these commentaries were also used. [4–6, 10–17] We hope readers and those interested in reviewing or conducting mixed methods research will find the information and resources provided in this series of articles useful.
Reflexivity statement
At this stage of our careers, we each view our ontological and epistemological perspectives toward research inquiry as on a continuum between postpositivism and constructivism. We are both trained in health research methodology and are experienced clinicians. We also collectively have over 100 publications; however, much of this work, particularly from earlier on in our research careers, was conducted through primarily a postpositivist lens. In this current series of papers, we present examples and findings from some of our own mixed methods research studies and have made a conscious effort to limit bias as well as an over-emphasis on quantitative findings in the organization and presentation of this information. We have also incorporated several examples from other authors of chiropractic mixed methods studies in our commentaries where relevant.
Discussion
Mixed methods research

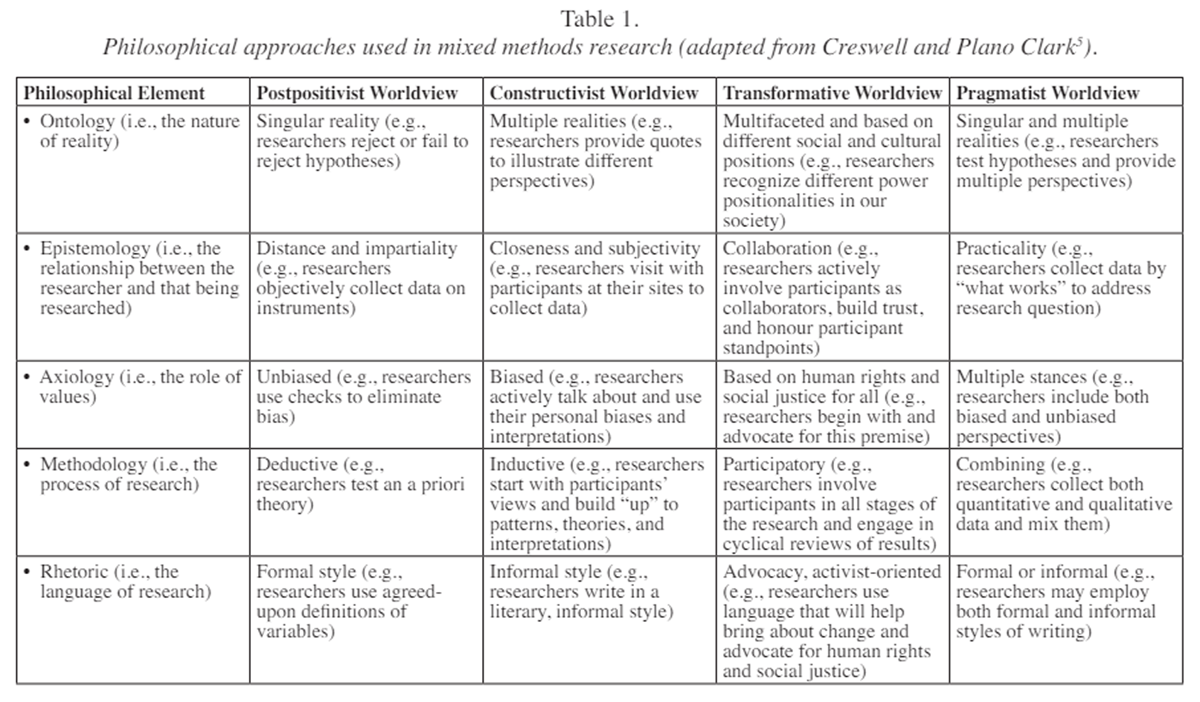
Table 1 Mixed methods research involves the mixing or integration of various elements of quantitative and qualitative methods, including viewpoints, data collection, analysis and inference techniques, for the purposes of breadth and depth of understanding and corroboration. [4] Mixed methods research is increasingly being recognized as a third research paradigm, distinct from purely quantitative or qualitative research. [4, 5] Mixed methods research is particularly useful for answering questions that are difficult to answer using only quantitative or qualitative methods and can serve as a powerful tool for investigating educational programs, knowledge translation strategies, or complex therapeutic interventions, such as multi-modal chiropractic. [5, 6] A common philosophical approach used in mixed methods research is ‘pragmatism,’ where the focus is on combining methods of data collection for “what works” best in answering a particular research question. [5] With this approach, the research question drives the study design [5], and both objective and subjective knowledge are valued.
The four philosophical approaches used in mixed methods research are outlined in Table 1.
Rationales for using mixed methods
There are several rationales for undertaking mixed methods research. These include, but are not limited to, a need to:
obtain more complete and corroborated results (e.g., to find points of convergence and divergence12);
explain initial quantitative results;
first explore questions, variables to be measured, or theories to guide a study before administering instruments;
enhance an experimental (i.e., randomized controlled) trial with a qualitative study, such as in a feasibility study or process evaluation;
describe and compare different types of cases;
involve participants in the study to ensure the research will bring about change that impacts people or communities (i.e., participatory-social justice); or
develop, implement and evaluate a program. [5]
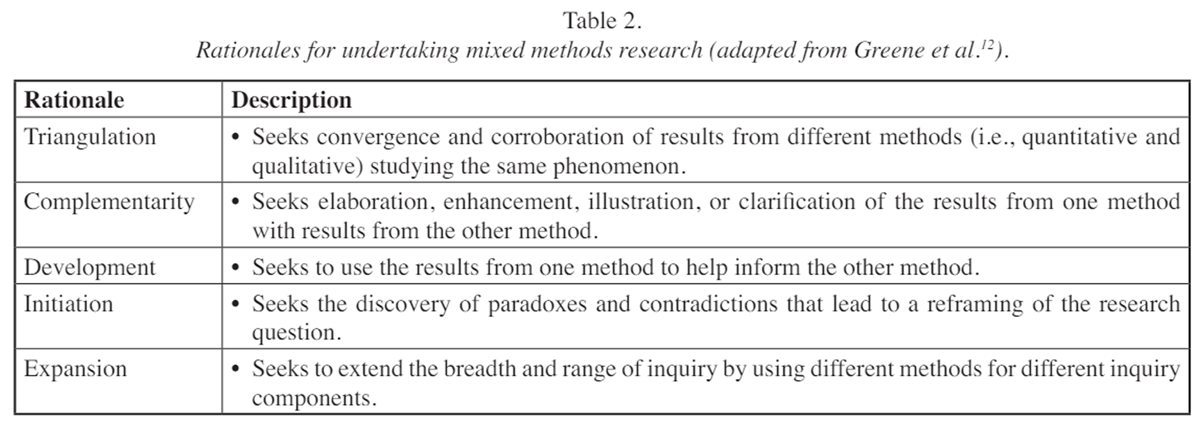
Table 2 The purposes or rationales for mixed methods research have been consolidated by Greene et al. [12] into five general categories, namely:
(1) triangulation,
(2) complementarity,
(3) development,
(4) initiation, and
(5) expansion (Table 2).In a 2021 mixed methods study, Emary et al. [9] used the rationale of complementarity, where the interview (i.e., qualitative) component of the study was used to obtain a more complete understanding of the barriers and facilitators to incorporating chiropractic services into primary care as well as whether these services were used by patients or general practitioners to reduce reliance on opioid prescribing for chronic non-cancer pain. Similarly, Stuber et al. [7] utilized a complementarity approach where qualitative and quantitative data were interwoven to provide an in-depth understanding of patients’ and chiropractors’ perspectives, perceptions, and experiences of patient-centred care in chiropractic. They also used triangulation in which their qualitative data were converged with their quantitative data for the purposes of corroborating the quantitative findings.
A mixed methods study is not always preferable. There are instances where only a quantitative or qualitative research approach is not only sufficient, it is preferable and more suitable. For instance, quantitative research may be the best approach when the aim is to understand the relationship between variables or determine if one group, compared to another group, performs better on a particular outcome of interest. A qualitative approach, on the other hand, may be optimal when the aim is to explore a particular phenomenon, map the complexity of the situation, or honour the voices and convey multiple perspectives of participants. [5]
In general, problems best suited for mixed methods research are those in which one data source (i.e., quantitative or qualitative) may be insufficient. For example, in a 2014 narrative review of the literature [13], we identified previously published studies on clinicians’ attitudes toward medication prescription rights in chiropractic practice. In all identified studies, traditional quantitative survey methods (e.g., Likert-scale items) were utilized for data collection. Based on the findings from these studies, we concluded that there was no clear definition or consensus on medication prescription rights within the chiropractic profession, and that further research was warranted. In a 2020 study of chiropractors in Switzerland, Emary et al. [19] utilized a mixed-methods (Q-methodology) approach and identified four distinct viewpoints among chiropractors toward medication prescribing (i.e., prescribers, non-prescribers, collaborators, and integrators) that were not identified in previous quantitative surveys.
Respondents’ rankings of agreement toward 38 statements from a Q-methodology survey (quantitative) were triangulated with their answers to a series of open-ended questions (qualitative) to identify the four typologies of individuals within the larger group (n = 286) of Swiss chiropractors. These findings provided new insights on chiropractic prescribing rights, and consensus was reached on this topic among participants in this study. [19] All except the non-prescriber group thought medication prescription privileges were advantageous for the chiropractic profession in Switzerland, and there was strong consensus among all four groups that medication prescribing should not replace manual therapy in chiropractic practice. [19]
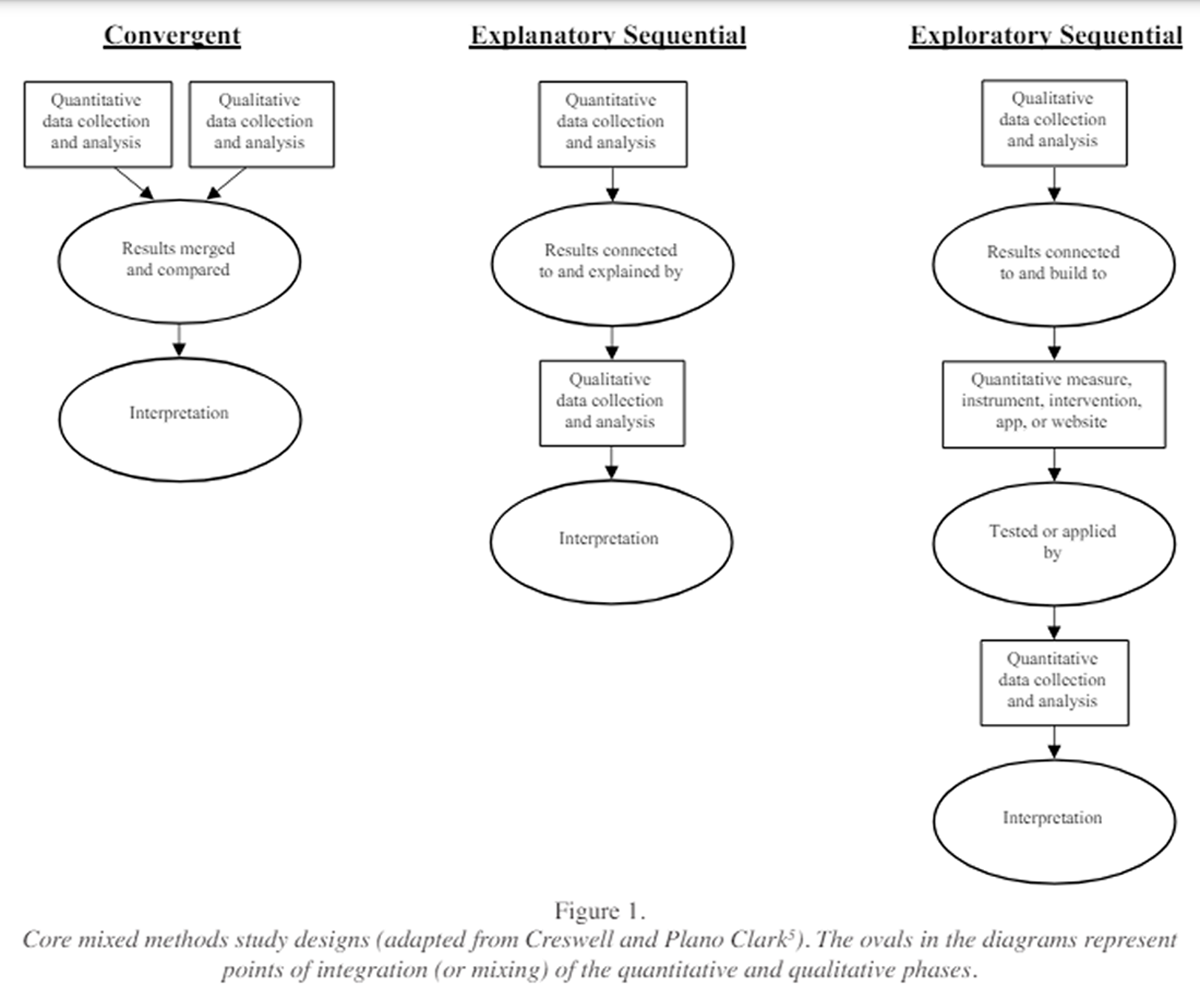
Mixed methods study designs
Figure 1 There are three core study designs used in mixed methods research, including:
(1) convergent,
(2) explanatory sequential, and
(3) exploratory sequential (Figure 1).In a convergent design, researchers compare and combine (or triangulate) quantitative and qualitative results to obtain a richer understanding of the research problem, or to validate one set of findings with the other. [5] With this design, the results from one method do not depend on the results of the other method; therefore, quantitative and qualitative data are collected and analyzed concurrently, but separately. The results from the two datasets are then merged and the researcher interprets to what extent and in what ways the two sets of results converge or diverge from one another. [5] For example, in an online survey of students, faculty, and staff at five international chiropractic educational institutions, Pohlman et al. [20] used closed- and open-ended questions (i.e., quantitative and qualitative data collection, respectively) to evaluate patient safety attitudes among stakeholders in chiropractic teaching clinics. The authors integrated quantitative and qualitative methods through ‘merging’ [6], by comparing the quantitative and qualitative findings through joint display figures and narrative discussion. By combining methods, the qualitative findings provided in-depth insight into the quantitative survey results and helped identify areas for improvement in patient safety education within chiropractic teaching programs. In a 2023 study, Emary et al. [14] used a convergent, mixed methods study design to examine 1,681 Canadian military Veterans’ use and preferences toward 12 specific health care disciplines and treatment approaches for the management of chronic low back pain. Qualitative (open-text) data were integrated with quantitative (closed-ended) survey data using a joint display table and contiguous narrative in the results to gain a deeper understanding of Veterans’ treatment preferences.
With an explanatory sequential design, quantitative data collection and analysis are followed by qualitative data collection and analysis, and the qualitative data are used to help explain or expand on the initial quantitative results. For example, in a mixed methods study on patient perceptions toward patient-centred care in chiropractic practice, Stuber et al. [7] used an explanatory sequential design, where follow-up qualitative interviews and focus groups were conducted to help explain initial quantitative survey results. Emary et al. [9] also used an explanatory sequential, mixed methods design in two separate analyses [10, 11] on the association between chiropractic integration and opioid use among patients with non-cancer spinal pain in an Ontario community health centre. In-depth, one-on-one interviews of patients and general practitioners (qualitative) were used to further explore differences in the number and dose of opioid prescriptions between recipients and non-recipients of chiropractic services measured via electronic medical record review (quantitative). In all three of these studies [7, 10, 11], integration was achieved using joint display, contiguous narrative, or weaving approaches. [6]
In contrast to an explanatory sequential design, an exploratory sequential design begins with an exploratory qualitative phase (i.e., qualitative data collection and analysis) followed by a developmental quantitative phase. The quantitative phase is based on the initial qualitative results, which are used to generate new quantitative variables, design a quantitative instrument, or develop activities for an intervention or digital product, such as an app or website. [5] The developmental quantitative phase is followed by a third phase where the new feature (i.e., variable[s], instrument, or product) is tested quantitatively to see how the quantitative findings build on the initial qualitative results or provide a clearer understanding of the research problem. In either case, the development of the quantitative feature is grounded in the initial qualitative perspectives of participants. [5] In a 2020 study investigating chiropractors’ understanding of building trust with patients, Connell and Bainbridge [20] used an exploratory sequential design, where initial interviews (qualitative) were conducted with six chiropractors in British Columbia (BC), Canada and used to develop a survey instrument (quantitative). This type of integration is an example of ‘building’ [6], where qualitative findings are used to create a quantitative questionnaire. In addition, the initial qualitative findings from the interviews in this study ensured that questions on the survey instrument reflected the perspectives of BC chiropractors. The questionnaire was then distributed to all members of the provincial chiropractic association (n = 1,154) and used to measure chiropractors’ perceptions of trust and confirm initial qualitative themes. [20] The authors further integrated their results through ‘merging’ [6], by comparing the qualitative and quantitative findings through narrative discussion.
Advantages and challenges of mixed methods research
There are several advantages with a mixed methods approach. [5] Mixing quantitative and qualitative methods allows the strengths of each methodology to account for weaknesses of the other. For instance, when there is good external validity (e.g., data collected in a representative epidemiological survey or pragmatic clinical trial), quantitative research findings are generalizable to larger populations. However, findings from qualitative research allow for greater in-depth knowledge and understanding of perspectives, experiences, or beliefs of individuals or groups. [15] Therefore, by incorporating both deductive and inductive reasoning [5, 16], mixed methods research builds on the strengths of quantitative and qualitative methods and provides more complete answers to research questions. Mixed methods research can also offer new insights into investigations that go beyond the results of the separate quantitative and qualitative components (i.e., meta-inferences) [5, 17], as illustrated in the following equation: 1 + 1 = 3, where the first ‘1’ is the quantitative component, the second ‘1’ is the qualitative component, and the ‘3’ is the combination of results and meta-inferences generated from mixing quantitative and qualitative methods. [17] Meta-inferences are a set of conclusions reached in a mixed methods study when researchers jointly draw on the quantitative and qualitative results. For example, in the 2022 mixed methods analyses by Emary et al. [10, 11], receipt of chiropractic services at an Ontario community health centre was inversely associated with opioid use among adults with non-cancer spinal pain. When combined with themes from the studies’ qualitative findings (i.e., patient self-efficacy, accessibility of non-pharmacological services, and impact of treatment), the meta-inferences drawn from these two studies were that,(1) patients who were referred for chiropractic services may have been
more resistant to taking opioids, and
(2) access to chiropractic treatment at the centre provided patients and
their general practitioners with another non-opioid pain management option.By combining inferences from the quantitative and qualitative components in each of the two studies, the authors gained additional insight into why chiropractic recipients were less likely to be prescribed opioids or had, among those already prescribed, reduced opioid use.
Mixed methods research also provides opportunities for collaboration, which can help bridge the historical divide (also known as the paradigm debate period [5] ) between quantitative and qualitative researchers. [5] Mixed methods research also encourages the use of multiple worldviews, or paradigms, including those such as pragmatism that encompass both quantitative and qualitative research (see Table 1). [5] A final advantage of mixed methods research is that it helps investigators develop broader skillsets or expertise in multiple forms of research methods (i.e., quantitative, qualitative, and mixed methods).
Despite its advantages, mixed methods research also entails unique challenges. For instance, mixed methods studies can often become complex, drawn-out investigations which may take several years to complete. [5, 6] Qualitative data collection and analysis are time-intensive, and additional time is needed for mixed methods studies that incorporate a sequential explanatory (i.e., two-phase) or exploratory (i.e., three-phase) study design. There are also cost considerations in mixed methods research, such as the need to purchase additional materials or services (e.g., quantitative and qualitative analysis software programs, audio recorders, printing, transcription services), as well as the need to work in larger teams requiring qualitative researchers and/or mixed methodologists (i.e., methodologists with graduate-level training or expertise in mixed methods research). Mixed methods studies can also create team management issues, particularly for members with diverse levels of mixed methodological or content expertise. Further, mixed methods investigators may need to educate team members or others (e.g., grant committees, journal editors, or peer reviewers) about mixed methods research, particularly if they are unfamiliar with this methodology. As such, mixed methods research must be carefully planned, and suitable training should be sought by novice researchers interested in conducting mixed methods research.
Conclusion
In this first paper, we have presented an overview of mixed methods research as well as the philosophical underpinnings and rationales for using this methodology. In addition, we have introduced readers to the three core mixed methods study designs, as well as the advantages and challenges of employing a mixed methods approach.
In part 2 of our commentary, we will present the primary and secondary findings from our doctoral work involving mixed methods research and provide recommendations for improving the quality of reporting and conduct of future chiropractic mixed methods studies.
Acknowledgments
The authors would like to acknowledge Professor Jason W. Busse, DC, PhD for providing edits to the original draft of this manuscript. The original version of this paper formed part of a PhD thesis undertaken by PCE in the Department of Health Research Methods, Evidence, and Impact at McMaster University.
References:
Emary PC, Stuber KJ, Mbuagbaw L, Oremus M, Nolet PS, Nash JV,
Bauman CA, Ciraco C, Couban RJ, Busse JW.
Quality of reporting in chiropractic mixed methods research:
a methodological review protocol.
Chiropr Man Therap. 2021;29(1):35.Emary PC, Stuber KJ, Mbuagbaw L, Oremus M, Nolet PS, Nash JV,
Bauman CA, Ciraco C, Couban RJ, Busse JW.
Risk of bias in chiropractic mixed methods research:
a secondary analysis of a meta-epidemiological review.
J Can Chiropr Assoc. 2022;66(1):7-20.Emary PC, Stuber KJ, Mbuagbaw L, Oremus M, Nolet PS, Nash JV,
Bauman CA, Ciraco C, Couban RJ, Busse JW.
Quality of reporting using Good Reporting of A Mixed Methods Study
criteria in chiropractic mixed methods research: a methodological review.
J Manipulative Physiol Ther. 2023 Dec 21:S0161-4754(23)00088-X.Johnson RB, Onwuegbuzie AJ, Turner LA.
Toward a definition of mixed methods research.
J Mix Methods Res. 2007;1(2):112-133.Creswell JW, Plano Clark VL.
Designing and Conducting Mixed Methods Research. 3rd ed.
Thousand Oaks, CA: Sage 2018.Fetters MD, Curry LA, Creswell JW.
Achieving integration in mixed methods designs –
principles and practices.
Health Serv Res. 2013;48(6 Part II):2134-2156.Stuber KJ, Langweiler M, Mior S, McCarthy PW.
Assessing patient-centered care in patients with chronic health
conditions attending chiropractic practice:
protocol for a mixed-methods study.
Chiropr Man Therap. 2016;24(1):15.Stuber KJ, Langweiler M, Mior S, McCarthy PW.
A pilot study assessing patient-centred care in patients with
chronic health conditions attending chiropractic practice.
Complement Ther Med. 2018;39:1-7.Emary PC, Oremus M, Mbuagbaw L, Busse JW.
Association of chiropractic integration in an Ontario community health
centre with prescription opioid use for chronic non-cancer pain:
a mixed methods study protocol. BMJ Open. 2021;11(11):e051000.Emary PC, Brown AL, Oremus O, Mbuagbaw L, Cameron DF, DiDonato J, Busse JW.
Association of Chiropractic Care With Receiving an Opioid
Prescription for Noncancer Spinal Pain Within a Canadian
Community Health Center: A Mixed Methods Analysis
J Manipulative Physiol Ther Volume 2022 (May); 45 (4): 235–247Emary PC., Brown AL, Oremus O, Mbuagbaw L, Cameron DF, DiDonato, J, Busse JW.
The association between chiropractic integration in an Ontario community
health centre and continued prescription opioid use for chronic
non-cancer spinal pain: a sequential explanatory mixed methods study.
BMC Health Serv Res. 2022;22(1):1313.Greene JC, Caracelli VJ, Graham WF.
Toward a conceptual framework for mixed-method evaluation designs.
Educ Eval Policy Anal. 1989;11(3):255-274.Emary PC, Stuber KJ.
Chiropractors’ attitudes toward drug prescription rights:
A narrative review.
Chiropr Man Therap. 2014;22(1):34.Emary PC, Ciraco C, DiDonato J, Deschambault B, Garas A, Sprague S, Busse JW.
Treatment preferences among Canadian military veterans living with
chronic low back pain: protocol for a mixed methods
cross-sectional survey.
J Contemporary Chiropr. 2023;6:129-148.Miller PJ, Jones-Harris AR.
The evidence-based hierarchy: is it time for change?
A suggested alternative.
J Manipulative Physiol Ther. 2005;28(6):453-457.Morgan DL.
Paradigms lost and pragmatism regained: methodological implications
of combining qualitative and quantitative methods.
J Mix Methods Res. 2007;1(1):48-76.Fetters MD, Freshwater D.
The 1 + 1 = 3 integration challenge.
J Mix Methods Res. 2015;9(2):115-117.Emary PC, Oremus M, Houweling TAW, Wangler M, Akhtar-Danesh N.
Attitudes, beliefs, and practices among Swiss chiropractors regarding
medication prescribing for musculoskeletal conditions:
a national Q-methodology study.
Chiropr Man Therap. 2020;28(1):54.Pohlman KA, Salsbury SA, Funabashi M, Holmes MM, Mior S.
Patient safety in chiropractic teaching programs:
a mixed methods study.
Chiropr Man Therap. 2020;28(1):50.Connell G, Bainbridge L.
Understanding how chiropractors build trust with patients:
A mixed-methods study.
J Can Chiropr Assoc. 2020;64(2):97-108.
Return to CHIROPRACTIC RESEARCH
Since 6-09-2024
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |