

Advancements in the Management of Spine Disorders This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Best Pract Res Clin Rheumatol. 2012 (Apr); 26 (2): 263–280 ~ FULL TEXT
Scott Haldeman, MD, Professor, Deborah Kopansky-Giles, DC, MSc, Eric L. Hurwitz, DC, PhD, Damian Hoy, BAppSc (Physio), MPH, PhD, W. Mark Erwin, DC, PhD, Simon Dagenais, DC, PhD, MSc, Greg Kawchuk, DC, PhD, Björn Strömqvist, MD, PhD, Nicolas Walsh, MD
Department of Neurology,
University of California,
Irvine, USA.
Spinal disorders and especially back and neck pain affect more people and have greater impact on work capacity and health-care costs than any other musculoskeletal condition. One of the difficulties in reducing the burden of spinal disorders is the wide and heterogeneous range of specific diseases and non-specific musculoskeletal disorders that can involve the spinal column, most of which manifest as pain. Despite, or perhaps because of its impact, spinal disorders remain one of the most controversial and difficult conditions for clinicians, patients and policymakers to manage. This paper provides a brief summary of advances in the understanding of back and neck pain over the past decade as evidenced in the current literature. This paper includes the following sections: a classification of spinal disorders; the epidemiology of spine pain in the developed and developing world; key advancements in biological and biomechanical sciences in spine pain; the current status of potential methods for the prevention of back and neck pain; rheumatological and systemic disorders that impact the spine; and evidence-based surgical and non-surgical management of spine pain. The final section of this paper looks to the future and proposes actions and strategies that may be considered by the international Bone and Joint Decade (BJD), by providers, institutions and by policymakers so that we may better address the burden of spine disorders at global and local levels.
From the FULL TEXT Article:
Introduction
Spinal pain and its associated disorders affect more people and have greater impact on work capacity and health-care costs than any other musculoskeletal condition. Recent studies suggest that, in many societies, spinal disorders are a greater source of disability and impact the consumption of more health-care resources than any other class of diseases or health problems. [1] Despite, or perhaps because of its impact, spinal disorders remain one of the most controversial and difficult conditions for clinicians, patients and policymakers to manage.

Table 1 One of the difficulties in reducing the impact of spinal pain is the wide and heterogeneous range of specific diseases and non-specific musculoskeletal disorders that can involve the spinal column, most of which manifest as spinal pain. These disorders have been classified in multiple ways but the most widely accepted classification includes four well-defined clinical categories as noted in Table 1.
Spinal disorders with serious or systemic pathology. This category includes disorders caused by congenital and developmental abnormalities, neoplasm, infection disorders, systemic inflammatory disorders and serious trauma. It has been reported that serious spinal pathology, however, accounts for only 1–2% of patients who present with symptoms of spinal pain. [2, 3]
Spinal pain with neurological deficits. The primary neurological deficits that fall into this category include compression of nerve roots, the spinal cord or the cauda equina. It has been estimated that 5–10% of patients presenting with low back pain (LBP) have substantial neurologic involvement. [3] In one survey, features of sciatica were reported by 11.6% of those with LBP; unfortunately, this study did not determine the frequency of actual neurological deficits which is estimated to be a considerably smaller percentage. [4] A recent 10–year survey from the US military noted an incidence of cervical radiculopathy at 1.79 per 1000 person-years. [5]
Non-specific spinal pain, which has also been described as mechanical pain or strain accounts for 90% or more of all people who experience spinal pain. There is growing evidence that it is not currently possible to identify the structure, pathology or source of pain in the majority of patients with these symptoms. Clinicians have postulated that pain can be generated by virtually all tissues of the spine and have defined pain syndromes based on the specific tissues, structures or suspected pathology which are assumed to be causing pain. These theories, however, have yet to be widely accepted and many of the testing methods for these suspected diagnoses have yet to be validated.
Spinal pain referred from non-spinal pathology. A number of systemic, abdominal and pelvic pathologies may present as spinal pain. There are no data to determine how frequently this type of referred pain occurs but it is commonly included as a symptom of a number of visceral disorders as listed in Table 1.
Given the broad scope of spinal problems and the impact of these disorders on all societies, irrespective of age, sex or social status, it would be reasonable to expect that there would be a uniform, generally-accepted approach to the assessment and management of these symptoms. Unfortunately, there are numerous studies that have demonstrated that the opposite is true.
In developed or wealthy nations, there is a rapid growth in the proportion of the health-care budgets being spent on the diagnosis and treatment of people with spinal pain. [1] A recent review was able to identify over 200 treatment options available to patients for the management of LBP alone. [6] Very few of these options have been shown to have significant support in the form of evidence. It is also becoming evident that the increased expenditure on the treatment of spinal pain has not had the desirable result and has, in fact, been associated with increasing disability. [1]
On the other hand, in developing countries, governments and other health funders, such as international and non-government organisations, have tended to focus the majority of resources on addressing communicable conditions such as diarrhoea and respiratory infections, and chronic conditions such as spinal pain, have been somewhat ignored. [7] While there are many traditional treatments for spinal disorders in many of these settings, mainstream services for the prevention and management of spinal disorders are minimal, and this is particularly the case in rural areas.
This report discusses a few of the developments and changes in our understanding of this topic over the past decade and assists in prioritising the goals of the Bone and Joint Decade (BJD) for the next 10 years as it applies to spinal disorders.
Burden and trends of spinal disorders
The past decade has greatly increased our understanding of the impact of spinal disorders on society in both developed or high-income countries and developing or ‘under served’ low- and middle-income countries.
Developed countries
The past decade has seen the publication of multiple epidemiologic studies that have demonstrated the widespread, almost universal nature of spinal pain syndromes and the extent of the impact of these symptoms on productivity in wealthy countries with high health expenditures. In the developed countries, LBP has a lifetime prevalence of between 50% and 85%. [8, 9] Point prevalence studies in adults have revealed that between 6% and 35% of the population experience LBP at any one point in time, and 1–year and 1–month period prevalence ranges from 10% to 50% and 21% and 39%, respectively. The incidence of lumbar intervertebral disc herniation is estimated to be only 0.1–0.5% per year. However, degenerative changes and disc abnormalities found in imaging studies, which initially were felt likely to be important, have not been demonstrated to be a causal factor in most cases of back pain. [8] The ranges of prevalence and incidence estimates of back pain among children and adolescents are not markedly different from those of adults. In addition to age and gender, several sociodemographic, physical, behavioural, psychological and psychosocial factors have been found to increase the risk of back pain, including socioeconomic status and level of education, body mass index, smoking and self-perceived health status. Depression and psychological distress are likely both causes and consequences of back and other musculoskeletal pain, all of which are often shared co-morbidities. [10, 11] Physical activity appears to improve prognosis. [12]
The Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders undertook a best-evidence synthesis to estimate the burden and identify determinants of neck pain(a) in the general population,
(b) following traffic collisions and
(c) in workers. [13–15]One-year prevalence estimates in adults ranged from 30% to 50%, though estimates of activity-limiting prevalence were typically less than 10%. [13] Incidence estimates ranged from 0.055 per 1000 person-years for disc herniation with radiculopathy to 213 per 1000 person-years for self-reported neck pain, which appears to peak in middle age. Reported frequencies of neck pain among children and adolescents are similar to those of adults. The incidence of whiplash-associated disorders is at least 300 per 100,000 individuals and appears to have increased markedly over the past 30 years. [14] Risk and prognostic factors for neck pain and disability are largely the same as those for back pain. With the exception of neck pain with radiculopathy, degenerative disc changes do not appear to be associated with neck pain incidence. Psychological distress and poor coping were found to impede recovery whereas physical activity may improve prognosis.
Although not as prevalent as back pain, neck pain is also very common in workers throughout the developed world and results in appreciable disability and reduced productivity. The one-year prevalence of activity-limiting neck pain in workers ranges between 11% and 14%, though 25% to almost 50% of workers experience at least some neck pain during the year. [15] Workers in jobs requiring prolonged sitting, repetitive or precision work or awkward postures are at increased risk of neck pain. LBP is the most common musculoskeletal disorder in the workplace in North America and Europe and the second-most frequent cause of worker absenteeism. [9] One-year prevalence of lost work time due to LBP in the United Kingdom has been estimated to be 11% in men and 7% in women. [16] The lifetime and 1–year prevalence of disabling back pain among workers in the US is an estimated 28% and 8%, respectively, with about 40% of lost work days attributable to disabling pain. [17] Pain and disability frequencies vary according to type of occupation and job demands. High physical load, low job satisfaction, monotonous work, poor social support and high-perceived stress and job demands have been linked to an increased risk of occupational back pain. [18]
Direct health-care costs associated with LBP management are substantial, with estimates from the US ranging from $12.2 billion to $90.6 billion in 1996 and 1998, respectively. [19, 20] Incremental health-care expenditures for adults with spine problems in the US in 2005 were an estimated $85.9 billion representing 9% of the total national expenditure. Indirect costs such as lost productivity and worker absenteeism push the economic burden of back and neck pain even higher. For example, in Australia, indirect costs associated with LBP in 2001 were estimated to be 9 times greater than direct costs. [21]
Evidence strongly suggests that the prevalence of musculoskeletal pain, including back and neck pain and the incidence of whiplash-associated disorder, has increased in recent years in at least some developed countries. [22] More people with back pain sought care from health-care providers as well. In the US, disability claims for musculoskeletal disease increased from 15.2% in 1992 to 28.2% in 2006, and the percentage of persons with spine problems reporting functional limitations increased from 20.6% in 1997 to 28.3% in 2006. [1] Total estimated spine-related expenditures among adults increased 65% between 1997 and 2005 and 82% between 1997 and 2006 in the US, while measures of mental health, physical functioning, work or school limitations and social limitations among adults with spine problems worsened. [1, 23] Heart disease and stroke are the only conditions with significantly higher health-care expenditures.
Developing countries
There is considerable variation in the reported prevalence of spinal problems in low- and middle income countries. The range of point prevalence for LBP is from 1% to 39% [24], and for neck pain is, from 3% to 41%. [25] The difference in prevalence between low- and high-income countries is not significant at the 0.05 level for either lowback or neck pain; however, a positive and significant correlation exists between a country’s Human Development Index and point prevalence. [25] The mean prevalence for both neck and LBP is highest in women and in the oldest age groups. [26, 27] Despite the prevalence differential, based on the most recent prevalence estimates, over four times as many people experience spinal pain at any one point in time in developing countries compared with high-income countries. [26, 27]
Many of the risk factors for spinal pain in high-income countries, such as age, gender, obesity, job demands, anxiety, depression and lack of social support in the workplace [13, 26–28] are also likely associated with spinal pain in low- and middle-income countries. It has been estimated that 80–90% of the population in these countries are involved in ‘heavy work’ [29]; subsistence communities, in particular, face enormous daily demands, and studies have found activities such as the collection of water and farming can increase the risk of spinal pain. [30, 31]
Spinal disorders can have a very large impact on individuals and their families, communities, health systems and businesses. [32, 33] It can present itself in a number of ways, including pain, activity limitations, participation restrictions, carer burden, use of health-care resources and financial burden. A number of studies have demonstrated the impact that spinal pain has on an individual’s ability to perform their daily activities in developing countries. [30, 34] In rural subsistence communities, many of these activities are directly related to the health of the individual and their family. For example, debilitating back pain may impact one’s ability to farm, or collect clean drinking water. A study in Nigeria found individuals with chronic spinal pain were more likely to have mood and substance abuse disorders and activity limitations as well. [35]
The number of people experiencing spinal pain in developing countries is likely to increase in the future. Age is one of the most common risk factors for spinal pain, and the greatest effects of population ageing are predicted in low- and middle-income countries [36]; by 2050, it is predicted there will be over five times as many people over the age of 40 years living in these countries compared to wealthier countries. [36] In addition, the number of people who are obese is expected to increase most dramatically in the developing world over the coming two decades. [37] In urban areas, there is also rapid industrial growth and the prevalence of occupational spinal pain is becoming common. [38] Furthermore, increased motorisation in developing countries is likely to increase the incidence of whiplash-associated disorders and other motor vehicular-related trauma, and while there is relatively little information on the incidence of these disorders in developing countries, one study has estimated that 238,000 people per year die in road crashes in South Asian countries alone, and for every death, there are 20 hospitalisations, 50 emergency room visits and more than 100 minor injuries. [39]
Key developments in research, prevention and management during the last decade
The basic sciences
Over the last century, the spine has been studied with increased specialisation in many different fields of basic and experimental science. As a result, distinct domains of spine-specific knowledge have been created. While each domain is deserving of its own investigative effort, each of these systems contribute to our understanding of the structure, function and pathology that affects the spine. There has been an especially close interaction within the fields of anatomy, neurophysiology, pathology and biomechanics.
A major research focus has been spinal biomechanics with the assumption that a better understanding of how the spine responds to injury and pathology may lead to better prevention efforts and treatment protocols. In the BJD (2000–2010), several investigative areas that originated within the lumbar spine have been applied to the cervical spine. These included the definition of normal kinematics [40], disc pressure measurements and concern regarding alterations in the segment adjacent to a surgical target [41] as well as insight into the mechanisms of whiplash through assessment of facet capsule motion. [42]
While the evaluation of various surgical constructs is a basic activity in spinal biomechanics, the last decade saw the advent of the artificial disc dominate biomechanics testing on the bench top and through modelling [43] as did testing of a variety of materials and procedures associated with vertebroplasty. [44]
Further advances were made in the creation of disc injury as a model for studying the aetiology of degenerative disc disease and its treatment. Specifically, a technique that disrupts the vertebral endplate has been shown to initiate degenerative change in pigs that is similar to humans. [45] Still, a model of disc injury that does not disrupt surrounding tissues has yet to be developed.
A dominant trend in the study of spinal function over the last 10 years has resulted in an explosion of knowledge of the spine at a cellular/molecular level and, as a result, has increased our understanding of the relation between spinal mechanics and cellular function. [46] At the other end of the spectrum, at the gross level, further advancements have been made into the understanding of pathogenesis and progression of disc herniation. [47]
While the intervertebral disc remained an area of intense investigation, the role of muscles in patients with back pain has been an important area of research. For example, the transversus– abdominus muscle has been shown to have altered function in patients with back pain. [48] Furthermore, a delay in this muscle’s reflex response has been observed to be predictive of low back injury in some people. [49]
Basic science studies are starting to be applied to non-surgical treatment modalities as well in an attempt to understand the mechanisms of these common interventions. One example is the observation that subjects who report benefits from spinal manipulation have been reported to have significant changes in spinal stiffness and muscle function compared to subjects who report no benefit. [50]
Attempts to define a pathological cause or pain generator for spinal pain in specific individuals continue to be a significant challenge. The most common theories often involve a presumed association with degenerative changes that can affect the intervertebral disc and/or facet joints. For the past decade, these structures have been the focus of much of the experimental and basic science research.
This research has resulted in an increase in our understanding of the precarious nature of the intervertebral disc nutrient supply and the impact of pH and low oxygen content on disc metabolism and pathology. [51, 52] It is only recently that the in-growth of nociceptive capable neurons, expression of neurotrophic and pain-inducing molecules, increased expression of inflammatory cytokines and a progressive loss of viable disc cells has been associated with degenerative disc disease. [53–55] These observations have led to further interest in the concept of the painful disc. Research efforts involving magnetic resonance imaging (MRI) studies coupled with epidemiological and basic science research have attempted to differentiate abnormal degenerative disc disease from normal ‘aging’. [56, 57] The notion that disc degeneration and ‘normal aging’ might be considered as different conditions may, at some time in the future, allow clinicians to better define patients who are likely to respond to interventions directed at the disc.
The potential use of anabolic growth factors and stem cell therapies for the treatment of degenerative disc disease represents a new approach to manage the process of degenerative disc disease. A number of clinical trials are currently underway to determine whether such approaches can ameliorate spinal pain. There are now attempts to ‘grow’ discs in the laboratory with the hope that an intervertebral disc, inclusive of the endplates, annulus and nucleus pulposus might be manufactured and used for potential surgical replacement. There have been some encouraging results looking at this option in animal trials.
The last decade has led to an almost complete revolution of the notion held not long ago that the intervertebral disc was a rather inert biological structure where now it is recognised that the intervertebral disc is a very complex structure with the potential of causing either directly or indirectly, a host of painful syndromes. The challenge for the next decade will be to decode the fundamental mechanisms central to the contribution of the intervertebral disc to spinal pain and to develop effective and efficacious treatment. The important question behind all this research, however, remains whether these scientific achievements will have any impact upon spinal pain and the burden it poses to the world’s population.
Prevention
Most individuals will experience an episode of back pain at some point in their lifetime. Furthermore, approximately 2/3 of people who have an episode of back pain will suffer recurrences and 1/3 will experience periods of disability [58]. At this time, however, it appears unlikely that a primary episode of back pain can be prevented in most people.
It is the consequences of LBP that may be more relevant in the consideration of prevention initiatives: that is, what can one do to prevent the next episode or minimise its impact? The European Guidelines for Prevention in Low Back Pain [58] identified these consequences as the ‘cost’ to individuals and society – work loss time and productivity, care seeking, health-related quality of life and compensation.
Unfortunately, the evidence surrounding the prevention of LBP is limited. Problematic is the wide variance of external and intrinsic factors influencing the onset and recurrence of back pain. The most powerful risk factor for a new episode of back pain is a history of back pain in the previous 12 months.
Beyond that, the most frequently reported risk factors include:age,
gender,
heavy physical work (frequent bending, twisting, lifting, pulling and pushing),
repetitive work,
static postures and vibrations;
lifestyle factors such as
smoking and obesity;
and psychosocial factors such as
level of education,
LBP beliefs,
depression,
anxiety,
job dissatisfaction,
mental stress at work and
compensation schemes.Common sense would dictate that controlling these risk factors through preventive efforts (e.g., work modification, weight loss and education) may impact the incidence of LBP. Unfortunately, there is little to no evidence to support these or any specific interventions as effective in preventing back pain recurrences or long-term low back disability in the general or working populations.
Several systematic reviews (Cochrane and others) evaluating back pain prevention have been published in the literature within the past decade. The review topics included:exercises for prevention of LBP recurrences [59],
use of lumbar supports [60],
shoe insoles [61],
manual materials handling advice and assistive lifting devices [62],
back schools [63],
individual patient education [64] and
behavioural intervention. [65]None of these reviews found solid evidence that these prevention mechanisms were effective.
Synthesising the results of these reviews as well as other published research and recognising the challenges of the back pain enigma, the European Guidelines working group came to the following conclusions regarding back pain prevention:
physical exercise is recommended to reduce the frequency and duration of repeat episodes of back pain. Unfortunately, no specific exercise approach was favoured.
information and education about back problems should be considered.
further research is required, specifically a need for good quality randomised clinical trials to determine the effectiveness of specific interventions aimed at certain risk/target groups.
Identified study areas included:health promotion programme effectiveness,
impact of daily physical activity,
information aimed at reducing fear-avoidance and demedicalisation of back pain and
the generalisability of different approaches to broad populations (adult, workers and adolescents).Amongst the recent literature reviewed, however, there is emerging, albeit limited evidence that maintaining a healthy weight, stopping smoking and daily physical exercise may have protective effects. These lifestyle approaches have been shown to also have a positive impact on other chronic diseases such as diabetes, cardiovascular disease and others.
Rheumatological and systemic spinal disorders
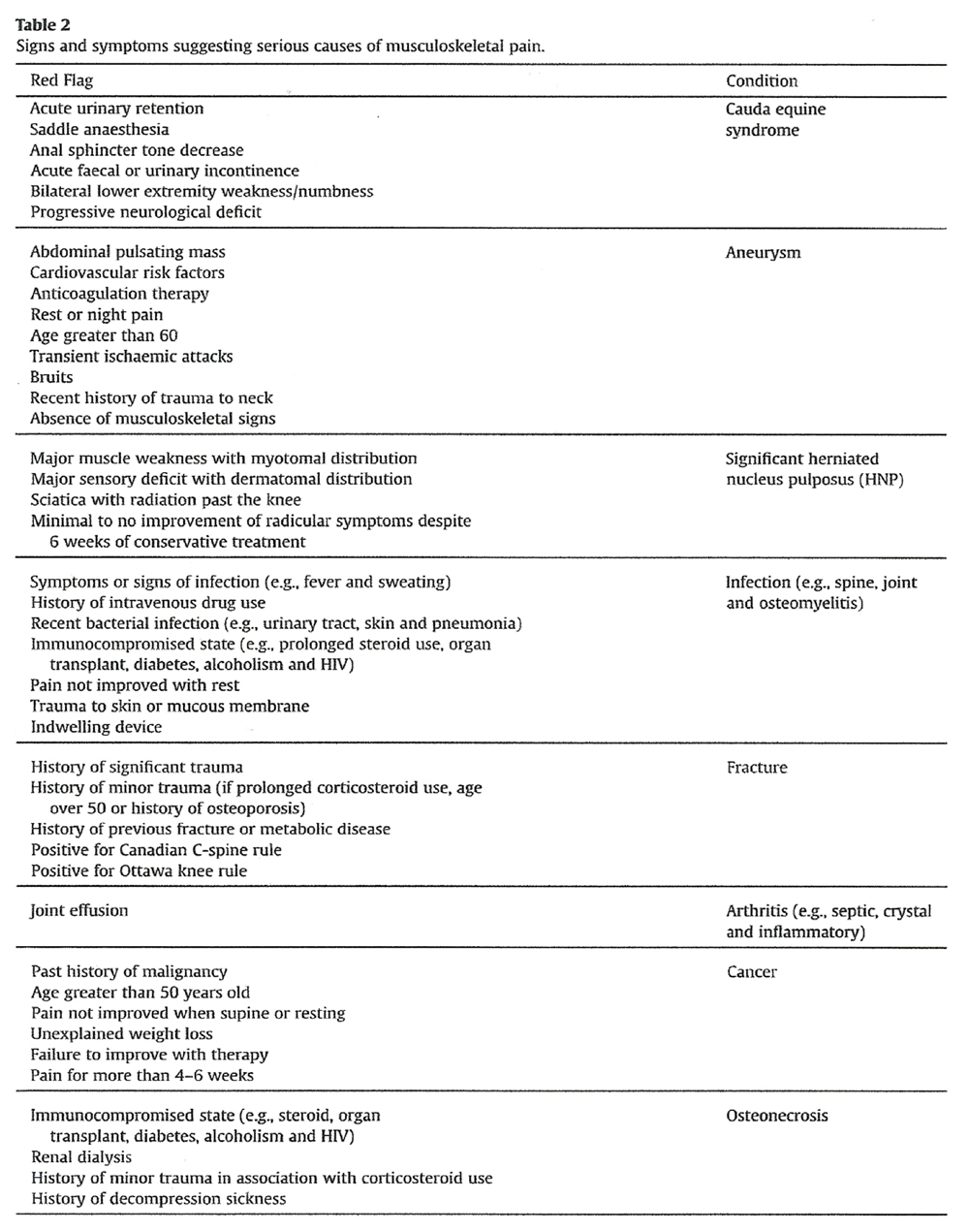
Over the last decade, most professional groups and guideline committees have stressed the importance of differentiating specific local or systemic diseases from non-specific musculoskeletal disorders manifesting as spinal pain. This distinction is now considered paramount in determining appropriate treatment. There is a growing emphasis on the importance of a detailed history and physical examination followed by appropriate studies to make the correct diagnosis and optimally treat. The primary goal of the initial history and physical examination is the identification of the so called ‘red flags’ for serious pathology which are likely to require further investigation.
Table 2 If red flags for serious pathology as noted in Table 2 are identified, then additional testing and a firm diagnosis is necessary to guide treatment.
In the absence of red flags, however, there is a growing realisation that advanced testing is unlikely to positively impact the care patients receive. There is increasing evidence that tests such as imaging in the absence of red flags might actually negatively impact the outcome of patients and prolong disability by reinforcing the perception of the possibility of severe injury.
Evidence-based guidelines and non-surgical care
As the number of clinical trials conducted and published each year on common and innovative diagnostic approaches to spinal disorders continues to increase, often with increasingly sophisticated research methodology, there has been a growing realisation that it is an impossible challenge for most practicing clinicians, patients and policymakers and payers of health-care to read and synthesise all relevant primary studies. To address this problem, there has been considerable focus on the undertaking of high-quality systematic reviews and clinical practice guidelines (CPGs). The methodology through which these clinical guidelines are developed has increased markedly in an attempt to identify, appraise, summarise and synthesise primary research studies to facilitate knowledge transfer for practicing clinicians. [66]Systematic reviews There are now multiple systematic reviews which have been published on the management of neck and LBP by various groups, including the Cochrane Collaboration, an international network of scientists dedicated to conducting methodologically rigorous systematic reviews to answer important clinical questions.
Its Cochrane Back Review Group has conducted systematic reviews for a variety of conditions related to the spine, including:disc disease [67, 68],
failed back surgery [69],
non-specific pain [63],
radiculopathy [70],
spondylosis [71] and
whiplash. [72]A wide range of interventions has been evaluated by the Cochrane Back Review Group, including
acupuncture [73],
bracing [74],
Chinese herbal medicine [67],
education [63],
exercise [59],
injections [75],
massage [76],
medications [77],
modalities [78],
multidisciplinary rehabilitation [79],
radiofrequency denervation [80],
spinal manipulation [81] and
surgery. [71]These systematic reviews now play an important role in determining the most appropriate use for these interventions (if any) in the management of spine pain.
Clinical practice guidelines Several CPGs have also been conducted in the past decade to help guide clinicians, patients, insurers, policymakers and other stakeholders making important decisions about neck pain and LBP. The Bone and Joint Decade Neck Pain Task Force conducted a best-evidence synthesis related to the epidemiology [13–15], diagnosis [82], prognosis [83–85] and treatment [86, 87] of neck pain and its associated disorders, including headache and radiculopathy. Its findings were disseminated in a series of presentations to stakeholders in different countries, and published as special issues of Spine (February 2008), European Spine Journal (April 2008) and the Journal of Manipulative and Physiologic Therapeutics (February 2009) to reinforce important messages.
This task force recommended the use of screening protocols to rule out cervical spine fracture in patients presenting with neck pain who are at high risk, and the use of history, examination and diagnostic imaging or electrodiagnostic testing to diagnose the aetiology of substantial neurologic findings. [79] There was insufficient evidence to support routine use of diagnostic imaging and other testing for the assessment of non-specific neck pain, as findings rarely lead to improved management and outcomes. Non-invasive interventions recommended for neck pain included spinal manipulation or mobilisation, particularly when combined with exercise therapy and patient education, were felt to be supported by the available evidence. [87] Evidence was found to support the use of epidural injections or decompression surgery for short-term improvement of neck pain with radicular symptoms, but not non-specific neck pain. [86]
CPGs related to the assessment and management of LBP have been conducted inAustralia [88],
Belgium [89],
Italy [90],
New Zealand [91],
Norway [3] and the
United States [92, 93], as well as
multinational European efforts. [94–96]A best-evidence synthesis was recently conducted to evaluate and compare 10 multidisciplinary CPGs from the past decade related to the assessment and management of LBP. [66] There was general agreement among the CPGs that clinicians should screen for red flags that may indicate rare but serious spinal pathology, including cancer, cauda equina syndrome, fracture and infection, which may require additional diagnostic laboratory testing or imaging to be ruled out.
Evidence from CPGs suggests that management of spinal disorders should focus on patient education, advice to remain active, and short-term use of acetaminophen, non-steroidal anti-inflammatory drugs, or spinal manipulative therapy to relieve symptoms. If symptoms persist beyond 6 weeks, the addition of therapeutic exercises, behavioural therapy or opioid analgesics can then be considered. A similar approach was recommended for spinal disorders with neurological involvement, although it may be necessary to consider epidural injections or decompression surgery if symptoms are incapacitating or fail to improve with more conservative care.
Surgery
Spine surgery has evolved rapidly over the past 10 years, increasingly based on evidence which has been, to some extent, industry driven and has led to some credibility concerns. [97] There has been an enhanced focus on patient-reported outcomes of surgery. Large national and international registers now emphasise the need for documentation to enable identification of, for example, new methods and inferior surgical techniques and for bench marking. [98] Spine surgery has actually been at the forefront in patient-reported outcome measures (PROMs).
The past decade has seen remarkable growth in the sophistication of research into spinal surgical procedures that hold the promise of greatly advancing our understanding of spinal disorders and which have increased the available treatment options. Stem cell transplantation for disc regeneration has shown promising results but mainly in vitro so far. More complex procedures to address spinal deformities in younger children with expanding sophistication of implants have been developed.
Techniques enabling primary tumour operation en bloc are now being carried out in highly specialised centres. There is increasing research on the use of vertebroplasty or kyphoplasty for painful primary and especially metastatic tumours of the spine. The past decade has seen further development of micro-invasive thermal ablation therapies. In the treatment of fractures, the use of percutaneous fixation techniques has expanded rapidly. The role of vertebroplasty/kyphoplasty in osteoporosis is currently the subject of a great deal of research and debate.
The last decade has seen remarkable growth in the number and sophistication of motion preservation surgical techniques which, to a large extent, are considered a substitution for fusion surgery but, so far, with limited long-term follow-up to determine effectiveness and especially cost-effectiveness. During the same period, inter-spinous implants under local anaesthesia has become the preferred surgical treatment for spinal stenosis replacing open procedures in many patients.
The significance of osteoporosis related to spine disorders on morbidity and mortality has been recognised and has resulted in improved awareness and better secondary prevention through fracture liaison programmes.
Opportunities in the next decade
Realistic goals
There is a growing realisation that it may not be possible to understand fully the impact of spinal disorders without a greater focus on large population-based surveys and longitudinal studies with standardised definitions of pain and disability so that current disease burden, geographic variations and trends over time may be accurately assessed. [26, 27]
There is good reason to expect that some of the advances in spine surgery during the next decade are not even within our frames of references today but the road to some of the improvements has been paved by recent research developments.
Minimising inefficient surgery for pain syndromes through more outcome studies and controlled clinical trials to identify patients likely to benefit from surgery can be expected. Improving clinical preoperative information by open MRI investigation performed in various body/spine positions may help in this regard. Operations in real-time MRI with dedicated non-magnetic instruments and perioperative three-dimensional (3D) navigation is being improved and simplified, making it possible to use in a multitude of spinal procedures on a routine basis, thereby reducing postoperative morbidity. Increasing research on combining synthetic bone substitutes with novel peptides for rapid and improved fusion healing is likely.
Further development of disc implants, mimicking normal disc function with mobility and shock absorption can be expected. The feasibility of stem cell treatment of disc degeneration still needs to be established to see if it is meaningful or possible to reverse the degenerative cascade that may lead to spinal degenerative pain. The host of changes inherent to degenerative disease such as vertebral endplate calcification, progressive apoptosis of nucleus pulposus cells and the development of a progressively more hostile nucleus pulposus ‘milieu’ create significant obstacles to restorative applications within the advanced degenerative disc. Enhancement of nerve regeneration after traumatic lesions of the spinal cord with a combination of peptides and scaffolds holds considerable promise. Establishing more clear indications for vertebroplasty in osteoporotic fractures hopefully will increase our understanding of the value of this procedure. At the same time, implementing knowledge on spine trauma for mechanics in injury prevention and treatment in the developing world and targeted tumour treatment with radio pharmaceuticals against, for example, spine metastases is being developed.
The opportunities for advances in future spine surgery, however, may be more restricted by our own conventional approaches and health economy than by the immense on-going research work in the field.
Consideration of recently developed conceptual models, such as the one for the onset, course and care of neck pain [33] should be explored further.
The thoughtful use of the principles of life-course epidemiology to identify(1) risk and prognostic factors and
(2) critical time points, over the next decade, should be considered a goal to gain greater understanding of potential preventive strategies and treatment approaches. [99]The impact of spinal pain in low- and middle-income countries may be compounded as health promotion and treatment services do not receive the resourcing seen in high-income countries, social security systems are uncommon, and it is rare for individuals to have health insurance. Having said that, many traditional treatments exist in developing countries, and a number of these may be effective at reducing spinal pain and improving function. Further research is needed on how spinal pain affects an individual’s participation, well-being and livelihood in the developing world. Investigating the methods that traditional healers are using to manage spinal disorders may open new windows for research of both psychosocial and physical factors that can help people in other countries with these problems.
It is important to be careful not to prioritise clinical interventions ahead of public health and preventive approaches to reduce the burden of spinal pain and disability. As observed in the United States, dramatically increased spine-related health-care expenditures in the past decade have not resulted in improved health status. [1, 23]
There is a growing recognition that it is important to emphasise studies designed(1) to optimise prevention of pain and disability and
(2) to research knowledge translation projects that publicise effective evidence-based strategies, such as promotion of physical activity, which has health benefits well beyond pain prevention and relief. [100]One realistic goal for the next decade is to encourage researchers to adopt recent recommendations on defining low back and neck pain in epidemiological studies. [33, 101] This goal has the potential to significantly enhance our ability to compare and pool results across studies, and thus significantly improve our understanding of spinal pain.
In developing countries, governments and other aid programme donors have traditionally prioritised high mortality, communicable diseases. [7] With the occurrence and impact from spinal conditions already substantial and likely to increase significantly over the coming decades, further research is needed to improve understanding of the occurrence, course, impact, risk factors and potential interventions for spinal pain in these countries. [29, 30, 102] The increasing World Health Organisation (WHO) focus on non-communicable diseases (NCDs), and the inclusion of musculoskeletal disorders within this initiative, has the potential to help direct resources towards research, prevention and treatment efforts.
A key focus of research and interventions in any context, and particularly in low- and middle income countries, should include local participation, ownership and coordination. [103] Research and any interventions should be integrated with existing mechanisms and structures where possible. National planning and policy development is needed. Advocacy and resource mobilisation are critical primary steps to these processes. In many places, it will be necessary to build local capacity in research methods and approaches to the prevention and management of spinal pain. In addition, programmes should adopt a shared-risk factor approach and be longitudinal or population-based where relevant. Attention should also be paid to cost effectiveness of interventions.
Although there are numerous high-quality guidelines for the management of neck and back pain, there remain areas of discrepancy between these guidelines that need to be resolved. One goal being considered by the BJD is to reconcile the differences between these guidelines and increase the scope of the guidelines. Also, many of the current guidelines are suitable only for the developed nations with access to advanced testing and high-tech treatment methods. They often do not apply to countries and communities where there are limited financial resources and clinical expertise. For example, it would be both beneficial and realistically possible to develop guidelines that include a review of the current evidence for the management of spinal deformities, spinal cord injuries, fractures and other red flag diseases to guide clinicians in the management of these more serious spinal disorders. This would require the establishment of an infrastructure for international, multidisciplinary collaboration on research and education which may be facilitated by the BJD.
Barriers and facilitators to achieving the goals
There are multiple barriers to reaching the goals noted above that will have to be addressed if we hope to advance our understanding and management of spinal disorders over the next decade. They include:(1) obtaining consensus from various stakeholders on definitions of conditions and outcomes. Without consensus on these definitions, it will be difficult to compare and analyse the results from different studies
(2) the utilisation of these case definitions in population-based surveys and longitudinal cohort studies needs encouragement and monitoring. In some instances, access to large national and stakeholder databases will be very useful even though these may be incomplete.
(3) unfortunately, certain stakeholders in the medical – pharmaceutical – surgical – industrial complex may perceive the research as not financially beneficial. There are already indications that certain stakeholders do not feel comfortable with the increased attention on prevention and low tech, low cost management of spinal pain. Recently, some of these stakeholders have actually walked away from interdisciplinary task forces or committees and elected to develop single-profession guidelines that support their approach to spinal pain. [104]
(4) research funding in the current economic climate is considerably challenging.
(5) researchers from low- and middle-income economies may, in some cases, experience greater barriers to research, such as difficulties in constructing accurate sampling frames, and accessing remote regions and villages. This can greatly add to the challenge of publishing academically rigorous studies. Further to this, the majority of peer-reviewed journals only accept submissions in English.There are, however, a number of factors that are facilitating the achievement of the goals.
(1) data showing increased prevalence of reported pain, disability and health-care expenditures have stressed the need to identify modifiable factors to reduce the individual and societal burden of spinal disorders.
(2) policymakers’ increased attention to the importance of health-care costs and comparative effectiveness of research in improving efficiency and quality of health-care.
Specific strategies/actions and who should undertake them
There are a number of relatively simple strategies that can be undertaken by the BJD to advance these goals. There are two feasible approaches that should be considered.
The first is geared towards obtaining the data necessary to convince stakeholders to support future projects to advance the health of people with spinal disorders.
This strategy should use the following steps:(1) establish musculoskeletal disorders, including spinal conditions, as a priority within the WHO non-communicable diseases initiative such that collaborative global efforts can be directed towards broad surveillance studies and towards funding of research, treatment and prevention programmes both at international and local levels.
(2) establish a multidisciplinary, international committee with wide representation from both clinical and epidemiological fields to develop standard definitions of low back and neck pain for use by researchers, policymakers and clinicians.
(3) work with national authorities and the WHO to help facilitate the development of culturally appropriate initiatives to address and mitigate the growing burden of spinal pain. Design and implement large, long-term population-based cohort studies focussed on musculoskeletal health and associated co-morbidities.
(4) improve awareness and education of the public and policymakers using social media, online tools, education systems and public health and entertainment entities to disseminate a common message and work towards making spine care a priority when research and health-care priorities are being considered.
Another feasible approach is to work towards increasing the standard of care available to people with spinal disorders.
This strategy should use the following steps:(1) establish a multidisciplinary, international committee with wide representation from both clinical and epidemiological fields to distil existing guidelines from multiple disciplines to identify areas of consensus.
(2) develop a methodology to assess the available guidelines on back and neck pain and to reconcile the differences between guidelines.
(3) work with national authorities to adapt guidelines so they are culturally appropriate and useful in developing nations.
(4) develop a methodology to produce guidelines for conditions such as red flags disorders and deformities where there are unlikely to be randomised or other controlled clinical trials.
(5) work with all relevant stakeholders to develop, implement, monitor and evaluate a guideline dissemination plan.
A feasible and realistic timeline
The timeline for these objectives will depend largely on obtaining appropriate levels of funding and commitment from governments, professional societies, public health organisations and the research community.
There are a number of initiatives that are already in the pipeline that should facilitate this process. For example, the global burden of low back and neck pain is currently being estimated as part of the Global Burden of Disease Study 2005/2010 and results will be available in 2012. [8, 23] The Burden of Disease rankings compare the amount of death and disability caused by disease. Global Burden of Disease studies provide these rankings for the world and its major regions, and governments often consider these when assessing health priorities, allocating resources and evaluating the potential costs and benefits of public health interventions.
The development of the World Spine Care Initiative is establishing multidisciplinary spine care centres in underserved communities in a number of countries and is cooperating with government health ministries and local hospitals to provide services. An underlying theme throughout this initiative will be ensuring that the planning and decision-making processes are locally owned and driven, that extensive community consultation takes place to facilitate this ownership and improve the likelihood of sustainability, and that the services themselves are integrated with existing policy and structures to avoid duplication and ensure that busy staff are not being pulled away from their usual activities.
The approach of the centres will be decided in close cooperation with the local community; traditional treatments will likely complement treatments such as physiotherapy and chiropractic care. For more Western concepts such as physiotherapy and chiropractic, no treatments will be recommended unless they are evidenced based. A key concept for the capacity-building activities will be to ensure that capacity can be applied to other areas of people’s work outside of spine care (e.g., project management, monitoring and evaluation, research methods, etc.).
More broadly, the initiative will partner with other organisations and government departments to develop public health campaigns that target risk factors that are shared among the chronic diseases (e.g., physical inactivity). This initiative as a whole will be informed through local research on the burden and perceived causes of spinal pain in these communities, the ways that people manage their spinal pain (including treatment) and other ways to address this burden. This initiative, still in its early development stages, commenced in 2011 and has begun work in Botswana and India.
The BJD has committed to forming a Multidisciplinary Guideline Development Committee with the goal of distilling existing guidelines from multiple disciplines to identify areas of consensus. The goal is to develop and culturally adapt evidence-based, practical, multidisciplinary, patient-centred guidelines for prevention and management of spinal disorders by 2015.
The BJD has also made the decision to improve awareness and to initiate a public education programme using social media, online tools, education systems, public health and entertainment entities to disseminate a common message and work towards prevention. It is expected that by 2015 there will be a concerted effort to empower patients to participate in care, as well as to target primary-care physicians and home-education programmes for community-based spine care.
Measurement of success and outcome of future goals
The ultimate goals of the BJD initiatives are to see a measurable reduction in:(1) reports of back and neck pain and related disability in population surveys and cohort studies;
(2) workers’ compensation and personal injury claims and costs; and
(3) interventional health-care services and costs associated with chronic spine pain and disability.These goals can be measured by accessing annual national population-based surveys and long-term prospective studies using validated outcome measures of pain, function and quality of life. Adoption of the International Classification of Diseases (ICD) coding by all countries will enable such tracking and contribute greatly to our understanding of the true burden of spinal disorders worldwide. The interim initial measurement of success will be the ability to mobilise the financial resources to initiate the recommended research and to develop the Committees tasked to develop the terminology and guideline projects.
Assuming the funding for the research projects and task forces is achieved and the projects are mobilised and become functional, the next measurement of success will be the publication of the conclusions of these committees. Once published, success will be determined by the ability of the BJD to disseminate the findings and ensure that patients and primary-care physicians are aware and are using guidelines for community-based spine care.
Conclusions
The last decade has seen an exponential increase in the amount of research devoted to spinal disorders. This research has been notable in the field of epidemiology and population-based research, experimental studies into disc pathology, neurophysiology and spinal biomechanics, the assessment of the efficacy of diagnostic techniques and prevention approaches, the introduction of advanced surgical techniques and the development of clinical guidelines.
This research has provided a set of tools and level of understanding that should allow for a much more rational and consistent approach to spinal disorders throughout the world and allow for some determination of the resources and personnel necessary to reduce the burden of this disorder on societies in both developed and developing countries.
At a June 2011 UN meeting on the WHO launch of the NCDs Initiative, a leading world health economist described NCDs as “an emergency in slow motion” and advised that by 2050, 50% of the world’s middle- and low-income countries will be bankrupted by the weight of NCDs if nothing is done.
We know that musculoskeletal disorders, and, in particular back and neck pain, are significant contributors to this burden. It is imperative that we act collectively and collaboratively to address spinal disorders and pain, to prevent the devastating impact it has at both personal and societal levels.
Acknowledgement
The authors would like to acknowledge Mr. Ngai Chow for his contribution to formatting the manuscript and references.
REFERENCES:
Martin, BI, Deyo, RA, Mirza, SK et al.
Expenditures and Health Status Among Adults With Back and Neck Problems
JAMA 2008 (Feb 13); 299 (6): 656–664Gozna E.
Guidelines for the diagnosis and treatment of low back pain.
New Brunswick, Canada: Workplace Health,
Safety and Compensation Commission of New Brunswick; 2001.The Norwegian Back Pain Network.
Acute low back pain: interdisciplinary clinical guidelines.
Oslo, Norway: The Norwegian Back Pain Network, Communication Unit; 2002.Deyo RA, Tsui-Wu YJ.
Descriptive epidemiology of low-back pain and its related medical care in the United States.
Spine 1987;12(3):264–8.Schoenfeld AJ, George AA, Bader JO, Caram PM.
Incidence and epidemiology of cervical radiculopathy in the United States military: 2000 to 2009.
J Spinal Disord Tech 2012 Feb;25(1):17–22.Haldeman S, Dagenais S.
A Supermarket Approach to the Evidence-informed Management of Chronic Low Back Pain
Spine Journal 2008 (Jan); 8 (1): 1–7Beaglehole R, Yach D.
Globalisation and the prevention and control of non-communicable disease: the neglected chronic diseases of adults.
Lancet 2003;263:903–8.Hurwitz E, Shekelle PG.
Low back syndromes: integrated clinical management.
New York: McGraw-Hill Publishers; 2006.
Epidemiology of low back syndromes; pp.83–118.Hoy D, March L, Brooks P,Woolf A, Blyth F, Vos T, et al.
Measuring the global burden of low back pain.
Best Practice and Research Clinical Rheumatology 2010;24(2):155–65.Hurwitz EL, Morgenstern H, Yu F:
Cross-sectional and Longitudinal Associations of Low-back Pain
and Related Disability with Psychological Distress Among
Patients Enrolled in the UCLA Low-Back Pain Study
Journal of Clinical Epidemiology 2003 (May); 56 (5): 463–471Hurwitz EL, Morgenstern H.
Correlates of back problems and back-related disability in the United States.
Journal of Clinical Epidemiology 1997;50(6):669–81.Hurwitz EL, Morgenstern H, Chiao C.
Effects of Recreational Physical Activity and Back Exercises on Low Back Pain
and Psychological Distress: Findings from the UCLA Low Back Pain Study
Am J Public Health. 2005 (Oct); 95 (10): 1817–1824Hogg-JohnsonS, van derVelde G, Carroll LJ, HolmLW, Cassidy JD,GuzmanJ, et al.
The Burden and Determinants of Neck Pain in the General Population: Results of the
Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S39–51Holm LW, Carroll LJ, Cassidy JD, Hogg-Johnson S, Cote P, Gusman J, et al.
The Burden and Determinants of Neck Pain in Whiplash-associated Disorders after Traffic Collisions:
Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S52-59Cote P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al.
The Burden and Determinants of Neck Pain in Workers: Results of the
Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S60-74Walsh K, Cruddas M, Coggon D.
Low back pain in eight areas of Britain.
Journal of Epidemiology and Community Health 1992;46(3):227–30.Social Security Administration.
Annual statistical report on the social security disability insurance program.
Baltimore, MD: Office of Research Evaluation and Statistics; 2006.National Research Council and the Institute of Medicine.
Musculoskeletal Disorders and the Workplace:
Low Back and Upper Extremities
Washington, DC: National Academy Press; 2001.Druss BG, Marcus SC, Olfson M, Pincus HA.
The most expensive medical conditions in America.
Health Affairs (Milwood) 2002;21(4):105–11.Luo X, Pietrobon R, Sun SX, et al.
Estimates and Patterns of Direct Health Care Expenditures Among Individuals
with Back Pain in the United States
Spine (Phila Pa 1976) 2004 (Jan 1); 29 (1): 79–86Walker BF, Muller R, Grant WD.
Low back pain in Australian adults: the economic burden.
Asia Pacific Journal of Public Health 2003;15(2):79–87.Harkness EF, Macfarlane GJ, Silman AJ, McBeth J.
Is musculoskeletal pain more common now than 40 years ago?:
Two population-based cross-sectional studies.
Rheumatology (Oxford) 2005;44(7):890–5.Martin BI, Turner JA, Mirza SK, Lee MJ, Comstock BA, Deyo RA.
Trends in Health Care Expenditures, Utilization, and Health Status Among US Adults
With Spine Problems, 1997-2006
Spine (Phila Pa 1976). 2009 (Sep 1); 34 (19): 2077–2084Hoy DG, Bain C, Williams G, March L, Brooks P, Blyth F, et al.
A systematic review of the global prevalence of low back pain.
Arthritis Rheumatology; 2012 Jan 9 [Epub].Hoy DG.
Personal communication. 2011.Hoy DG, Protani M, De R, Buchbinder R.
The epidemiology of neck pain.
Best Practice and Research Clinical Rheumatology 2010;24(6):783–92.Hoy DG, Brooks P, Blyth F, Buchbinder R.
The epidemiology of low back pain.
Best Practice and Research Clinical Rheumatology 2010;24(6):769–81.Haldeman S, Carroll L, Cassidy JD, Schubert J, Nygren A.
The Bone and Joint Decade 2000–2010 Task Force on Neck Pain
and Its Associated Disorders: Executive Summary
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S5–7Volinn E.
The epidemiology of low back pain in the rest of the world: a review of surveys
in low- and middle-income countries.
Spine 1997;22(15):1747–54.Hoy D, Toole MJ, Morgan D, Morgan C.
Low back pain in rural Tibet.
Lancet 2003;361(9353):225–6.Geere JA, Hunter PR, Jagals P.
Domestic water carrying and its implications for health: a review and mixed methods
pilot study in Limpopo Province, South Africa.
Environmental Health 2010;9:52.Haldeman S, Carroll L, Cassidy JD.
Findings From the Bone and Joint Decade 2000 to 2010 Task Force
on Neck Pain and its Associated Disorders
Journal of Occupational and Environmental Medicine 2010 (Apr); 52 (4): 424–427Guzman J, Hurwitz EL, Carroll LJ, Haldeman S, Cote P, Carragee EJ, et al.
A New Conceptual Model Of Neck Pain: Linking Onset, Course, And Care
Results of the Bone and Joint Decade 2000–2010 Task Force on
Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S14–23Chopra A, Abdel-Nasser A.
Epidemiology of rheumatic musculoskeletal disorders in the developing world.
Baillieres Best Practice and Research Clinical Rheumatology 2008;22(4):583–604.Gureje O, Akinpelu AO, Uwakwe R, Udofia O, Wakil A.
Comorbidity and impact of chronic spinal pain in Nigeria.
Spine 2007;32(17):E495–500.The World Bank.
Population projections [Internet] [cited 2011 June 15].
Available from, http://web.worldbank.org/; 2011.Kelly T, Yang W, Chen CS, Reynolds K, He J.
Global burden of obesity in 2005 and projections to 2030.
International Journal of Obesity (London) 2008;32(9):1431–7.Joshi TK, Menon KK, Kishore J.
Musculoskeletal disorders in industrial workers of Delhi.
International Journal of Occupational and Environmental Health 2001;7(3):217–21.Rahman AF.
The burden of road traffic injuries in South Asia: a commentary.
Journal of College of Physicians and Surgeons Pakistan 2004;14(12):707–8.Bogduk N, Mercer S.
Biomechanics of the cervical spine. I: normal kinematics.
Clinical Biomechanics 2000;15(9):633–48.Eck JC, Humphreys SC, Lim TH, Jeong ST, Kim JG, Hodges SD, et al.
Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion.
Spine 2002;27(22):2431–4.Pearson AM, Ivancic PC, Ito S, Panjabi MM.
Facet joint kinematics and injury mechanisms during simulated whiplash.
Spine 2004;29(4):390–7.Goel VK, Grauer JN, Patel TC, Biyani A, Sairyo K, Vishnubhotla S, et al.
Effects of charite artificial disc on the implanted and adjacent spinal segments mechanics using a hybrid testing protocol.
Spine 2005;30(24):2755–64.Liebschner MA, Rosenberg WS, Keaveny TM.
Effects of bone cement volume and distribution on vertebral stiffness after vertebroplasty.
Spine 2001;26(14):1547–54.Holm S, Holm AK, Ekstrom L, Karladani A, Hansson T.
Experimental disc degeneration due to endplate injury.
Journal of Spinal Disorders and Techniques 2004;17(1):64–71.Lotz JC, Chin JR.
Intervertebral disc cell death is dependent on the magnitude and duration of spinal loading.
Spine 2000;25(12):1477–83.Tampier C, Drake JD, Callaghan JP, McGill SM.
Progressive disc herniation: an investigation of the mechanism using radiologic, histochemical, and microscopic dissection techniques on a porcine model.
Spine 2007;32(25): 2869–74.Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC.
Experimental muscle pain changes feedforward postural responses of the trunk muscles.
Experimental Brain Research 2003;151(2):262–71.Cholewicki J, Silfies SP, Shah RA, Greene HS, Reeves NP, Alvi K, et al.
Delayed trunk muscle reflex responses increase the risk of low back injuries.
Spine 2005;30(23):2614–20.Fritz JM, Koppenhaver SL, Kawchuk GN, Teyhen DS, Hebert JJ, Childs JD.
Preliminary Investigation of the Mechanisms Underlying the Effects of Manipulation:
Exploration of a Multivariate Model Including Spinal Stiffness,
Multifidus Recruitment, and Clinical Findings
Spine (Phila Pa 1976). 2011 (Oct 1); 36 (21): 1772-1781Urban JPG, Roberts S.
Degeneration of the intervertebral disc.
rthritis Research and Therapy 2003;5(3):120–30.Bibby SR, Jones DA, Lee RB, Yu J, Urban JPG.
The pathophysiology of the intervertebral disc.
Joint, Bone, Spine 2001; 68(6):537–42.Freemont AJ, Watkins A, Le Maitre C, Baird P, Jeziorska M, Knight MT, et al.
Nerve growth factor expression and innervation of the painful intervertebral disc.
Journal of Pathology 2002;197(3):286–92.Burke JG,Watson RWG, McCormack D, Dowling FE,Walsh MG, Fitzpatrick JM.
Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators.
Journal of Bone and Joint Surgery British 2002;84(2):196–201.Le Maitre CL, Freemont AJ, Hoyland JA.
The role of interleukin-1 in the pathogenesis of human intervertebral disc degeneration.
Arthritis Research and Therapy 2005;7(4):R732–45.Rajasekaran S, Vidyadhara S, Subbiah M, Kamath V, Karunanithi R, Shetty A, et al.
ISSLS prize winner: a study of effects of in vivo mechanical forces on human lumbar discs with scoliotic disc as a biological model: results from serial postcontrast diffusion studies, histopathology and biochemical analysis of twenty-one human lumbar Scoliotic discs.
Spine 2010;35(21):1930–43.Rajasekaran S, Venkatadass K, Naresh Babu J, Ganesh K, Shetty AP.
Pharmacological enhancement of disc diffusion and differentiation of healthy, ageing and degenerated discs: results from in-vivo serial post-contrast MRI studies in 365 human lumbar discs.
European Spine Journal 2008;17(5):626–43.Burton A, Balague F, Cardon G, Eriksen HR, Henrotin Y, Lahad A, et al.
European Guidelines for Prevention in Low Back Pain
Bergen, Norway: European Commission Research Directorate General; 2004.Choi BK, Verbeek JH, TamWW-S, Jiang JY.
Exercises for prevention of recurrences of low-back pain.
Cochrane Database of Systematic Reviews 2010;(1):CD006555.van Duijvenbode IC, Jellema P, van Poppel MN, van Tulder MV.
Lumbar supports for prevention and treatment of low back pain.
Cochrane Database of Systematic Reviews 2008;(2):CD001823.Sahar T, Cohen MJ, Uval-Ne’eman V, Kandel L, Odebiyi DO, Lev I, et al.
Insoles for the prevention and treatment of back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group.
Spine 2009;34(9): 924–33.Verbeek JH, Martimo KP, Karppinen J, Kuijer PP, Viikari-Juntura E, Takala EP.
Manual material handling advice and assistive devices for preventing and treating back pain in workers.
Cochrane Database of Systematic Reviews 2011;(6): CD005958.Heymans MW, van Tulder MW, Esmail R, Bombardier C, Koes BW.
Back schools for non-specific low-back pain.
Cochrane Database of Systematic Reviews 2004;(4):CD000261.Engers AJ, Jellema P, Wensing M, van der Windt DA, Grol R, van Tulder MW.
Individual patient education for low back pain.
Cochrane Database of Systematic Reviews 2008;(1):CD004057.Henschke N, Ostelo RW, van Tulder MW, Vlaeyen JW, Morley S, Assendelft JW, et al.
Behavioural treatment for chronic low-back pain.
Cochrane Database of Systematic Reviews 2010;(7):CD002014.Dagenais S, Tricco AC, Haldeman S.
Synthesis of Recommendations for the Assessment and Management of Low Back Pain
From Recent Clinical Practice Guidelines
Spine J. 2010 (Jun); 10 (6): 514–529Trinh K, Cui X,Wang YJ.
Chinese herbal medicine for chronic neck pain due to cervical degenerative disc disease.
Spine 2010;35(24):2121–7.Jacobs W, Willems PC, van Limbeek J, Bartels R, Pavolv P, Anderson PG, et al.
Single or double-level anterior interbody fusion techniques for cervical degenerative disc disease.
Cochrane Database of Systematic Reviews 2011;(1): CD004958.Mailis-Gagnon A, Furlan A, Sandoval JA, Taylor RS.
Spinal cord stimulation for chronic pain.
Cochrane Database of Systematic Reviews 2004;(3):CD003783.Haines T, Gross A, Burnie SJ, Goldsmith CH, Perry L.
Patient education for neck pain with or without radiculopathy.
Cochrane Database of Systematic Reviews 2009;(1):CD005106.Gibson JA, Waddell G.
Surgery for degenerative lumbar spondylosis.
Cochrane Database of Systematic Reviews 2005;(4):CD001352.Verhagen AP, Scholten-Peeters GG, van Wijngaarden S, de Bie RA.
Conservative treatments for whiplash.
Cochrane Database of Systematic Reviews 2007;(2):CD003338.Trinh K, Graham N, Gross A, Goldsmith CH, Wang E, Cameron ID, et al.
Acupuncture for neck disorders.
Cochrane Database of Systematic Reviews 2006;(3):CD004870.Negrini S, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N.
Braces for idiopathic scoliosis in adolescents.
Cochrane Database of Systematic Reviews 2010;(1):CD006850.Staal JB, de Bie RA, de Vet HCW, Hlidebrandt J, Nelemans P.
Injection therapy for subacute and chronic low back pain:
an updated Cochrane review.
Spine 2009;34(1):49–59.Furlan AD, Imamura M, Dryden T, Irvin E.
Massage for low-back pain.
Cochrane Database of Systematic Reviews 2008;(4):CD001929.Roelofs PD, Deyo RA, Koes BW, Scholen RJ, van Tulder MW.
Non-steroidal anti-inflammatory drugs for low back pain.
Cochrane Database of Systematic Reviews 2008;(1):CD000396.Kroeling P, Gross A, Goldsmith CH, Burnie SJ, Haines T, Graham N, et al.
Electrotherapy for neck pain.
Cochrane Database of Systematic Reviews 2009;(4):CD004251.Karjalainen K, Malmivaara A, Mutanen P, Roine R, Hurri H, Pohjolainen T.
Mini-intervention for subacute low back pain: two-year follow-up and modifiers of effectiveness.
Spine 2004;29(10):1069–76.Niemisto L, Kalso E, Malmivaara A, Seitsalo S, Hurri H.
Radiofrequency denervation for neck and back pain.
A systematic review of randomized controlled trials.
Cochrane Database of Systematic Reviews 2003;(1):CD004058.Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for chronic low-back pain.
Cochrane Database of Systematic Reviews 2011;(2):CD008112.Nordin M, Carragee EJ, Hogg-Johnson S, Weiner SS, Hurwitz EL, Peloso PM, et al.
Assessment of Neck Pain and Its Associated Disorders:
Results of the Bone and Joint Decade 2000–2010 Task Force on
Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S101–S122Carroll, LJ, Hogg-Johnson, S, van der Velde, G et al.
Course and Prognostic Factors for Neck Pain in the General Population:
Results of the Bone and Joint Decade 2000–2010 Task Force
on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S75–82Carroll LJ, Hogg-Johnson S, Cote P, van der Velde G, Holm LW, et al.
Course and Prognostic Factors for Neck Pain in Workers: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S93–100Carroll LJ, Holm LW, Hogg-Johnson S, Cote P, Cassidy JD, Haldeman S, et al.
Course and Prognostic Factors for Neck Pain in Whiplash-associated Disorders (WAD): Results of the Bone
and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S83–92Carragee EJ, Hurwitz EL, Cheng I, Carroll LJ, Nordin M, Guzman J, et al.
Treatment of Neck Pain: Injections and Surgical Interventions: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S153–169Hurwitz, EL, Carragee, EJ, van der Velde, G et al.
Treatment of Neck Pain: Noninvasive Interventions: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S123–152Australian Acute Musculoskeletal Pain Guidelines Group.
Evidence-based Management of Acute Musculoskeletal Pain
Brisbane, Australia: Australian Academic Press Pty. Ltd; 2003.Nielens H, van Zundert JMP, Gailly J, Mairiaux P, Van Den Hecke N, et al.
Chronic Low Back Pain
Brussels, Belgium: Belgian Health Care Knowledge Centre; 2006
[Report No.: KCE reports vol 48C].Negrini S, Giovannoni S, Minozzi S, Barneschi G, Bonaiuti D, et al.
Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guidelines.
Europa Medicophysica 2006;42(2):151–70.Accident Compensation Corporation.
New Zealand Acute Low Back Pain Guide
Wellington, New Zealand:
New Zealand Guidelines Group; 2004.Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr., Shekelle P, Owens DK:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline
from the American College of Physicians and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491Chou R, Loeser JD, Owens DK, Rosenquist RW, Atlas SJ, Baisden J, et al.
Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain:
An Evidence-based Clinical Practice Guideline From the American Pain Society
Spine (Phila Pa 1976). 2009 (May 1); 34 (10): 1066–1077van Tulder M, Becker A, Bekkering T, Breen A, del Real MT et al.
European Guidelines for the Management of Acute Nonspecific Low Back Pain in Primary Care
European Spine Jou 2006 (Mar); 15 Suppl 2: S169–191Airaksinen O, Brox J, Cedraschi C, Hildebrandt J, Klaber-Moffett J, et al.
European Guidelines for the Management of Chronic non-specific Low Back Pain
Bergen, Norway: European Commission Research Directorate General; 2005.National Institute for Health and Clinical Excellence (NICE).
Low Back Pain: Early Management of Persistent Nonspecific Low Back Pain
London: National Institute for Health and Care Excellence; 2009.
[Report No.: Clinical guideline 88].Carragee EJ, Hurwitz EL, Weiner BK.
A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned.
Spine Journal 2011;11(6):471–91.Strömqvist B, Fritzell P, Hägg O, Jönsson B.
The Swedish spine register: development, design and utility.
European Spine Journal 2009;18(3S):S294–304.Dunn KM.
Extending conceptual frameworks: life course epidemiology for the study of back pain.
BMC Musculoskeletal Disorders 2010;11(23):1–11.Weiner SS, Nordin M.
Prevention and management of chronic back pain.
Best Practice and Research Clinical Rheumatology 2010;24(2):267–79.Dionne CE, Dunn KM, Croft PR, Nachemson AL, Buchbinder R, Walker BF, et al.
A consensus approach toward the standardization of back pain definitions for use in prevalence studies.
Spine 2008;33(1):95–103.Walker BF.
The prevalence of low back pain: a systematic review of the literature from 1966 to 1998.
Journal of Spinal Disorders 2000;13(3):205–17.Hoy DG, Rickart KT, Durham J, Puntumetakul R, Mansoor GF, et al.
Working together to address disability in a culturally-appropriate and sustainable manner.
Disability and Rehabilitation 2010;32(16):1373–5.Kmietowicz Z.
President of British Pain Society is forced from office after refusing to denounce
NICE guidance on low back pain.
British Medical Journal 2009;339:b3049
Return to OPIOID EPIDEMIC
Return to CHRONIC NECK PAIN
Return to SPINAL PAIN MANAGEMENT
Since 2-10-10

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |