

Headaches in Children: Part 1. The Changing
Phenotypes of Migraine Headache in
Infants, Children and AdolescentsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2022 (May); 20 (1): 1747–1756 ~ FULL TEXT
OPEN ACCESS Sue A. Weber DC, MSc, FEAC, FRCC
Private practitioner in Stockholm, Sweden
EAC Chairperson of special interest group (SIG) within Pediatrics
Educator internationally in chiropractic pediatrics

Headaches in children are common and the prevalence is increasing worldwide. The phenotype of migraine headache changes with continuing development of the nervous system. Children of all ages experience headaches but these are typically difficult to recognize and diagnose in the younger ages. Early intervention addressing the chemical, mechanical and psychological factors contributing to an individual’s headache is essential. This reduces the risk for central sensitization associated with chronicity and disability including reducing the risk for headache in adulthood.
Keywords: migraine headache, children, headache, periodic syndrome, abdominal migraine, cyclical vomiting, aura.
From the Full-Text Article:
Introduction
Headaches are a primary cause of disability worldwide and are highly disabling in adults and children [1]. Headaches occur commonly in children and can be a source of significant disability affecting activities of daily living and quality of life. Headaches occur in children of all ages and commonly progress into adulthood. Symptoms vary from infancy to adolescence and can be difficult to differentially diagnose in children delaying appropriate management. Early intervention can change the trajectory of headaches reducing chronicity and disability.
Incidence/Prevalence of Pediatric Headache
The prevalence of headaches in children is increasing worldwide [2] and they increase with age, particularly after the age of 5. [3] It is thought that the stress of starting school is related to this clear increase. [4] Frequent headache prevalence has increased significantly as well [5] and is accompanied by an earlier debut in children. [6] They are more prevalent among children in a lower socioeconomic class [7] with consequences of lower grades [8] and for some, lower educational achievement [9], a self-perpetuating negative spiral.
Chronic headaches negatively affect the quality of life of the child and their families. [10, 11] Looking at the trajectory of headaches, children with recurrent headaches are more likely to develop central sensitization and suffer from chronic headaches as adults. [4]
The diagnostic criteria for headache in children have been based on adult criteria for many years. The first edition of the international headache criteria was published in 1988. Since then, it has been updated in two versions and most recently, 30 years later, modified to better include children in the ICDH-3 beta version. [12] An expert group within pediatrics has evaluated these criteria and are in agreement that they lack sensitivity for children under 6 years of age. [13] Therefore, prevalence estimates in younger children and infants are likely under-estimated and under-reported increasing the risk for inadequate management [14-16] and central sensitization.
Co-Morbidities and Trajectories
The World Health Organization recognizes headaches as a common disorder of the nervous system. Headache sufferers commonly have other somatic complaints and emotional disturbances [17, 18] which change with increasing age. There is a high degree of co-morbidity with asthma, respiratory disorders, hay fever, frequent ear infections,18 depression and anxiety, [19] as well as other musculoskeletal pain syndromes [20] such as low back pain, neck and shoulder pain. [21, 22] There is co-relationship with physical inactivity; it acts as both a risk factor and a consequence of headaches. [2, 19, 23] There is a higher prevalence of headache in the population of obese children. [24]
Neuropsychiatric disorders occur commonly in childhood. [18] Emotional problems and behavioral disorders in preschool are over-represented in the headache population. Children often display features of hyperactivity, impulsivity, inattentiveness and have the diagnosis ADHD. [25]
Anxiety/depression and headache are bi-directional and present concurrently in children and adolescents. [19] Sleep disorders occur commonly in children with headache in all age groups [26] and both provoke and relieve headache. There is a relationship as well with the primary headache disorders and the regulation of sleep [27] involving vitamin D and neurotransmitters.
Diagnosis

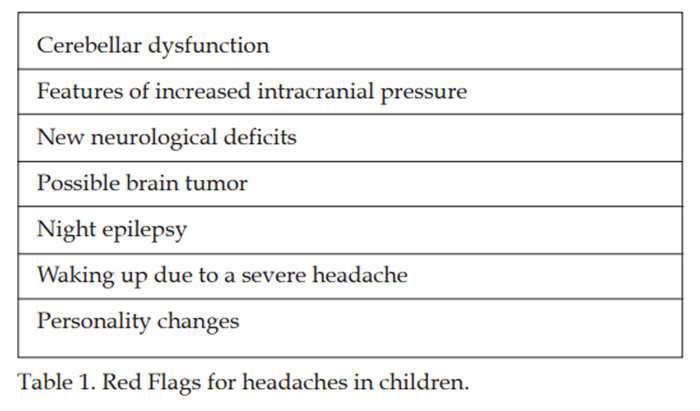
Table 1
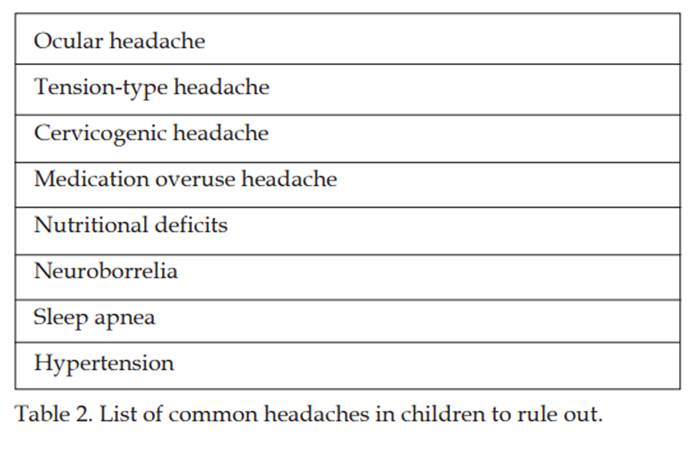
Table 2 The phenotype of headaches differs between adults and children due the differences in myelination and cerebral maturation. [28] The most common types of headaches seen in practice reflect the triad of health. The major headache categories involve chemical, psychological and mechanical factors which activate the trigeminovascular system resulting in a neuroinflammatory cascade causing and exacerbating headaches. One primary headache form is a result of a complex neurochemical, neurovascular disorder. [29] Another primary headache form has more of a psychological profile [25, 30] and a common secondary headache form is due to biomechanical dysfunction. [31] The threshold for headache decreases when more than one of these factors is present simultaneously.
Red flags that indicate neuroimaging for headaches should always be ruled out and are listed in Table 1. [32]
Secondary headaches that need to be ruled out are several (Table 2). This list is not meant to be exhaustive, more so, a list of common problems that show up in a non-medical practice. A more detailed description will follow in the next issue where tension-type headache and cervicogenic headache will also be described and compared.
Migraine Headaches
In adults, migraine headaches are a result of neuronal dysfunction with a critical imbalance between excitatory and inhibitory neurotransmission. There is a bioelectric phenomenon which activates the trigeminovascular system by releasing inflammatory neurotransmitters and causing vasodilation. There is a stimulation of C1-C3 nerve roots afferent as well as craniofacial afferents. Sensory overload and lowered energy reserve are thought to ignite the major pain signaling system of the brain, the trigeminovascular system. This abnormal cortical responsivity and sensory processing may constitute the fingerprint of the migraine brain. [33] More simply said, there is a dysfunction of the pain modulating system. This system is easily triggered by other inflammatory states, mechanical noxious input [31] and stress. [30]
Migraine headache has two major subgroups in adults according to the ICHD headache criteria. [16] Migraine headache without aura and migraine headache with aura. These headaches have a genetic predisposition. [34] Migraine without aura is a recurrent headache that in adults lasts from 2-72 hours. [35] It is a moderate to severe pulsating headache which is accompanied by nausea, vomiting, photo and/or phonophobia. The headache changes sides, it is aggravated by physical activity and is relieved by sleep. Once headaches become chronic the risk for central sensitization [36] and cutaneous allodynia increases. The extracranial pain sensitive structures include the skin, muscles, arteries, periosteum and joints, particularly of the head and neck. [13]
Migraine with aura is distinguished by the presence of transient, focal neurological symptoms that usually precede or accompany the migraine headache. [37] It is a reversible neurological disturbance affecting different senses, often vision, sensation and speech function. In children, these usually occur unilaterally, while adults experience them bilaterally. Visual disturbances, in the form of scintillating crescents [38] occur most often, followed by, a sensation of pins and needles migrating in the body, numbness and aphasia. [39] Metamorphopsia, micropsia and macropsia are other visual disturbances which alter how things appear, either changing shape, becoming smaller or bigger. [40] Some children also experience things changing colors. Olfactory and auditory hallucinations may also be experienced. [41]
Migraine headaches in children differ from those in adults in symptomatology, duration and location. Headache duration in young children can be from minutes to one hour, falling short of the required time listed in the ICDH guidelines. This is the most common reason why children do not fit into the present diagnostic guidelines. [13] Headaches regardless of type are classically bilateral, frontal or supraorbital in children. Syndromes occurring in children are not necessarily accompanied by headache pain, are common and recognized as an expression of migraine headache. [12] Migraine headaches may be accompanied by vegetative symptoms of pallor, nausea and vomiting. [28] Young children may exhibit behavior indicating they are light and noise sensitive. [42, 43] With increasing age, photo and phonophobia usually accompany a migraine headache. Children with migraine headache are more often home from school with other illnesses. There are different expressions of migraine, episodic syndromes, which occur during growth and development, with some continuing on into adulthood.
Age group headache presentations:Infant Headaches not uncommonly present already in infancy [44] and are diagnosed based on the history of a difficult, assisted or traumatic delivery and/or suboptimal positioning in-utero. [45] Clinical exam findings include behavioral and palpatory abnormalities. Post-delivery pictures can provide evidence of trauma or non-neutral positioning in-utero. The infants behave like they have a headache, holding their heads, scratching and pulling at the face and head. They are difficult to console and are not uncommonly diagnosed with infantile colic. Infants having had a complicated or prolonged delivery can have a headache due to the trauma. [46] Infants that suffer from pain due to a traumatic delivery are more likely to develop central sensitization [47] and go on to later develop migraine headaches. [48]
One of the mhe most common periodic syndrome associated with migraine is infantile colic. [49] Several studies have focused on a subgroup of irritable infants, describing them as having a periodic syndrome which later develops into a migraine headache without aura. [49-51] Gelfand discusses reasons why the baby cries and suggests that it may be due to having a headache, being overly sensitive to stimulus or perhaps having abdominal pain analogous to abdominal migraine. [51] A small study focusing on reducing sensory stimulus has shown effect in calming the irritable infant. [52] There appears to be a genetic component involved where mothers suffering from migraine have greater than double the risk of having a colicky baby. [51] The gut and the nervous system are derived from the same embryologic tissues. [53] The enteric nervous system and the central nervous system (CNS) are interconnected and strongly influence each other. [53] This bi-directional relationship, in predisposed individuals, is thought to be involved in the mechanism of a subgroup of infants with colic, and other gastrointestinal syndromes which appear during growth and development. [28] There seems to be an increased arousal in the CNS to triggers leading to a release of inflammatory neurochemicals resulting in gastrointestinal dysregulation. [28]
Long term studies on infants with colic reveal more often than expected, sleep disorders, temper tantrums, recurrent abdominal pain, allergic manifestations and aggressiveness. [54, 55] Romanello’s study showed that school age children presenting with a new onset of migraine headache have greater than a 6-fold increased prevalence of having had infantile colic. [56] Guidetti’s study from nearly 40 years ago showed that infants that were classified as hyper-reactive were more likely to suffer from migraine headache later in childhood. [42]
The other periodic syndromes which occur in order of age may exist by themselves or change into other episodic syndromes. Paroxysmal torticollis appears later in infancy, not following birth or traumatic delivery. During the first year of life the infant presents with torticollis which alternates sides. This disorder occurs periodically and regularly lasting from minutes to days resolving first in toddlerhood. This is the most uncommon periodic syndrome. Vegetative symptoms co-occur commonly with irritability, drowsiness, pallor, vomiting, ataxia, or tortipelvis. [57, 58]
Preschool to early school age Benign paroxysmal vertigo presents in the preschool period with recurrent episodes of dizziness, lasting frequently just a few minutes, but may extend to a few days. [59] The episode begins suddenly and may be accompanied by nystagmus, ataxia, nausea/vomiting or pallor, even headache. [60] The child often appears unsteady and may be frightened by the episode. This condition commonly resolves around the age of school start (5-6 years of age), but may continue on through childhood into young adulthood. Motion sickness is common as well. The risk for developing migraine headache was significantly greater among those who experienced vertigo for a longer time period. [61]
In the preschool years, some children experience recurring episodes of vegetative symptoms which negatively affect their ability to participate in activities. They suffer from pallor, nausea, anorexia, and less commonly, episodes of joint pain and fever. [5, 62]
A variety of sleep disturbances begin in preschool and can progress and change with age. Early on, apnea, [63] sleep disordered breathing and night terrors [64] may be expressions of migraine headache. Bedtime resistance with sleep anxiety, [42] bruxism, [65] sleep talking [66] and sleep walking [62] are also common.
Cyclical vomiting in childhood commonly starts around five years old and occurs regularly with bouts of frequent vomiting lasting up to several days. [67] This involves the enteric nervous system resulting in gastrointestinal dysregulation. [28] It is common with a family history of migraine.
Abdominal migraine is the most common periodic syndrome67 which begins around seven years of age. [69] It is commonly disabling, negatively affecting quality of life and participation in school and other activities. [70] There is an increased arousal in the CNS triggering a release of inflammatory neurochemicals resulting in gastrointestinal dysregulation. [28]
Aura often appears in school-age children but may occur at any age. [71]
Besides periodic syndromes, children and adults may experience premonitory symptoms prior to the onset of a migraine headache. These include: yawning, mood change, fatigue, neck stiffness, visual blurring and light headedness but exclude photophobia, phonophobia, osmophobia and nausea. [4] It is common with more than one symptom, but there does not seem to be any correlation with age.
Adolescence Migraine headache in adolescence is the most common severe recurrent headache. The disability of migraine headache in adolescence is significant resulting in school absences, difficulties concentrating, [1] and lower academic performance. [8] There is an increase in prevalence of migraine headache in boys in the childhood years. [71] The prevalence of headaches in boys’ levels off while the prevalence among females increases into young adulthood. During puberty there is a clear shift in gender predominance with girls much more commonly suffering from headaches. Headaches are commonly experienced in the temporal region and the duration of headaches increase with age. [48] The phenotype of headache is similar to that in adults presenting as a unilateral pulsating headache of moderate to severe intensity. Nausea, vomiting, photo and phonophobia are often concurrent. This headache may change sides and is relieved with sleep, with stress being a primary risk factor. [73]
Other more prevalent modifiable risk factors in this age group are lack of regular physical activity, smoking, alcohol, caffeine ingestion, obesity and abuse. [2, 10, 23] Being bullied creates an inflammatory process in the body and can contribute to the neurovascular and neurochemical insult affecting the frequency and intensity of headaches [73] as well as increasing the risk for obesity. [75] Obesity results in systemic inflammation which may be a possible trigger to the inflammatory cascade seen in headaches.
Among adolescents, headache, back pain and stomach pain coexist more commonly than each disorder existing by itself. [20] Neck pain is commonly associated with migraine in adolescents [76] as well as cranial autonomic symptoms such as runny nose and tearing of the eyes. [70] It is not uncommon for the juvenile migraine headache to remit, improve and change forms with increasing age. [77] But the frequency of chronic migraine headaches doubles in adolescence particularly among girls. [78] Most disturbing is that the risk for suicide is elevated in teens with chronic headaches. [79]
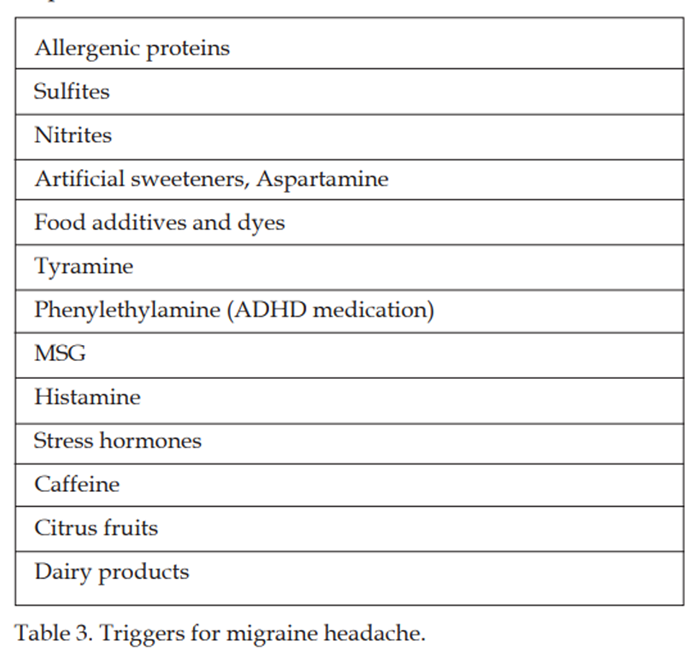
Triggers for migraine include light, sounds, odors, emotional, and/or endogenous factors. Individual triggers seem to have an additive effect, leading to an attack only when a threshold has been reached. This observation suggests that trigger factors act on common pathways provoking the neuroinflammatory cascade. [38]
Table 3
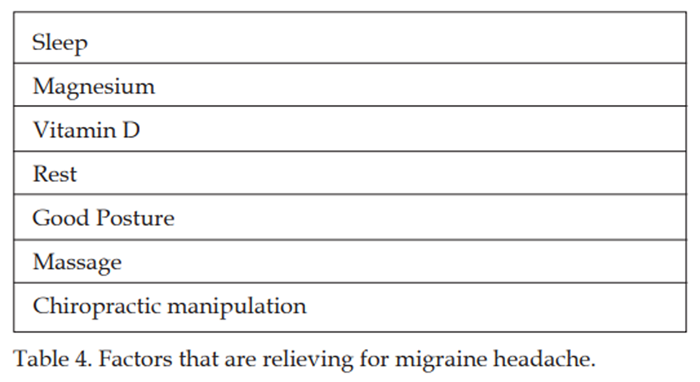
Table 4 The commonly described triggers in childhood and adolescence include impaired sleep, stress, skipping meals, physical overexertion, fatigue and bright flickering lights. [38] Later in adolescence, hormones, odors, anxiety and depression play a bigger role. [38]
There is a host of foods and chemicals which for some individuals can contribute to an ongoing inflammatory response listed below in Table 3. [80]
Factors that have been found to be relieving for migraine headaches are listed in Table 4. [81, 82]
Treatment: Manual therapy, Pharmaceuticals and Nutriceuticals
Despite the suffering and economic consequences, the majority of headache sufferers do not seek medical care. Manual therapy is the most common non-medical treatment requested by patients [83] and pediatric guidelines dictate manual therapy and other non-medical care as a first line intervention for children. [84] Appropriate early intervention is highly recommended to reduce the frequency and disability of headaches. [31, 85, 86]
Identifying and addressing mechanical, chemical and psychological triggers may reduce the disability and chronicity associated with migraine headache. For the inconsolable infant with a history of a traumatic delivery, mechanical dysfunction should be assessed and addressed. This reduces nociception from mechanoreceptors overloading the trigeminocervical nucleus.
Infants should be assessed for signs of allergy/intolerance and the status of the developing microbiome (antibiotic or pharmaceutical exposure, mother’s microbiome, immune status). [87] These factors may result in irritation or inflammation in the gut which may act to perpetuate the nociception in the enteric nervous system.
The clinician should note how well the parents have bonded with the infant. Depression during pregnancy and the postnatal period is associated with bonding impairment [88] which may be expressed by excessive crying in the infant.
The threshold for pain decreases with multiple contributing factors, highlighting the importance of recognizing and addressing triggers in the three primary areas (mechanical, chemical and psychological) mentioned. Proper treatment early on can reduce and interrupt the disability and chronicity associated with pain sensitization. [89]
Medication use for headaches is common in adolescence and is related to medication use in the family. [90] Regular medication use is associated with developing a medication overuse headache. [21] Education of teenagers is important to avoid this secondary headache by restricting medication to at most 2-3 times a week. [91]
Vitamin D deficiency is a global problem and highly over-represented in the headache population of both children and adults. [92] Vitamin D controls over 200 genes and has an important role in reducing inflammation. [93] D vitamin deficiency is directly coupled to headaches and musculoskeletal pain syndromes by propelling the body into an inflammatory state. [94] Vitamin D and magnesium are cofactors which when working together reduce an inflammatory state reducing pain and headaches. [95] Vitamin D also influences the release of neurotransmitters and neurochemicals directly involved in migraine headache pathology, anxiety and depression. [96, 97]
There are nutraceuticals which have been shown to be effective in treating migraine headache without associated adverse effects. Besides vitamin D, these include magnesium, L-tryptophan, niacin and vitamin B2. Another recommended combination is magnesium with partenium, andrographis paniculate and coenzyme Q10. [98] The current pediatric guidelines recommend non-medical alternative treatment for pediatric headache. [84] The role of diet is important before initiating long term pharmaceutical therapy. [98] Treatment with prophylactic and/or acute migraine with drugs is often unsatisfactory and counterproductive with a potential for toxicity. [99, 100]
The neuromusculoskeletal result of spinal dysfunction can initiate or perpetuate a migraine headache. Noxious input from the cervical spine can activate the trigeminovascular system resulting in a neuroinflammatory cascade [101, 102] potentiating the process occurring in a migraine headache. Chiropractic manipulation for children has been shown to be effective in reducing the disability of migraine headache. [103] The duration, intensity, frequency is reduced as well as medication use. [102, 104] The reactive tension in the cervical paraspinal and suboccipital muscles contribute as well to the ongoing pain cycle and is important to address in treatment. [81]
Management of headaches should be multimodal addressing the central and peripheral pain sensitization generators. [105] Manual therapy has been shown to be effective in reducing headaches in children and is an example of managing the peripheral pain generator, or the bottom-up strategy. [82] The top-down strategy, or addressing the central mechanism is needed with central sensitization, changing how the brain interprets afferent input. Different modalities may be used, but stress, sleep and exercise are the main top-down interventions used for the management of chronic pain. [106]
Besides skills in manual therapy, holistic management is important for success in treatment. This includes educating families in the area of sleep hygiene, stress management, regular mealtimes, adequate nutrition, sensitivities to certain foods and chemicals, regular physical activity and in appropriate cases, addressing the consequences of obesity.
Conclusion
Migraine headache is the most common headache in the pediatric population. The phenotype of this headache changes with age and development which can make it difficult to interpret. Recognizing it early, addressing the peripheral and central mechanisms which activate the headache are important in avoiding central sensitization and chronic headache. This headache is particularly sensitive to cervical spine dysfunction, chemical imbalance, and psychosocial stress. Addressing inflammatory states associated with vitamin D deficiency, obesity and abuse will be critical in management. Identifying and treating psychological and biomechanical stressors will reduce the frequency, intensity and medication use associated with this headache. Finally helping families to understand and avoid the specific triggers for their child will reduce the disability of this headache and improve the quality of for the family.
References:
Disease GBD;
Global, Regional, and National Incidence, Prevalence, and Years Lived With
Disability for 328 Diseases and Injuries for 195 Countries, 1990-2016:
A Systematic Analysis for the Global Burden of Disease Study 2016
Lancet. 2017 (Sep 16); 390 (10100): 1211–1259Nieswand V, Richter M, Gossrau G.
Epidemiology of Headache in Children and Adolescents-Another Type of Pandemia.
Curr Pain Headache Rep 2020;24(10):62.
doi: 10.1007/s11916-020-00892-6.Battistella PA, Fiumana E, Binelli M, Bertossi E, Battista P, Perakis E, Soriani S.
Primary headaches in preschool age children: clinical study and follow-up in 163 patients.
Cephalalgia 2006;26(2):162–171.42.
Barlow CF.
Migraine in the infant and toddler.
J Child Neurol 1994;9(1):92-4.
doi: 10.1177/088307389400900123.Sillanpää M, Saarinen MM.
Long term outcome of childhood onset headache: A prospective community study.
Cephalalgia 2018;38(6):1159-1166.
doi: 10.1177/0333102417727536.Straube A, Heinen F, Ebinger F, von Kries R.
Headache in school children: prevalence and risk factors.
Dtsch Arztebl Int 2013;110(48):811-818.
doi:10.3238/arztebl.2013.0811.Rothner AD.
Migraine Variants in Children.
Pediatr Ann 2018 ;47(2):e50-e54.
doi: 10.3928/19382359-20180126-02.Holstein BE, Andersen A, Denbaek AM, Johansen A, Michelsen SI, Due P.
Short communication: Persistent socio-economic inequality in
frequent headache among Danish adolescents from 1991 to 2014.
Eur J Pain 2018;22(5):935-940.
doi: 10.1002/ejp.1179.Grimby-Ekman A, Ĺberg M, Torén K, Brisman J, Hagberg M, Kim JL.
Pain could negatively affect school grades -
Swedish middle school students with low school grades most affected.
PLoS One. 2018;13(12):e0208435.
doi: 10.1371/journal.pone.0208435.Lampl C, Thomas H, Tassorelli C, Katsarava Z, et al.
Headache, depression and anxiety: associations in the Eurolight project.
J Headache Pain 2016;17:59.
doi: 10.1186/s10194-016-0649-2.Waldie KE, Thompson JM, Mia Y, Murphy R, Wall C, Mitchell EA.
Risk factors for migraine and tension-type headache in 11 year old children.
J Headache Pain 2014;15(1):60.
doi: 10.1186/1129-2377-15-60.van Suijlekom HA, Lamé I, Stomp-van den Berg SG, Kessels AG, Weber WE.
Quality of life of patients with cervicogenic headache:
a comparison with control subjects and patients with
migraine or tension-type headache.
Headache 2003;43(10):1034-41.
doi: 10.1046/j.1526-4610.2003.03204.x.Headache Classification Committee of the International Headache Society.
The International Classification of Headache Disorders, 3rd edition (beta version).
Cephalalgia 2013;33:629–808.Özge A, Faedda N, Abu-Arafeh I, et al.
Experts’ opinion about the primary headache diagnostic criteria
of the ICHD-3rd edition beta in children and adolescents.
J Headache Pain 2017;18(1):109.
doi: 10.1186/s10194-017-0818-y.Papetti L, Salfa I, Battan B, et al.
Features of Primary Chronic Headache in Children and Adolescents
and Validity of ICDHd 3 Criteria.
Front Neurol 2019;10:92. Published 2019 Feb
doi:10.3389/fneur.2019.00092.Raieli V, D’Amico A, Piro E.
Migraine in Children Under 7 Years of Age: a Review.
Curr Pain Headache Rep 2020;24(12):79.
doi: 10.1007/s11916-020-00912-5.Straube A, Andreou A.
Primary headaches during lifespan.
J Headache Pain 2019;20(1):35.
doi: 10.1186/s10194-019-0985-0.Lateef, Merikangas, Khoromi, Kalaydijan, Knigh, Nelson.
Headache in a national sample of American children: prevalence and comorbidity.
J Clincial Neurology 2009;24(5)536-43.Lateef T, He JP, Nelson K, Calkins ME, Gur R, Gur R, Merikangas KR.
Physical-Mental Comorbidity of Pediatric Migraine in
the Philadelphia Neurodevelopmental Cohort.
J Pediatr 2019;205:210-217.
doi: 10.1016/j.jpeds.2018.09.033.Bektas Ö, Ugur C, Gençtürk ZB, Aysev A, Sireli Ö, Deda G.
Relationship of childhood headaches with preferences in leisure time
activities, depression, anxiety and eating habits:
A population-based, cross-sectional study.
Cephalalgia 2015;35(6):527-37.
doi: 10.1177/0333102414547134.Swain MS, Henschke N, Kamper SJ, Gobina I, Ottová-Jordan V, Maher CG.
An international survey of pain in adolescents.
BMC Public Health 2014;14:447.
doi:10.1186/1471-2458-14-447.Hasseleid SN, Clench-Aas J, Raanaas RK, Lundqvist C.
The association between adolescent and parental use of non-prescription
analgesics for headache and other somatic pain - A cross-sectional study.
Scand J Pain 2017;16:114-121.
doi: 10.1016/j.sjpain.2017.04.069.Oksanen A, Pöyhönen T, Ylinen JJ, Metsähonkala L et al.
Force production and EMG activity of neck muscles in adolescent headache.
Disabil Rehabil 2008;30(3):231-9.
doi: 10.1080/09638280701265430.Torres-Ferrus M, Vila-Sala C, Quintana M, Ajanovic S, Gallardo VJ, et al.
Comorbidities and lifestyle in an adolescent population (The TEENs Study).
Cephalalgia 2019;39(1):91-99.
doi: 10.1177/0333102418777509.Han L.
Obesity Prevalence in Pediatric Headaches.
Korean Child Neurol Soc 2018;26(4):263-268.
doi.org/10.26815/jkcns.2018.26.4.263pISSN 1226-6884•eISSN 2383-897394.Salem H, Vivas D, Cao F, Kazimi IF, Teixeira AL, Zeni CP.
ADHD is associated with migraine: a systematic review and meta-analysis.
Eur Child Adolesc Psychiatry 2018;27(3):267-277.
doi: 10.1007/s00787-017-1045-4.Jacobs H, Gladstein
J. Pediatric headache: a clinical review.
Headache 2012;52:333–339.
doi: 10.1111/j.1526-4610.2011.02086.x.Rains JC, Poceta JS, Penzien DB.
Sleep and headaches.
Curr Neurol Neurosci Rep 2008;8(2):167-75.
doi: 10.1007/s11910-008-0027-9.Spiri D, Rinaldi VE, Titomanlio L.
Pediatric migraine and episodic syndromes that may be associated with migraine.
Ital J Pediatr 2014;40:92.Iftikhar W, Cheema FF, Khanal S, Khan QU.
Migrainous Infarction and Cortical Spreading Depression.
Discoveries (Craiova). 2020;8(3):e112.
doi: 10.15190/d.2020.9.Genizi J, Khourieh Matar A, Zelnik N, Schertz M, Srugo I.
Frequency of pediatric migraine with aura in a clinic-based sample.
Headache 2016;56(1):113-7.
doi: 10.1111/head.12741.Chaibi A, Saltyte Benth J, Tuchin PJ, Russell MB.
Chiropractic Spinal Manipulative Therapy for Migraine: A Study Protocol
of a Single-blinded Placebo-controlled Randomised Clinical Trial
BMJ Open. 2015 (Nov 19); 5 (11): e008095Tsze DS, Ochs JB, Gonzalez AE, Dayan PS.
Red flag findings in children with headaches: Prevalence
and association with emergency department neuroimaging.
Cephalalgia. 2019;39(2):185-196.
doi: 10.1177/0333102418781814.de Tommaso M, Vecchio E, Quitadamo SG, et al.
Pain-Related Brain Connectivity Changes in Migraine: A Narrative Review
and Proof of Concept about Possible Novel Treatments Interference.
Brain Sci 2021;11(2):234.
doi: 10.3390/brainsci11020234.Sutherland HG, Griffiths LR.
Genetics of Migraine: Insights into the Molecular Basis of Migraine Disorders.
Headache 2017;57(4):537-569.
doi: 10.1111/head.13053.Olesen J.
Headache Classification Committee of the International Headache Society
(IHS) the international classification of headache disorders.
Cephalalgia 2018;38(1):1 –211.Burstein R, Noseda R, Borsook D.
Migraine: Multiple processes, complex pathophysiology.
J. Neurosci 2015;35, 6619–6629.Youssef PE, Mack KJ.
Episodic and chronic migraine in children.
Dev Med Child Neurol 2020;62(1):34-41.
doi: 10.1111/dmcn.14338.Tarasco V, Grasso G, Versace A et al.
Epidemiological and clinical features of migraine
in the pediatric population of Northern Italy.
Cephalalgia 2016;36(6):510–517.Bigal ME, Lipton RB, Stewart WF.
The epidemiology and impact of migraine.
Curr Neurol Neurosci Rep 2004;4(2):98-104.
doi: 10.1007/s11910-004-0022-8.Ilik F, Ilik K.
Alice in Wonderland syndrome as aura of migraine.
Neurocase 2014;20(4):474-5.
doi: 10.1080/13554794.2013.826676.Agessi LM, Villa TR.
Vestibular Migraine with Visual Aura and Olfactory Hallucination in Children:
Two Case Reports.
Neuropediatrics 2018;49(6):414-416.
doi: 10.1055/s-0038-1673642.Guidetti V, Ottaviano S, Pagliarini M.
Childhood headache risk: warning signs and symptoms
present during the first six months of life.
Cephalalgia 1984;4(4):236-42.
doi: 10.1046/j.1468-2982.1984.0404237.x.Barlow CF.
Migraine in the infant and toddler.
J Child Neurol 1994;9(1):92-4.
doi: 10.1177/088307389400900123.Nachit-Ouinekh F, Chrysostome V, Henry P, Sourgen C, Dartigues JF, El Hasnaoui A.
Variability of reported headache symptoms and diagnosis
of migraine at 12 months.
Cephalalgia 2005;25:117–123.Marchand AM, Miller JE, Mitchell C.
Diagnosis and Chiropractic Treatment of Infant Headache
Based on Behavioral Presentation and Physical Findings:
A Retrospective Series of 13 Cases
J Manipulative Physiol Ther. 2009 (Oct); 32 (8): 682–686Taddio A, Katz J.
The effects of early pain experience in neonates
on pain responses in infancy and childhood.
Paediatr Drugs 2005;7(4):245-57.
doi: 10.2165/00148581-200507040-00004.Puretic MB, Demarin V.
Neuroplasticity mechanisms in the pathophysiology of chronic pain.
Acta Clin Croat 2012;51(3):425-9.Karsan N, Prabhakar P, Goadsby PJ.
Characterising the premonitory stage of migraine in children:
a clinic-based study of 100 patients in a specialist headache service.
J Headache Pain. 2016;17(1):94.
doi:10.1186/s10194-016-0689-7.Sillanpää M, Saarinen MM.
Infantile colic associated with childhood migraine:
A prospective cohort study.
Cephalalgia 2015;35(14)
DOI: 10.1177/0333102415576225.Gelfand AA, Thomas KC, Goadsby PJ.
Before the headache: infant colic as an early life expression of migraine.
Neurology 2012;79(13):1392-1396.
doi:10.1212/WNL.0b013e31826c1b7b.Gelfand AA.
Episodic Syndromes That May Be Associated With Migraine:
A.K.A. “the Childhood Periodic Syndromes”.
Headache. 2015;55(10):1358-1364.
doi:10.1111/head.12624.McKenzie S.
Troublesome crying in infants: effect of advice to reduce stimulation.
Archives of disease in childhood 1991;66:1416–20.Weydert JA, Ball TM, Davis MF.
Systematic review of treatments for recurrent abdominal pain.
Pediatrics. 2003;111:e1–e11.
doi: 10.1542/peds.111.1.e1.Rautava P, Lehtonen L, Helenius H, et al.
Infantile colic: Child and family three years later.
Pediatrics 1995;96: 43–47.Savino F, Castagno E, Bretto R, et al.
A prospective 10–year study on children who had severe infantile colic.
Acta Paediatr 2005; 94(Suppl): 129–132.Romanello S, Spiri D, Marcuzzi E, et al.
Association between childhood migraine and history of infantile colic.
JAMA 2013;309: 1607–1612.Hadjipanayis A, Efstathiou E, Neubauer D.
Benign paroxysmal torticollis of infancy: An underdiagnosed condition.
J Paediatr Child Health 2015;51(7):674-8.
doi: 10.1111/jpc.12841.Rosman NP, Douglass LM, Sharif UM, Paolini J.
The neurology of benign paroxysmal torticollis of infancy:
report of 10 new cases and review of the literature.
Journal of child neurology 2009; 24:155–60.Krams B, Echenne B, Leydet J, Rivier F, Roubertie A.
Benign paroxysmal vertigo of childhood: long-term outcome.
Cephalalgia: an international journal of headache 2011;31:439–43.Batu ED, Anlar B, Topcu M, Turanli G, Aysun S.
Vertigo in childhood: A retrospective series of 100 children.
European journal of paediatric neurology:
EJPN: official journal of the European Paediatric Neurology Society 2015; 19:226–32.Batuecas-Caletrio A, Martin-Sanchez V, Cordero-Civantos C, Guardado-Sanchez L, et al.
Is benign paroxysmal vertigo of childhood a migraine precursor?
European journal of paediatric neurology:
EJPN: official journal of the European Paediatric Neurology Society 2013;17:397–400.Arruda MA, Guidetti V, Galli F, Albuquerque RC, Bigal ME.
Childhood periodic syndromes: a population-based study.
Pediatr Neurol 2010;43(6):420-4.
doi:10.1016/ j.pediatrneurol. 2010.06.016.Bruni O, Miano S, Galli F, Verrillo E, Guidetti V.
Sleep apnea in childhood migraine.
J Headache Pain 2000;1(3):169-172.
doi:10.1007/s101940070039.Howell MJ.
Parasomnias: an updated review.
Neurotherapeutics 2012; 9(4):753–775.Bortoletto CC, Salgueiro MDCC, Valio R, et al.
The relationship between bruxism, sleep quality, and headaches in schoolchildren.
J Phys Ther Sci 2017;29(11):1889-1892.
doi: 10.1589/jpts.29.1889.Dosi C, Riccioni A, Della Corte M, Novelli L, Ferri R, Bruni O.
Comorbidities of sleep disorders in childhood and adolescence: focus on migraine.
Nat Sci Sleep 2013;5:77-85.Lee LY, Abbott L, Mahlangu B, Moodie SJ, Anderson S.
The management of cyclic vomiting syndrome: a systematic review.
European journal of gastroenterology & hepatology 2012; 24:1001–6.Tarantino S, Capuano A, Torriero R, Citti M, Vollono C, Gentile S, et al.
Migraine equivalents as part of migraine syndrome in childhood.
Pediatric neurology 2014; 51:645–9.Abu-Arafeh I, Russell G.
Prevalence and clinical features of abdominal migraine
compared with those of migraine headache.
Archives of disease in childhood 1995;72:413–7.Quek SH.
Recurrent abdominal pain in children: a clinical approach.
Singapore Med J 2015 Mar;56(3):125-8.
doi: 10.11622/smedj.2015038.Lewis DL.
Pediatric migraine.
Neurol Clin 2009;27(2):481–501.Russell MB, Rasmussen BK, Thorvaldsen P, Olesen J (1995)
Prevalence and sex-ratio of the subtypes of migraine.
Int J Epidemiol 24(3):612–618.Robberstad L, Dyb G, Hagen K, Stovner LJ, Holmen TL, Zwart JA:
An unfavorable lifestyle and recurrent headaches among adolescents: the HUNT study.
Neurology 2010;75: 712–7WF:
Psycho - pathology in children and adolescents with migraine
in clinical studies: a systematic review.
Pediatrics 2010; 126: 323–32.Gini G, Pozzoli T, Lenzi M, Vieno A.
Bullying victimization at school and headache: a meta-analysis of observational studies.
Headache 2014;54(6):976-86.
doi: 10.1111/head.12344.Takizawa R, Danese A, Maughan B, Arseneault L.
Bullying victimization in childhood predicts inflammation
and obesity at mid-life: a five-decade birth cohort study.
Psychol Med 2015;45(13):2705-15.
doi: 10.1017/S0033291715000653.Haytoglu Z, Herguner MO.
Cranial Autonomic Symptoms, Neck Pain: Challenges in Pediatric Migraine.
Ann Indian Acad Neurol 2019;22(3):282-285.
doi: 10.4103/aian.Kienbacher C, Wöber C, Zesch HE, et al.
Clinical features, classification and prognosis of migraine and tension-type
headache in children and adolescents: a long-term follow-up study.
Cephalalgia 2006;26: 820–30.McAbbee GN, Morse AM, Assadi M.
Pediatric aspects of headache classification in the international
classification of headache disorders—3 (ICHD-3 beta version).
Curr Pain Headache Rep 2016;20:7.Lin YK, Liang CS, Lee JT, Lee MS, Chu HT, Tsai CL, Lin GY, Ho TH, Yang FC.
Association of Suicide Risk With Headache Frequency
Among Migraine Patients With and Without Aura.
Front Neurol 2019;10:228.
doi: 10.3389/fneur.2019.00228.Millichap JG, Yee MM.
The diet factor in pediatric and adolescent migraine.
Pediatr Neurol 2003;28(1):9-15.
doi: 10.1016/s0887-8994(02)00466-6.Haque B, Rahman K, Hoque A, et al.
Precipitating and relieving factors of migraine versus tension type headache.
BMC Neurology 2012 ;12:82
http://www.biomedcentral.com/1471-2377/12/82.Lynge S, Dissing KB, Vach W, Christensen HW, Hestbaek L.
Effectiveness of Chiropractic Manipulation Versus Sham Manipulation
for Recurrent Headaches in Children Aged 7-14 Years -
A Randomised Clinical Trial
Chiropractic & Manual Therapies 2021 (Jan 7); 29: 1Moore CS, Sibbritt DW, Adams J.
A critical review of manual therapy use for headache disorders:
Prevalence, profiles, motivations, communication
and self-reported effectiveness.
BMC Neurol 2017;17- 61.Sarchielli P, Granella F, Prudenzano, M, Pini LA, Guidetti V, et al.
Italian guidelines for primary headaches: 2012 revised version.
J. Headache Pain 2012;13, S31–S70.GBD 2016 Headache Collaborators.
Global, Regional, and National Burden of Migraine and
Tension-type Headache, 1990-2016: A Systematic Analysis
for the Global Burden of Disease Study 2016
Lancet Neurol. 2018 (Nov); 17 (11): 954–976Gallelli L, Iannacchero R, De Caro E, Peltrone F, Colosimo M, De Sarro G.
A questionnaire-based study on prevalence and treatment
of headache in young children.
J Headache Pain 2005;6(4):277-80.
doi: 10.1007/s10194-005-0206-x.Loughman A, Quinn T, Nation ML, Reichelt A, Moore RJ, Van TTH, Sung V, Tang MLK.
Infant microbiota in colic: predictive associations with
problem crying and subsequent child behavior.
J Dev Orig Health Dis. 2021 Apr;12(2):260-270.
doi: 10.1017/S2040174420000227.Dubber S, Reck C, Müller M, Gawlik S.
Postpartum bonding: the role of perinatal depression,
anxiety and maternal-fetal bonding during pregnancy.
Arch Womens Ment Health 2015;18(2):187-195.
doi: 10.1007/s00737-014-0445-4.Charles JA, Peterlin BL, Rapoport AM, et al.
Favorable outcome of early treatment of new onset child and
adolescent migraine-implications for disease modification.
J. Headache Pain 2009;10, 227–233.Piazza F, Chiappedi M, Maffioletti E, Galli F, Balottin U.
Medication overuse headache in school-aged children: more common than expected?
Headache 2012;52(10):1506-10.
doi: 10.1111/j.1526-4610.2012.02221.x.El-Chammas, Keyes, Thompson, Viajayakumar.
Pharmalogical treatment of pediatric headaches: a meta-analysis.
JAMA Pediatrics 2013;1;167(3)250-8.Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al.
Prevalence of vitamin D deficiency in Africa:
a systematic review and meta-analysis.
Lancet Glob Health. 2020 Jan;8(1):e134-e142.
doi: 10.1016/S2214-109X(19)30457-7.Autier P, Boniol M, Pizot C, Mullie P.
Vitamin D status and ill health: A systematic review.
Lancet Diabetes Endocrinol 2014;2, 76–89.Gaikwad M, Vanlint S, Mittinity M, Moseley GL Stocks N.
Does vitamin D supplementation alleviate chronic nonspecific
musculoskeletal pain? A systematic review and meta-analysis.
Clin. Rheumatol 2017;36, 1201–1208.Uwitonze AM, Razzaque MS.
Role of Magnesium in Vitamin D Activation and Function.
J Am Osteopath Assoc 2018;118(3):181-189.
doi: 10.7556/jaoa.2018.037.Messlinger K, Lennerz JK, Eberhardt M, Fischer MJ.
CGRP and NO in the trigeminal system:
Mechanisms and role in headache generation.
Headache 2012;(52)1411–1427.Langdon 2017.
Pediatric Headache: An Overview.
Curr Probl Pediatr Adolesc Health Care 2017;47:44-65.Onofri A, Necozione S, Tozzi E.
Complementary and alternative medicine (CAM) in headache
of children and adolescents: open-label Italian study.
Clin Ter 2020;171(5):e393-e398.
doi: 10.7417/CT.2020.2246.Oskoui M, Pringsheim T, Billinghurst L, et al.
Practice guideline update summary: Pharmacologic treatment for pediatric
migraine prevention: Report of the Guideline Development,
Dissemination, and Implementation Subcommittee of
the American Academy of Neurology and the
American Headache Society.
Neurology 2019;93(11):500-509.
doi: 10.1212/WNL.0000000000008105.Slater SK, Powers SW, O’Brien HL.
Migraine in children: presentation, disability and response to treatment.
Curr Opin Pediatr 2018;30(6):775-779.
doi: 10.1097/MOP.0000000000000694.Bronfort G, Haas M, Evans R, Leiniger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Chaibi A, Benth JS, Tuchin P, et al.
Chiropractic Spinal Manipulative Therapy For Migraine: A Three-Armed,
Single-Blinded, Placebo, Randomized Controlled Trial
European Journal of Neurology 2017 (Jan); 24 (1): 143–153Chaibi A, Tuchin PJ, Russell MB.
Manual Therapies for Migraine: A Systematic Review
J Headache Pain. 2011 (Apr); 12 (2): 127–133Maduro De Camargo VM, Alburquerque-Sendin F, Berzin F, et al.
Immediate effects on electromyographic activity and pressure pain thresholds
after a cervical manipulation in mechanical neck pain:a randomized controlled trial.
J Manipulative Physiol Ther 2011;34:211–20.Falsiroli Maistrello L, Rafanelli M, Turolla A.
Manual Therapy and Quality of Life in People with Headache:
Systematic Review and Meta-analysis of Randomized Controlled Trials
Curr Pain Headache Rep 2019 (Aug 10); 23 (10): 78Daenen L, Varkey E, Kellmann M, Nijs J.
Exercise, not to exercise, or how to exercise in patients
with chronic pain? Applying science to practice.
Clin. J. Pain 2015;31, 108–114.
Return to PEDIATRICS
Return to MIGRAINE HEADACHE
Since 2-05-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |