Despite the historic emphasis on treatment, prevention and health promotion
are receiving increased attention within the US health care system.1
These same health promotion tasks are considered by the National Academy of
Science and others as essential components of health services delivered by
primary care providers.2
Chiropractors are viewed by many as capable of and actively delivering
prevention and health promotion in addition to providing other primary care
services. 3–6
Prevention and health promotion activities administered by chiropractors are
in 2 general categories: those considered orthodox by the medical community (eg,
weight loss, exercise, smoking cessation) and those that are not (eg,
soft-tissue and osseous manual procedures and some dietary supplementation).
Previous research demonstrates that the orthodox activities used by primary care
medical providers are also used by chiropractors. 7–9
The nontraditional activities that rely on procedures such as spinal
manipulation have not been investigated. The concept that chiropractic care is
of value in maintaining health and preventing disease began with the work of
Palmer.10
This preventive treatment is traditionally referred to as maintenance care (MC).
MC has been defined as “a regimen designed to provide for the patient's
continued well-being or for maintaining the optimum state of health while
minimizing recurrences of the clinical status.”11
Many chiropractors believe that periodic patient visits permit the doctor to
identify joint dysfunction or subluxations and make corrections with spinal
manipulation or other manual procedures. These treatments are believed to
prevent disease of both neuromusculoskeletal and visceral origin.12
The purpose of this research is to explore the primary care prevention and
health promotion attitudes and practice patterns of chiropractors, in particular
the concept of MC, which has not been investigated in the United States. The
study uses a common instrument for health care research, the postal
questionnaire, and attempts to evaluate the therapeutic components believed
necessary for maintenance patient care, the rationale for its use, what
conditions respond most favorably, how frequently it is required, for which
patients it is recommended, and its economic impact.
Literature search methods
To identify information about chiropractic wellness and health promotion
activities and the concept of MC, comprehensive literature reviews were
conducted. This literature served the usual functions of assisting in creating
the contextual background and search for possible similar work and guided the
development of a survey instrument. Multiple online database searches including
all years available in all languages were conducted through both Medline and
Manual, Alternative, and Natural Index System (formerly Chirolars). Other
databases were excluded because they either did not index chiropractic
literature or the material indexed was redundant. Several search strategies were
developed with the following Medical Subject Headings: chiropractic, health
promotion, prevention, primary health care, and physician's practice patterns.
In addition, manual searches were conducted through the Chiropractic Research
Archives Collection and the Index to Chiropractic Literature as well as a
limited manual search and bibliographic tracking. The search identified only a
few studies related to the chiropractic physician's practice patterns directed
at health promotion and prevention activities. With the exception of the
development of a protocol and pilot study by Rupert et al,13
no other studies identified in the literature addressed the possible health
promotion role of manipulation/adjustment or other manual procedures used by
chiropractors. Although there has been some limited study of MC in Australia and
to an even lesser extent in Europe, there has been no similar study in the
United States. 12,14
Population sampling methods
This descriptive study was conducted with a weighted randomized sample of US
licensed chiropractors. A postal survey instrument was then mailed to the
selected doctors. Sampling was conducted with the database of the National
Directory of Chiropractic.15
The computerized version of the directory contains nearly 40,000 chiropractors
who are in active practice. Unlike the hard copy version that is published
annually, the computerized directory is updated continually. This database was
used to create printouts and mailing labels based on zip code. Zip codes are
created by the US Postal Service, with the first digit representing groups of
states and the second and third subdividing the regions into smaller geographic
areas. The final 2 digits are randomly assigned by the postal service and
represent small post offices in rural areas or postal zones in larger
cities.16
These final 2 numbers are randomly assigned by the postal service in such a
manner that selecting a number would ensure selection from all states, with
representation from rural areas and small and large cities. Selection with the
ending numbers of the zip code would also ensure a “weighting” of the sample
based on size of the state. The larger the state the more zip codes are used
ending in the same number. The ending numbers to be used for selection from the
computerized database were selected by a manual random drawing. This method
helped ensure that chiropractors from each state and from rural areas and large
cities were included in the mailing (but did not ensure their participation in
the study). Such assurances would not have been possible with a pure random
sample.
To obtain a sufficient sample size of US chiropractors for a confidence level
of 0.05, 390 completed and returned surveys were required. This sample size was
calculated in the same manner as described by Hawk and Dusio.7
The return rate of previous surveys of the profession has ranged from 20% to
60%. To ensure adequate response with an estimated response rate of
approximately 30%, 1500 surveys were prepared and mailed.
Questionnaire design
Postal questionnaires are a well-established method for research. The
chiropractic profession has a history of using these instruments for assessing
the health promotion activities of chiropractors. 7,12,13
No previous research questionnaire had been developed for investigating MC. The
instrument used for this study was created by the principal investigator with
the available literature on MC and discussions with practitioners. Revisions
were made after use in a pilot study. Questionnaires from the medical literature
were reviewed; key health promotion strategies, including exercise and smoking
cessation, were included to determine if chiropractors believed these to be
components of MC. To determine what chiropractors believed MC to be and to
prevent biasing that process, no definition of MC was provided with the survey.
Issues of questionnaire content, including length, manner of question design,
and order of questions, were created with established conventions. 17–19
The questionnaire developed for this research had a total of 40 questions. The
first 5 were demographic questions followed by 35 questions related to MC. Of
the 35 MC questions, 28 were developed with a 5-point ordinal Likert scale. With
each question related to MC, the doctor could select 1 of the following
responses: strongly agree, agree, undecided, disagree, or strongly disagree. The
final 7 questions required short fill-in answers. Twenty-three of the questions
related to 5 issues:
- What is the purpose of MC? (6 questions)
- Does the professional research adequately support MC? (2 questions)
- What body systems/conditions respond best to MC? (6 questions)
- What age groups of patients benefit most from MC? (4 questions)
- What therapeutic interventions constitute MC? (5 questions)
The remaining 12 questions related to usage, economic issues, and other
practice patterns.
Once the questionnaire content was established, it was administered to a
convenience sample of 24 chiropractors. As a result of this pilot, minor
modifications were made to some questions and the layout of the form. The
revised questionnaire was kept to a single page with fields that could be
checked in response to the Likert scale questions (Appendix 1). A special
printed message on the outside of the envelope stated “Please contribute five
minutes to professional research.” This notice was added to encourage a response
and also to advise that it was not the typical solicitation that floods
chiropractic offices. In addition to the questionnaire, a postage-paid envelope
was included. To make follow-up possible, a number was assigned to each of the
1500 doctors selected to receive a survey. This number was placed on a master
control list of the doctors and was kept by the principal investigator. The
number corresponding to each doctor was also placed on the top of the
questionnaire. Doctors were advised that their responses would be
confidential.
Data analysis
There were 40 data points for each of the 658 returned surveys. This created
a possible 25,920 data elements that were entered into a spreadsheet created by
the principal investigator with Statistical Product and Service Solutions 7.5
for Windows. The person commissioned to enter these data had a history of
accurate work and proofread questionnaire data after entry. In addition, the
principal investigator performed a random review of data entry to ensure
accuracy. SPSS was then used to create basic descriptive statistics, frequency
distribution, tables, and related analysis.
A total of 1500 surveys were mailed, and of those 701 (46.7%) were returned.
Of these, 43 (2.9%) were returned by the postal service as undeliverable, and
658 (44%) were returned with completed surveys. This provided an adequate rate
to be representative at a confidence level of <.05. At least 1 questionnaire
was returned for each state, and the states densely populated with chiropractors
provided the greatest response (California, 98; New York, 47; Florida, 42;
Texas, 37; Minnesota, 34; New Jersey, 28; Ohio, 27; Missouri, 26; Michigan, 25;
Illinois, 21; Colorado, 20). All other states had fewer than 20 surveys
returned. The demographics of the respondents included age, sex, and years in
practice (Table 1).
Table 1. Demographic characteristics of
surveyed chiropractors
| Sex (%) |
|
Years in
practice (mean 12.33) |
| Male |
83.4 |
1
to 5 |
22.4% |
| Female |
16.6 |
6
to 10 |
34.6% |
| Age (mean
44.0)(y) |
|
11
to 15 |
42.3% |
| 25
to 34 |
29.6% |
16
to 20 |
9.0% |
| 35
to 44 |
46.4% |
>20 |
14.1% |
| 45
to 54 |
13.2% |
New patients per
month |
|
| >55 |
10.8% |
Mean |
19.5 |
Of the respondents, 83.4% were men and 16.6% were women.
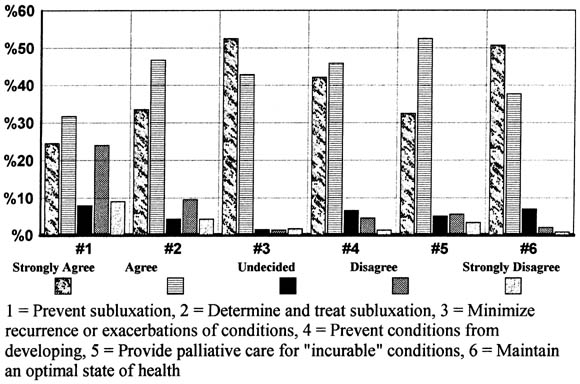
In general, there was a high level of agreement among respondents for most of
the questions. The 6 questions directed at understanding the reason for MC
resulted in agreement or strong agreement that its purpose was to minimize
recurrence or exacerbation (95.4%), maintain or optimize state of health
(88.3%), prevent conditions from developing (88.1%), provide palliative care for
“incurable” problems (84.9%), and determine and treat subluxation (80.2%). Only
56.2% agreed that the purpose of MC was to prevent subluxation. All but 2% of
responding chiropractors believed that MC provided benefit for 1 of 6 purposes
reflected in Fig 1.
|
Fig. 1. Purpose of MC. |
|
|
Click on Image to view full
size |
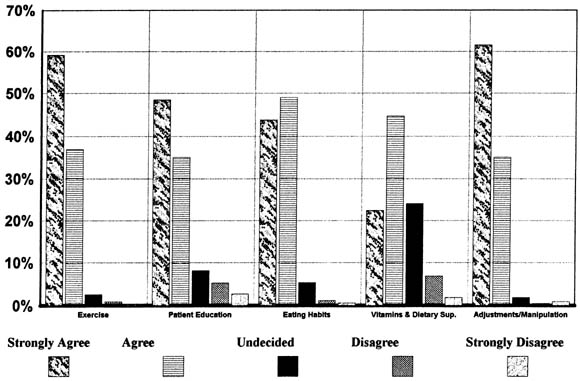
There was also agreement
about what the chiropractors saw as important therapeutic components to MC:
adjustments/manipulation (96.7%), exercise (96.1%), proper eating habits
(92.8%), patient education (eg, smoking, alcohol, drugs) (83.6%), and weaker
agreement on the use of vitamins and supplements (67.1%) (Fig 2).
|
Fig. 2. Therapeutic composition of MC. |
|
|
Click on Image to view full
size |
US chiropractors agreed
that MC was of value to all age groups, with the value increasing slightly with
an increase in a patient's age (Fig 3).
|
Fig. 3. Value of MC for patient subsets by age. |
|
|
|
Click on Image to view full
size |
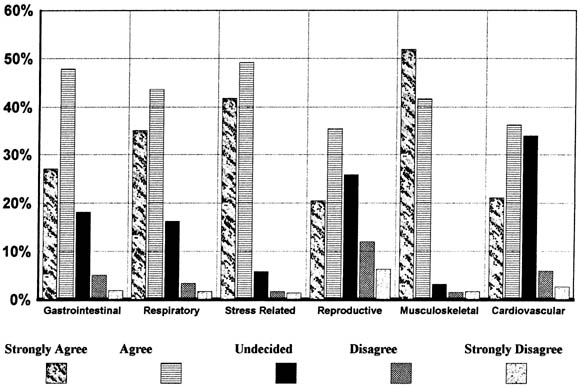
There was less agreement
on the issue of which body systems/conditions could be helped by MC:
musculoskeletal (93.6%), stress (91%), respiratory system (78.8%),
gastrointestinal system (74.9%), cardiovascular system (57.6%), and reproductive
system (56%) (Fig 4).
|
Fig. 4. Patients' response to MC condition/body
system. |
|
|
Click on Image to view full
size |
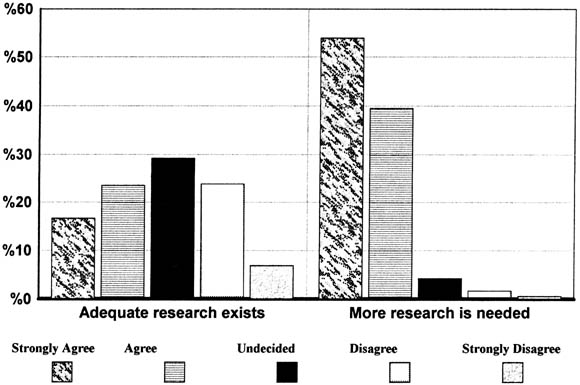
There were 2 questions that addressed research. Only 40.2% agreed that
adequate research existed to support the concept of MC and 93.4% agreed there
was a need for more research (Fig 5).
|
Fig. 5. Research status and MC. |
|
|
Click on Image to view full
size |
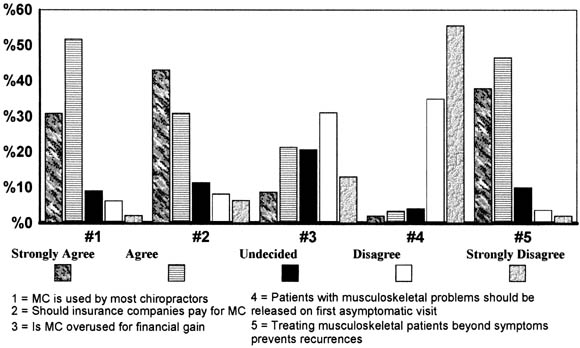
Fig 6 reflects the
responses of chiropractors about several issues: there was agreement that MC was
being performed by most chiropractors (81.9%), that it should be paid for by
insurance (72.3%), and that it helped prevent the return of musculoskeletal
conditions (84.5%).
|
Fig. 6. Miscellaneous questions. |
|
|
Click on Image to view full
size |
Based on the response to this survey, 78.7% of chiropractic patients are
recommended for MC and 34.4% of those elect to receive these services. These
patients average 14.4 visits annually for MC. Chiropractors estimated that 22.9%
of their total practice income was generated from MC services (Table 2).
Table 2. Doctors recommendations and reasons
for MC
|
Mean
(%) |
| Patients encouraged
to receive MC |
78.7 |
| Patients who
actually receive MC |
34.4 |
| MC patients treated
to prevent a return of specific conditions (eg, backache and
headache) |
55.2 |
| MC patients treated
to promote general well-being (not to prevent return of specific
conditions) |
36.0* |
| Average number of
visits required by MC patients each year |
14.4
visits |
| Income from MC
(%) |
22.9 |
* Estimated values do not total
100%. |
There was a significant inverse correlation (P < .05) between the
number of new patients per month and income from MC. The recommendation by
doctors for patients to receive MC was not related to practice income. The
belief of most chiropractors (98%) that MC provided some value in prevention or
health promotion was not correlated to practice income from MC services.
Postal surveys have inherent weaknesses but are a well-established form of
biomedical research. One of the specific weaknesses in this study involves
requesting chiropractors to provide the number of new patients per month, the
percentage of income derived from MC, and other data that are not based on
accurate counts and calculations but on estimates. In addition, the response
rate (44%), although disappointing, was relatively strong for a chiropractic
postal survey. Surveys within the profession rarely result in as much as a 50%
response rate; previous survey response rates related to chiropractic and
prevention have ranged from 22% to 65%. 7,12
A control number was assigned to each questionnaire to facilitate follow-up of
nonrespondents. However, this did not prove effective because many doctors who
did respond either obliterated, marked out, or actually tore off the number from
the form to ensure anonymity. With the accuracy of written follow-up
compromised, a selected follow-up was made by telephone. Eighty-five doctors for
whom there was no record of a completed questionnaire were called and asked (1)
if they completed the survey, (2) if they did not respond, why, and (3) if they
used MC in their practice. Doctors indicated that the most common reason for
nonparticipation was that they were too busy. The majority of nonrespondents
also reported that they used some form of MC in their practices.
A review of the demographics of chiropractors who completed and returned
questionnaires for this study did not vary significantly from other large
contemporary surveys, with the exception of sex. The annual survey conducted in
1995 by the American Chiropractic Association reflected a sex mix within the
profession of 88% men and 12% women.20
The response to this MC study and previous prevention-related research conducted
by Hawk and Dusio 7 both had a slightly higher percentage of female respondents
than the national American Chiropractic Association survey (83% male and 17%
female; 81% male and 19% female, respectively). Hawk and Dusio 7 indicated that
the larger number of female respondents may reflect a bias.7
However, a recent medical study suggests that female physicians may have a
greater interest in prevention activities than male physicians.21
This same phenomenon may in fact be operative within chiropractic and may
account for the greater participation of women in this prevention-related
survey. The average age of respondents in this study was 41 years compared with
an average age of 44 years in the 1995 American Chiropractic Association
survey.20
Prevalence of use
Previous work outside the United States suggests that the use of MC accounts
for a significant amount of services rendered by chiropractors. In England,
Breen22
noted that after management for conditions like low-back pain, “39% of patients
made further visits for maintenance treatment.” The Jamison12
study of Australian chiropractors found that 62% performed MC on up to one third
of their patients; 32% performed MC on 34% to 66% of their patients; and 6%
performed MC on 67% to 100% of their patients.23
This study attempted to address the same issues for chiropractors in the United
States. Chiropractors were asked to provide the percentage of their patient load
that received MC; the mean response was 34.4%. This suggests that a large
percentage of chiropractic care given around the world is directed at prevention
and health promotion. Shekelle24
reported that 42.1% of patient visits to chiropractors were for low-back
symptoms followed by 10.3% for neck/face symptoms. However, if as this study
suggests, 34.4% of patient visits are for the purpose of MC, then preventive
services may be the second most common reason for visits to a chiropractor. In
addition to this high percentage of patients receiving MC, a much higher number,
78.7% of US patients, receive the recommendation to continue with preventive MC.
This strong recommendation to receive preventive services suggests attitudes
that are similar to Australian chiropractors: 41% asserted that everybody would
benefit from such care, 38% believed that most would benefit, and 14% believed
that some patients would benefit.12
Despite the emphasis by the US Government on initiatives such as Healthy
People 2000,1
the medical community continues to face many obstacles to providing preventive
and health promotion services. 25–28
With the use of MC to the extent described in this study, the chiropractic
physician appears to place more emphasis on, derive more income from, and
perhaps commit more patient time to prevention and health promotion purposes
than many other health care professionals.
Another Australian study by Webb and Leboeuf14
found that there was a higher level of MC performed by doctors who had a lower
number of new patients per month. The current research confirmed similar
practice patterns (although number of MC visits was not ascertained) with a
statistically significant inverse relation and correlation (P < .05)
between the number of new patients per month and the practice income generated
from MC.
Economics of MC
In conjunction with the high percentage of patients who have been recommended
for MC and the nearly half that comply, there also is a relatively high
financial impact with an average 22.9% of all chiropractic income in the United
States generated from these services. Based on an annual gross income of
$225,783,20
MC accounts for an average annual income of $51,930 per practice. When the 22.9%
is viewed in the context of the total revenues of all chiropractors,29
this would equate to $48 million in MC services delivered to US citizens during
1994.
It was not possible to be more specific about how patients paid for MC
because of the necessity for reasonable brevity of professional surveys. Because
most health insurance policies will not reimburse policyholders for health
promotion services, future research should explore the methods of payment for
MC.
A few authors have stated or implied that there are serious ethical issues
with maintenance programs and that there is an inappropriate financial motive
for what is termed “spurious” services. 22,30
Homola30
states that “It is unfair to patients to allow them to believe that they must
have regular spinal adjustments in order to stay healthy.” Two findings from
this survey suggest appropriate financial motive to MC services. First, the
majority of the respondents (98%) agree that MC is of value for prevention and
promoting the health of their patients. Twelve respondents, representing only
1.9% of the responding population, indicated that they never recommended MC.
This consensus about the value of MC is remarkable considering the historical
disagreement within the profession about so many other issues. In addition to
the 98.1% of chiropractors recommending MC to their patients, 98% also agreed
with at least 1 of the 6 questions describing the possible health benefits of
MC. Chiropractors believe in the value of MC (98%) and therefore 98% recommend
its use to their patients. Recommending the use of a procedure without belief in
its value would suggest possible financial or other inappropriate motives, but
this is not the case with MC. Secondly, 70.5% of chiropractors responded that
they did not agree that MC was used for financial gain. Only 8.9% strongly
agreed that MC was overused. The belief that MC was overused was significantly
negatively correlated (P < .01), with both recommending MC to patients
and the belief in the value of MC. Thus doctors who did not believe there was
therapeutic value to MC (and did not or rarely recommended its use) were the
ones who believed MC might be overused for financial gain.
This survey did find a significant inverse relation (P < .05)
between the number of new patients per month and practice income from MC.
However, the recommendation to receive MC was not related to practice income.
There was also no correlation between income from MC and the doctors' belief
that MC was of value in promoting health. These facts suggest that despite the
number of new patients per month, chiropractors believe in the value of MC
regardless of whether or not they are actually deriving income from MC services
in their practices. It is possible that those chiropractors with lower patient
loads are simply able to dedicate more time, and thus a higher percentage of
their income is generated from MC services. Chiropractors, like all health care
providers, must meet financial obligations and must charge for their services.
It is reasonable to expect that they would focus on services for which they can
expect reimbursement. MC, which is not covered in the United States by most
health insurance, Medicare, or worker's compensation programs, is not one of
those services. Therefore chiropractors with high volumes of patients with
low-back pain and other reimbursable conditions might be less likely to spend as
much time on services for which reimbursement is difficult, such as MC.
Composition of MC
Previously, no data existed that described the therapeutic constituents of
MC. Recently, there has been speculation by authors that chiropractors “keep
people well through spinal adjustments”31
and that diet, exercise, lifestyle changes, and other prevention-directed
activities are not part of the profession's prevention efforts. This view
appears inaccurate because this study depicts the preventive MC activities of
chiropractors as a combination of interventions that rely heavily on exercise,
nutrition, and lifestyle changes. Although most doctors (96.7%) responding did
agree that spinal manipulation was an essential component of preventive MC
services, the respondents also agreed that exercise was an equally important
component (96.1%), followed closely by proper eating (92.8%), patient education
(83.6%), and vitamin and supplement usage (67.1%).
Value of maintenance care
To ensure a response from field doctors, the questionnaire was only 1 page.
Because of the short length of the questionnaire, there were only 4 age groups
of patients listed: children, adolescents, adults, and the aged. The survey
described a consensus about the value of MC for all 4 patient groups. This was a
consistent response, considering the high percentage of patients recommended to
receive MC. In addition, there is a prevalent belief that preventive MC services
are helpful in a variety of visceral conditions and musculoskeletal problems.
Because of the eclectic nature of the therapies used in MC and because it is
standard medical practice to make exercise, nutritional, and other
recommendations for many visceral problems, it is not surprising that
chiropractors would also address these conditions. It was beyond the scope of
this initial study to ascertain to what extent chiropractors believe specific
visceral and musculoskeletal conditions benefit specific therapeutic components
of MC. Five different purposes for MC were given with this survey. Relatively
strong agreement was found for all but 1 (ie, the prevention of subluxation).
Slightly more than half of chiropractors believed MC was valuable for this
purpose. This response raises questions about the belief system of chiropractors
because it relates to prevention and the subluxation concept. If MC cannot
prevent subluxation, how is it prevented? Future studies should be directed at
exploring wellness and prevention in the context of subluxation.
Research
The 658 doctors who responded to the survey were relatively unaware of the
scarce research that supports the use of MC. Forty percent believed that
“chiropractic research adequately supports the value of MC” and <7% strongly
disagreed with that statement. This misconception exists despite the fact that
the deficiency in supporting research has been brought to the profession's
attention on many occasions by both the medical community and those involved in
chiropractic research. 32–35
The survey did establish that the overwhelming majority (93.4%) of the
profession agreed that there was a need for further research. The research issue
questions the education of chiropractors as it relates to MC. Future research
should be directed at why there is such a strong belief in the value of the
spinal manipulation component of MC among both new and established
chiropractors. In what manner is this subject addressed in chiropractic colleges
and to what extent does practice experience have an impact on the belief in MC?
One reason why chiropractors may believe that adequate research exists is simply
because, as this survey suggests, MC includes a wide variety of well-researched
health promotion components, including exercise, food supplementation, and
diet.
The chiropractic profession has had a historic interest in and emphasis on
health promotion and prevention, often referred to as MC. The literature to date
consists primarily of individual opinions that, based on this work, have often
misrepresented the motivation, therapeutic components, extent of use, and other
elements of MC. The respondents to this survey, like their European and
Australian counterparts, strongly believe in the preventive and health-promoting
merits of periodic visits for MC. MC is believed to benefit patients of all ages
for a wide variety of visceral and musculoskeletal conditions. Belief in the
efficacy of MC translates into a high rate of recommendation to patients and a
substantial economic impact on chiropractic practice. Although chiropractors
with low new patient traffic tended to recommend MC services more often, both
chiropractors with low and high new patient traffic believed that MC was
valuable for promoting patient health. The recommendation that patients receive
MC was also not related to practice income from MC. Therefore the belief in the
value of MC appears to be motivated by its potential value to the patient and
not for financial gain as some have suggested. Chiropractors concur that MC is
not simply administering periodic manipulative treatments but rather that
exercise, nutritional, and lifestyle recommendations are equal or nearly equal
in importance.

)
)
)
)
)
)
