

Chiropractic Care for Patients with Asthma:
A Systematic Review of the LiteratureThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc. 2010 (Mar); 54 (1): 24–32 ~ FULL TEXT
OPEN ACCESS Adrienne Kaminskyj, BKin, DC, Michelle Frazier, BA, DC,
Kyle Johnstone, BGS, DC, Brian J. Gleberzon, BA, DC*
Professor and Chair,
Department of Applied Chiropractic,
Canadian Memorial Chiropractic College,
6100 Leslie St,
Toronto, ON M2H 3J1
bgleberzon@cmcc.caOBJECTIVE: To provide a review of the literature and rate the quality of published studies regarding chiropractic care, including spinal manipulation, for asthmatic patients.
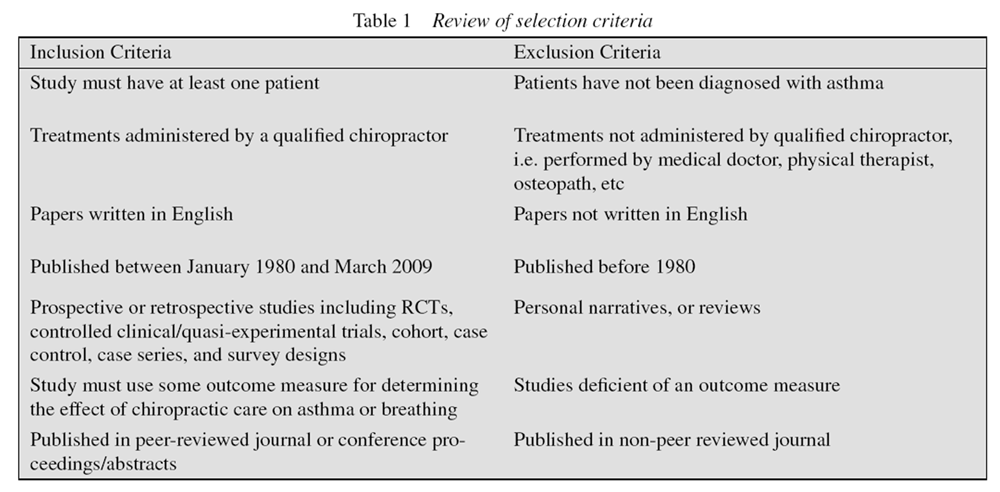
METHODS: A multimodal search strategy was conducted, including multiple database searches, along with reference and journal hand-searching. Studies were limited to those published in English and in peer-reviewed journals or conference proceedings between January 1980 and March 2009. All study designs were considered except personal narratives or reviews. Retrieved articles that met the inclusion criteria were rated for quality by using the Downs and Black checklist. A brief summary was also written for each retrieved study.
RESULTS: Eight articles met the inclusion criteria of this review in the form of one case series, one case study, one survey, two randomized controlled trials (RCTs), one randomized patient and observer blinded cross-over trial, one single blind cross study design, and one self-reported impairment questionnaire. Their quality scores ranged from 5 to 22 out of 27.
CONCLUSION: Results of the eight retrieved studies indicated that chiropractic care showed improvements in subjective measures and, to a lesser degree objective measures, none of which were statistically significant. It is evident that some asthmatic patients may benefit from this treatment approach; however, at this time, the evidence suggests chiropractic care should be used as an adjunct, not a replacement, to traditional medical therapy.
From the FULL TEXT Article
Introduction
Chiropractic is among the three most commonly utilized complementary and alternative medicine (CAM) therapies. [1] As a result, practitioners in this realm of health care are certain to encounter a vast array of clinical conditions ranging from common to obscure. According to the World Health Organization, asthma is now a serious public health problem with over 100 million sufferers worldwide. [2] It can be expected that chiropractors, along with other CAM practitioners, will be treating asthmatic patients. Sources of management and treatment guidelines mention pharmaceutical interventions and trigger avoidance as key items; however, many of these sources fail to mention CAM therapies.
Many chiropractors have experienced success in the treatment of non-musculoskeletal conditions, dating back to the very first adjustment. In this day and age, the scope of chiropractic care ranges from traditional spinal manipulation, to nutritional advice, to exercise prescription. The clinical question, however, is whether CAM interventions can benefit the asthmatic, and whether chiropractors should be the primary health care providers or provide co-management. Moreover, it must be determined if the chiropractic care provided to asthmatic conditions is directed at improving asthma-related symptoms (i.e. breathing) or if it is targeted towards the spinal symptoms (i.e. pain, stiffness, lose of motion) secondary to the asthma.
Towards that end, a number of studies have been aimed towards analyzing the effects of spinal manipulative therapy (SMT) in relation to forced expiratory volume (FEV), quality of life, self reported asthma severity, medication dependency and other measures, without consideration of the complete chiropractic encounter. The purpose of this systematic review of the literature was to rate the quality of the existing evidence for the chiropractic care of patients with asthma.
Methods
This study was approved by the Ethics Review Board of the Canadian Memorial Chiropractic College. MEDLINE, CINAHL, AMED, Alt Healthwatch, Index to Chiropractic Literature, MANTIS and the Cochrane Database of Systematic Reviews were searched for relevant literature between January 1980 and March 2009. The MeSH terms used were: Asthma, Chiropractic, Manipulation, Chiropractic, Manipulation, Spinal, Musculoskeletal Manipulations. Text words for the same concepts were also searched. The search terms were combined to limit the amount of articles obtained as each individual term used yielded greater than 1000 results and the findings were not specific to the chiropractic profession. Hand-searching of conference abstracts and proceedings that were deemed acceptable for inclusion were obtained where appropriate. The reference lists of all retrieved articles and conference proceedings from the database searches were hand-searched for further relevant articles not included in the electronic literature search. The table of contents of relevant journals including the Journal of the Canadian Chiropractic Association and the Journal of Manipulative and Physiological Therapeutics were hand-searched for additional relevant articles.
The authors scrutinized the electronic search results, the titles and abstracts in particular, and the full articles of the citations were obtained if they included outcomes of chiropractic care for patients with asthma. All study designs were considered except personal narratives or review articles.

Table 1 The inclusion and exclusion criteria used for this review are described in Table 1. These criteria were applied to all of the obtained full articles and conference proceedings. The reference lists of all retrieved articles, conference abstracts, and proceedings from the database searches were hand-searched for further relevant articles not included in the electronic literature search.
The three principal authors reviewed the studies meeting the inclusion criteria and conducted a critical appraisal of the full-text articles. The data from all included articles and conference abstracts/proceedings were recorded onto a data extraction sheet by the authors as part of the review. The authors checked and edited all entries for accuracy and consistency. Recorded data included study authors and quality score, details of the study design, sample, interventions, outcome measures, and main results/conclusions of the study.
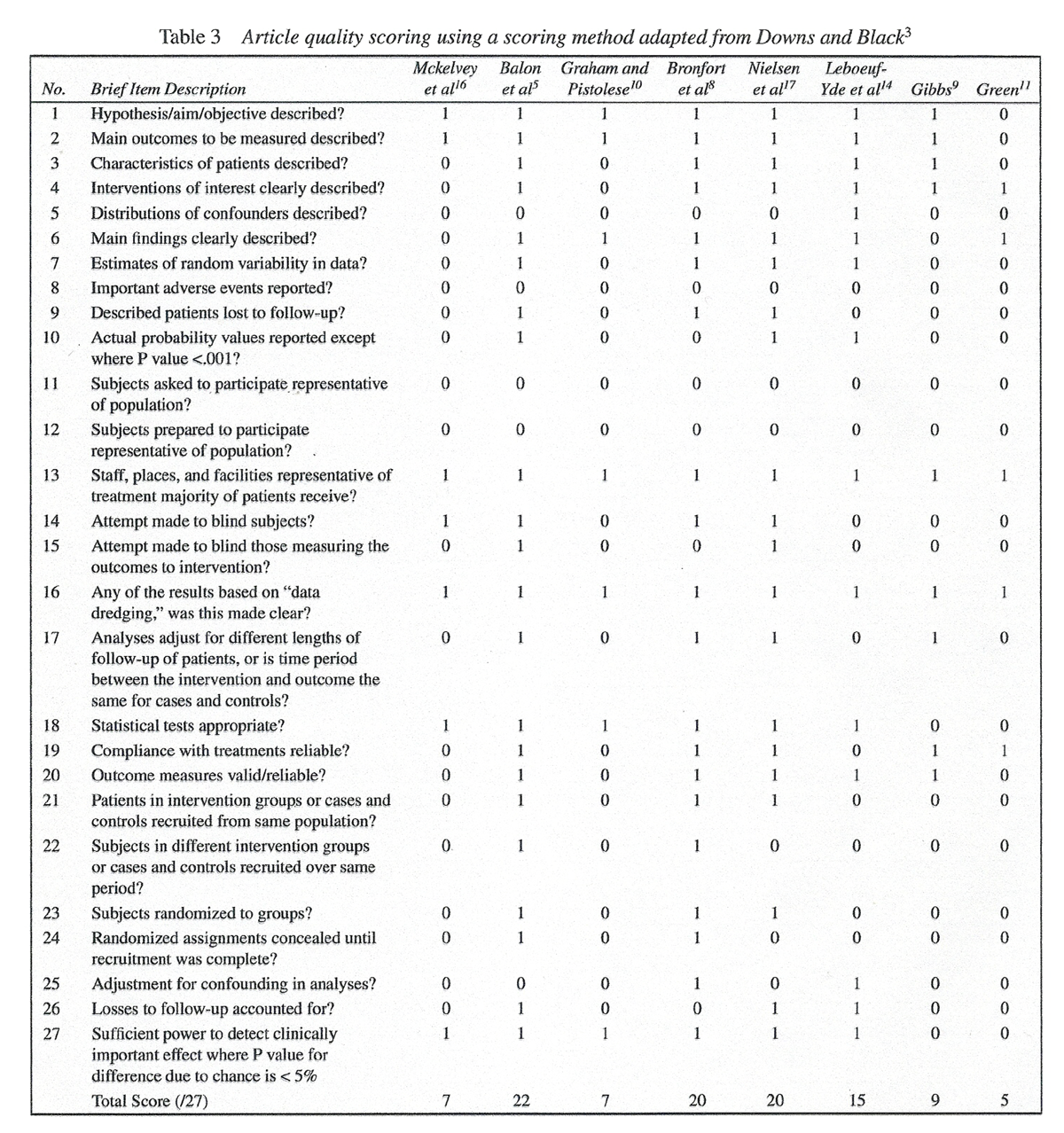
The methodological quality of the studies that met the selection criteria was assessed by the authors using the 27-item scoring checklist developed by Downs and Black. [3] The scoring checklist is considered valid and reliable for assessing randomized and nonrandomized studies. [3] It was determined, partially through retrieving articles, that there likely would not be many randomized controlled trials, and as such, a methodological scoring system allowing nonrandomized studies to be evaluated was considered necessary. Items 5 and 27 were revised from the original Downs and Black checklist to be worth 1 point each so that the modified total score was 27. The authors individually reviewed each included article for quality (based on the Downs and Black checklist) using a quality scoring sheet. Quality scores above 20 were considered good; 11–20, moderate; and below 11, poor. [7] The three authors independently rated all the studies, recorded final scores for each article, and resolved any differences by discussion.
Results
The initial electronic searches identified 152 citations (including overlapping citations between databases), three from AMED, two from Alt HealthWatch, 12 from MEDLINE, 34 from CINAHL, 45 from the Index to Chiropractic Literature, 56 from MANTIS and one from the Cochrane Database of Systematic Reviews. This systematic review evaluated the evidence for the effects of manual therapies for treatment of patients with bronchial asthma. While chiropractic manipulation was mentioned as a method of manual therapy in the Cochrane review, it was not included as it did not meet the inclusion criteria. However, the Cochrane review was utilized by hand searching the reference list for additional articles but none were found. One additional article was identified by hand searching the reference list from the review article written by Hawk et al. [4] Hand searching the table of contents of several chiropractic journals did not yield any additional articles. The full texts of 13 articles [4–17] were obtained after screening the titles and/or abstracts to determine if they would meet the inclusion criteria. Eleven articles came from electronic database searches, one came from hand searching conference proceedings, and one came from reference list evaluations.
Eight articles met all of the inclusion/exclusion criteria for this review. Seven [5, 8, 9–11, 14, 17] were identified by the electronic database searches and one was identified by hand searching conference proceedings. [16] The remaining five articles [6, 7, 12, 13, 15] were excluded for a variety of reasons. All 13 articles were written in English.
Table 2 The eight selected articles included: one case series, one case study, one survey, two randomized controlled trials (RCTs), one randomized patient and observer blinded cross-over trial, one single blind cross study design, and one self-reported impairment questionnaire. Table 2 provides information on each of the eight included studies with respect to study design, sample, interventions, outcome measures, results, and conclusion. As well, the quality scores for each article have been included.
Description of Studies
McKelvey SE, Hayek R, Ali S.
Asthma and chiropractic. A multi-centre approach.
Proceedings 5th Biennial Congress, Auckland, NZ.
World Federation of Chiropractic, May 17–22 1999: 166–7.
Score on Down’s and Black Checklist: 7
McKelvey et al, [17] conducted a 6-week single blind cross study, reported as an abstract only, on 32 patients diagnosed with asthma and under medical management. Peak flow, spirometry, and salivary samples were recorded from each subject. Subjects were treated with an adjustive manoeuvre that was accompanied by an audible joint cavitation or an examination with little or no intervention. There was no statistically significant difference in group spirometry readings before and after treatment. Clinically important subjective improvements include reduced number of asthma attacks and reduced medication use reported by all subjects in the trial.
Balon J, et al.
A Comparison of Active and Simulated Chiropractic Manipulation
as Adjunctive Treatment for Childhood Asthma
New England Journal of Medicine 1998; 339(15): 1013-1020
Score on Down’s and Black Checklist: 22
Balon et al [5] conducted a randomized controlled trial on 91 children aged 7–16 who had continuing symptoms of asthma despite medical treatment. Subjects were randomly assigned to receive either active or simulated chiropractic manipulation for four months. Peak expiratory flow was measured from a change in base line. Of the 91 children, 80 had outcome data that could be evaluated. Small increases in both treatment groups were noted, with no statistically significant difference between groups with reference to a change in baseline measurements. Asthma symptoms and use of β-agonists decreased and quality of life increased in both groups with no statistically significant difference between groups. The authors concluded that children with mild to moderate asthma would not benefit from the inclusion of chiropractic spinal manipulation to usual medical care.
Graham RL, Pistolese RA.
An Impairment Rating Analysis Of Asthmatic Children Under Chiropractic Care
Journal of Vertebral Subluxation Research 1997 (Jul); 1 (4): 1–8
Score on Down’s and Black Checklist: 7
Graham and Pistolese [10] conducted a self-reported impairment study on 81 children aged 1–17 before and after a two month period of chiropractic care. Significant reduction (improvement on the modified Oswestry rating scale) was reported for 90.1% of subjects after 60 days of chiropractic treatment. Girls reported less improvement after care compared to boys, however significant decreases in impairment ratings were reported for both sexes.
Bronfort G, Evans RL, Kubic P, Filkin P.
Chronic Pediatric Asthma and Chiropractic Spinal Manipulation:
A Prospective Clinical Series and Randomized Clinical Pilot Study
J Manipulative Physiol Ther 2001 (July); 24 (6): 369–377
Score on Down’s and Black Checklist: 20
Bronfort et al [8] conducted a prospective clinical case series and observer blinded randomized controlled trial on 36 patients aged 6–17 with mild and moderate persistent asthma. Patients were randomly assigned to receive either active spinal manipulation or sham spinal manipulation. At the conclusion of the 12-week intervention, lung function tests and patient-rated day and night-time symptoms showed little or no change. A 20% reduction in β-bronchodilator use was seen, quality of life scores increased by 10% to 28%, and asthma severity rating showed a 39% reduction. The changes in patient-rated severity remained unchanged at 12-month post treatment follow-up.
Nielsen NH, Bronfort G, Bendix T, Madsen F, Weeke B.
Chronic Asthma and Chiropractic Spinal Manipulation:
A Randomized Clinical Trial
J Clinical and Experimental Allergy 1995 (Jan); 25 (1): 80–88
Score on Down’s and Black Checklist: 20
Nielson et al [17] conducted a randomized patient and observer blinded cross-over trial on 31 patients aged 18–44 suffering from chronic asthma. Patients were randomized to receive either active chiropractic spinal manipulative treatment or sham spinal manipulative treatment two times per week for four weeks. No clinically important or statistically significant differences were found between active and sham manipulations on forced expiratory volume, use of inhaled bronchodilators, patient-rated asthma severity, and non-specific bronchial reactivity. Non specific bronchial hyperreactivity improved by 36% and patient-rated asthma severity decreased by 34%.
Leboeuf-Yde C, Pedersen EN, Bryner P, Cosman D, Hayek R, Meeker WC, et al.
Self-reported Nonmusculoskeletal Responses to Chiropractic Intervention:
A Multination Survey
J Manipulative Physiol Ther 2005 (Jun); 28 (5): 294–302
Score on Down’s and Black Checklist: 15
Leboeuf-Yde et al [14] conducted a multination survey from 385 chiropractors on 5,607 patients receiving spinal manipulation with or without additional therapy. Positive reactions in non-musculoskeletal symptoms were reported by 2–10% of patients. Of these patients, 27% noted positive reactions in non-musculoskeletal symptoms and also noted improved breathing. Variables identified that may influence the outcome included: patients informed that the reactions may occur (odds ratio [OR] 1.5); treatment directed to the upper cervical spine (OR 1.4); treatment directed to the lower thoracic spine (OR 1.3) and; female sex (OR 1.3).
Gibbs AL.
Chiropractic Co-management of Medically Treated Asthma
Clinical Chiropractic 2005 (Sep); 8 (3): 140–144
Score on Down’s and Black Checklist: 9
Gibbs [9] conducted a case series on three patients with asthma treated with chiropractic manipulation to the upper thoracic spine two times per week for six weeks. All three cases resulted in increased objective changes in peak flow using a spirometer. As well, increased subjective data was noted in all patients from a recorded asthma diary.
Green A.
Chronic asthma and chiropractic spinal manipulation: a case study.
Br J Chiropractic. 2000; 4 (2): 32–35.
Score on Down’s and Black Checklist: 5
Green [11] conducted a case study on one patient aged 43 years old with asthma diagnosed at 38 years of age. The subject was treated with spinal manipulation to the lower cervical spine, upper thoracic spine, and costovertebral joints. Trigger-point therapy and post-isometric relaxation techniques were used to the hypertonic musculature. Initial spirometry measurements demonstrated a peak expiratory flow of 430 L/min. Over a 12-month treatment period, there was an increase in the peak flow from 430 to 550 L/min. As well, the subject noted a decrease in medication use.None of the studies indicated any adverse effects or evidence of harm (other than exacerbations of asthma) to patients treated by chiropractors. Studies by Balon [5] and Nielsen [17] were the only ones to mention adverse effects/reactions as part of the article and to formally state that there were no adverse events. All other articles included in this study did not mention adverse effects. None of the included articles included a comprehensive list of possible adverse effects from the intervention.
Quality of Articles
Table 3 Table 3 depicts the quality scoring of each of the included articles. The overall level of disagreement of the evaluators, after independent rating, was 3.2% (7/216). These differences were rectified through discussion. The methodological quality of the articles was poor to good. The highest score on the Downs and Black [3] scoring system was 22/27, achieved by the Balon et al [5] study. The studies by Bronfort et al, [8] Nielsen et al, [17] and Leboeuf-Yde et al1 [4] achieved moderate quality ratings of 20, 20, and 15 respectively. The other four studies [9–11, 16] all rated poorly (<11) in methodological quality.
The included studies yielded good to low quality ratings on the Down and Black3 scoring checklist. The poor and moderate ratings were primarily due to problems with external validity (questions 11 and 12, Table 3), which addresses the representativeness of the findings of the study and determines whether they can be generalized to the population from which the study subjects were derived. Poor and moderate ratings were also due to a lack of randomization to groups, blinding of subjects or those measuring the outcomes.
Discussion
In treating asthmatic patients, the objective of chiropractic spinal manipulative therapy (high amplitude, low velocity thrusts) is to increase the motion of the thoracic cage, mobilize the ribs, enhance arterial supply and lymphatic return, and to affect nervous system activity, all in hope of reducing symptomatology of the patient.
To the knowledge of the authors, this is the first systematic review of the literature specifically examining chiropractic care for the treatment of asthma. For the purposes of this review, chiropractic care encompassed spinal manipulative therapy, mobilizations, soft tissue therapy and/ or breathing exercises. Although the studies evaluated for this review showed some patient improvement with chiropractic care, the quality of this evidence was, at times, questionable and for this reason it is insufficient in determining direct therapeutic benefit. Assessing the effectiveness of chiropractic treatment of patients with asthma is multifactorial and an array of outcome measures exist, both subjective and objective.
Subjective measures varied amongst the selected literature, including reported number of asthma attacks, medication use, quality of life, patient-reported changes in asthma symptomatology, modified Oswestry rating scale, and asthma diary logs. A noticeable trend of improvement in these measures was recognized across the reviewed literature, although none were statistically significant.
Spirometry readings were the main objective measures used in the selected literature. These included peak expiratory flow, vital capacity and forced expiratory volume. Some improvements in these objective measures were noted, however, as with the subjective measures, none were statistically significant.
The main limitation amongst the selected literature was the lack of detail regarding the location and type of manipulative technique used. This lack of information hinders the reproducibility of the study design. With this being stated, chiropractors are trained to locate and manipulate restricted vertebral segments in the attempt to induce motion. Whether or not certain types of chiropractic manipulations are more beneficial than others is a pertinent question that should be explored in further investigations.
It is encouraging to note that, in the two articles that commented on it, no patients were reported to experience any worsening of symptoms or injuries while under care. Although it is tempting to attribute this to the care provided, it is equally possible that, since these children were being medicated during the time they received chiropractic care, any worsening of their condition would have been masked by their drugs. Additionally, although it is encouraging that many of the children in the studies referred to in these articles were able to experience a decrease in their medication use, it is possible that these same children were being over-medicated initially.
No statistical significances were obtained with chiropractic care during the treatment of children with asthma. However, positive clinical changes were seen in a number of subjects leading to the conclusion that spinal manipulative therapy may be sought as an adjunct to medical management. In stating this, it is important to note that there is a chance that this treatment modality may be of little to no benefi t for certain patients and therefore the authors recommend a trial of care to identify whether or not chiropractic care should be included in the overall management of their condition.
Conclusion
Despite a paucity of evidence supporting the successful management of patients with asthma under chiropractic care, and despite the fact that the evidence that does exist is heterogeneous with respect to its quality strength, there is nonetheless some indication that patients experience positive subjective and at times positive objective results while under chiropractic care. The approaches described in many of the manuscripts reviewed refl ect common clinical practice activities used by chiropractors, including an array of different outcome measures. That said, more evidence is required before any defi nitive statements can be made with respect to the clinical effectiveness of chiropractic care for patients with asthma and with respect to the most appropriate role chiropractors should play in the management of these patients. Such studies may benefi t from the use of a valid and reliable outcome measure such as the Pediatric Asthma Health Outcome Measure (PAHOM). [18]
References:
Ni H, Simile C, Hardy AM.
Utilization of complementary and alternative medicine by United States adults:
Results from the 1999 National Health Interview Survey.
Med Care. 2002;40:353–358National Institutes of Health Global Initiative for Asthma,
HNLBI/WHO Report. Jan, 1995.Downs S, Black N.
The feasibility of creating a checklist for the assessment of the methodological quality both of randomized and
non-randomized studies of health care interventions.
J Epidemiol Community Health. 1998;52:377–384Hawk C, Knorsa R, Lisi A, Ferrance RJ, Evans MW.
Chiropractic Care for Nonmusculoskeletal Conditions: A Systematic Review
With Implications For Whole Systems Research
J Altern Complement Med. 2007 (Jun); 13 (5): 491–512Balon J, Aker PD, Crowther ER, Danielson C, Cox GP, O’Shaugnessy D, Walker C, Goldsmith CH, et al.
A comparison of active and simulated chiropractic manipulation as adjunctive treatment for childhood asthma.
N Engl J Med. 1998;339:1013–1020Balon JW, Mior SA.
Chiropractic care in asthma and allergy.
Ann Allergy Asthma Immunol. 2004;93:S55–60Brockenhauer SE, Julliard KN, Sing K, Huang E, Sheth A.
Quantifiable effects of osteopathic manipulative techniques on patients with chronic asthma.
J Am Osteopath Assoc. 2002;102:371–375Bronfort G, Evans RL, Kubic P, Filkin P.
Chronic pediatric asthma and chiropractic spinal manipulation:
A prospective clinical series and randomized clinical pilot study.
J Manipulative Physiol Ther. 2001;21:369–377Gibbs AL.
Chiropractic Co-management of Medically Treated Asthma
Clinical Chiropractic 2005 (Sep); 8 (3): 140–144Graham RL, Pistolese RA.
An Impairment Rating Analysis Of Asthmatic Children Under Chiropractic Care
Journal of Vertebral Subluxation Research 1997 (Jul); 1 (4): 1–8Green A.
Chronic asthma and chiropractic spinal manipulation: a case study.
Br J Chiropr. 2000;4:32–35Hartling L, Brison RJ, Crumley ET, Klassen TP, Pickett W.
A systematic review of interventions to prevent childhood farm injuries.
Pediatrics. 2004;114:483–496Hondras MA, Linde K, Jones AP.
Manual therapy for asthma.
Cochrane Database Syst Rev. 2005;(2)Leboeuf-Yde, C., Pedersen, E.N., Bryner, P., Cosman, D., Hayek, R.
Self-reported Nonmusculoskeletal Responses to Chiropractic Intervention:
A Multination Survey
J Manipulative Physiol Ther 2005 (Jun); 28 (5): 294–302Markham AW, Wilkinson JM.
Complementary and alternative medicines (CAM) in the management of asthma:
An examination of the evidence.
J Asthma. 2004;41:131–139McKelvey SE, Hayek R, Ali S,
Asthma and chiropractic . World Federation of Chiropractic 5th Biennial Congress Symposium Proceedings.
Auckland, New Zealand: World Federation of Chiropractic; 1999. 1999.
A multi-centre approach; pp. 167–168Nielsen NH, Bronfort G, Bendix T, Madsen F, Weeke B.
Chronic asthma and chiropractic spinal manipulation a randomized clinical trial.
Clin Exp Allergy. 1995;25:80–88Chiou CF, Weaver M, Bell M, Lee T, Krieger J.
Development of the multi-attribute Pediatric Asthma Health Outcome Measure (PAHOM)
Int J Qual Health Care. 2005;17:23–30
Return to ASTHMA
Since 4-02-2010
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |