

Soy Food Consumption and
Breast Cancer PrognosisThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Cancer Epidemiol Biom Prev. 2011 (May); 20 (5): 854–858 ~ FULL TEXT
Bette J. Caan, Loki Natarajan, Barbara Parker, Ellen B. Gold, Cynthia Thomson,
Vicky Newman, Cheryl L. Rock, Minya Pu, Wael Al-Delaimy, and John P. Pierce
Division of Research,
Kasier Permanente,
Oakland, CA 94612, USA.
bette.caan@kp.orgBACKGROUND: Contrary to earlier clinical studies suggesting that soy may promote breast tumor growth, two recent studies show that soy-containing foods are not adversely related to breast cancer prognosis. We examined, using data from the Women's Healthy Eating and Living (WHEL) study, the effect of soy intake on breast cancer prognosis.
METHODS: Three thousand eighty-eight breast cancer survivors, diagnosed between 1991 and 2000 with early-stage breast cancer and participating in WHEL, were followed for a median of 7.3 years. Isoflavone intakes were measured postdiagnosis by using a food frequency questionnaire. Women self-reported new outcome events semiannually, which were then verified by medical records and/or death certificates. HRs and 95% CIs representing the association between either a second breast cancer event or death and soy intake were computed, adjusting for study group and other covariates, using the delayed entry Cox proportional hazards model.
RESULTS: As isoflavone intake increased, risk of death decreased (P for trend = 0.02). Women at the highest levels of isoflavone intake (>16.3 mg isoflavones) had a nonsignificant 54% reduction in risk of death.
CONCLUSION: Our study is the third epidemiologic study to report no adverse effects of soy foods on breast cancer prognosis.
IMPACT: These studies, taken together, which vary in ethnic composition (two from the United States and one from China) and by level and type of soy consumption, provide the necessary epidemiologic evidence that clinicians no longer need to advise against soy consumption for women with a diagnosis of breast cancer.
From the Full-Text Article:
Introduction
Soy foods, a major source of phytoestrogens show both antiestrogenic and estrogen-like properties. Many studies have shown that soy consumption may protect against breast cancer, whereas other studies have shown that isoflavones, the major component of soy, enhance the proliferation of breast cancer cells in vitro [1], promote mammary tumor growth in rats [2], and possibly interfere with the effectiveness of tamoxifen. [3, 4] As a result, clinicians treating women with breast cancer frequently caution them to either avoid soy foods entirely or use them in moderation. [2, 5, 6]
To add to the uncertainty, 2 recent epidemiologic studies examining breast cancer survivors, 1 in Asian women from the Shanghai Breast Cancer Survival Study (SBCS; ref. 7) and 1 in U.S. women from the Life After Cancer Epidemiology (LACE) study [8], suggest that soy-containing foods do not adversely affect breast cancer prognosis, do not counteract the benefits of tamoxifen and may, in fact, offer some potential benefits in decreasing risk of recurrence or death from breast cancer. Before clinical recommendations can be made, these findings need to be replicated in other large cohorts with longer follow-up. We have explored this question further in secondary analyses by using data from the Women's Healthy Eating and Living (WHEL) study, a randomized controlled trial of a high fruit/vegetable/fiber and low fat dietary intervention in early-stage breast cancer survivors in the United States.
Materials and Methods
The WHEL study population has been previously described. [9] Briefly, 3,088 breast cancer survivors with a diagnosis between 1991 and 2000 who participated in a dietary intervention trial were followed throughout and after completion of the trial that ended in 2006. Enrolled participants had a diagnosis of and completed treatment (within the previous 4 years) of stage I, II, or III (AJCC VI classification) invasive breast cancer. Participants were 18 to 70 years of age and had no evidence of disease within the 12 months prior to study enrollment. During semiannual telephone interviews, women were queried about the occurrence of new outcome events. Any report of a breast cancer event was confirmed by medical records and/or death certificates and oncologist review. Finally, we searched the National Death Index by using Social Security Number, name, and date of birth to confirm cause of death.
Women included in this study had a median follow-up of 7.3 years from the time of enrollment. Soy intake (milligrams of isoflavones) was measured postdiagnosis (median 2 years, range: 2 months to 4 years) at study entry by using the Arizona Food Frequency Questionnaire (AFFQ), a 153-item semiquantitative, scannable questionnaire [10, 11] that included specific line items for “Meat Substitutes (such as Tofu, Veggie Burgers)” and “Soy Milk,” as well as an opportunity to include other soy food items on the “additional foods” list portion of the food frequency questionnaire (FFQ). Modified from the Block-National Cancer Institute Health Habits and History Questionnaire, the AFFQ, which has previously been validated against both 4-day food records [11] and 24-hour recalls [10], elicits information about the usual foods consumed and the frequency of consumption, using age- and gender-specific estimates of portions estimated as small, medium, or large.
In addition, information on soy supplement use since diagnosis was obtained by a separate questionnaire [12] asking respondents about the frequency and duration of use by using an extensive list of supplements and herbs and allowing participants to report their supplements not listed on the predetermined list in an open-ended question. A yes/no use variable was created, as the responses indicating the frequency and duration of soy supplement use were low.
Daily isoflavone intake, derived from totaling isoflavone intake across all line items in the FFQ, was generated using the USDA-Iowa State University Database on the Isoflavone Content of Foods. [13] Isoflavone contents of foods in the USDA database were collected from scientific articles published in refereed journals and were generated by extensive sampling of soy-containing foods and subsequent analysis at Iowa State University.
Data analyses
Women were divided into 4 groups, with the highest category (upper 5th percentile: 6.3–86.9 mg/d) representing intakes similar to those consumed in Asian populations. Delayed entry multiple Cox proportional hazards models [14] were developed and HRs and 95% CIs representing the association between either a second breast cancer event or all-cause mortality and level of soy intake were computed. A second breast cancer event included both local and distant recurrences and new breast primaries. All cause mortality included death due to any cause, although 81% of the deaths were due to breast cancer. The models were adjusted for randomization group, soy supplement use, and other demographic and clinical covariates known to be associated with breast cancer outcomes. Score tests were used to assess trends across quintiles. Residual plots were used to examine model fit. Likelihood ratio tests were used to examine interactions between isoflavone intake and each of tamoxifen use and estrogen receptor (ER)/progesterone receptor (PR) status, to examine whether these factors modified the association between isoflavones and outcomes. The software package R was used for all statistical analysis. [15]
Results

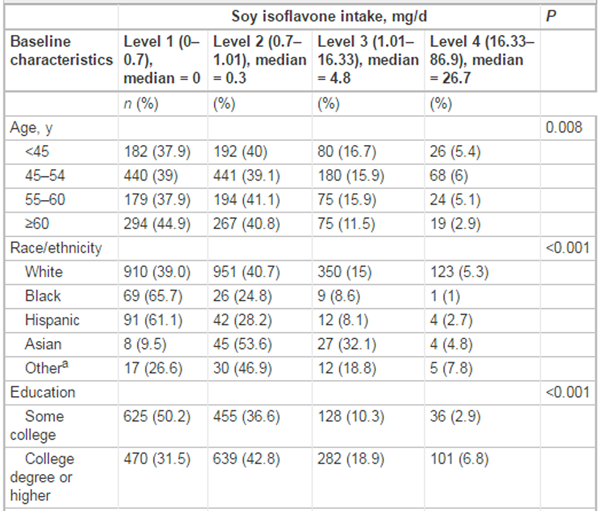
Table 1A
Table 1B
Table 2A
Table 2B
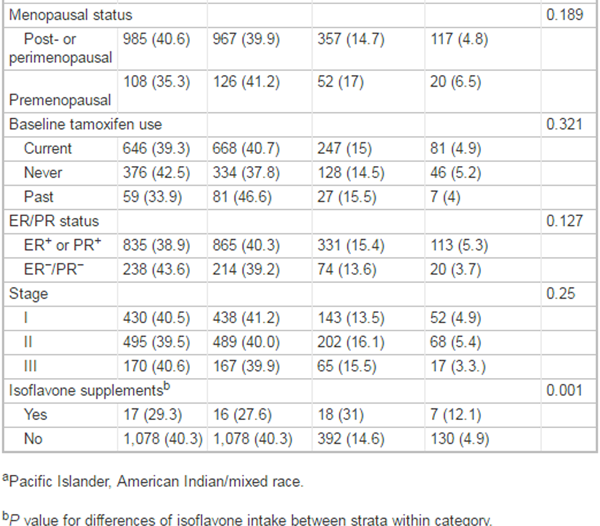
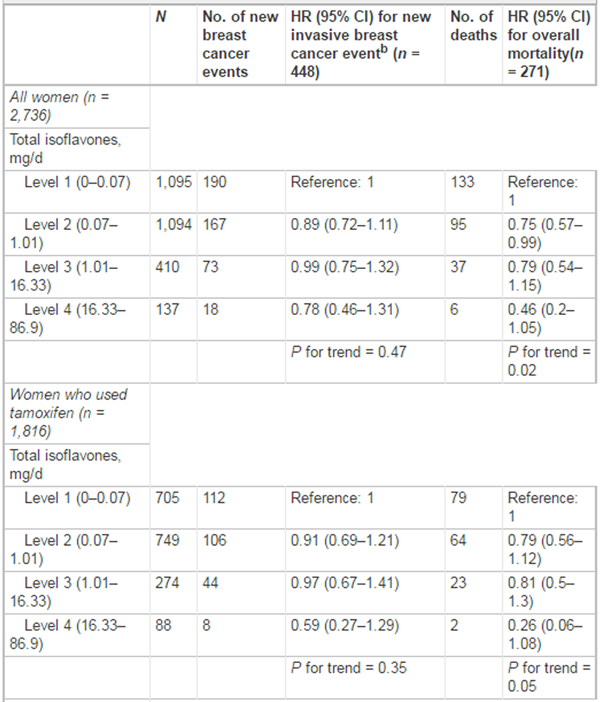
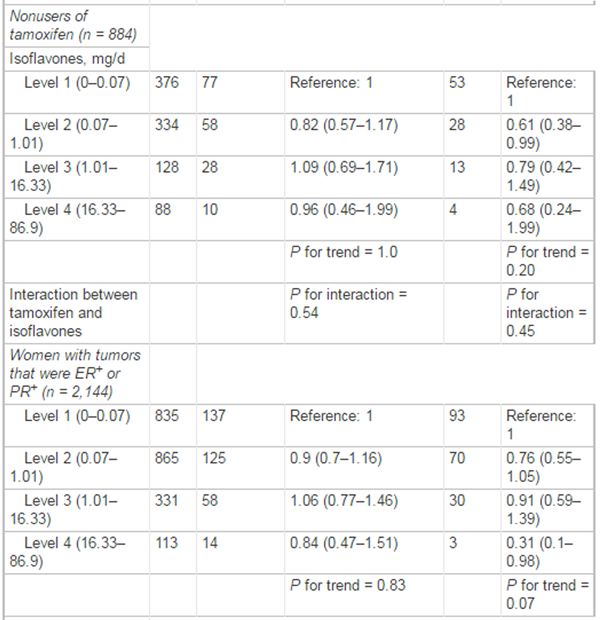
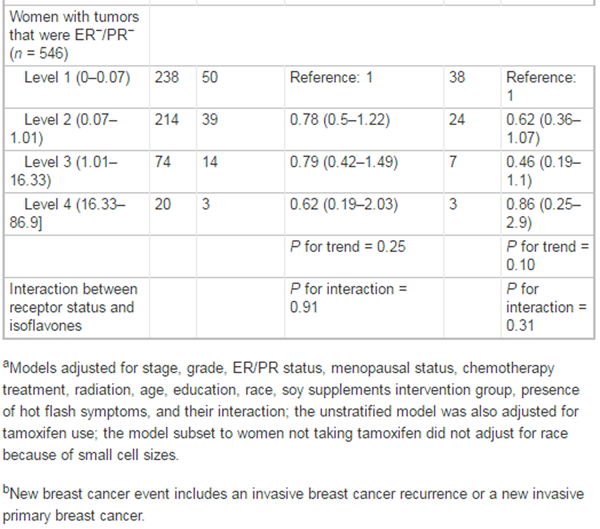
Table 2C Baseline isoflavone intakes did not differ between the intervention and control groups. Among women in the intervention and control groups, 19.2% and 20.8%, respectively, consumed greater than 10.1 mg of isoflavones daily (data not shown). Isoflavone intake differed by age, race/ethnicity, and education but did not differ by tamoxifen use, hormone receptor status, or menopausal status. Younger women, Asians, and women with a college degree or higher were the most likely to consume soy in the upper category (Table 1). Isoflavone intake was unrelated to the risk of a second breast cancer event overall or within strata of women defined by hormone receptor status or whether they ever used tamoxifen (Table 2). Furthermore, no significant increased or decreased risk was associated with any level of intake within strata (Table 2). In contrast, for overall mortality, risk of death tended to be lower as isoflavone intake increased (P for trend = 0.02). Women at the highest levels of isoflavone intake (>16.3 mg isoflavones, equivalent to at least one-half cup soymilk or 2-oz tofu each day) had a nonsignificant 54% reduction in risk of death compared with the lowest quintile of soy intake. Although the interaction between soy intake and tamoxifen use on mortality was not statistically significant (Table 2), the observed trend toward lower mortality with increased soy seemed stronger in women who had ever used tamoxifen (P for trend = 0.05). The trend toward lower mortality with increasing soy did not differ by hormone receptor status of the tumor. Sensitivity analyses were conducted by repeating the analysis restricted to the subgroup of women who were currently (at baseline) taking tamoxifen (N = 1,642); the results did not change (data not shown).
Discussion
Our study is now the third epidemiologic study in the recent past to report no adverse effects of soy food intake on breast cancer recurrence [7, 8] or total mortality [7] either alone or in combination with tamoxifen. [7, 8] Contrary to soy being harmful, these recent reports, to varying degrees, suggest possible benefits for breast cancer survivors.
Although the mean soy intake in the WHEL population is much lower than that observed among Chinese women in the SBCS (7), the suggested protective associations seen with total mortality for women in WHEL at the highest soy intake level are comparable with what was seen for Chinese women consuming similar levels of isoflavones. Similar to results from both the SBCS study [7] and the LACE study [8], the largest benefits associated with soy consumption in our study were seen in women who used tamoxifen. Continued research is needed to further understand and confirm these relationships, as in WHEL, power to detect associations at the highest level of soy intake was limited.
Strengths of the WHEL study include being one of the few existing studies of early-stage breast cancer survivors with long-term follow-up on both recurrence and survivial and information on postdiagnosis soy food intake. Although our analyses relied on self-report of soy food intake from the AFFQ, several validation studies have reported that assessment of soy intake by FFQs that use soymilk and tofu alone correlates well with isoflavone biomarkers either in blood or in urine. [16-19] In one study of U.S. adults [17], in which they compared a soy-specific 40-item FFQ to the more general 122-item WHI FFQ and examined intakes from both with plasma concentrations, they found that isoflavone intake was highly correlated between the 2 FFQ instruments (r = 0.84) and that isoflavone intake derived from both instruments were significantly correlated with plasma concentration of isoflavones. They also found that soymilk and tofu were the 2 major contributors to isoflavone intake and accounted for approximately 40% of total intake.
Because the WHEL cohort consists of early-stage breast cancer survivors who were enrolled on average 2 years after diagnosis, our results are not generalizable to women with a diagnosis of advanced-stage breast cancer and apply only to women who have survived, on average, 2 years since diagnosis.
In summary, we found no adverse associations of soy food consumption with breast cancer prognosis, even at levels similar to those consumed in Asian populations. Our study and the 2 previous epidemiologic studies, taken together, which vary in racial/ethnic composition (2 from the United States and 1 from China) and by level and type of soy consumption, provide the necessary evidence that clinicians no longer need to advise against soy food consumption for women with a diagnosis of breast cancer.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
References:
Taylor CK, Levy RM, Elliott JC, Burnett BP.
The effect of genistein aglycone on cancer and cancer risk:
a review of in vitro, preclinical, and clinical studies.
Nutr Rev 2009;67:398–415.Helferich WG, Andrade JE, Hoagland MS.
Phytoestrogens and breast cancer: a complex story.
Inflammopharmacology 2008;16:219–26Ju YH, Doerge DR, Allred KF, Allred CD, Helferich WG.
Dietary genistein negates the inhibitory effect of tamoxifen on growth
of estrogen-dependent human breast cancer (MCF-7) cells implanted in athymic mice.
Cancer Res 2002;62:2474–7Schwartz JA, Liu G, Brooks SC.
Genistein-mediated attenuation of tamoxifen-induced antagonism from
estrogen receptor-regulated genes.
Biochem Biophys Res Commun 1998;253:38–43Doyle C, Kushi LH, Byers T, Courneya KS,
Demark-Wahnefried W, Grant B, et al.
Nutrition and physical activity during and after cancer treatment:
an American Cancer Society guide for informed choices.
CA Cancer J Clin 2006;56:323–53Velentzis LS, Woodside JV, Cantwell MM,
Leathem AJ, Keshtgar MR.
Do phytoestrogens reduce the risk of breast cancer and breast cancer recurrence?
What clinicians need to know.
Eur J Cancer 2008;44:1799–806Shu XO, Zheng Y, Cai H, Gu K, Chen Z, Zheng W, et al.
Soy food intake and breast cancer survival.
JAMA 2009;302:2437–43Guha N, Kwan ML, Quesenberry CP, Weltzien EK, Castillo AL, Caan BJ, et al.
Soy isoflavones and risk of cancer recurrence in a cohort of breast cancer survivors:
the Life After Cancer Epidemiology study.
Breast Cancer Res Treat 2009;118:395–405Pierce JP, Natarajan L, Caan BJ,
Parker BA, Greenberg ER, Flatt SW, et al.
Influence of a diet very high in vegetables, fruit, and fiber and low in fat
on prognosis following treatment for breast cancer:
the Women's Healthy Eating and Living (WHEL) randomized trial.
JAMA 2007;298:289–98Thomson CA, Giuliano A, Rock CL,
Ritenbaugh CK, Flatt SW, Faerber S, et al.
Measuring dietary change in a diet intervention trial:
comparing food frequency questionnaire and dietary recalls.
Am J Epidemiol 2003;157:754–62Martínez ME, Marshall JR, Graver E,
Whitacre RC, Woolf K, Ritenbaugh C, et al.
Reliability and validity of a self-administered food frequency questionnaire
in a chemoprevention trial of adenoma recurrence.
Cancer Epidemiol Biomarkers Prev 1999;8:941–6Newman V, Rock CL, Faerber S,
Flatt SW, Wright FA, Pierce JP, et al.
Dietary supplement use by women at risk for breast cancer recurrence.
The Women's Healthy Eating and Living Study Group.
J Am Diet Assoc 1998;98:285–92Nutrient Data Laboratory.
USDA-Iowa State University Database on the Isoflavone Content of Foods,
Release 1.3–2002 [cited 2002].
Available from:
http://www.nal.usda.gov/fnic/foodcomp/Data/isoflav/isoflav.htmlTherneau TM, Grambsch PM,
Modeling Survival Data: Extending the Cox Model.
New York: Springer-Verlag; 2000R-Project.org [Internet].
Vienna: Vienna University of Economics and Business, Institute
for Statistics and Mathematics c2011
[updated 2009 May 13; access 2010 Nov 1].
Available from:
http://www.r-project.orgFrankenfeld CL, Patterson RE, Horner NK,
Neuhouser ML, Skor HE, Kalhorn TF, et al.
Validation of a soy food-frequency questionnaire and evaluation
of correlates of plasma isoflavone concentrates in postmenopausal women.
Am J Clin Nutr 2003;77:674–80Frankenfeld CL, Patterson RE, Kalhorn TF,
Skor HE, Howald WN, Lampe JW, et al.
Validation of a soy food frequency questionnaire with plasma concentrations
of isoflavones in US adults.
J Am Diet Assoc 2002;102:1407–13Jaceldo-Siegl K, Fraser GE, Chan J, Franke A, Sabate J.
Validation of soy protein estimates from a food-frequency questionnaire
with repeated 24-h recalls and isoflavonoid excretion in overnight urine
in a Western population with a wide range of soy intakes.
Am J Clin Nutr 2008;87:1422–7Williams AE, Maskarinec G, Hebshi S,
Oshiro C, Murphy S, Franke AA, et al.
Validation of a soy questionnaire with repeated dietary recalls
and urinary isoflavone assessments over one year.
Nutr Cancer 2003;47:118–25
Return to SOY PROTEIN
Since 3-29-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |