

A Randomized Trial of Combined Manipulation, Stabilizing Exercises,
and Physician Consultation Compared to Physician Consultation
Alone for Chronic Low Back PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine (Phila Pa 1976) 2003 (Oct 1); 28 (19): 2185–2191 ~ FULL TEXT
Niemistö, Leena, MD; Lahtinen-Suopanki, Tiina, PT; Rissanen, Pekka, PhD; Lindgren,
Karl-August, MD, PhD; Sarna, Seppo, PhD; Hurri, Heikki, MD, PhD
Rehabilitation Unit of the Orthopaedic Hospital Orton,
Invalid Foundation,
Helsinki, Finland.
Study design: A prospective randomized controlled trial.
Objectives: To examine the effectiveness of combined manipulative treatment, stabilizing exercises, and physician consultation compared with physician consultation alone for chronic low back pain.
Summary of background data: Strong evidence exists that manual therapy provides more effective short-term pain relief than does placebo treatment in the management of chronic low back pain. The evidence for long-term effect is lacking.
Methods: Two hundred four chronic low back pain patients, whose Oswestry disability index was at least 16%, were randomly assigned to either a manipulative-treatment group or a consultation group. All were clinically examined, informed about their back pain, provided with an educational booklet, and were given specific instructions based on the clinical evaluation. The treatment included four sessions of manipulation and stabilizing exercises aiming to correct the lumbopelvic rhythm. Questionnaires inquired about pain intensity, self-rated disability, mental depression, health-related quality of life, health care costs, and production costs.
Results: At the baseline, the groups were comparable, except for the percentage of employees (P = 0.01). At the 5- and 12-month follow-ups, the manipulative-treatment group showed more significant reductions in pain intensity (P < 0.001) and in self-rated disability (P = 0.002) than the consultation group. However, we detected no significant difference between the groups in health-related quality of life or in costs.
Conclusions: The manipulative treatment with stabilizing exercises was more effective in reducing pain intensity and disability than the physician consultation alone. The present study showed that short, specific treatment programs with proper patient information may alter the course of chronic low back pain.
KEYWORDS: low back pain, randomized controlled trial, spinal manipulation
From the FULL TEXT Article:
Background
Chronic low back pain (CLBP) is the most common complaint of the working-age population. In addition to human suffering, it causes a substantial economic burden due to the wide use of medical services and absence from work. [1] Although in most patients acute LBP resolves with conservative treatment or without any treatment, the back pain appears to recur and become chronic more often than expected. [2, 3]
According to the latest extensive systematic literature review of the management of CLBP, strong evidence exists that manual therapy provides more effective shortterm pain relief than does placebo treatment. [4] Moderate evidence indicates that manual therapy is more effective than the usual care prescribed by the general practitioner, including bed rest, analgesics, and massage, for short-term pain relief. [4] However, the evidence for longterm effects is lacking. [4, 5]
A recent focus in the management of CLBP patients has been the specific training of the deep abdominal (internal oblique and transversus abdominis) and lumbar multifidus muscles. The primary role of these muscles is considered to be the provision of dynamic stability and segmental control of the spine. [6] A randomized controlled trial (RCT) of specific stabilizing exercises in the treatment of CLBP with radiologic diagnosis of spondylolysis or spondylolisthesis showed significant reduction in pain intensity and functional disability levels compared with that of other commonly prescribed conservative treatment programs. The results were maintained during a 30–month follow-up. [7]
It has also been shown that subchronic LBP can be treated successfully with an approach that includes a clinical examination and information to patients about the nature of the problem to reduce fear and motivate them to resume light activity. [8]
The hypothesis of the present study was that manipulative treatment with stabilizing exercises and physician consultation would provide more effective pain relief and alleviation of disability than physician consultation alone. We wished to compare manipulative treatment with an approach expected to be the most cost-effective method. [9] The clinical objectives were to examine the one-year effectiveness and cost-effectiveness of combined manipulative treatment, stabilizing exercises, and physician consultation compared with those from physician consultation and patient education alone.
Patients and Methods
Study Sample and Design.
The present study was conducted in the Rehabilitation Unit of the Orthopedic Hospital ORTON, Invalid Foundation, Helsinki, Finland. The study was initiated in March 1999 and completed in September 2000. Chronic LBP patients were recruited voluntarily by a widely circulated newspaper advertisement in February 1999. The patients had 1 week to register for the study by phone, fax, mail, or e-mail. The research nurse then contacted the patients by telephone or e-mail to ensure that the candidate met the inclusion criteria.
We included 24– to 46–year-old employed (including students and temporary housewives) patients who had LBP (with or without sciatica) of at least 3 months’ duration. The selfrated disability index (Oswestry Low Back Pain Disability Questionnaire) [10] score had to be at least 16%. We excluded patients with malignancies, ankylosing spondylitis, severe osteoporosis, severe osteoarthritis, paralysis, progressive neurologic disease, hemophilia, spinal infection, previous spinal operation, vertebral fracture during the previous 6 months, severe psychiatric disease, or severe sciatica with a straight leg raising test less than 35° or with at least 1 recent motor deficit. Other exclusion criteria included pregnancy, severe overweight (body mass index [BMI] >32), or simultaneous spinal rehabilitation or other spinal study.
We invited eligible patients to attend the baseline trial for further evaluation. The clinical examination was performed before randomization to confirm the admission criteria. The Hospital Medical Ethics Review Board approved the study. Patients were provided written and oral information on the study as required by the Declaration of Helsinki [9] before they were asked to sign a document signifying informed consent.
InterventionManipulative-Treatment Group. Patients in the manipulative- treatment group attended 60–minute evaluation, treatment, and exercise sessions 4 times in the course of 4 weeks. An experienced manual therapist conducted the treatment sessions. The therapy included manipulation using a muscleenergy technique and stabilizing exercises aiming to correct the lumbopelvic rhythm. [11, 12] Manipulation with a muscle-energy technique was used to correct any biomechanical dysfunctions in the lumbar or pelvic segments. [13] Muscle-energy technique is a manipulative treatment procedure that uses a voluntary contraction of the patient’s muscles against a distinctly controlled counterforce from a precise position and in a specific direction. Any muscular tension in either biceps femoris, rectus femoris, [14] iliopsoas, or gluteus was treated by passively stretching the muscles and teaching autostretching techniques. [15]
Muscle strain/tension was diagnosed by testing the range of motion of the hip and knee joints. The restriction was measured with a goniometer. The stabilizing exercises were taught by asking the patients to draw in the stomach while giving them verbal, visual, and tactile feedback and measuring the pressure change with a biofeedback meter. In a prone position with the pressure cushion under the lower abdomen, a pressure decrease of 4mm Hg was considered to be the lower limit for actual independent activation of the transversus abdominis muscle. Gradually the patients were instructed to perform the stabilizing exercises in a more functional manner. [16] Finally, the patients learned to do these isometric exercises during their daily activities. All exercise was by definition pain-free.
Physician’s Consultation Group. Both the manipulative treatment group and the consultation group received a 25–page educational booklet on basic anatomy and physiology of the spine, principles of ergonomics for LBP patients, and instructions on how to exercise and to cope with the acute phase of LBP. [17] The clinical findings were explained with the aid of a human skeleton, and the radiograph findings and possible causes of pain were clarified. The patients were told that LBP generally has a benign, self-limiting natural course. They could hasten the process by simple regular exercises and by avoiding immobility.
The patients received individual instructions regarding posture and three to four exercises aiming to increase spinal mobility, muscle stretch, and/or trunk muscle stability based on the clinical evaluation. They were also advised to avoid long-standing static work by performing several countermovements. When lifting heavy objects, they were told to avoid bending and twisting and instead to use their legs. The main principle was to encourage the patients to treat themselves instead of undergoing passive treatments. At the 5–month followup, this information was reinforced. Both appointments lasted an average of 1 hour. During the follow-up, the patients were free to use other health care services for LBP, use of which they were asked to record.OutcomeMeasures.
The primary outcomes were pain intensity and back-specific disability. Degree of experienced pain and disability was quantified by: 1) a visual analogue scale (VAS; from 0–100); 2) frequency of LBP experienced; and 3) the Oswestry Low Back Pain Disability Questionnaire (ODI; from 0–100). [10, 18]
The secondary outcomes were the degree of mental depression, which was assessed by a Finnish Depression Questionnaire (DEPS) [19]; health-related quality of life (HRQoL) (15D), [20] days on sick leave, costs of health care consumption, and productivity costs. The questionnaires were presented at the initial examination before randomization and at follow-up examinations 5 and 12 months after randomization. Costs were assessed from a societal point of view. Use of health services, direct drug and traveling costs to the patients, and productivity costs due to absence from work were measured by a questionnaire in the study sample before randomization and at the 12–month follow-up.
The service fees to the patients were not included in the cost analysis. In monetary valuation of health services, we applied Finnish standard cost information at the year 2000 price level. [21] Standard costs are average costs for various specified procedures or diagnostic tests by representative Finnish health care providers. Productivity costs were valued by the average year 2000 wage level in Finland. Because of theoretical and methodologic controversy surrounding such valuation, we tested the effect of the valuing algorithm on total costs by using a 50% lower estimate of the average wage level. Costs were converted into dollars ($1 = 1.06 euros, June 2002).
Statistical Analysis.
Power calculations were carried out before the study to attain a power of at least 0.80 at a significance level of 0.05. NQuery 4.0 2-group, univariate, repeated measures analysis of variance (ANOVA) (Greenhouse-Geisser correction) were used. [22] A clinically significant difference between the groups in the primary outcome pain intensity (VAS 0–100), was considered to be 7 in the second phase and 5 in the third phase, with a standard deviation of 22. Thus, the levels for the study group were 55, 35, and 40, and for the control group 55, 42, and 45, respectively. Accordingly, this required 94 patients per group for a total of 188 patients. Considering an expected dropout rate of 8%, we increased the group size to 102. Patients were included in the analysis as part of the group allocation by randomization. Missing values in questionnaires were not substituted for.
Baseline data were presented as means, medians, percentages, and standard deviations. Categorical baseline variables were analyzed by the χ2 test. Continuous baseline variables were analyzed by an independent sample t test or in the case of skewed distribution of the data, the Mann-Whitney U test. Continuous outcomes were analyzed according to the intention- to-treat principle, with repeated measures ANOVA (group x time of assessment). In case of skewed distribution of the data, the logarithmic or square root transformation was used. Categorical variables (frequency of LBP experienced) were analyzed by the likelihood ratio test for the difference in change between time points and study groups. The heterogeneity of the changes within the groups were tested with the McNemar χ2 test. The data were analyzed with SYSTAT 10 for Windows software. [23] Significance was accepted at the 5% level. All P values were two-tailed.
Assignment.

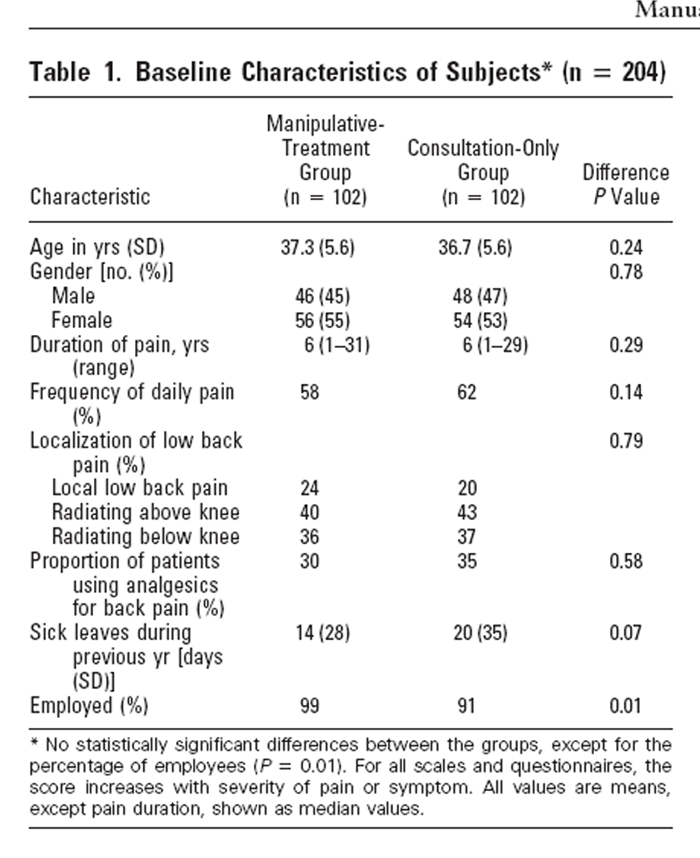
Table 1 After the patients had agreed to participate in the study, and the anamnestic inclusion criteria were confirmed, they were asked to complete baseline questionnaires (Table 1) and then underwent medical examination to check the clinical inclusion criteria. Once this was done, the research nurse randomized the patients to either a manipulative-treatment or a consultation group. The fixed allocation randomization procedure was performed to guarantee an equal number of patients in both groups. The assignments were presented in sealed, sequentially numbered envelopes. No stratification was based on prognostic factors. The research nurse was not responsible for determining patient eligibility.
Masking.
Patients could not be blinded in this study, [9] but a blinded clinical assessment was performed before randomization and at the 5–month follow-up. In addition, all the primary outcomes were completed by the patients themselves.
Results
Participant Flow and Follow-up
A patient sample of 210 was selected on the basis of anamnestic criteria for 900 volunteers. The clear majority of 900 volunteers were disqualified by virtue of a low (<16%) Oswestry score. Other reasons for exclusion were prior spinal surgery, inflammatory diseases (i.e., colitis ulcerosa, Mb Bechterew, rheumatoid arthritis, etc.), simultaneous spinal rehabilitation, and unemployment status. After the physician’s examination, 204 patients were included in the trial: 102 assigned to the manipulative- treatment and 102 to the consultation group.
All patients visited the physician at least once before randomization and received a back booklet, information on the etiology of their back pain, and instructions on how to cope with low back trouble. Of the subjects in the manipulative-treatment group, 94% and 92% in the control group visited the physician for the second checkup. All subjects assigned to the manipulative treatment group visited the manual therapist at least once. The mean number of therapy sessions was 4. Five patients had a lumbar discectomy during the 12–month follow-up: 3 in the manipulative-treatment group and 2 in the consultation group.
A total of 8 out of 204 (3.9%) patients dropped out of the study at the 12–month follow-up. Three subjects could not be reached after moving to an unknown address, and five other subjects did not return the questionnaires for unknown reasons. The trial profile is summarized in Figure 1.
Baseline Characteristics
The manipulative-treatment group and the consultation group were comparable in age, gender, duration and localization of LBP, pain intensity, self-rated disability, depression, and HRQoL (Table 1). The level of education and vocational training in both groups was comparable to that of the Finnish working-age population. The study sample differed from the metropolitan working-age population of Helsinki in that the proportion of white-collar workers was larger (45% vs. 28%) and blue-collar workers smaller (7% vs. 25%). [24] There was no difference between the groups in the use of analgesics for LBP. The percentage of employees were higher in the manipulative-treatment group (99%) than in the consultation group (91%) (P = 0.01). The number of days on sick leave during the previous year was slightly higher in the consultation group (P = 0.07, Mann-Whitney U test). The previous use of health care services (medical services, physiotherapy, chiropractic, massage) was similar in both groups. Tobacco use was equally common in both groups (32% vs. 36%).
Outcomes
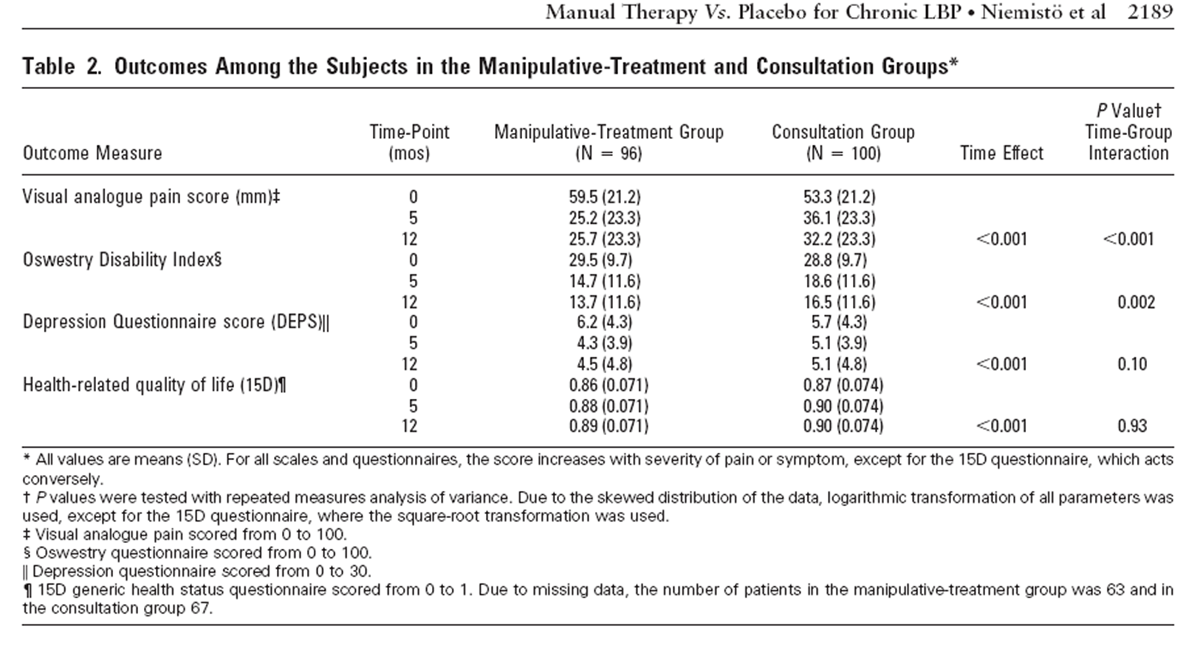
The logarithmic transformation to adjust for the nonnormal distribution was made for the VAS, ODI, and DEPS. The square-root transformation was made for HRQoL. Significant improvement occurred in both groups on every self-rated outcome measure. In the follow-up, significant differences emerged between the groups in pain intensity (P < 0.001, ANOVA) and in self-rated disability (P = 0.002, ANOVA), in favor of the manipulative treatment group. The difference between the groups in self-rated depression was nonsignificant (P = 0.10, ANOVA).
Table 2 At baseline, 58% of the subjects in the manipulative treatment group and 62% in the consultation group reported daily LBP. At the 12–month follow-up, the percentage of daily LBP reported decreased to 37% (P = 0.001, McNemar Symmetry χ2) in the manipulative treatment group and to 39% (P < 0.001) in the consultation group. There were no statistically significant differences in change between the groups. The proportion of the patients using analgesics for their back pain decreased from 32% to 23% in the manipulative-treatment group and from 36% to 26% in the consultation group. Both groups showed clinically and statistically significant increases in HRQoL (P < 0.001, ANOVA). However, the groups did not differ at the 12–month follow-up (P = 0.93, ANOVA) (Table 2).
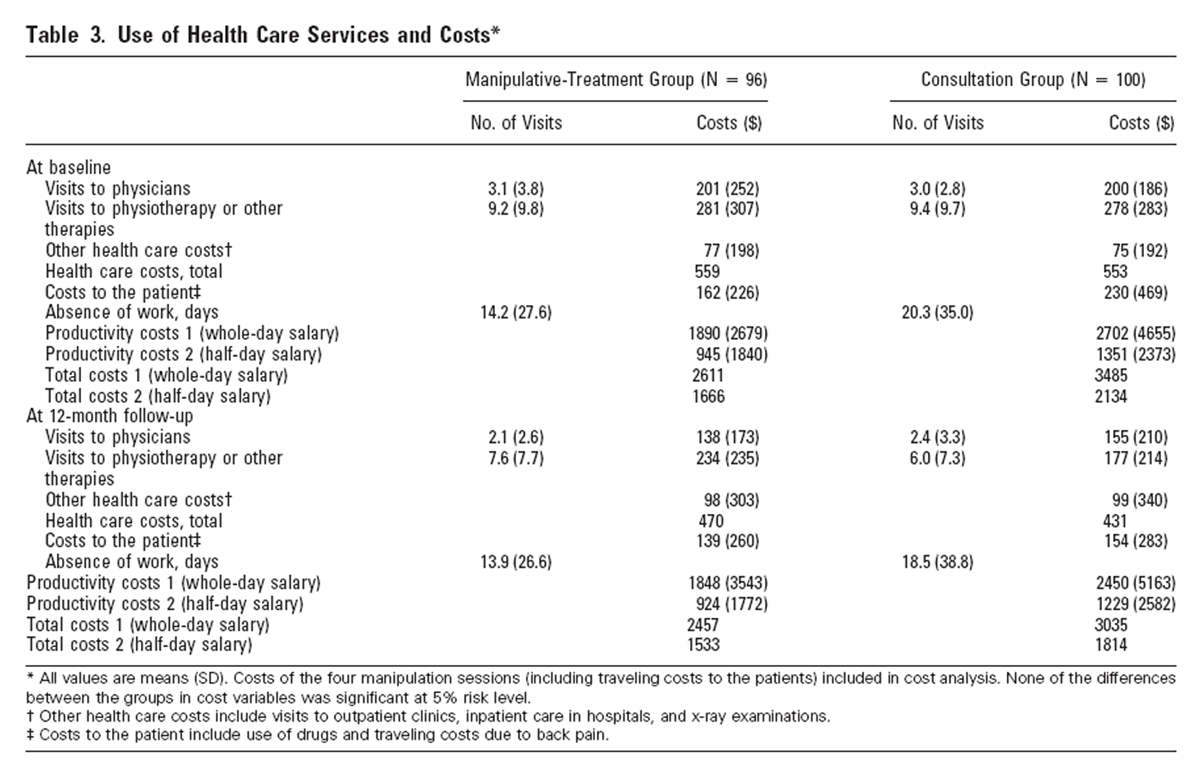
Table 3 In both groups, the number of visits to physicians or use of physiotherapy or manual therapy decreased during the 12–month follow-up, but no significant difference existed between the groups. Use of other health services, such as hospital services, was minor in both groups, and changes in these were also very small and nonsignificant (Table 3).
Absence from work during the previous 12 months already differed slightly between the groups at baseline, but this difference was not statistically significant (P = 0.07, Mann-Whitney U test). The difference was not explained by the employment status. In the consultation group, the number of sick leave days decreased an average of 2 days during the 12–month follow-up, whereas in the manipulative-treatment group, the decrease was smaller. The variance in productivity costs was large, and consequently the difference between the groups was not statistically significant (mean change P = 0.46, Mann- Whitney U test). Nevertheless, the total costs decreased $154 in the manipulative-treatment group and $450 in the consultation group at the 12–month follow-up compared to baseline costs (Table 3). Incremental analysis showed that a one-point change in VAS scale cost $23 with manipulative treatment compared to the physician consultation. Neither group reported adverse effects.
Discussion
This study showed that manipulative treatment with stabilizing exercises and physician consultation reduced self-rated disability and pain more than did physician guidance and an educational booklet alone. However, both groups also showed significant improvement concerning all primary and secondary outcome measures in the follow-up. Visits to physicians, physiotherapy, or other therapies decreased in both groups, which resulted in decreased costs for health care and for the patients.
Previous studies comparing spinal manipulation and physiotherapy [25–28] or standard medical care [29, 30] have found no significant differences in pain intensity and disability. In the study by Cherkin et al, manipulative therapy and physiotherapy separately resulted in limited benefits and higher costs than for the educational booklet. [28] In the study by Koes et al, manipulative therapy and physiotherapy showed better outcomes than continued treatment by general practitioners. [25] Data on the effectiveness of patient information from an educational booklet on LBP are controversial. [31–33] The effect of an educational booklet appears to increase with personal contact with a medical professional. [34] Two Norwegian studies showed that early intervention with examination, information, and recommendations for remaining active reduced sickness leaves. [8, 35–37]
All of the studies have focused on patients with acute to subchronic pain, during which period the natural recovery rate is considerable. In our study focused on CLBP patients, to achieve longer-lasting effects, we combined manipulative treatment and stabilizing exercises. Our control group with educational information alone might not totally reflect the natural course of the LBP syndrome. Naturally, the outcomes may be explained by regression to the mean. On the other hand, as the baseline mean duration of low back pain was 8 years (the median duration 6 years) in both groups and the follow- up period was 1 year, the recurrences of the symptoms might as well have been expected. [3] Our consultation approach has also been shown to be effective compared to general practice or usual care in other studies. 8 Besides, total placebo intervention would have been almost impossible to implement, for practical and ethical reasons.
In our experience, this is the first randomized controlled trial evaluating the combined effects of manipulation and stabilizing exercises. The economic consequences have been evaluated thus far in only a small number of similar studies. [27, 30] Our patient sample was adequate for statistical power. Randomization was successful because there were no significant differences in baseline characteristics. The dropout rate was very low (3.9%), suggesting that compliance to the study in both groups was good.
The patients were recruited voluntarily by a widely circulated newspaper advertisement which may have motivated them more than it would the usual CLBP population. However, the study sample was, by and large, comparable, regarding subjective pain and disability, to the CLBP population needing inpatient rehabilitation in Finland. We cannot specify the effect of manipulation, the stabilizing exercises, or the information provided separately.
Both groups received the same information and encouragement by the physician. The manipulative treatment group had four more contacts than did the consultation group, which in itself can be beneficial. A positive association can occur between the number of contacts with providers and improvement of backrelated symptoms. [37] Thus, the improvement in the manipulative- treatment group may partly be due to nonspecific effects such as general encouragement and supporting guidance rather than to specific treatment effects.
Conclusion
For patients with chronic low back pain (CLBP), the short, specific manipulative treatment program with stabilizing exercises and a physician’s clinical examination, information, encouragement, and simple advice was more effective in reducing pain and disability than was merely a physician’s consultation and an educational booklet. Both treatment methods enhanced HRQoL and reduced the use of health-care services and costs. Results within these groups seem clinically significant. Whether the difference in 1–year outcomes between the groups is clinically significant remains debatable. However, patients recovered with no greater costs by the short manipulative-treatment method. We believe that our treatment modality is effective for most mechanical-origin CLBP patients.
Key Points
This randomized controlled trial showed that a short, specific manipulative-treatment program with stabilizing exercises and physician’s clinical examination, information, encouragement, and simple advice was more effective than physician consultation alone in reducing self-assessments of pain and disability for patients with chronic low back pain in a 1–year follow-up.
Further evaluations are needed to identify the patient subgroups that particularly benefit from the manipulative-treatment method and correspondingly the factors predicting the poorer outcome.
References:
van Tulder MW, Koes BW, Bouter LM.
A cost-of-illness study of back pain in The Netherlands.
Pain 1995;62:233–40.Klenerman L, Slade PD, Stanley IM, et al.
The prediction of chronicity in patients with an acute attack of low back pain in a general practice setting.
Spine 1995;20:478–84.Von Korff M.
Studying the natural history of back pain.
Spine 1994; 19(suppl):2041S–2046S.van Tulder MW, Goossens ME, Waddell G, et al, eds.
Conservative Treatment of Chronic Low Back Pain. 1st ed.
Philadelphia, PA: Lippincott Williams & Wilkins; 2000.van Tulder MW, Koes BW, Bouter LM.
Conservative treatment of acute and chronic nonspecific low back pain.
A systematic review of randomized controlled trials of the most common interventions.
Spine 1997;22:2128–56.Richardson C, Jull G.
Muscle control—pain control. What exercises would you prescribe?
Man Ther 1995;1:2–10.O’Sullivan PB, Phyty GD, Twomey LT, et al.
Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with
radiologic diagnosis of spondylolysis or spondylolisthesis.
Spine 1997;22:2959–67.Indahl A, Velund L, Reikeraas O.
Good prognosis for low back pain when left untampered. A randomized clinical trial.
Spine 1995;20:473–7.World Medical Association Declaration of Helsinki.
Ethical principles for medical research involving human subjects.
JAMA 2000;284:3043–5.Fairbank J.
Use of Oswestry Disability Index (ODI).
Spine 1995;20:1535–7.Woerman AL.
Evaluation and Treatment of Dysfunction in the Lumbar-Pelvic-Hip Complex. 2nd ed.
New York, NY: Churchill Livingstone; 1994.van Wingerden J-P, Vleeming A, Kleinrensink G-J, et al.
The Role of the Hamstrings in Pelvic and Spinal Function.
Edinburgh: Churchill Livingstone; 1997.Chun L, editor.
Muscle Energy Techniques. Treating Sacral Dysfunctions.
Philadelphia, PA: Lippincott Williams & Wilkins; 1991.Hamberg J, Bjorklund M, Nordgren B, et al.
Stretchability of the rectus femoris muscle: investigation of validity and intratester reliability of
two methods including X-ray analysis of pelvic tilt.
Arch Phys Med Rehabil 1993;74:263–70.Butler D.
Mobilization of the Nervous System.
Edinburgh: Churchill Livingstone; 1991.Richardson C, Jull G, Hodges P, et al.
Analysis and Treatment of Motor- Control Problems in the Local Muscles of the Lumbopelvic Region. 1st ed.
London: Churchill Livingstone; 1999.Gerlander E, Hurri H, Kaunola R, et al.
[The Back Triumph].
Helsinki: Rehabilitation Center of Orton, Invalid Foundation; 1995.Fairbank JC, Pynsent PB.
The Oswestry Disability Index
Spine (Phila Pa 1976) 2000 (Nov 15); 25 (22): 2940–2952Salokangas R, Stengard E, Poutanen O.
[DEPS - New tool for screening of depression].
Duodecim 1994;110:1141–8.Sintonen H.
15D-measure of health-related quality of life. I. Reliability, validity, and sensitivity
of its health state descriptive system.
National Centre for Health Program Evaluation, Working Paper 41, 1994.Heikkinen K, Hujanen T, Rusanen H.
[Unit Expenses of the Healthcare System in Finland in the Year of 2000].
Helsinki: Stakes; 2001.NQuery 4.0.
Cork: Statistical Solutions Ltd, 2000.SYSTAT 10 Data,
Statistics I, Statistics II.
Chicago. SPSS Inc., 2000.Central Statistics of Finland, 2000.
Koes BW, Bouter LM, van Mameren H, et al.
The effectiveness of manual therapy, physiotherapy, and treatment by the general practitioner
for nonspecific back and neck complaints. A randomized clinical trial.
Spine 1992; 17:28–35.Skargren EI, Oberg BE, Carlsson PG, et al.
Cost and effectiveness analysis of chiropractic and physiotherapy treatment for low back and neck pain.
Six-month follow-up.
Spine 1997;22:2167–77.Skargren EI, Carlsson PG, Oberg BE.
One-year follow-up comparison of the cost and effectiveness of chiropractic and physiotherapy as
primary management for back pain. Subgroup analysis, recurrence, and additional health care utilization.
Spine 1998;23:1875–83; discussion 1884.Cherkin, DC, Deyo, RA, Battie, M, Street, J, and Barlow, W.
A Comparison of Physical Therapy, Chiropractic Manipulation, and Provision
of an Educational Booklet for the Treatment of Patients
with Low Back Pain
New England Journal of Medicine 1998 (Oct 8); 339 (15): 1021-1029Andersson GB, Lucente T, Davis AM, et al.
A comparison of osteopathic spinal manipulation with standard care for patients with low back pain.
N Engl J Med 1999;341:1426–31.Carey TS, Garrett J, Jackman A, et al.
The Outcomes and Costs of Care for Acute Low Back Pain Among Patients
Seen by Primary Care Practitioners, Chiropractors, and Orthopedic Surgeons
New England J Medicine 1995 (Oct 5); 333 (14): 913–917Hazard RG, Reid S, Haugh LD, et al.
A controlled trial of an educational pamphlet to prevent disability after occupational low back injury.
Spine 2000;25:1419–23.Burton AK, Waddell G, Tillotson KM, et al.
Information and advice to patients with back pain can have a positive effect.
A randomized controlled trial of a novel educational booklet in primary care.
Spine 1999;24:2484–91.Roland M, Dixon M.
Randomized controlled trial of an educational booklet for patients presenting with back pain in general practice.
J R Coll Gen Pract 1989;39:244–6.Cherkin DC, Deyo RA, Street JH, et al.
Pitfalls of patient education. Limited success of a program for back pain in primary care.
Spine 1996;21:345–55.Indahl A, Haldorsen EH, Holm S, Reikeras O, Ursin H.
Five-year follow-up study of a controlled clinical trial using light mobilization and an
informative approach to low back pain.
Spine 1998;23:2625–30.Hagen EM, Eriksen HR, Ursin H.
Does early intervention with a light mobilization program reduce long-term sick leave for low back pain?
Spine 2000;25:1973–6.Coxhead CE, Inskip H, Meade TW, et al.
Multicentre trial of physiotherapy in the management of sciatic symptoms.
Lancet 1981;1:1065–8.
Return to WORKERS' COMPENSATION
Return to EXERCISE AND CHIROPRACTIC
Since 5-21-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |