

Extrapolating Beyond the Data in a Systematic Review of
Spinal Manipulation for Nonmusculoskeletal Disorders:
A Fall From the SummitThis section was compiled by Frank M. Painter, D.C.
Make comments or suggestions to Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2021 (May); 44 (4): 271–279 ~ FULL TEXT
Christine M. Goertz, DC, PhD, Eric L. Hurwitz, DC, PhD, Bernadette A. Murphy, DC, PhD, Ian D. Coulter, PhD
Duke Clinical Research Institute,
Duke University,
200 Morris Street,
Durham, NC 27701Objective The purpose of this article is to discuss a literature review — a recent systematic review of nonmusculoskeletal disorders — that demonstrates the potential for faulty conclusions and misguided policy implications, and to offer an alternate interpretation of the data using present models and criteria.
Methods We participated in a chiropractic meeting (Global Summit) that aimed to perform a systematic review of the literature on the efficacy and effectiveness of mobilization or spinal manipulative therapy (SMT) for the primary, secondary, and tertiary prevention and treatment of nonmusculoskeletal disorders. After considering an early draft of the resulting manuscript, we identified points of concern and therefore declined authorship. The present article was developed to describe those concerns about the review and its conclusions.
Results Three main concerns were identified: the inherent limitations of a systematic review of 6 articles on the topic of SMT for nonmusculoskeletal disorders, the lack of biological plausibility of collapsing 5 different disorders into a single category, and considerations for best practices when using evidence in policy-making. We propose that the following conclusion is more consistent with a review of the 6 articles. The small cadre of high- or moderate-quality randomized controlled trials reviewed in this study found either no or equivocal effects from SMT as a stand-alone treatment for infantile colic, childhood asthma, hypertension, primary dysmenorrhea, or migraine, and found no or low-quality evidence available to support other nonmusculoskeletal conditions. Therefore, further research is needed to determine if SMT may have an effect in these and other nonmusculoskeletal conditions. Until the results of such research are available, the benefits of SMT for specific or general nonmusculoskeletal disorders should not be promoted as having strong supportive evidence. Further, a lack of evidence cannot be interpreted as counterevidence, nor used as evidence of falsification or verification.
Conclusion Based on the available evidence, some statements generated from the Summit were extrapolated beyond the data, have the potential to misrepresent the literature, and should be used with caution. Given that none of the trials included in the literature review were definitively negative, the current evidence suggests that more research on nonmusculoskeletal conditions is warranted before any definitive conclusions can be made. Governments, insurers, payers, regulators, educators, and clinicians should avoid using systematic reviews in decisions where the research is insufficient to determine the clinical appropriateness of specific care.
Key Indexing Terms Humans, Manipulation, Spinal. Publications. Policy Making. Public Health
From the FULL TEXT Article:
Introduction
In “Pathways to ‘Evidence-Informed’ Policy and Practice: A Framework for Action,” Bowen and Zwi state, “The extent to which individual, organizational, and system-level values influence a decision to accept or reject the policy-related evidence is largely unexplored in the literature.” [1] Researchers frequently do not recognize the political, ideological, and economic factors that influence policy development or the social context within which evidence will be used. As Dobrow et al note, evidence-based medicine (EBM) and evidenced-based policy are 2 different constructs: Evidence-based policy is not simply an extension of EBM; instead, it involves moving from the individual clinical level to a population-policy level. Noting the requirement for explicit justification, they state that “decisions are subject to greater public scrutiny and outcomes directly affect larger numbers of people heightening the requirement for explicit justification.” [2] Policy decisions should be made carefully with practical operational orientations. Dobrow et al propose 3 components that should be involved in such decision-making:The internal decision-making context accounts for the environment in which a decision is made and includes factors such as the purpose for the decision-making activity, the role of participants in a decision-making process and the process employed to arrive at a decision outcome. [2]
In 2019, a “Global Summit” aimed to perform a systematic review of the literature on the efficacy and effectiveness of mobilization or spinal manipulative therapy (SMT) for the primary, secondary, and tertiary prevention and treatment of nonmusculoskeletal (non-MSK) disorders. [3] However, the resulting article extrapolated beyond the data, resulting in overstated policy implications and conclusions.
Specifically, we are concerned that the Summit review fails to adequately address the limitations of such a systematic review in making policy implications given the limited scope of evidence available on the topic of SMT for non-MSK disorders, the biological plausibility of collapsing 5 completely different disorders into a single “viscerosomatic” category, and best practices for using evidence in policy-making. Therefore the purpose of the present article is to discuss concerns regarding the potential for misguided policy and to offer an alternate interpretation of the data using current models and criteria.
Methods
In September 2019, 49 scientists were invited to meet in Toronto, Canada, for the Summit meeting. The meeting coordinators stated that the goal was to develop a rigorous review of the scientific literature regarding the effectiveness of spinal manipulation as a stand-alone therapy in treating non-MSK conditions based on randomized controlled trials (RCTs). [3] Participants identified 16 articles, reporting on 14 RCTs, that met their inclusion criteria. They performed a comprehensive quality rating on the articles, and included in the review those that were rated to be of either high [4–6] (n = 3) or acceptable quality [7–9] (n = 3).
We attended the meeting and participated in this process, [3] as scientific reviewers and 1 as a program moderator. As participants, we were invited to coauthor the Summit review. However, upon review of the manuscript draft, we identified concerns relating to the process and the interpretation of the materials. Therefore, we declined to be listed as coauthors on that review. After considering the published review from the Summit, we developed the present article to discuss the weaknesses we found in the Summit study's methods and interpretation and to offer an alternate interpretation of the data. [3]

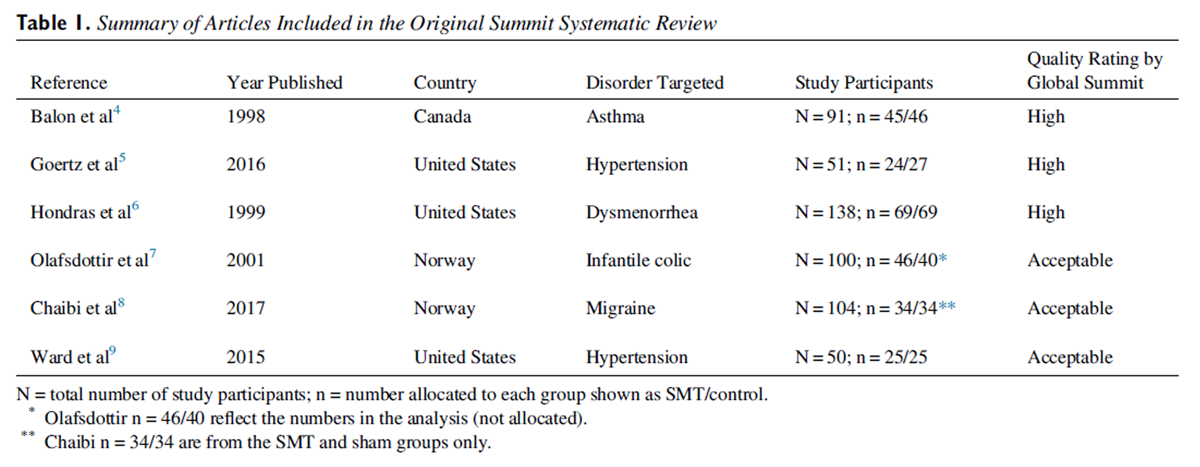
Table 1
Results
Of the articles identified by the Summit, a total of 6 RCTs investigating 5 non-MSK disorders were selected, representing 534 study participants (Table 1).
Discussion
In our review of the final Summit article, we identified 3 primary areas for discussion: limitations of systematic reviews for decision-making on the topic of SMT for non-MSK disorders, the biological plausibility of collapsing 5 different disorders into a single category, and best practices for using evidence in policymaking.
Limitations of Systematic Reviews
Although there is general agreement in health-services research about the usefulness of systematic reviews, there is also agreement about their limitations. These become especially pertinent when implications are made regarding appropriate health policy. Systematic reviews are a necessary but insufficient method for making clinical judgments, [10, 11] and are an aid to clinical decision-making but not a substitute for it. Given this, we express our concern that the Summit article used a systematic review to support policy implications targeted toward health care delivery systems, regulatory agencies, educational institutions, educational regulators, clinicians, and researchers. We wish to point out the limitations inherent in this process for those who may be unaware.
The Summit review was limited to RCTs, and due to the paucity of RCTs available, no meta-analysis was conducted. There are sufficient examples in the literature of single RCTs later being contradicted by other RCTs. There is also sufficient evidence that high-quality RCTs are not the only type of study that can inform clinical efficacy and effectiveness. [12] Systematic reviews are based on a hierarchy for evidence, with RCTs at the higher levels. But as Rothman states, “mindlessly ascribing greater validity to a study based on a hierarchy of designs is fallacious.” [12] Privileging certain forms of evidence over others may ultimately be a political act, not a scientific one. As noted by Blunt:The conclusion is that hierarchies in general embed untenable philosophical assumptions: principally that information about average treatment effects backed by high-quality evidence can justify strong recommendations, and that the impact of evidence from individual studies can and should be appraised in isolation. Hierarchies are a poor basis for the application of evidence in clinical practice. [13]
Jonas includes a wide range of evidence, [14] and given the few studies available on the topics considered by the Summit, it behooves those making policy to consider the totality of this topic. The issues of concern would include health-services research, [15] practice-based studies, [16, 17] comparative-effectiveness studies, [18] qualitative and observational studies, [19] and expert panels. [20]
Further, by confining the review to RCTs of spinal manipulation as a stand-alone treatment in controlled environments, the Summit reviewers ignored the actualities of chiropractic practice in the real world. We know that in addition to SMT, supportive treatments are commonly used by doctors of chiropractic, including self-care recommendations, therapeutic exercise, myofascial therapies, and patient education. [21] In the RCTs chosen for review by the Summit, these adjunctive therapies were intentionally excluded based on the research design.
Given these concerns, in evaluating the Summit publication we asked ourselves several questions. First: Was it appropriate to use P < .05 alone to determine effectiveness or efficacy, given the small sample sizes of the studies evaluated? Second: Can findings from only 6 studies be considered generalizable? And third: Were the findings robust enough to support the stated policy implications?
Use of P < .05 alone
The Summit review describes first dichotomizing point estimates of between-group differences in each study at P < .05. If those criteria were not met, the study was judged to be negative, without consideration of clinically meaningful effects or power. As Greenland et al point out, “a definitive conclusion of ‘no association’ cannot be deduced from a P value, no matter how large.” [22] Even with high-quality RCTs, not all the assumptions underlying P values are likely to be true, such as the test (null) hypothesis plus all assumptions associated with issues such as sampling, participation, and missing data. An examination of the confidence intervals found in the 6 studies examined by the Summit authors reveals estimates that are compatible with meaningful differences. Moreover, P value functions associated with each estimate demonstrate that several hypotheses favoring the benefit of SMT are more likely than the null hypothesis. This has the same support as the counter-null, which is when the evidence favors no association by exactly the same amount. [23] Thus, a reliance on statistical significance and the point estimate for clinical relevance can result in erroneous interpretation of the evidence.
Confidence intervals and P value functions should be examined for clinically meaningful effects that are more or less compatible with the data. In addition, it is important to consider if there is a small sample size for each RCT and thus an inherent difficulty in statistically detecting clinically meaningful effects which larger studies and pooling of similar studies of the same intervention may detect. As Greenland et al state, “lack of statistical significance of individual studies should not be taken as implying that the totality of evidence supports no effect.” [22]
Studies not generalizable
It is unlikely that the estimates from 6 studies included in the Summit review were generalizable to the source populations, nor were they transportable to populations outside the source populations of the samples. As Westreich et al point out:When a study sample is not formally representative of (or alternately, the same as) the target population, we cannot assume that the true causal effect in a study sample will be the same as the true effect in the population, and thus that the (even unbiased) estimate of the study sample effect will also be an accurate estimate of the target population effect. [24]
In the case of the Summit document, the small sample sizes in each individual study indicate that even collectively, the study population is likely not representative of any target populations of clinical interest.
Policy implications
The evidence in the Summit review is not sufficient to support its sweeping policy implications and statements against clinical application and continued study of SMT for all non-MSK conditions. The 6 selected RCTs lacked perfect measurement and adherence, and all had missing data or loss to follow-up. Therefore, it cannot be assumed that the estimated effects are valid even in the study populations. The consideration of SMT for migraine headaches is illustrative of this point. The Summit review included only 1 article evaluating the effectiveness of SMT for migraine headaches, which was rated as acceptable quality. Based on this 1 article, the Summit concluded that SMT was not effective and should not be studied further. However, in a systematic review and meta-analysis of 6 RCTs (pooled sample size of 677) published in Headache in April 2019, Rist et al conclude that “SMT may be an effective therapeutic technique to reduce migraine days and pain/intensity” and recommend further research in this area. [25]
It is not clear why there is a difference between the Summit conclusions and the findings by Rist et al on migraines. A recent article by Dieckmann and Johnson suggests that several factors may influence scientific disagreement, including issues of bias (intentional and unintentional), differences in the use of scientific methods, and “historical developments in their respective fields or sub-disciplines.” [26] Regarding differences in scientific methods, the Summit review describes the assessment of the methodological quality of eligible studies using the Scottish Intercollegiate Guidelines Network criteria, [27] whereas Rist et al use the Cochrane Risk of Bias Tool. [28] As a result of this methodological choice, the Summit review includes only the 1 study on migraine headaches, with 104 participants. By comparison, Rist et al pooled data across 6 studies, resulting in a pooled sample size of 677 participants. The Summit review dismisses the Rist et al study because it included studies with potential risk of bias, but fails to mention the strengths inherent in a significantly greater overall sample size. [3] Therefore, by the design of inclusion or exclusion, these study findings were quite different.
Biological Plausibility
Biological plausibility is an essential component to consider when undergoing scientific scrutiny. Therefore, the basis on which biological plausibility is established must be sound to provide for a sound investigation. When there is limited evidence for or against the use of a particular clinical intervention, the given intervention must have “biological plausibility.” [29] This means that there needs to be a scientifically plausible anatomical or biological rationale by which the intervention might work.
In the Summit paper, 5 distinct clinical entities — asthma, dysmenorrhea, hypertension, infantile colic, and migraine — were collapsed into 1 category as if these disorders all have a common underlying mechanism. The only scientifically acceptable reason to consider the 6 articles under a single health disorder instead of as 6 articles on 5 different conditions would be if the conditions all shared a common underlying pathophysiological cause. The Summit review assumes that the rationale for treatment was “the same across non-musculoskeletal disorders conditions; specifically, that treating spinal dysfunctions with SMT has a physiological effect on organs and their function.” [3] However, based on current medical literature, the mechanisms of the 5 conditions either are unknown or are distinct for each condition, thus providing no biologically plausible reason to consider these 5 different clinical entities as 1 condition.
According to the World Health Organization, hypertension is “when blood pressure is too high.” [30] The cause of essential hypertension is unknown. The World Health Organization identifies modifiable risk factors as unhealthy diet including excessive salt consumption, high saturated or trans-fat intake, and low intake of fruits and vegetables; physical inactivity, consumption of tobacco and alcohol; and being overweight or obese — so there is no 1 cause to link primary hypertension to the other 5 conditions.
The cause of primary dysmenorrhea is also not clear. The most widely accepted cause is overproduction of uterine prostaglandins. [31] Dysmenorrhea is the leading cause of gynecologic morbidity in women of reproductive age, independent of age, nationality, or economic status, [31] and a World Health Organization systematic review indicates that it is the most important cause of pelvic pain. [32]
The cause of migraine is multifactorial. A recent review article on migraine headache summarizes many of the potential biological causes of migraine. [33] During a migraine headache, there are increased blood flow changes in the brainstem, pons, thalamus, basal ganglia, and cortex. A positron emission tomography imaging study in people with migraine who experience nausea found changes in nausea-related brain circuits including the nucleus of the tractus solitarius, the dorsal motor nucleus of the vagus nerve, the nucleus ambiguus, and the periaqueductal gray. [34] Another article indicates that central sensitization of third-order thalamic neurons is likely the cause of the allodynia, which occurs during the headache phase of migraine and is a symptom in around 65% of migraines. [35]
Asthma is an inflammatory condition of the airways, with symptoms that include shortness of breath, wheezing, and coughing. [36] There are different underlying causes with at least 4 different phenotypes: early-onset allergic, early-onset allergic moderate to severe remodeled, late-onset nonallergic eosinophilic, and late-onset nonallergic, non-eosinophilic. The diverse phenotypes of asthma do not have the same underlying causes. Because of their differing etiologies, it is unlikely that all types of asthma share a common mechanism. Therefore, this disorder should not be combined with other non-MSK syndromes and treated as if all were the same condition.
Infantile colic is “excessive crying for at least 3 hours per day, on at least 3 days per week for at least 3 weeks.” [7] No single cause for infantile colic has been identified, although several hypotheses are being considered. Recently the gut microbiome has been indicated, with some evidence in breastfed infants that the probiotic Lactobacillus reuteri decreases periods of crying. [37]
The Summit review draws the following conclusion:Collectively, the evidence from six high and acceptable quality RCTs casts doubt on the hypothesis that SMT is efficacious or effective for the management of non-musculoskeletal disorders and thereby also challenge the validity of the underlying theories relating to the subluxation and the autonomic nervous system. [3]
However, it is important to note that none of the authors of the 6 studies in question stated that they were testing “theories relating to the subluxation.” It seems that the Summit authors may have applied their own post hoc hypothesis to the work of others, which is a contributing bias that would likely influence the results. Additionally, with vast possibilities for the etiology of these 5 non-MSK conditions, there is no unifying, scientifically validated mechanism. Therefore, there is no biologically plausible reason to consider them as a single entity.
Evidence-Based Policy
Making strong policy implications based on weak scientific evidence is a cause for concern. The Summit review states:We found no evidence of an effect of SMT for the management of non-musculoskeletal disorders including infantile colic, childhood asthma, hypertension, primary dysmenorrhea, and migraine. This finding challenges the validity of the theory that treating spinal dysfunctions with SMT has a physiological effect on organs and their function. Governments, payers, regulators, educators, and clinicians should consider this evidence when developing policies about the use and reimbursement of SMT for non-musculoskeletal disorders. [3]
After this, the article then gives policy implications, suggesting that the findings be used to substantially affect payment policies, chiropractic education, regulations related to chiropractic scope of practice, clinical practice, and research. We suggest that these implications are not properly grounded in the review and far exceed what can be justified scientifically or ethically based on 6 studies of heterogeneous illnesses. This concern is based on our experience of scientific perspectives [38–51]and conducting policy research at academic institutions that are not affiliated with any chiropractic organizations.
As mentioned earlier, EBM and evidence-based policy are 2 different constructs. Policy decisions should be made carefully and should consider the 3 components proposed by Dobrow et al, namely “the purpose for the decision-making activity, the role of participants in a decision-making process and the process employed to arrive at a decision outcome.” [2]
One requirement for making the transition from EBM to evidence-based policy is defining what constitutes the evidence. The methods used for the Summit, based on systematic reviews, are considered philosophical-normative, which means that the quality of the evidence is judged on normative qualities such as structural characteristics and properties of the evidence. [2] In the case we are discussing, those properties are reliability and validity, rigor, and the research design (eg, double-blinded RCTs). These characteristics then lead to scoring the studies and the quality of the evidence. This approach was used by Cochrane and was the basis of the Canadian Task Force on the Periodic Health Examination in 1994. It is highly dependent on quality of the studies that are available. Therefore, one must question whether using the same evaluation and recommendation processes is appropriate when the number of quality studies is substantially lacking.
As a solution, Dobrow et al describe how to evaluate an issue when the number of studies is low. For example, in screening for colorectal cancer, where various tests are available, an RCT existed only for the fecal occult blood test. In this case, evidence other than from RCTs can also be included, and subjected to strict evaluation protocols. Dobrow et al note that such an approach also needs to consider ethnic and cultural acceptability for both providers and patients. This approach to policy-making they call a practical operational orientation, in contrast to the following description of the philosophical-normative orientation:While the philosophical-normative orientation allows important questions to be raised regarding the quality and appropriateness of evidentiary sources, this orientation also restricts thinking on evidence-based decision-making to narrowly defined scientific evidence, neglecting the role context plays in impacting on what constitutes evidence. [2]
However, when we compare the solution of Dobrow et al to the processes used by the Summit, this strategy was not adopted, even in situations where there was only a single RCT available. Given the paucity of the data, which was already known before the conference, other clinical data should have been reviewed and considered.
Since policy can have far-reaching implications, it would be expected that those who have expertise in policy-making and analysis would be included in the process. A group made up only of scientists may not necessarily be appropriate as the sole decision-makers for policy implications. Although a very diverse group of policy-makers attended the Summit meeting, including the closing session where the voting occurred, policy was not part of the discussion during the meeting. None of the policy implications included in the resulting article were proposed at the meeting for discussion. No policy implications were considered or voted on as was the case for the research evidence conclusions.
Including policy-makers at that time in a dialogue about the implications of the evidence on policy would have been an appropriate approach. However, that dialog did not occur, even though it appears that policy conclusions have been inserted into an article that was supposed to be a reflection of the Summit meeting. Since the implications of the findings are aimed at policy-makers, their exclusion from the discussion, even though they were present, seems disconcerting.
The processes by which the policy implications were arrived at after the Summit are unclear. These processes were not described during the conference, which is in stark contrast to how well the methods for reviewing the literature were described. If the claim is that the stated implications are based solely on the evidence hierarchies from the systematic reviews, and not any political or ideological considerations, then there is not sufficient evidence to support them.
Dobrow et al describe this type of problem:With growing interest in evidence-based health policy it has become increasingly clear that existing models of evidence-based decision-making, focused solely on evidence, cannot adapt to the contextual features of broader policy environments. [2]
While the Summit review suggests that further research may lead to new evidence, the conclusions place untenable restrictions on the types of research to be done by stating that future studies should include “interventions that have a clear biological target.” [3] One should consider the expectations that are needed for any study involving SMT.
To put this into a broader context, consider the studies published by the RAND Corporation, which is a research organization with the primary purpose of providing solutions to public policy challenges. Two of the present authors (E.L.H. and I.D.C.) participated in the first systematic reviews on manipulation for acute and chronic low back and neck pain conducted by the RAND Corporation. [38, 39, 48–51]In the 1992 study, there were 5 RCTs of SMT for acute low back and 1 for chronic low back pain. [37] Three of these 6 low-quality RCTs suggested no benefit; the other 3 suggested a benefit. Lower-quality studies may be more likely to detect benefits than higher-quality studies, and none of the 6 in that review would likely meet the threshold for inclusion in a best-evidence synthesis today. Thus, that review of SMT for low back pain found insufficient evidence to make statements about policy implications or recommendations, but certainly no high-quality supportive evidence. [38]
A similar result would also have been true for cervical spine pain, which also showed insufficient evidence. [49, 51] Therefore, by Summit standards there would have been no quality evidence supporting the effectiveness of SMT for acute or chronic low back pain or for cervical pain. Consider 2 systematic reviews on chronic neck pain [47] and chronic low back pain, [45] both showing positive effects with the current body of literature. The work informing these reviews would perhaps not exist if earlier authors had made similar negative implications as those made in the Summit review. And it is likely that chiropractic practice would be different if health care policy-makers had received such information. One might suggest that the RAND studies led to the inclusion of SMT in the Bigos et al guidelines [52] and to an increasing research focus on SMT and back pain of all kinds. Thus, it would be unfortunate if clinical investigations were prematurely cut short based on what we suggest are untenable restrictions on research.
Based upon these observations and given the evidence that suggests a potential clinical benefit and that none of the trials were definitively negative (ie, with a confidence interval tightly wound around the null), the evidence more accurately suggests that more research on non-MSK conditions is warranted.
Summary of Our Observations
As we were a part of the early Summit process, we observed that the Summit authors worked together on a single research task and invited nonscientific observers, some of whom are responsible for shaping policy. However, during the process, weak evidence was extrapolated to prescriptive policy implications, and these statements were not crafted in the same careful way that the scientific literature was evaluated. The result was an overreach of the available evidence and conclusions that undermine the quality of the research.
This problem was exacerbated when a biologically plausible rationale was not included for collapsing 5 unrelated disorders together into 1 broad category labeled “non-MSK conditions.” The Summit review had the potential to answer at least part of this with regard to the existing evidence on efficacy through RCTs. However, it is not able to answer definitively with regard to effectiveness or develop sweeping policy implications as a result.
The Summit process provides a telling example of the potential disconnect between evidence and policy, particularly with respect to those whose expertise is not in policy creation. Even for the Cochrane Effective Practice and Organization of Care, which makes practice recommendations based on systematic reviews, there are standards that must be followed. We propose that the more important question after the Summit should have been what policy should be considered when there is insufficient evidence to provide a basis for resolving controversial issues. [1]
This is not a new issue among policy-makers. [1, 2, 51–53] One could argue that it is an integral part of all health policy-making. To make sweeping policy implications on such a paucity of evidence goes far beyond what is justified by the evidence. Based upon the selection of the research evidence, we propose a more accurate conclusion as follows.
Conclusion for SMT for Non-MSK Disorders
The small cadre of high- or moderate-quality randomized controlled trials reviewed in this study found either no or equivocal effects from SMT as a stand-alone treatment for infantile colic, childhood asthma, hypertension, primary dysmenorrhea, or migraine, and found no or low-quality evidence available to support other nonmusculoskeletal conditions. Therefore, further research is needed to determine if SMT can have an effect in these and other nonmusculoskeletal conditions. Until the results of such research are available, the benefits of SMT for specific or general nonmusculoskeletal disorders should not be promoted as having strong supportive evidence. Further, a lack of evidence cannot be interpreted as counterevidence or used as evidence of falsification or verification.
Limitations
This article offers different conclusions based on the same studies as those reviewed by the Summit conference. It is possible that including other authors or adding other RCTs could have changed our conclusions.
Conclusion
Based on the available evidence, some statements generated from the Summit event have extrapolated beyond the data, have the potential to misrepresent the literature, and should be used with caution. Given that none of the trials included in the literature review were definitively negative, the current evidence suggests that more research on nonmusculoskeletal conditions is warranted before any definitive conclusions can be made. Governments, insurers, payers, regulators, educators, and clinicians should avoid using systematic reviews in decisions where the research is insufficient to determine the clinical appropriateness of specific care.
Practical Applications
The overly decisive nature of the Global Summit's conclusions is not scientifically justified by the work presented.
The limitations of the systematic reviews were not properly addressed.
Grouping 5 physiologically different health conditions into a single category is inappropriate on the basis of biological implausibility.
Best practices regarding the use of evidence to support the stated policy implications were not followed.
The evidence from the Global Summit suggests that more research on nonmusculoskeletal conditions is warranted before any definitive conclusions can be made.
Governments, insurers, payers, regulators, educators, and clinicians should avoid using systematic reviews to make decisions when the research is insufficient to determine the clinical appropriateness of specific care
Funding Sources and Conflicts of Interest
No funding sources were reported for this study. C.M.G. reports no current conflicts of interest but has received personal fees within the past 3 years from the Spine Institute for Quality, personal fees from Palmer College of Chiropractic, and personal fees from American Chiropractic Association. No other conflicts of interest were reported.
Contributorship Information
Concept development (provided idea for the research): C.M.G., E.L.H., B.A.M., I.D.C.
Design (planned the methods to generate the results): C.M.G., E.L.H., B.A.M., I.D.C.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): C.M.G., E.L.H., B.A.M., I.D.C.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): C.M.G., E.L.H., B.A.M., I.D.C.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): C.M.G., E.L.H., B.A.M., I.D.C.
Literature search (performed the literature search): C.M.G., E.L.H., B.A.M., I.D.C.
Writing (responsible for writing a substantive part of the manuscript): C.M.G., E.L.H., B.A.M., I.D.C.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): C.M.G., E.L.H., B.A.M., I.D.C.
References:
Bowen S Zwi AB
Pathways to “evidence-informed” policy and practice: a framework for action.
PLoS Med. 2005; 2: e166Dobrow MJ Goel V Upshur R
Evidence-based health policy: context and utilisation.
Soc Sci Med. 2004; 58: 207–217Côté P Hartvigsen J Axén I et al.
The global summit on the efficacy and effectiveness of spinal manipulative therapy
for the prevention and treatment of non-musculoskeletal disorders: a systematic review of the literature.
Chiropr Man Therap. 2021; 29: 8Balon J Aker PD Crowther ER et al.
A Comparison of Active and Simulated Chiropractic Manipulation as Adjunctive Treatment
for Childhood Asthma
New England Journal of Medicine 1998; 339(15): 1013-1020Goertz CM Salsbury SA Vining RD et al.
Effect of Spinal Manipulation of Upper Cervical Vertebrae on Blood Pressure:
Results of a Pilot Sham-Controlled Trial
J Manipulative Physiol Ther. 2016 (Jun); 39 (5): 369–380Hondras MA Long CR Brennan PC
Spinal manipulative therapy versus a low force mimic maneuver for women with
primary dysmenorrhea: a randomized, observer-blinded, clinical trial.
Pain. 1999; 81: 105–114Olafsdottir E, Forshei S, Fluge G, Markestad T:
Randomised Controlled Trial of Infantile Colic Treated With Chiropractic Spinal Manipulation
Archives of Disease in Childhood 2001 (Feb); 84 (2): 138–141Aleksander Chaibi, Jurate Šaltyte Benth, Peter J Tuchin, Michael Bjřrn Russell
Chiropractic Spinal Manipulative Therapy For Migraine: A Three-Armed, Single-Blinded,
Placebo, Randomized Controlled Trial
European Journal of Neurology 2017 (Jan); 24 (1): 143–153Ward J Tyer K Coats J Williams G Kulcak K
Immediate effects of upper thoracic spine manipulation on hypertensive individuals.
J Man Manip Ther. 2015; 23: 43–50Linde K Coulter ID
Systematic reviews and meta-analyses.
in: Lewith GJW Walach H Clinical Research in Complementary Therapies. 2nd ed.
Elsevier, Oxford, UK2011: 119–134Coulter ID
Evidence summaries and synthesis: necessary but insufficient approach for determining
clinical practice of integrated medicine?
Integr Cancer Ther. 2006; 5: 282–286Rothman KJ
Six persistent research misconceptions.
J Gen Intern Med. 2014; 29: 1060–1064Blunt C
Hierarchies of Evidence in Evidence-Based Medicine.
The London School of Economics and Political Science London, UK, Location 2015Jonas WB
Building an evidence house: challenges and solutions to research in complementary and alternative medicine.
Complement Med Res. 2005; 12: 159–167Coulter ID
Evidence-based dentistry and health services research: is one possible without the other?
J Dent Educ. 2001; 65: 714–724Coulter ID
Evidence-based practice and appropriateness of care studies.
J Evid Based Dent Pract. 2001; 1: 222–226Coulter ID
Putting the practice into evidence-based dentistry.
J Calif Dent Assoc. 2007; 35: 45–49Coulter ID
Comparative effectiveness research: does the emperor have clothes?
Altern Ther Health Med. 2011; 17: 8–15Coulter ID
Observational studies and evidence-based practice: can't live with them, can't live without them.
J Evid Based Dent Pract. 2003; 3: 1–4Coulter I Elfenbaum P Jain S Jonas W
SEaRCH™ expert panel process: streamlining the link between evidence and practice.
BMC Res Notes. 2016; 9: 16Long CR Lisi AJ Vining RD et al.
Veteran Response to Dosage in Chiropractic Therapy (VERDICT): study protocol of
a pragmatic randomized trial for chronic low back pain.
Pain Med. 2020; 21: S37–S44Greenland S Senn SJ Rothman KJ et al.
Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations.
Eur J Epidemiol. 2016; 31: 337–350Infanger D Schmidt-Trucksäss A
P value functions: an underused method to present research results and to promote quantitative reasoning.
Stat Med. 2019; 38: 4189–4197Westreich D Edwards JK Lesko CR Cole SR Stuart EA
Target validity and the hierarchy of study designs.
Am J Epidemiol. 2019; 188: 438–443Rist PM, Hernandez A, Bernstein C, et al.
The Impact of Spinal Manipulation on Migraine Pain and Disability:
A Systematic Review and Meta-Analysis
Headache: The Journal of Head and Face Pain. 2019 (Apr); 59 (4): 532–542Dieckmann NF Johnson BB
Why do scientists disagree? explaining and improving measures of the perceived causes of scientific disputes.
PLoS One. 2019; 14e0211269Harbour R Miller J
A new system for grading recommendations in evidence based guidelines.
BMJ. 2001; 323: 334–336Higgins JP Thomas J Chandler J et al.
Cochrane Handbook for Systematic Reviews of Interventions.
John Wiley & Sons, Chichester, UK2019Leboeuf-Yde C, Lanlo O, Walker BF:
How to Proceed When Evidence-based Practice Is Required
But Very Little Evidence Available?
Chiropractic & Manual Therapies 2013 (Jul 10); 21 (1): 24World Health Organization.
Hypertension. Available at:
https://www.who.int/news-room/fact-sheets/detail/hypertension
Accessed February 17, 2021.Bernardi M Lazzeri L Perelli F Reis FM Petraglia F
Dysmenorrhea and related disorders.
F1000Res. 2017; 6 (1645–1645)Latthe P Latthe M Say L Gülmezoglu M Khan KS
WHO systematic review of prevalence of chronic pelvic pain: a neglected reproductive health morbidity.
BMC Public Health. 2006; 6: 1–7Straube A Andreou A
Primary headaches during lifespan.
J Headache Pain. 2019; 20: 35Maniyar FH Sprenger T Schankin C Goadsby PJ
The origin of nausea in migraine—a PET study.
J Headache Pain. 2014; 15: 84Aguggia M Saracco MG Cavallini M Bussone G Cortelli P
Sensitization and pain.
Neurological Sciences. 2013; 34: 37–40Kaur R Chupp G
Phenotypes and endotypes of adult asthma: moving toward precision medicine.
J Allergy Clin Immunol. 2019; 144: 1–12Ouald Chaib A Levy EI Ouald Chaib M Vandenplas Y
The influence of the gastrointestinal microbiome on infant colic.
Expert Rev Gastroenterol Heptaol. 2020; 14: 1–13Shekelle PG Adams AH Chassin MR Hurwitz EL Brook RH
Spinal manipulation for low-back pain.
Ann Intern Med. 1992; 117: 590–598Hurwitz EL, Aker PO, Adams AH, Meeker WC, Shekelle PG.
Manipulation and Mobilization of the Cervical Spine:
A Systematic Review of the Literature
Spine (Phila Pa 1976) 1996 (Aug 1); 21 (15): 1746–1760Goertz GM, Pohlman KA, Vining RV, et al.
Patient-centered Outcomes of High-velocity, Low-amplitude Spinal Manipulation
for Low Back Pain: A Systematic Review
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 670-691Hurwitz, EL, Carragee, EJ, van der Velde, G et al.
Treatment of Neck Pain: Noninvasive Interventions: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S123–152Carragee EJ, Hurwitz EL, Cheng I, Carroll LJ, Nordin M, Guzman J, et al.
Treatment of Neck Pain: Injections and Surgical Interventions: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S153–169Carragee EJ Hurwitz EL Weiner BK
A critical review of recombinant human bone morphogenetic protein-2 trials i
n spinal surgery: emerging safety concerns and lessons learned.
Spine J. 2011; 11: 471–491Hurwitz EL Randhawa K Torres P et al.
The Global Spine Care Initiative: a systematic review of individual and
community-based burden of spinal disorders in rural populations in low-and middle-income communities.
Eur Spine J. 2018; 27: 802–815Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, Suttorp Booth M, Herman PM.
Manipulation and Mobilization for Treating Chronic Low Back Pain:
A Systematic Review and Meta-analysis
Spine J. 2018 (May); 18 (5): 866–879Nordin M Randhawa K Torres P et al.
The Global Spine Care Initiative: A Systematic Review for the Assessment of Spine-related Complaints
in Populations with Limited Resources and in Low- and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 816–827Coulter ID Crawford C Vernon H et al.
Manipulation and Mobilization for Treating Chronic Nonspecific Neck Pain:
A Systematic Review and Meta-Analysis for an Appropriateness Panel
Pain Physician. 2019 (Mar); 22 (2): E55–E70Coulter I
Manipulation and mobilization of the cervical spine: the results of a literature survey and consensus panel.
J Musculoskelet Pain. 1996; 4: 113–124Shekelle PG Coulter I
Cervical spine manipulation: summary report of a systematic review of
the literature and a multidisciplinary expert panel.
Clin Spine Surg. 1997; 10: 223–228Coulter ID
Efficacy and risks of chiropractic manipulation: what does the evidence suggest?
Integr Med. 1998; 1: 61–66Coulter ID Adams AH Hurwitz EL Meeker W Hansen DT
The Appropriateness of Manipulation and Mobilization of the Cervical Spine, Vol. 781.
Rand Corporation Santa Monica, CA, Location1996Stanley J. Bigos, MD, Rev. O. Richard Bowyer, G. Richard Braen, MD, et al.
Acute Lower Back Problems in Adults. Clinical Practice Guideline No. 14.
Rockville, MD: Agency for Health Care Policy and Research, [AHCPR Publication No. 95-0642].
Public Health Service, U.S. Department of Health and Human Services; 1994Atkins D Siegel J Slutsky J
Making policy when the evidence is in dispute.
Health Aff. 2005; 24: 102–113
Return to NON-MUSCULOSKELETAL DYSFUNCTION
Since 4-18-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |