

Attitudes of Clinicians at the Canadian Memorial
Chiropractic College Towards the Chiropractic
Management of Non-musculoskeletal ConditionsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc. 2011 (Jun); 55 (2): 107–119 ~ FULL TEXT
OPEN ACCESS Jodi Parkinson, BSc, Jennifer Lau, BSc (Hons), Sandeep Kalirah, BHSc (Hons), and Brian J. Gleberzon, DC, BA, MHSc
Professor and Chair, Department of Applied Chiropractic,
Canadian Memorial Chiropractic College,
6100 Leslie St. Toronto, ON M2H 3J1,
bgleberzon@cmcc.caOBJECTIVE: The objective of this study was to determine the attitudes of clinical faculty during the 2009-2010 academic year at the Canadian Memorial Chiropractic College towards the treatment of various non-musculoskeletal disorders.
METHODS: A confidential survey was distributed to the clinical faculty via email. It consisted of several questions polling the demographic of the respondent such as years in clinical practice, and a list of 29 non-musculoskeletal conditions. Clinicians were asked to indicate their opinions on each condition on rating scale ranging from strongly agree to strongly disagree.
RESULTS: Twenty of 22 clinicians responded. The conditions garnering the greatest positive ratings include: asthma, constipation, chronic pelvic pain, dysmenorrhea, infantile colic, and vertigo. The options regarding vertigo and asthma, while demonstrating an overall positive attitude towards the benefits of chiropractic care, were stratified amongst clinicians with varying years in clinical practice.
CONCLUSION: This study suggests clinicians at this college are moderately open towards the chiropractic treatment of some non-musculoskeletal disorders.
KEYWORDS: CMCC; chiropractic; non-musculoskeletal; treatment
From the FULL TEXT Article:
Introduction“I was deaf 17 years ago and expected to remain so, for I had doctored a great deal without any benefit … Last January, Dr. Palmer told me that my deafness came from an injury in my spine. This was new to me; but it is a fact that my back was injured at the time I went deaf. Dr. Palmer treated my spine; in two treatments I could hear quite well. That was eight months ago. My hearing remains good.”(1p9)
The epochal event in the history of chiropractic occurred on September 18, 1895 when D.D. Palmer adjusted Harvey Lillard’s spine with the intent of restoring his lost hearing and, what may be lesser known, is that Palmer’s second patient presented with heart problems, a chief complaint that was also addressed using spinal adjusting directed to the patient’s mid back. [1–3] Two features of this well-known story are especially relevant. One is that it was Palmer’s intent to restore these patients functions via spinal adjusting of vertebrae that were “racked out of place,” [4, 5] since it is the intention of the practitioner which is often of paramount importance to many chiropractors6 and, secondly, the first two chiropractic patients did not present with the types of chief complaints that are typically associated with chiropractic care today. Rather than present with back pain, Palmer’s first two patients sought out his help to cure their non-musculoskeletal (non-MSK) conditions.
Palmer rationalized this therapeutic intention using the terms “tone” and “dis-ease” respectively, whereby “tone” referred to the intensity of an organ’s function as a reflection of the purported vibratory frequency of its associated nerves and “dis-ease” referred to the loss of innate intelligence, meaning the loss of the body’s ability to adapt to internal or external stressors. [7] Palmer posited that nerves supplying the organs were adversely affected when the nerves were impinged by subluxated spinal joints, [8] negatively influencing the body’s innate recuperative ability to heal. [7] D.D.’s son B.J. Palmer continued with this ideological approach, eventually developing the Meric technique system that linked specific spinal segments (vertemeres) to their corresponding end organs or structures. [9] Eventually the Meric Technique system evolved into the Full Spine Specific Technique, a technique system taught principally at the two Cleveland Colleges of Chiropractic today. [9]
Over the next century, there has been something of a divergence in the profession with, on the one hand, groups of chiropractors advocating the profession exclusively championing a “spinal health care model”10 to, on the other hand, groups of chiropractors who maintain the profession ought to pay homage to its vitalistic roots and continue with a more holistic, tonal-based worldview. [11–13] And of course there are chiropractors who bridge the gap between these two dichotomous poles, both in terms of practice activities and ideology.
Although the concept of chiropractic treatment for non-MSK conditions is controversial, students at the Canadian Memorial Chiropractic College (CMCC) are exposed to a variety of opinions on the subject. During their fourth and final year of studies students undergo their internship under the direct supervision of a licensed clinician at one of six clinics across the Greater Toronto Area. Clinicians, who are experienced Doctors of Chiropractic, have opinions based upon the accrual of their own education, clinical experience and personal ideology and it is possible they communicate these opinions to their interns during their rotation with them, not unlike how clinicians imprint their own personal preference on elements within the core curriculum taught to students during their undergraduate training. [14] In addition, since interns are providing chiropractic care under the direct supervision of the clinician, and technically are providing services under that clinician’s certificate of registration/license, it is the clinician who will be the final arbiter as to whether or not care is provided for this or that diagnosed condition at all.
Bearing all this in mind, the purpose of this study was to determine the attitudes of the supervising clinicians at CMCC towards the chiropractic management of various non-musculoskeletal conditions.
Methods
The study was approved by the Research and Ethics Board at CMCC.
Survey
An online survey using SurveyMonkey™ was conducted on 22 CMCC clinicians, instructing at any one of the six affiliated clinics during the 2009–2010 academic year. Using a 5-point rating scale (“strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”) clinicians were instructed to indicate their opinion on the efficacy of chiropractic treatment for specified non-musculoskeletal complaints. Each question required a response before the participant could proceed to the next question. (Appendix A)
SurveyMonkey™ is a web-based software program that enables users to create their own web-based surveys and/or questionnaires. An enhanced paid account was made available through the existing license purchased by CMCC. Clinician emails were obtained through requesting a directory from the human resources department at CMCC. The emails were uploaded into the survey tool (SurveyMonkey™). Emails consisting of a description of the study, as well as informed consent, were sent to the clinicians along with the survey URL. Clinicians were asked to read the description and informed consent form and given an option to proceed with the study, (implying agreement,) or to decline from participation.
Clinicians were not asked to input any personal identifiers on the survey. Survey responses were collected using the “Email Invitation Collector” (EIC) option provided by SurveyMonkey™. EIC allowed the survey tool system to automatically generate unique links tied to a specific email address. Only the recipient knew his/her link. Survey authors and data collectors were not able to see the assigned link inside the collector. As a person responds, only the email was tracked as a status – as having responded/completed the survey. No personal identifiers were linked to any particular survey. Data collection was handled by the authors of the survey who held the license to the “pro” account.
Confidentiality
Clinicians were not required to identify themselves in any way on the survey. Electronic identifiers only included email addresses which were removed from the raw data before analysis by the principal investigators.
Selecting conditions
The outcome measure was the ranking of effectiveness of chiropractic care for the following list of non-MSK conditions: ADHD/learning disabilities, arrhythmias/ECG abnormalities, asthma, autism, bowel/bladder dysfunction, cerebral palsy, chronic obstructive pulmonary disorder, chronic pelvic pain, constipation, Crohn’s Disease, depression, dysfunction of nursing, dysmenorrhea/PMS, eczema/psoriasis, hearing loss/tinnitus, hypertension, infantile colic, infertility/amenorrhea, multiple sclerosis, nocturnal enuresis, otitis media, Parkinson’s disease, pneumonia, seizures, ulcers, upper respiratory infection, urinary tract infection, vertigo, and visual disturbances. [15] This list was compiled from the 2001 literature review by Cheryl Hawk et al, [15] which in turn was based on their analysis of the most prevalent non-MSK complaints seen in chiropractic practice.
Data Analysis
This survey was intended to be a descriptive study based on overall trends, means, and proportions with groups stratified by years in practice. Using Microsoft Excel, responses were sorted by years in practice (<10, 10–20 and >20) and analyzed by the number of positive (strongly agree and agree), neutral and negative (strongly disagree and disagree) responses. By graphically examining the data, any observable trends were noted and that data was then analyzed again, calculating the percentage response of each tier. The percentage response allowed for comparison by proportions.
Results
Response Rate
All 22 clinicians were surveyed and 20 responded, yielding a response rate of 90.9%. All returned surveys were sufficiently completed to be used in the data analysis.

Table 1 Clinicians were asked to indicate their year of graduation, how many years they have been in practice, as well as to which ideologies they subscribe. Table 1 is a summary of the population demographics. It was observed that all clinicians surveyed had been educated at CMCC either for their doctor of chiropractic degree or for their post-graduate studies. Of the possible 22 respondents, it is observed that there is a disproportionate ratio of men (15) to women (7). Five clinicians had been in practice less than 10 years, nine had been in practice less than 20 years, and six had been in practice more than 30 years (Table 1). With respect to technique systems, most clinicians reported to use Diversified technique. [16]
When asked, the majority of respondents subscribed to more than one ideology (which accounts for this total response rate exceeding 100%), with the majority indicating they were functional based (n = 19), pain based (n = 17) and structural based practitioners (n = 11). Of the 20 respondents, two reported they were subluxation based (Table 1).
Table 2 Table 2 depicts the percentage of CMCC clinicians that strongly agree, agree, are neutral to, disagree, or strongly disagree to chiropractic treatment being beneficial to the conditions listed above. More than 50% of the clinicians agreed or strongly agreed that chiropractic could be effective for the treatment of asthma, chronic pelvic pain, constipation, dysmennorhea, infantile colic and vertigo (Table 2). Similarly, strong negative responses (disagree or strongly disagree) were noted for ADHD/learning disabilities, arrhythmias/ECG abnormalities, autism, Crohn’s disease, eczema/psoriasis, infertility/amenorrhea, Parkinson’s disease, pneumonia, seizures, upper respiratory infection, urinary tract infection and vision problems (Table 2). It is also observed that no one condition had a neutral response higher than 45% (Table 2).
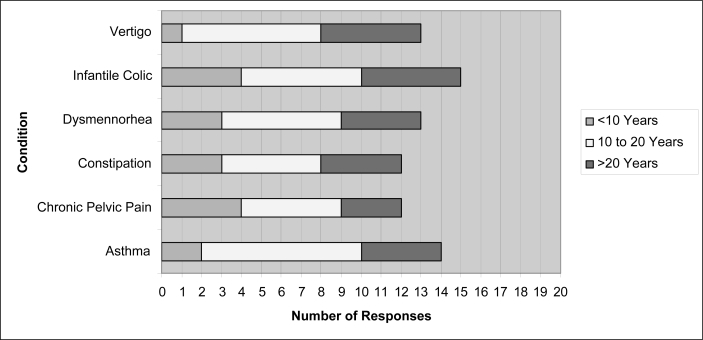
Figure 1
Table 3
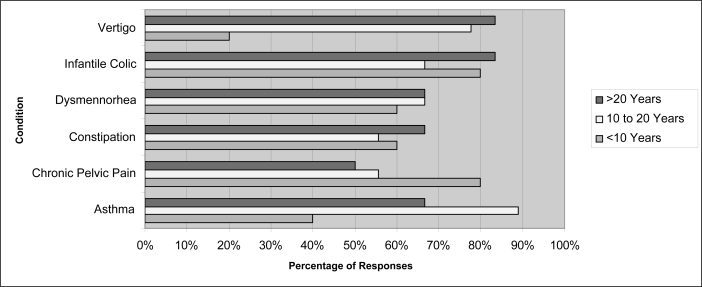
Figure 2 After analysis of the raw data, Figure 1 represents the conditions listed above that showed high favorable responses toward the benefit of chiropractic treatment. For the sake of simplicity, a positive response was considered whenever the chosen answer was either strongly agree or agree. The number of clinicians that indicated a positive response are depicted, divided into categories by number of years in practice (<10, 10–20 or >20).
Because the population surveyed was limited in size, the results were analyzed by percentage proportions only for the purposes of comparison; high percentages are not an indication of statistically significant responses (Table 3 and Figure 2).
Using the data from Table 3, Figure 2 graphically displays significant differences in opinion between the “years in practice” groups for conditions such as asthma, chronic pelvic pain and vertigo. Positive responses for treatment of asthma totaled 12 out of 15 clinicians who have been in practice longer than ten years, whereas only 2 out of 5 clinicians in the under 10 year bracket gave a positive response. This demonstrates a proportional difference of 40%. In the case of chronic pelvic pain, 4 out of 5 clinicians in the <10 year bracket had a positive response, compared to 5 out of 9 in the 10–20 bracket and 3 out of 6 in the >20 year bracket. Positive responses for vertigo showed the opposite; only 1 out of 5 in the <10 year bracket but 7 out of 9 (10–20) and 5 out of 6 (>20) in the other two brackets; a proportional difference of 58% and 63% respectively (Table 3 and Figure 2).
Similarly, conditions listed from Table 2 with a largely negative response (disagree and strongly disagree) were analyzed; however no clear trends or differences were seen in regards to years in practice.
Discussion
As demonstrated by this study, opinion on chiropractic treatment for certain non-musculoskeletal conditions differs greatly between individual CMCC clinicians with some congruence due to years in practice and condition. A fourth year intern may formulate their own opinion on chiropractic treatment of a non-musculoskeletal condition, or, depending on the clinicians they are assigned to during their clinical rotations, may be influenced by their clinician’s opinions and experiences. Some chiropractors, especially more recent graduates, shy away from treating non-musculoskeletal disorders and instead approach patient care from a musculoskeletal perspective only.
Initially the study attempted to correlate clinician ideology with the clinician’s attitude toward the appropriateness of treating of non-musculoskeletal conditions. However, as the sample size was very limited, the data collected was not sufficiently robust to draw any conclusions with respect to ideology. Perhaps not surprisingly, conditions that garnered greater than 50% or higher positive response with respect to appropriateness of chiropractic management are the conditions that generally have the most supportive retrievable research available for them. For the conditions where 50% or higher negative responses were ascertained, the opposite is generally demonstrated through a paucity of peer-reviewed evidence in the literature.
Further analysis of five conditions (asthma, chronic pelvic pain, vertigo, infantile colic, constipation) was done to observe any trends with respect to years in practice to see if opinions were related to clinical experience. Three conditions demonstrated clear differences between decades in practice: asthma, chronic pelvic pain, and vertigo. From these results, a percentage proportion was calculated. It was noted that asthma and vertigo showed the most significant difference within the stratification of years in practice. Specifically, a high proportion of CMCC clinicians with greater than 10 years experience indicated a favorable response toward the chiropractic treatment of both asthma and vertigo. Conversely, very few clinicians with less than 10 years experience concurred with their more experienced colleagues. Considering that the literature regarding the efficacy of chiropractic treatment for asthma is equivocal, it is possible that clinicians with less clinical experience rely more heavily on evidence-based literature thus accounting for their low favorable response rate. That said, since the research on vertigo is generally more favorable towards the effectiveness of manual therapies (see further discussion below), it was expected there would be a higher congruence amongst all three tiers of experience. Although more experienced clinicians (>20 years) did report their belief that chiropractic care was effect for vertigo (83% in favor), it is noteworthy that relatively few chiropractors with less than 10 years experience mirrored this sentiment (20%). Overall, asthma, chronic pelvic pain, constipation, dysmennorhea, infantile colic and vertigo showed the strongest positive clinician response for chiropractic treatment. Though research exists for each one of these conditions, the quality of the literature is varied and the strength is debatable.
Brontfort et al have recently published a systematic review of the literature on the effectiveness of manual therapies for a variety of musculoskeletal and non-musculoskeletal conditions. [17] In it, the authors stated that, overall, there is moderate quality evidence that spinal manipulation is effective for cervicogenic dizziness (short term), is not effective (similar to sham manipulation) for the treatment of asthma, infantile colic and primary dysmenorrhea, and inconclusive evidence exists regarding the effectiveness of manipulation for otitis media, hypertension, premenstrual syndrome. [17]
Asthma is one of the most common chronic diseases amongst children causing increased mucous production and airway hypersensitivity resulting in decreased air-flow. [18, 19] Chiropractic treatment has been thought to be beneficial in the treatment of this condition as it posited that it may modify the autonomic system and elicit viscerosomatic reactions to it. [18–20] Additionally, it has been hypothesized that misalignments at the levels of the upper C-spine create spinal reflexes that can induce asthma and correcting the misalignments could potentially alleviate the symptoms. [19, 21, 22] In addition, a more recent review by Kaminskyj et al [23] reported in their systematic review of the literature that chiropractic care should be used as an adjunct, not a replacement to traditional medical therapy. It is interesting to note that there exists a large positive response (70%) amongst CMCC clinicians with respect to this condition, even though the literature is extremely polar and generally equivocal (Table 2). This incongruence may suggest that clinicians consider their treatment to be beneficial for the musculoskeletal symptoms associated with asthma rather than the condition itself.
Chronic pelvic pain is described as non-cyclic pelvic pain persisting longer than three months and distinct from dysmenorrhea (a fairly common syndrome causing pain and disability in women). [24] The etiology is considered to be multi-factorial, attributed to anatomical, neurological, hormonal, musculoskeletal and psychosocial factors. [24] There has been very little research conducted on the effect of chiropractic care on chronic pelvic pain. One study by Hawk et al concluded that chronic pelvic pain is best treated using a multi-disciplinary approach including spinal manipulative therapy which showed positive short-term effects compared with sham adjustments. [24] This conclusion is supported by the data from this study as 60% of CMCC clinicians responded positively toward the benefit of chiropractic treatment for chronic pelvic pain (Table 2).
Constipation is a common condition amongst the young and the elderly. Difficulty and infrequency in the elimination of feces is often accompanied with pain, fear, and discomfort. [25] In a study conducted by Alcantara and Mayer on three pediatric patients, they found successful resolution of the condition after a regiment of spinal manipulative therapy by observing an increased frequency in bowel movements, with less straining and pain. [25] Similarly, a case study done on a 64 year old Caucasian female demonstrated a positive resolution to chronic constipation after ten treatments of spinal manipulative therapy. [26] While there is no extensive, high quality research on this issue, CMCC clinicians responded favorably (60%) toward the use of chiropractic treatment for constipation. This may be explained by personal experience as referenced by the above case studies.
Dysmenorrhea, painful menstrual cramps of uterine origin, is differentiated from chronic pelvic pain by its cyclic nature and is grouped into two categories, primary and secondary. [17] Primary dysmenorrhea is not associated with pelvic disease while secondary dysmenorrhea is associated with underlying pelvic pathology such as endometriosis. [17, 24] Hondras et al conducted a randomized, blinded clinical trial concluding that there was no significant difference between spinal manipulative therapy and sham treatment on the symptoms of primary dysmenorrheal. [27, 28] In a narrative review conducted by Spears, the author concluded that dysmenorrhea is best treated by a multi-modal approach including nutrition, chiropractic, medication and other alternative healthcare practices. [29] Sixty-five percent of the respondents in this study indicated a positive opinion; while this may not be reflected in research studies, clinicians may have approached this question with a multi-modal treatment plan in mind.
Infantile colic is an easily identified condition in infancy; however its etiology is relatively unknown. [30] Originally defined by Wessel et al infantile colic must meet three criteria: crying for three hours a day, for at least three days a week, for at least three weeks. [31] Many infants suffering from colic were observed to have cranial and spinal dysfunction as a result from a traumatic birth process and it has also been theorized that colic may be associated with gastrointestinal dysfunction. [32, 33] Some chiropractors opine that manipulative therapy could effectively treat infantile colic because misalignments in the spine may be inhibiting sympathetic output. Since an “adjustment” theoretically causes sympathetic stimulation which, based on physiology, in turn relaxes the smooth muscle of the gastrointestinal tract, reduces peristalsis, and inhibits bowel function, infantile colic could be effectively treated through manual therapy [32] A random controlled study conducted in Denmark showed a 67% reduction in daily crying with spinal manipulation, another study conducted in South Africa showed complete resolution of symptoms in 93% of infants in the manipulation group. [33] On the other hand, Olafsdottir et al conducted a blinded, randomized, and placebo controlled clinical trial on the effectiveness of chiropractic treatment on infantile colic and found it was no more effective than placebo. [34] Despite the extremes of opinion demonstrated by the research, 75% of CMCC clinicians responded favorably toward the chiropractic treatment of infantile colic. This may attributed to personal clinical experience and/or their choice of what research they have read.
Vertigo is a fairly common condition described as a false sensation of movement of self or the environment. [17] Underlying pathologies vary from trauma to infection in the inner ear, or pathological disorders such as vertebrobasilar insufficiency or central nervous system lesions. [17, 27] In some patients, the cause of the dizziness may not fall in the above categories, and it is suspected that the cause may originate from the cervical spine, termed cervicogenic dizziness. [35] Cervicogenic dizziness is defined as vertigo induced by changes in position of the neck or originating from the cervical region. [36]
A retrospective study conducted by Elster showed 100% positive response with either symptoms having improved or completely reversed within one to six months of care using a treatment plan of upper cervical adjustments. [37] In contrast, a review study conducted by Reid and Rivett cited a lack of randomized clinical trials and insufficient clinical research fails to prove the efficacy of manual therapy in treating vertigo. [36] Similarly, Bracher et al observed that a conservative treatment protocol including spinal manipulative therapy, soft tissue therapy, analgesic electrotherapy and exercise demonstrated a consistent improvement for patients experiencing cervicogenic vertigo. [37] However, they also concluded that further studies are needed to assess the treatment validity. [37] Considering that most of the research regarding this condition is positive for chiropractic treatment the results from this study (65%) concur with the literature (Table 2).
Limitations
This study had several limitations. The clinicians could have misinterpreted the questions regarding each condition to mean whether or not chiropractic care was effective in treating the condition itself or the musculoskeletal symptoms associated with them. For example, conditions such as asthma and chronic pelvic pain have been associated with higher incidences of thoracic and lower back pain respectively. [19, 24] Moreover, several clinicians did suggest that those individuals exhibiting any of the above listed conditions may have co-morbidities or dysfunction in their musculoskeletal systems, making chiropractic treatment both practical and beneficial. Although clarifications were made about the question to those who asked, it cannot be assumed that all respondents were accurate in their interpretation of each question in the survey. Future studies ought to take greater care in differentiating whether a respondent believes that chiropractic care can effectively manage a condition listed, the musculoskeletal effects associated with it or a combination of the two.
Including the option of “neutral” as a possible response was also open to respondent interpretation. Since the survey required an answer for each question, respondents may have chosen the answer “neutral” not because they genuinely had no positive or negative position on the matter, but rather because they were required to select an answer in order to continue with the survey. Furthermore, a neutral response could be translated as a mixed opinion; in that personal clinical experience has shown some positive and some negative responses in treating the above listed conditions, again not a “true” neutral response. It can also be argued that, by responding “agree,” “neutral” or “disagree,” a respondent does not have a strong opinion at all. That said, surveys such as the one used in this study conventionally collapse “strongly agree” and “agree together and “strongly disagree” and “disagree” together. In the future, this study may be replicated with the inclusion of an interview component that would clarify reasons for a neutral, “agree” or “disagree” response.
Finally, as this survey study was restricted to the 22 CMCC clinicians of the 2009–2010 academic school year, the sample size was very small, and not all clinicians participated. Had all clinicians responded, the response frequencies would have been different. Bearing in mind the above limitations of the study, the small sample size may have created a skew in the distribution of the results and the attitudes of CMCC clinicians towards the management of non-MSK conditions may not be representative of the attitudes of field practitioners in general.
Lastly, it might be interesting to conduct similar surveys of clinicians at other accredited chiropractic college and compare their attitudes towards the effectiveness of chiropractic care of non-MSK from those institutions to the ones discussed here.
Conclusion
Overall, there appears to be a positive response toward the chiropractic treatment of non-MSK conditions such as asthma, constipation, chronic pelvic pain, dysmenorrhea, infantile colic, and vertigo amongst CMCC clinicians. It was noted that, regardless of number of years in clinical practice, most opinions amongst CMCC clinicians were congruent with the exception of asthma and vertigo. However, a majority of the more experienced clinicians posited that chiropractic care would be of benefit to patients affected by these two conditions. Both conditions are fairly prevalent in the population and many patients with these conditions seek chiropractic care, not necessarily for the condition itself, but for related/associated MSK symptoms.
The unexpected result regarding vertigo indicates that research may not play as significant a role as predicted since clinicians with less than 10 years of clinical experience had a low positive response result compared to their more experienced colleagues despite the availability of literature indicating there is evidence of moderate strength supporting the use of chiropractic in treating this condition.
Future studies should be conducted to reveal any influences clinicians may have on their interns. Similarly, CMCC students in years one through three receive a variety of theoretical knowledge and opinions pertaining to the non-musculoskeletal conditions discussed. A study should be conducted to gather similar data to determine if there is any vertical integration/continuity between the theory taught in class in the undergraduate program, and the opinions formed by fourth year interns.
Appendix A.
Attitudes towards Non-Musculoskeletal Survey
This study is designed to determine the attitudes of the clinicians, specifically towards the chiropractic management of a set of non-musculoskeletal conditions. From the results of this study, we will discuss the influence of the clinicians on year 4 chiropractic students and how well that integrates with the first three years of study at the Canadian Memorial Chiropractic College.
Please indicate your year of graduation from an accredited chiropractic college An external file that holds a picture, illustration, etc.

Please indicate the number of years in practice
☐ 0–5
☐ 6–10
☐ 11–15
☐ 16–20
☐ 21–25
☐ 26–30
☐ >30Please indicate which philosophies you subscribe to and/or practice. Please check all that apply.
☐ Subluxation-based
☐ Pain-based
☐ Functional-based
☐ Structural-based
☐ Tonal-based
☐ Other (please specify) _______________________________Please indicate whether you think chiropractic is beneficial in treating the following conditions:
Strongly Agree Agree Neutral Disagree Strongly Disagree ADHD/Learning Disabilities Arrhythmias/ECG abnormalities Asthma Autism Bowel/Bladder Dysfunction Cerebral Palsy Chronic Obstructive Pulmonary Disorder Chronic Pelvic Pain Constipation Crohn’s Disease Depression Dysfunction of nursing Dysmenorrhoea/PMS Eczema/Psoriasis Hearing Loss/Tinnitus Hypertension Infantile Colic Infertility/Amenorrhea Multiple Sclerosis Nocturnal enuresis Otitis Media Parkinson’s Disease Pneumonia Seizures Ulcers Upper Respiratory Infection Urinary Tract Infection Vertigo Vision
OR: Open the Check List
Thank you for your participation in our survey.
References:
Keating JC, Jr, Cleveland CS, Menke M.
Chiropractic History: A Primer.
Association for the History of Chiropractic.
Davenport, Io.: 2004Montgomery PD, Nelson MJ.
Evolution of chiropractic theories of practice and spinal adjustment, 1900–1950.
Chiro Hist. 1985;5:71–77Ted J. Kaptchuk, OMD; David M. Eisenberg, MD
Chiropractic. Origins, Controversies and Contributions
Archives of Internal Medicine 1998 (Nov 9); 158 (20): 2215-2224Keating JC., Jr
Several pathways in the evolution of chiropractic manipulation.
J Manipulative Physio Ther. 2003;26(5):300–321Paget J.
Cases that bonesetters cure.
BMJ. 1867;1:1–4Meeker, W., & Haldeman, S. (2002).
Chiropractic: A Profession at the Crossroads of Mainstream and Alternative Medicine
Annals of Internal Medicine 2002 (Feb 5); 136 (3): 216–227Masarsky CS, Todres-Masarsky M. Churchhill Livingstone; USA:
Somatovisceral Aspects of Chiropractic: An Evidence-Based Approach, 2001Owens E.
Theoretical constructs of vertebral subluxation as applied to chiropractic practitioners and researchers.
T Clin Chiropr. 2000;7(1):74–79Cooperstein R, Gleberzon BJ.
Technique Systems in Chiropractic.
Churchill-Livingstone; 2004.
Full-Spine Specific (FSS) Technique (Meric Technique, Meric Recoil Technique) pp. 155–159Nelson, C., Lawrence, D., Triano, J., Bronfort, G., Perle, S., Metz, R. D., et al.
Chiropractic As Spine Care: A Model For The Profession
Chiropractic & Osteopathy 2005 (Jul 6); 13: 9Hawk C.
Should chiropractic be a wellness profession?
Top Clin Chiropr. 2000;7:23–26Hawk C.
When Worldviews Collide: Maintaining a Vitalistic Perspective in Chiropractic
in the Postmodern Era
Journal of Chiropractic Humanities 2005; 12 (1): 2-7 55-66Coopestein R, Gleberzon BJ.
Towards a taxonomy of subluxation-equivalents.
Top Clin Chiropr. 2000;8(1):49–60Vermet S, McGinnis K, Boodham M, Gleberzon BJ.
Degree of vertical integration between the undergraduate program and clinical internship with respect
to lumbopelvic diagnostic and therapeutic procedures at a chiropractic college.
J Chiro Ed. 2010;24(1):46–56Hawk C, Long CR, Boulanger KT.
Prevalence of Nonmusculoskeletal Complaints in Chiropractic Practice:
Report From a Practice-based Research Program
J Manipulative Physiol Ther 2001 (Mar); 24 (3): 157–169Cooperstein R, Gleberzon BJ.
Technique Systems in Chiropractic.
Churchill-Livingstone; 2004. Diversified TechniqueBronfort G, Haas M, Evans R, Leiniger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Balon JW, Mior SA.
Chiropractic care in asthma and allergy.
Ann Allergy Asthma Immunol. 2004;93(Suppl 1):S55–60Bronfort G.
Childhood and adolescent asthma: the scientific basis for chiropractic management.
European J Chiropr. 2002;49:8–12Balon J, et al.
A Comparison of Active and Simulated Chiropractic Manipulation as Adjunctive Treatment
for Childhood Asthma
New England Journal of Medicine 1998; 339(15): 1013-1020Bronfort G, Evans R, Kubic P, Filkin P.
Chronic Pediatric Asthma and Chiropractic Spinal Manipulation:
A Prospective Clinical Series and Randomized Clinical Pilot Study
J Manipulative Physiol Ther 2001 (July); 24 (6): 369–377Gibbs AL.
Chiropractic Co-management of Medically Treated Asthma
Clinical Chiropractic 2005 (Sep); 8 (3): 140–144Kaminskyj A, Frazier M, Johnstone K, Gleberzon BJ.
Chiropractic Care for Patients with Asthma: A Systematic Review of the Literature
J Can Chiropr Assoc. 2010 (Mar); 54 (1): 24–32Hawk C, Long C, Azad A.
Chiropractic care for women with chronic pelvic pain: a prospective single-group intervention study.
J Manipulative Physiol Ther. 1997;20(2):73–79Alcantara J, Mayer D.
The successful resolution of chronic constipation in three pediatric patients following chiropractic
spinal manipulative therapy.
European J Integrative Med. 2008;1:25–26Redly M.
The effects of chiropractic care on a patient with chronic constipation.
JCCA. 2001;45(3):185–191Ernst E.
Chiropractic manipulation for non-spinal pain – a systematic review.
NZMJ. 2003;116:1179Hondras MA, Long CR, Brennan PC.
Spinal manipulative therapy versus a low force mimic maneuver for women with primary dysmenorrheal:
a randomized, observer-blinded, clinical trial.
Pain. 1999;81:105–114Spears LG.
A narrative review of medical, chiropractic, and alternative health practices in the treatment
of primary dysmenorrhea.
J Chiropr Med. 2005;4(2):76–88Cohen-Silver J, Ratnapalan S.
Management of infantile colic: a review.
Clinical Pediatrics. 2009;48(1):14–17Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC.
Paroxysmal fussing infancy, sometimes called ‘colic’
Pediatrics. 1954;14:421–434Hipperson A.
Chiropractic Management of Infantile Colic
Clinical Chiropractic 2004 (Dec); 7 (4): 180–186Wiberg JMM.
Infantile colic: the scientific evidence for chiropractic management.
European J Chiropr. 2002;48:3–7Olafsdottir E, Forshei S, Fluge G, Markestad T:
Randomised Controlled Trial of Infantile Colic Treated With Chiropractic Spinal Manipulation
Archives of Disease in Childhood 2001 (Feb); 84 (2): 138–141Elster E.
Sixty Patients With Chronic Vertigo Undergoing Upper Cervical Chiropractic Care to Correct
Vertebral Subluxation: A Retrospective Analysis
J Vertebral Subluxation Research 2006 (Nov 8); 1–9Reid S, Rivett D.
Manual Therapy Treatment of Cervicogenic Dizziness: A Systematic Review
Man Ther. 2005 (Feb); 10 (1): 4–13Bracher ES, Almeida C, Almeida R, Duprat A, Bracher C.
A combined approach for the treatment of cervical vertigo.
J Manip Physiol Thera. 2000;23(2):96–100
Return to PEDIATRICS
Since 4-20-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |