

Headaches in Children: Part 2. The Changing
Phenotypes of Migraine Headache in
Infants, Children and AdolescentsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2021 (Nov); 20 (2): 1802–1813 ~ FULL TEXT
OPEN ACCESS Sue A. Weber DC, MSc, FEAC, FRCC
Private practitioner in Stockholm, Sweden
EAC Chairperson of special interest group (SIG) within Pediatrics
Educator internationally in chiropractic pediatrics

Headaches in children are common and the prevalence is increasing worldwide. The phenotypes of headaches change throughout growth and development making differential diagnosis a challenge. Children of all ages experience headaches but these can be difficult to recognize and diagnose particularly in the younger ages. Early intervention addressing the chemical, mechanical and psychological factors contributing to an individual’s headache is essential. This reduces the risk for central sensitization associated with chronicity and disability including the risk for headache in adulthood.
Keywords: ’Pediatric headache’, ’Tension-type headache children’, ’cervicogenic headache children’, ’migraine headache children’, ’new persistent daily headache children’, ADHD headache childhood’, ’headache vitamin D’, ’manual therapy headache childhood’, ’chiropractic headache’.
From the Full-Text Article:
Introduction
This is a second article in a series to help the clinician recognize and understand the most common headache types that present in children. The first article described how migraine headache can present through age and development from infancy to adolescence. [1] The second article reports on the wide variety of headache types that afflict children along with therapeutic treatments.
Headaches are a primary source of disability worldwide in both children and adults [2] and are one of the most common pain syndromes in childhood. [3] Children that suffer from headaches commonly have other somatic and emotional disturbances [4] which together significantly affect quality of life for the child and their family. [5, 6] Children with headaches are less socially and physically active, [7] and more often absent from school, [8] which negatively affects academic achievement and eventually socioeconomic status. [4]
Appropriate early intervention is recommended as it has been shown to decrease the frequency, disability and chronicity of headaches. [9–11]
Incidence/Prevalence of Pediatric Headache
Headache prevalence and the prevalence of frequent headaches in children is increasing worldwide. [12, 13] Headaches debut earlier now, [14] and for a long time, it has been known that the prevalence increases with age [15] peaking between 11 and 13 years. [16]
Co-Morbidities and trajectories
The World Health Organization recognizes headaches as a common disorder of the nervous system. A primary headache is one that is intrinsic to the nervous system [17] and not caused by a secondary problem. Headache sufferers commonly have other somatic complaints and emotional disturbances, [4, 18] which may change during growth and development. There is a high degree of co-morbidity with non-musculoskeletal and musculoskeletal disorders. [18, 19] These include asthma, respiratory disorders, hay fever, frequent ear infections, depression and anxiety, [20] low back pain, [21] along with neck and shoulder pain. [22]
There is co-relationship with physical inactivity; it acts as both a risk factor and a consequence of headaches. [13, 20, 23] There is a higher prevalence of headache in the population of obese children. [24]
Neuropsychiatric disorders commonly co-occur with headaches in childhood. [18] Emotional problems and behavioral disorders in pre-school are over-represented in the headache population. Children with headaches often display features of hyperactivity, impulsivity, inattentiveness and the complex diagnosis of ADHD with learning disabilities. [4, 25]
Anxiety/depression and headache are bidirectional and present concurrently in children and adolescents. [20] Sleep disorders have a complex relationship with headaches, co-occurring commonly in children of all ages. [26] There is a relationship as well with Vitamin D and neurotransmitters in primary headache disorders and the regulation of sleep. [27]
Diagnosis
The phenotypes of headaches differ between adults and children due the differences in myelination and cerebral maturation. [28] The most common types of headaches seen in practice reflect the triad of health. The major headache categories involve chemical, psychological and mechanical factors which activate the trigeminal nociceptive system resulting in a neuroinflammatory cascade causing and exacerbating headaches. The threshold for headache decreases when more than one provoking factor is present simultaneously. A primary headache is caused by dysfunction or overactivity of pain-sensitive structures in the head, and is not a symptom of an underlying disease. Migraine headaches, tension-type headaches and new persistent daily headaches are common examples of primary headaches in children. A secondary headache is a headache that is due to an underlying condition, such as a neck injury, concussion, an infection, or rarely, a serious underlying medical condition.
One primary headache form is a result of a complex neurochemical, neurovascular disorder. [29] Another primary headache form has more of a psychological profile [25, 30] and a common secondary headache form is due to biomechanical dysfunction involving the cervical spine. [9]
Migraine headaches and tension-type headaches are by far the most common types of primary headaches in children. [31] Migraine headaches are more common early on in childhood while tension-type headaches predominate in adolescence. Symptoms change and overlap significantly during growth and development which raises the question whether these are actually expressions of one disorder (the continuum model) [32–34] or if they are separate disorders as described by the ICHD II and III Beta criteria. [35, 36] Genizi’s (2016) results support the theory of the continuum model for migraine headache without aura and tension-type headache and differentiates these from those suffering from a mix of the two headaches concomitantly. [30] Other studies describe adolescents with headaches more often as highly motivated over-achievers. [37] (Migraine with aura appears to be a uniquely separate entity and this is supported by several studies). [38]
Migraine headache subtypes in children are described in more detail in part I of the headache series. [1] Migraine headache is a complex neuronal disorder resulting in a release of inflammatory neurotransmitters and vasodilation. [39] Migraine with aura is distinguished by the presence of transient, focal neurological symptoms that usually precede or accompany the migraine headache. [40] The aura is a reversible neurological disturbance affecting different senses, often vision, sensation and speech function. Visual disturbances, in the form of scintillating crescents occur most often, [41] followed by a sensation of pins and needles migrating in the body, numbness and aphasia. [42] In children, these usually occur unilaterally, while adults experience them bilaterally.
The phenotype of migraine headache changes with age and development. [1] It is associated with such significant morbidity that it has received the majority of attention in research on headaches. [3] Tension-type headache and cervicogenic headache are also common in children but generally less disabling. It is not unusual for a child to experience more than one headache type simultaneously, though when combined with a migraine headache, a more severe headache is experienced.
Tension-type headache (TTH) is a primary headache disorder which presents in childhood and becomes the most common primary headache in adolescence. Tension-type headache is considered to be coupled to psychosocial stress. [43] It is described as a mild to moderate headache in intensity and is experienced as a pressing headache with pericranial tenderness. [44] This is a recurrent headache which can be infrequent, frequent or chronic. A frequent headache is experienced 1–14 days per month while a chronic headache is experienced more often than 15 days a month. Bendtsen proposes a pathophysiological model for chronic TTH. [45] The peripheral nociceptive input drives central sensitization and once this loop is established, elimination of the peripheral nociception is not sufficient to interrupt the central sensitization. This results in increased pericranial muscle activity or release of neurotransmitters in the myofascial tissues. This is thought to be the mechanism responsible for the conversion of frequent TTH to chronic TTH. Jensen emphasizes that tension-type headache is a multifactorial disorder with several concurrent pathophysiological mechanisms, and that extracranial myofascial nociception may constitute only one of them. [46] Obesity, sleep disturbance, behavioral and psychiatric problems have all been linked with childhood TTH. There is an increase in frequency and disability of headaches as body mass increases. [47] Overweight and obesity lead to an inflammatory state in the body which acts to perpetuate the trigemino-inflammatory cascade.
Psychopathological symptoms also affect children with TTH particularly anxiety and depression. [48] Behavioral problems include concentration difficulties, hyperactivity, conduct disorders and poor emotional regulation. [49] Children with tension-type headache have been found to have significantly higher levels of somatic symptoms and family problems. [50] Family problems can cause insecure attachments which are related to cognitive affective regulation deficits and alexithemia. [51] Alexithemia is significantly more common among children with TTH. [52] This is described as having difficulty with verbal emotional expression, or difficulty identifying their feelings. Studies have not found a linear transmission of alexithemia between mother and child, but have found mood and anxiety disorders common in parents of children with headaches. [53] Children with TTH are generally more shy and less sociable having more behavioral, emotional and temperamental difficulties. [49]
TTH has been associated with antenatal maternal smoking, problem behavior at 3.5 years, higher body fat, and being bullied at 11 years. [5] Being bullied has been shown to result in an inflammatory process in the body which can perpetuate the trigemino-inflammatory cascade which hallmarks headaches. [54]
TTH lacks significant associated vegetative symptoms as seen in migraine headaches in children. TTH is less severe, and is not associated with the disability seen with migraine headache. Parents may not even be aware that the child is suffering from headache and therefore, do not seek care. [55] Due to issues with communication, it may be difficult to understand that younger children are having headaches.

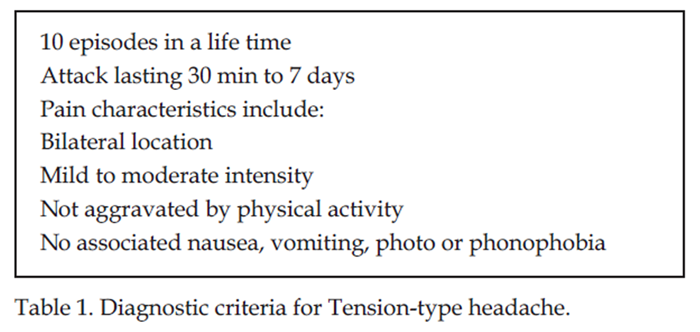
Table 1 The International Classification for Headache Disorders (ICDH-III) presents headache diagnostic criteria and pediatric experts agree that the most recent edition lacks sensitivity for headache types for the child under six years. [56] The diagnostic criteria have not been modified for TTH in children as they have been for migraine headache. The criteria for TTH are listed in Table 1.
Headache episodes in children are commonly shorter in duration than in the adult, but increase with age.
TTH presents equally among boys and girls in preadolescence [5] but with the onset of puberty the prevalence is higher among girls. Boys in preadolescence experienced more headache pain than girls did. [5] The higher HA prevalence among girls in adolescence is thought to be due to hormonal changes, [57] but the influence of hormones on tension-type headache is much less than in migraine headache. Gender differences in cognitive and social reactions to pain are considered to influence reporting of headaches. [58]
New persistent daily headache (NPDH) is a primary headache disorder whose signature is an abrupt onset of headache which persists daily for at least three months. It more commonly lasts for 10–12 months with a spontaneous resolution within 24 months. [59] Incidence is higher in children and adolescents than in adults [60] though it is uncommon in children under 10 years of age. [61] Strong’s 2021 study indicated this type of headache is more common among white females which raises the question of socioeconomics in health care in the United States. [62] Do other less advantaged groups of females have the same access for care? Onset of NPDH appears to be related to school start in the fall and the winter months with an identifiable specific trigger. [63] Pathogenesis is unknown but pro-inflammatory cytokines and cervicogenic dysfunction are thought to be involved. Two common triggers identified were stress related to an increase in school work, a minor head injury and an infection. [61] Studies are now identifying patients recovering from COVID-19 who are suffering from NPDH [64] which may influence the numbers of patients presenting with this type of headache. The pain is constant and lacks specific characteristics though it has some migrainous features making misdiagnosis common. It is difficult to treat and highly disabling, with conflicting results regarding pharmaceutical therapy. [65, 66] To date, no studies have been identified which evaluated the effect of spinal manipulation on this type of headache.
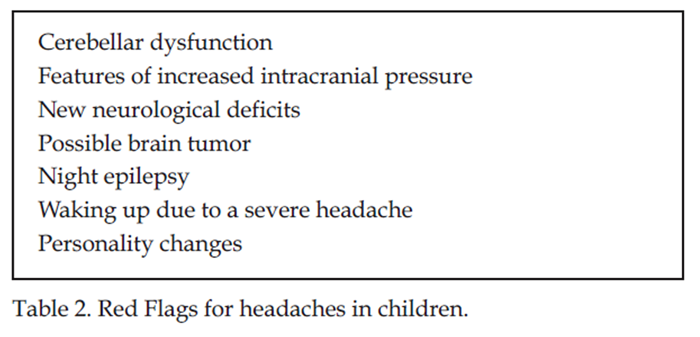
Table 2 The etiology of secondary pediatric headaches is multiple and when these are combined with other headache forms the clinical picture becomes complex. Contributing factors include but are not limited to infections, trauma, vascular disorders, substance use/withdrawal, psychiatric conditions, sleep disorders, family disharmony, stress and spinal dysfunction. [67] A minority of headaches (0.5–1%) are secondary to undiagnosed emergent intracranial abnormalities. [68] It is essential that the clinician seeing pediatric patients with headaches recognizes and refers out in a timely manner a child presenting with a malignant headache. These causes of secondary pediatric headache are seen in Table 2.
Ocular headaches are a common cause of headache which need to be assessed by a specialist. [69] These headaches usually present following prolonged ocular tasks. [70] Excessive use of digital media has resulted in a rise in adverse physical, psychological, social and psychoneurological health including impaired vision in children, obesity, poor stress regulation and poor sleep. [71] All of these factors influence the prevalence of headaches and need to be addressed for resolution.
Blood pressure measurement is an important part of the examination and can rule out high blood pressure as a cause of headache. In adolescents a blood pressure greater than 130/80 mm/Hg is considered hypertension. The prevalence of hypertension in adolescents is about six percent and nearly doubles in adolescents who are obese. [72] Adolescents presenting with high blood pressure should be screened for underlying medical disorders, particularly, diabetes, cardiovascular and kidney diseases. [72]
ADHD and primary headache disorders commonly co-occur, are significantly disabling impacting quality of life, impairing cognition, emotion and behavior. [73] The relationship between migraine and psychiatric disorders are bidirectional; one enhances the occurrence rate of other. [74] Some findings support the hypothesis which proposes that association between migraine and ADHD operates via hyperactive-impulse behavior pattern and sleep disturbances. [75] Uyar Cankay’s study further indicates a negative effect of a hypersensitized pain axis among individuals with severe headache on cognitive functions.
Medications for ADHD can result in high blood pressure, headaches and sleeping problems [76] highlighting the need for diligence during history and examination. Medication use for headaches is common in adolescence and is strongly influenced by parental use of analgesics. [19] Taking pain medication 10–15 times a month, for longer than three months can result in a medication overuse headache. [77] This is a new headache or a worsening of a pre-existing headache. [78] Pharmaceutical therapy lacks efficacy and evidence in children, and is associated with adverse effects. [79] Headache diaries are recommended to track information including medication use to help get a better understanding of the headache. [80]
Lyme neuroborreliosis is a tick-borne infectious disorder of the nervous system caused by Borrelia burgdorferi spirochetes. It is endemic in many areas and in children commonly causes a headache, Bell’s Palsy and or neck stiffness. [81] This is an important headache to rule out as it can progress to an irreversible neurological condition.
Nutritional deficits can commonly cause headaches. Recognition and resolution are critical in management and are considered first line of treatment for pediatric headaches. [82] Celiac disease in children is often undiagnosed, results in nutritional deficiencies and often presents with headache. [83, 84]
Vitamin D deficiency is a global problem and highly over-represented in the headache population of both children and adults. [85] It is a common cause of headache and musculoskeletal pain. Vitamin D controls over 200 genes and has an important role in reducing inflammation. [82] Vitamin D has several different functions in the body. Important functions include activating the immune system, maintaining brain and bone health [86] as well as controlling the neuromuscular system. [87] Magnesium is an essential cofactor for Vitamin D synthesis and normal levels are critical for Vitamin D utilization. [88] D vitamin deficiency is directly coupled to headaches and musculoskeletal pain syndromes by propelling the body into an inflammatory state. [89] Vitamin D and magnesium are cofactors which when working together reduce an inflammatory state decreasing pain and headaches. [88] Vitamin D also influences the release of neurotransmitters and neurochemicals directly involved in migraine headache pathology, anxiety and depression. [90, 91]
Sleep and headache have a complex and extensive interrelationship where both headache and sleep disorder may be manifestations of a same systemic dysfunction. [92] The interaction between sleep and headache is powerful and an elevated comorbidity between these two disorders is found in children. [93] There is a clear relationship between obstructive sleep apnea (OSA) and snoring and morning headache. [94] The assessment of children with headache should always include a thorough sleep history for the child. Successful treatment of headache in children and adolescents requires an integrated method of evaluation and management of both disorders. [93] Treatment of headache cannot be optimized without attention to sleep hygiene and sleep disorders. A sleep questionnaire should be part of every chronic headache evaluation. [95]
Cervicogenic headache (CEH) is a secondary headache characterized by unilateral headache and symptoms and signs of neck involvement. [35, 96–98] It is often worsened by neck movement, sustained awkward head position or external pressure over the upper cervical or occipital region on the symptomatic side. [96, 97] The pathogenesis of CEH may originate from various anatomic structures in the cervical spine. Convergence of afferents of the trigeminal and upper three cervical spinal nerves onto the second-order neurons in the trigemino-cervical nucleus in the upper cervical spinal cord is likely to lead to the headache. [99] The pathogenesis and etiology of CEH remain a challenge as different structures can be causative as opposed to a single entity. [100]
Due to significant phenotypic overlap, differentiating CEH from primary headache disorders such as migraine or tension-type headache, or other secondary headache disorders, can be clinically challenging. Cervicogenic headache commonly coexists with other headache types potentiating the headache making them less resistant to treatment.
Mechanical dysfunction of the cervical spine is one of the primary causes of recurrent neck pain and/or headaches causing a cervicogenic headache. [101–103] The findings in adults with cervicogenic headache include faulty head posture, cervical joint dysfunction (CJD), trigger points (TPs) in associated cervical paraspinal muscles, and reduction in cervical range of motion. [101, 104–109] Forward head posture is a deviation from normal leading to forward head carriage which acts to strain the upper cervical spine and can be a cause of neck pain and headache. [110–112] Children with recurring headache were found to have cervical joint dysfunction. [113] Trigger points or focal points of increased tension in a muscle, when present in the cervical spine, can also lead to neck pain and/or headaches. [114–121] Studies indicate that the upper cervical spine is the primary area of dysfunction in adults with cervicogenic headache. [101, 106, 107, 122–128]
These factors are not only a cause of neck pain and/or headache, but they can initiate or exacerbate both migraine headaches and tension-type headaches. [112, 114–116, 120, 121, 123–125] Cervicogenic headaches commonly become chronic. This is thought to be the result of the production of proinflammatory cytokines which contribute to neuronal sensitization resulting in chronic pain syndromes. [120, 129, 130]
Because the cervical spine influences all three headache types, its importance should not be underestimated. [115, 131, 132]
Treatment: Manual therapy, Pharmaceuticals and Nutraceuticals
Recurrent headaches result in significant suffering and economic consequences both for the health care system and the families affected. This is despite the fact that the vast majority of patients with headaches do not seek medical care. Manual therapy is the most common non-medical treatment requested by patients [133] and guidelines dictate non-medical care as a first line intervention for children. [134] Lynge’s is the first large scale randomized controlled trial evaluating the effect of spinal manipulation on headaches in children. The results indicated that children with headache had a reduction in headache frequency as well as a better global perceived effect than children who received validated sham manipulation. [135]
A holistic approach to treatment encompassing the associated factors and co-occurring conditions with headache is critical to success. It is equally important that this is addressed at an early stage to reduce the frequency, disability and chronicity of headaches. [10, 136]
Identifying and addressing the mechanical, chemical and psychological triggers that may reduce the disability and chronicity associated with the different headaches should begin in infancy. For the inconsolable infant with a history of a traumatic delivery, mechanical dysfunction should be assessed and addressed. This reduces nociception from mechanoreceptors overloading the trigeminocervical nucleus. For children, a detailed history of trauma which could have influenced the cervical spine is essential to understand the biomechanics contributing to headaches. Palpation by a chiropractor skilled in pediatrics would confirm these results or be the clue to revealing trauma which is no longer remembered.
Infants should be assessed for signs of allergy/intolerance and the status of the developing microbiome (antibiotic or pharmaceutical exposure, mother’s microbiome, immune status). [137] These factors affect the gut and act to perpetuate nociception in the enteric nervous system and for some cause a migraine headache. In the child, allergy or intolerance may present with stomach ache, delayed growth, with skin conditions, excessive mucous production, hematochizia, constipation and/or loose stools. [138]
Children who have social difficulties may experience stress and possibly be exposed to bullying. This would be optimal to address to reduce the inflammatory state associated with this.
Medication use for headaches is common in adolescence and is related to medication use in the family. [139] With regular medication use, developing a medication overuse headache is a risk. [19] Education of teenagers is important to avoid this secondary headache by restricting medication to at most 2–3 times a week. [78]
The current pediatric guidelines recommend non-medical alternative treatment for pediatric headache. [134] Treatment with prophylactic and/or acute migraine with drugs is often unsatisfactory and counterproductive with a potential for toxicity. [79, 140] The role of diet is important before initiating long term pharmaceutical therapy. [141] Working to achieve an optimal weight will reduce inflammation associated with overweight and obesity. There are nutraceuticals which have been shown to be effective in treating headache without associated adverse effects. Besides vitamin D and magnesium, these include L-tryptophan, niacin and vitamin B2. [142] Another recommended combination is magnesium with partenium, andrographis paniculate and coenzyme Q10. [141]
It is interesting that several studies have shown an association between headache occurrence and seasonality. [61, 143, 144] This occurrence has been attributed to the stress of starting school in the fall and winter, but it is possible there exists a correlation with vitamin D deficiency.
The neuromusculoskeletal result of spinal dysfunction can initiate or perpetuate a primary headache. Noxious input from the cervical spine can activate the trigeminovascular system resulting in a neuroinflammatory cascade [140, 145, 146] potentiating the process occurring in another headache. Appropriate treatment for age and development is effective in reducing the disability of headaches. [147] This includes instruction in normal posture, exercises to strengthen the spine and education in proper ergonomics. There was a decrease in duration, intensity, and frequency of headache as well as medication use with manual therapy including chiropractic manipulation. [146, 148] The reactive tension in the cervical paraspinal and suboccipital muscles also contribute to the ongoing pain cycle and is important to address in treatment. [149]
The threshold for pain decreases with multiple contributing factors, highlighting the importance of recognizing and addressing triggers in the three primary areas (mechanical, chemical and psychological) mentioned. Proper treatment early on can reduce and interrupt the disability and chronicity associated with pain sensitization. [150]
Management of headaches should be multimodal, addressing the central and peripheral pain sensitization generators. [151] Manual therapy in the form of chiropractic spinal manipulation has been shown to be effective in reducing headaches in children and is an example of managing the peripheral mechanism, or the bottom-up strategy. [135] The top-down strategy, or addressing the central mechanism is needed with central sensitization, changing how the brain interprets afferent input. Different modalities may be used, but stress, sleep and exercise are the main top-down interventions used for the management of chronic pain. [152]
Besides skills in manual therapy, holistic management is important for success in treatment. This includes educating families in the area of sleep hygiene, stress management, regular mealtimes, adequate nutrition, sensitivities to certain foods and chemicals, regular physical activity and in appropriate cases, along with addressing the consequences of obesity.
Conclusion
Headaches in children are complex and multifactorial. There are different headache types that children suffer from and it is not uncommon that these headache types both change during growth and development and co-occur, creating a disabling state. The changing phenotypes of headaches can make them difficult to interpret, particularly in young children. Recognizing headaches early as well as addressing the peripheral and central mechanisms which activate the headache are important in avoiding central sensitization and chronic headache. Inflammatory states potentiate the nociceptive trigeminovascular cascade particularly in cases of vitamin D deficiency, obesity and abuse, all of which will be critical in management. Identifying and treating psychological and mechanical stressors will reduce the frequency, intensity and medication use associated with headache. Finally, helping families to understand and avoid the specific triggers for their child will reduce the disability of headaches and improve the quality of life for the family.
References:
Weber S.
Headaches in Children: Part 1. The Changing Phenotypes of
Migraine Headache in Infants, Children and Adolescents
The Journal of Clinical Chiropractic Pediatrics 2021; 20 (1): 1747–1756Disease GBD;
Global, Regional, and National Incidence, Prevalence, and Years Lived With
Disability for 328 Diseases and Injuries for 195 Countries, 1990-2016:
A Systematic Analysis for the Global Burden of Disease Study 2016
Lancet. 2017 (Sep 16); 390 (10100): 1211–1259Hershey AD, Kabbouche MA, Powers SW.
Chronic daily headaches in children.
Curr Pain Headache Rep. 2006;10(5):370-6.
doi: 10.1007/s11916-006-0062-7. PMID: 16945254.Lateef TM, Merikangas KR, He J, Kalaydjian A, Khoromi S, Knight E, Nelson KB.
Headache in a national sample of American children:
prevalence and comorbidity.
J Child Neurol 2009;24(5):536-43.
doi: 10.1177/0883073808327831.Waldie KE, Thompson JM, Mia Y, Murphy R, Wall C, Mitchell EA.
Risk factors for migraine and tension-type headache in 11 year old children.
J Headache Pain 2014;15(1):60.
doi: 10.1186/1129-2377-15-60.van Suijlekom HA, Lamé I, Stomp-van den Berg SG, Kessels AG, Weber WE.
Quality of life of patients with cervicogenic headache:
a comparison with control subjects and patients with
migraine or tension-type headache.
Headache 2003;43(10):1034-41.
doi: 10.1046/j.1526-4610.2003.03204.x.Pogliani L, Spiri D, Penagini F, Nello FD, Duca P, Zuccotti GV.
Headache in children and adolescents aged 6-18 years in
northern Italy: prevalence and risk factors.
Eur J Paediatr Neurol. 2011 May;15(3):234-40.
doi: 10.1016/j.ejpn.2010.11.005.Anttila P, Metsähonkala L, Aromaa M, Sourander A, Salminen J.
Determinants of tension-type headache in children.
Cephalalgia. 2002 Jun;22(5):401-8.
doi: 10.1046/j.1468-2982.2002.00381.x.Chaibi A, Saltyte Benth J, Tuchin PJ, Russell MB.
Chiropractic Spinal Manipulative Therapy for Migraine: A Study Protocol
of a Single-blinded Placebo-controlled Randomised Clinical Trial
BMJ Open. 2015 (Nov 19); 5 (11): e008095Gallelli L, Iannacchero R, De Caro E, Peltrone F, Colosimo M, De Sarro G.
A questionnaire-based study on prevalence and treatment
of headache in young children.
J Headache Pain 2005;6(4):277-80.
doi: 10.1007/s10194-005-0206-x.GBD 2016 Headache Collaborators.
Global, Regional, and National Burden of Migraine and
Tension-type Headache, 1990-2016: A Systematic Analysis
for the Global Burden of Disease Study 2016
Lancet Neurol. 2018 (Nov); 17 (11): 954–976Singhi S, Jacobs H, Gladstein J.
Pediatric headache: where have we been and where do we need to be.
Headache 2014;54(5):817-29.
doi: 10.1111/head.12358.Nieswand V, Richter M, Gossrau G.
Epidemiology of Headache in Children and Adolescents-Another Type of Pandemia.
Curr Pain Headache Rep 2020;24(10):62.
doi: 10.1007/s11916-020-00892-6.Straube A, Heinen F, Ebinger F, von Kries R.
Headache in school children: prevalence and risk factors.
Dtsch Arztebl Int 2013;110(48):811-818.
doi:10.3238/arztebl.2013.0811.Battistella PA, Toldo I.
Headache and recurrent abdominal pains in preschool children.
J Headache Pain. 2006;7(5):322-3.
doi: 10.1007/s10194-006-0321-3.Fearon P, Hotopf M.
Relation between headache in childhood and physical and psychiatric
symptoms in adulthood: national birth cohort study.
BMJ. 2001 May 12;322(7295):1145.
doi: 10.1136/bmj.322.7295.1145.Dao JM, Qubty W.
Headache Diagnosis in Children and Adolescents.
Curr Pain Headache Rep. 2018 Feb 23;22(3):17.
doi: 10.1007/s11916-018-0675-7.Lateef T, He JP, Nelson K, Calkins ME, Gur R, Gur R, Merikangas KR.
Physical-Mental Comorbidity of Pediatric Migraine in
the Philadelphia Neurodevelopmental Cohort.
J Pediatr 2019;205:210-217.
doi: 10.1016/j.jpeds.2018.09.033.Hasseleid SN, Clench-Aas J, Raanaas RK, Lundqvist C.
The association between adolescent and parental use of non-prescription analgesics
for headache and other somatic pain - A cross-sectional study.
Scand J Pain 2017;16:114-121.
doi: 10.1016/j.sjpain.2017.04.069.Bektas Ö, Ugur C, Gençtürk ZB, Aysev A, Sireli Ö, Deda G.
Relationship of childhood headaches with preferences in leisure time
activities, depression, anxiety and eating habits:
A population-based, cross-sectional study.
Cephalalgia 2015;35(6):527-37.
doi: 10.1177/0333102414547134.Swain MS, Henschke N, Kamper SJ, Gobina I, Ottová-Jordan V, Maher CG.
An international survey of pain in adolescents.
BMC Public Health. 2014;14:447.
doi: 10.1186/1471-2458-14-447.Oksanen A, Pöyhönen T, Ylinen JJ, Metsähonkala L et al.
Force production and EMG activity of neck muscles in adolescent headache.
Disabil Rehabil 2008;30(3):231-9.
doi: 10.1080/09638280701265430.Torres-Ferrus M, Vila-Sala C, Quintana M, Ajanovic S, et al.
Headache, comorbidities and lifestyle in an adolescent population
(The TEENs Study).
Cephalalgia 2019;39(1):91-99.
doi: 10.1177/0333102418777509.Han L.
Obesity Prevalence in Pediatric Headaches.
Korean Child Neurol Soc 2018;26(4):263-268.
doi.org/10.26815/jkcns.2018.26.4.263 pISSN 1226-6884•eISSN 2383-897394.Salem H, Vivas D, Cao F, Kazimi IF, Teixeira AL, Zeni CP.
ADHD is associated with migraine:
a systematic review and meta-analysis.
Eur Child Adolesc Psychiatry. 2018;27(3):267-277.
doi: 10.1007/s00787-017-1045-4.Jacobs H, Gladstein J.
Pediatric headache: a clinical review.
Headache 2012;52:333–339.
doi: 10.1111/j.1526-4610.2011.02086.x.Rains JC, Poceta JS, Penzien DB.
Sleep and headaches.
Curr Neurol Neurosci Rep 2008;8(2):167-75.
doi: 10.1007/s11910-008-0027-9.Spiri D, Rinaldi VE, Titomanlio L.
Pediatric migraine and episodic syndromes that may be associated with migraine.
Ital J Pediatr 2014;40:92.Iftikhar W, Cheema FF, Khanal S, Khan QU.
Migrainous Infarction and Cortical Spreading Depression.
Discoveries (Craiova) 2020;8(3):e112.
doi: 10.15190/d.2020.9.Genizi J, Khourieh Matar A, Zelnik N, Schertz M, Srugo I.
Frequency of pediatric migraine with aura in a clinic-based sample.
Headache 2016;56(1):113-7.
doi: 10.1111/head.12741.Ozge A, Termine C, Antonaci F, Natriashvili S, Guidetti V, Wöber-Bingöl C.
Overview of diagnosis and management of paediatric headache.
Part I: diagnosis.
J Headache Pain. 2011;12(1):13-23.
doi: 10.1007/s10194-011-0297-5.Viswanathan V, Bridges SJ, Whitehouse W, Newton RW.
Childhood headaches: discrete entities or continuum?
Dev Med Child Neurol 1998;40(8):544-50.
doi: 10.1111/j.1469-8749.1998.tb15413.x.Wöber-Bingöl C, Wöber C, Karwautz A, Auterith A, et al.
Clinical features of migraine: a cross-sectional study
in patients aged three to sixty-nine.
Cephalalgia 2004;24(1):12-7.
doi: 10.1111/j.1468-2982.2004.00621.x.Turkdogan D, Cagirici S, Soylemez D, Sur H, et al.
Characteristic and overlapping features of migraine and tension-type headache.
Headache 2006;46(3):461-8.
doi: 10.1111/j.1526-4610.2006.00377.x.Headache Classification Subcommittee of the International Headache Society.
The International Classification of Headache Disorders: 2nd edition.
Cephalalgia 2004;24 Suppl 1:9-160.
doi: 10.1111/j.1468-2982.2003.00824.x.Headache Classification Committee of the International Headache Society.
The International Classification of Headache Disorders,
3rd edition (beta version).
Cephalalgia 2013;33:629–808.Borge AI, Nordhagen R.
Recurrent pain symptoms in children and parents.
Acta Paediatr 2000;89(12):1479-83.
doi: 10.1080/080352500456688.Burstein R, Noseda R, Borsook D.
Migraine: multiple processes, complex pathophysiology.
J Neurosci 2015;35(17):6619-29. doi: 10.1523/JNEUROSCI.0373-15.2015.de Tommaso M, Vecchio E, Quitadamo SG, Coppola G, et al.
Pain-Related Brain Connectivity Changes in Migraine: A Narrative Review
and Proof of Concept about Possible Novel Treatments Interference.
Brain Sci 2021;11(2):234.
doi: 10.3390/brainsci11020234.Youssef PE, Mack KJ.
Episodic and chronic migraine in children.
Dev Med Child Neurol 2020;62(1):34-41.
doi: 10.1111/dmcn.14338.Tarasco V, Grasso G, Versace A et al.
Epidemiological and clinical features of migraine in
the pediatric population of Northern Italy.
Cephalalgia 2016;36(6):510–517.Bigal ME, Lipton RB, Stewart WF.
The epidemiology and impact of migraine.
Curr Neurol Neurosci Rep 2004;4(2):98-104.
doi: 10.1007/s11910-004-0022-8.McAbbee GN, Morse AM, Assadi M.
Pediatric aspects of headache classification in the international
classification of headache disorders—3 (ICHD-3 beta version).
Curr Pain Headache Rep 2016;20:7.Soee AB, Skov L, Kreiner S, Tornoe B, Thomsen LL.
Pain sensitivity and pericranial tenderness in children
with tension-type headache: a controlled study.
J Pain Res 2013;6:425-34.
doi: 10.2147/JPR.S42869.Bendtsen L.
Central sensitization in tension-type headache--
possible pathophysiological mechanisms.
Cephalalgia. 2000 Jun;20(5):486-508.
doi: 10.1046/j.1468-2982.2000.00070.x.Jensen R.
Pathophysiological mechanisms of tension-type headache:
a review of epidemiological and experimental studies.
Cephalalgia. 1999 Jul;19(6):602-21.
doi: 10.1046/j.1468-2982.1999.019006602.x.Hershey AD, Powers SW, Nelson TD, Kabbouche MA et al.
American Headache Society Pediatric Adolescent Section.
Obesity in the pediatric headache population:
a multicenter study.
Headache 2009;49(2):170-7.
doi: 10.1111/j.1526-4610.2008.01232.x.Balottin U, Fusar Poli P, Termine C, Molteni S, Galli F.
Psychopathological symptoms in child and adolescent migraine
and tension-type headache: a meta-analysis.
Cephalalgia 2013;33(2):112-22.
doi: 10.1177/0333102412468386.Mazzone L, Vitiello B, Incorpora G, Mazzone D.
Behavioural and temperamental characteristics of children
and adolescents suffering from primary headache.
Cephalalgia 2006;26(2):194-201.
doi: 10.1111/j.1468-2982.2005.01015.x.Anttila P, Sourander A, Metsähonkala L, Aromaa M, Helenius H, Sillanpää M.
Psychiatric symptoms in children with primary headache.
J Am Acad Child Adolesc Psychiatry 2004;43(4):412-9.
doi: 10.1097/00004583-200404000-00007.Pedrosa Gil F, Scheidt CE, Hoeger D, Nickel M.
Relationship between attachment style, parental bonding
and alexithymia in adults with somatoform disorders.
Int J Psychiatry Med 2008;38(4):437-51.
doi: 10.2190/PM.38.4.d.Gatta M, Spitaleri C, Balottin U, Spoto A, Balottin L, Mangano S, Battistella PA.
Alexithymic characteristics in pediatric patients with primary headache:
a comparison between migraine and tension-type headache.
J Headache Pain. 2015;16:98.
doi: 10.1186/s10194-015-0572-y.Feldman JM, Ortega AN, Koinis-Mitchell D, Kuo AA, Canino G.
Child and family psychiatric and psychological factors associated
with child physical health problems: results from the Boricua youth study.
J Nerv Ment Dis. 2010 Apr;198(4):272-9.
doi: 10.1097/NMD.0b013e3181d61271. PMID: 20386256; PMCID: PMC2958697.Copeland WE, Wolke D, Lereya ST, Shanahan L, et al.
Childhood bullying involvement predicts low-grade
systemic inflammation into adulthood.
Proc Natl Acad Sci USA 2014;111(21):7570-5.
doi: 10.1073/pnas.1323641111.Weber Hellstenius SA (2009)
Recurrent Neck Pain and Headaches in Preadolescents Associated with
Mechanical Dysfunction he Cervical Spine: A Cross-Sectional
Observational Study With 131 Students
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 625—634Özge A, Faedda N, Abu-Arafeh I, et al.
Experts’ opinion about the primary headache diagnostic criteria
of the ICHD-3rd edition beta in children and adolescents.
J Headache Pain 2017;18(1):109.
doi: 10.1186/s10194-017-0818-y.Delaruelle Z, Ivanova TA, Khan S, Negro A, et al.
European Headache Federation School of Advanced Studies (EHF-SAS).
Male and female sex hormones in primary headaches.
J Headache Pain 2018;19(1):117.
doi: 10.1186/s10194-018-0922-7.Lynch AM, Kashikar-Zuck S, Goldschneider KR, Jones BA.
Sex and age differences in coping styles among children with chronic pain.
J Pain Symptom Manage 2007;33(2):208-16.
doi: 10.1016/j.jpainsymman.2006.07.014.Meineri P, Torre E, Rota E, Grasso E.
New daily persistent headache: clinical and
serological characteristics in a retrospective study.
Neurol Sci 2004;25 Suppl 3:S281-2.
doi: 10.1007/s10072-004-0310-8.Yamani N, Olesen J.
New daily persistent headache: a systematic review on an enigmatic disorder.
J Headache Pain 2019;20(1):80.
doi:10.1186/s10194-019-1022-z.Papetti L, Sforza G, Tarantino S, Moavero R, Ruscitto C, Ursitti F.
Features and Management of New Daily Persistent Headache
in Developmental-Age Patients.
Diagnostics (Basel) 2021;11(3):385.
doi: 10.3390/diagnostics11030385. PMID: 33668316.Strong E, Pierce EL, Langdon R, Strelzik J, McClintock W.
New Daily Persistent Headache in a Pediatric Population.
J Child Neurol 2021;36(10):888-893.
DOI: 10.1177/08830738211004514.Reidy BL, Riddle EJ, Powers SW, Slater SK, et al.
Clinic-based characterization of continuous headache in children and adolescents:
Comparing youth with chronic migraine to those with
new daily persistent headache.
Cephalalgia 2020;40(10):1063-1069.
DOI: 10.1177/0333102420920644.Liu JW, de Luca RD, Mello Neto HO, Barcellos I.
Post-COVID-19 Syndrome? New daily persistent headache
in the aftermath of COVID-19.
Arq Neuropsiquiatr. 2020;78(11):753-754.
doi: 10.1590/0004-282X20200187.Evans RW.
New daily persistent headache.
Headache 2012;52 Suppl 1:40-4.
doi: 10.1111/j.1526-4610.2012.02135.x.Baron EP, Rothner AD.
New daily persistent headache in children and adolescents.
Curr Neurol Neurosci Rep 2010;10(2):127-32.
doi: 10.1007/s11910-010-0097-3.Kelly M, Strelzik J, Langdon R, DiSabella M.
Pediatric headache: overview.
Curr Opin Pediatr 2018;30(6):748-754.
doi: 10.1097/MOP.0000000000000688.Tsze DS, Ochs JB, Gonzalez AE, Dayan PS.
Red flag findings in children with headaches: Prevalence
and association with emergency department neuroimaging.
Cephalalgia 2019;39(2):185-196.
doi: 10.1177/0333102418781814.Headache Classification Committee of the International Headache Society.
The International Classification of Headache Disorders,
3rd edition (beta version).
Cephalalgia 2013;33:629–808.Abdulrahman JA.
Pediatric Headache: Ocular Approach.
Med Surg Ophthal Res 2020; 2(5). MSOR.000550.2050.
DOI: 10.31031/MSOR.2020.02.000550.Lissak G.
Adverse physiological and psychological effects of screen time
on children and adolescents: Literature review and case study.
Environ Res 2018;164:149-157.
doi: 10.1016/j.envres.2018.01.015.Riley M, Hernandez AK, Kuznia AL.
High Blood Pressure in Children and Adolescents.
Am Fam Physician 2018;98(8):486-494.Parisi P, Verrotti A, Paolino MC, Ferretti A, Raucci U, Moavero R.
Headache and attention deficit and hyperactivity disorder in children:
common condition with complex relation and disabling consequences.
Epilepsy Behav 2014;32:72-5.
doi: 10.1016/j.yebeh.2013.12.028.Pompili M, Di Cosimo D, Innamorati M, Lester D, et al.
Psychiatric comorbidity in patients with chronic daily headache and migraine:
a selective overview including personality traits and suicide risk.
J Headache Pain 2009;10(4):283-90.
doi: 10.1007/s10194-009-0134-2.Uyar Cankay T, Besenek M.
Negative effects of accompanying psychiatric disturbances
on functionality among adolescents with chronic migraine.
BMC Neurol. 2021;21(1):97.
doi: 10.1186/s12883-021-02119-6.Konikowska K, Regulska-Ilow B, Rózanska D.
The influence of components of diet on the symptoms of ADHD in children.
Rocz Panstw Zakl Hig. 2012;63(2):127-34.Gelfand AA, Goadsby PJ.
Medication overuse in children and adolescents.
Curr Pain Headache Rep 2014;18(7):428.
doi: 10.1007/s11916-014-0428-1.El-Chammas K, Keyes J, Thompson N, Vijayakumar J, Becher D, Jackson JL.
Pharmacologic treatment of pediatric headaches: a meta-analysis.
JAMA Pediatr 2013;167(3):250-8.
doi: 10.1001/jamapediatrics.2013.508.Oskoui, Maryam et al.
Practice guideline update summary: Pharmacologic treatment for pediatric
migraine prevention: Report of the Guideline Development,
Dissemination, and Implementation Subcommittee of
the American Academy of Neurology and
the American Headache Society
Neurology 2019;93,11: 500-509.
doi:10.1212/WNL.0000000000008105.Larsson B, Fichtel Ĺ.
Headache prevalence and characteristics among school children
as assessed by prospective paper diary recordings.
J Headache Pain 2012;13(2):129-36.
doi: 10.1007/s10194-011-0410-9.Krawczuk K, Czupryna P, Pancewicz S, Oldak E, Król M, Moniuszko-Malinowska A.
Comparison of Neuroborreliosis Between Children and Adults.
Pediatr Infect Dis J 2020;39(1):7-11.
doi: 10.1097/INF.0000000000002493.Autier P, Boniol M, Pizot C, Mullie P.
Vitamin D status and ill health: a systematic review.
Lancet Diabetes Endocrinol 2014;2(1):76-89.
doi: 10.1016/S2213-8587(13)70165-7.Talarico V, Giancotti L, Mazza GA, Miniero R, Bertini M.
Iron Deficiency Anemia in Celiac Disease.
Nutrients 2021;13(5):1695.
doi: 10.3390/nu13051695.Jericho H, Sansotta N, Guandalini S.
Extraintestinal Manifestations of Celiac Disease:
Effectiveness of the Gluten-Free Diet.
J Pediatr Gastroenterol Nutr 2017;65(1):75-79.
doi: 10.1097/MPG.0000000000001420.Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al.
Prevalence of vitamin D deficiency in Africa:
a systematic review and meta-analysis.
Lancet Glob Health. 2020 Jan;8(1):e134-e142.
doi: 10.1016/S2214-109X(19)30457-7.Charoenngam N, Holick MF.
Immunologic Effects of Vitamin D on Human Health and Disease.
Nutrients 2020;12(7):2097.
doi: 10.3390/nu12072097.Mottaghi T, Askari G, Khorvash F, Maracy MR.
Effect of Vitamin D supplementation on symptoms and
C-reactive protein in migraine patients.
J Res Med Sci 2015;20(5):477-82.
doi: 10.4103/1735-1995.163971.Uwitonze AM, Razzaque MS.
Role of Magnesium in Vitamin D Activation and Function.
J Am Osteopath Assoc 2018;118(3):181-189.
doi: 10.7556/jaoa.2018.037.Gaikwad M, Vanlint S, Mittinity M, Moseley GL Stocks N.
Does vitamin D supplementation alleviate chronic nonspecific
musculoskeletal pain? A systematic review and meta-analysis.
Clin. Rheumatol 2017;36, 1201–1208.Messlinger K, Lennerz JK, Eberhardt M, Fischer MJ.
CGRP and NO in the trigeminal system:
mechanisms and role in headache generation.
Headache 2012;52(9):1411-27.
doi: 10.1111/j.1526-4610.2012.02212.x.Langdon R, DiSabella MT.
Pediatric Headache: An Overview.
Curr Probl Pediatr Adolesc Health Care 2017;47(3):44-65.
doi: 10.1016/j.cppeds.2017.01.002.Ferini-Strambi L, Galbiati A, Combi R.
Sleep disorder-related headaches.
Neurol Sci 2019;40(Suppl 1):107-113.
doi: 10.1007/s10072-019-03837-z.Dosi C, Figura M, Ferri R, Bruni O.
Sleep and Headache.
Semin Pediatr Neurol 2015;22(2):105-12.
doi: 10.1016/j.spen.2015.04.005.Stark CD, Stark RJ.
Sleep and chronic daily headache.
Curr Pain Headache Rep 2015;19(1):468.
doi: 10.1007/s11916-014-0468-6.Brennan KC, Charles A.
Sleep and headache.
Semin Neurol 2009;29(4):406-18.
doi: 10.1055/s-0029-1237113.Classification and diagnostic criteria for headache disorders,
cranial neuralgias and facial pain.
Headache Classification Committee of the International Headache Society.
Cephalalgia 1988;8 Suppl 7:1-96.Sjaastad O, Fredriksen TA, Pfaffenrath V.
Cervicogenic headache: diagnostic criteria.
The Cervicogenic Headache International Study Group.
Headache 1998;38(6):442-5.
doi: 10.1046/j.1526-4610.1998.3806442.x.Sjaastad O, Fredriksen TA, Pfaffenrath V.
Cervicogenic headache: diagnostic criteria.
Headache 1990;0(11):725-6.
doi: 10.1111/j.1526-4610.1990.hed3011725.x.Bogduk N.
The anatomical basis for cervicogenic headache.
J Manipulative Physiol Ther 1992;15(1):67-70.Chaibi A, Russell MB.
Manual Therapies for Cervicogenic Headache: A Systematic Review
J Headache Pain. 2012 (Jul); 13 (5): 351–359Sjaastad O.
The International Headache Society. A new multi-disciplinary forum.
Cephalalgia 1983;3(1):10.
doi: 10.1046/j.1468-2982.1983.0301010.x.Antonaci F, Fredriksen TA, Sjaastad O.
Cervicogenic headache: clinical presentation, diagnostic criteria,
and differential diagnosis.
Curr Pain Headache Rep 2001;5(4):387-92.
doi: 10.1007/s11916-001-0030-1. PMID: 11403744.Biondi DM.
Cervicogenic headache: diagnostic evaluation and treatment strategies.
Curr Pain Headache Rep 2001;5(4):361-8.
doi: 10.1007/s11916-001-0026-x. PMID: 11403740.Bogduk N.
The neck and headaches.
Neurol Clin 2004;22(1):151-71, vii.
doi: 10.1016/S0733-8619(03)00100-2.Biondi DM.
Cervicogenic headache: mechanisms, evaluation, and treatment strategies.
J Am Osteopath Assoc 2000;100(9 Suppl):S7-14.Grimshaw DN.
Cervicogenic headache: manual and manipulative therapies.
Curr Pain Headache Rep 2001;5(4):369-75.
doi: 10.1007/s11916-001-0027-9.Mitchell Haas, DC, Elyse Groupp, PhD, Mikel Aickin, PhD, Alisa Fairweather, MPH
Dose Response for Chiropractic Care of Chronic Cervicogenic Headache
and Associated Neck Pain: A Randomized Pilot Study
J Manipulative Physiol Ther 2004 (Nov); 27 (9): 547—553Haldeman S, Dagenais S.
Cervicogenic headaches: a critical review.
Spine J 2001;1(1):31-46.
doi: 10.1016/s1529-9430(01)00024-9. PMID: 14588366.Antonaci F, Bono G, Chimento P.
Diagnosing cervicogenic headache.
J Headache Pain 2006;7(3):145-8.
doi: 10.1007/s10194-006-0277-3.Watson DH, Trott PH.
Cervical Headache: An Investigation of Natural Head Posture
and Upper Cervical Flexor Muscle Performance
Cephalalgia 1993 (Aug); 13 (4): 272—284Kendall H, Kendall F, Boynton D.
Posture and Pain.
Florida: Robert Krieger Publishing Company, Inc; 1952.Fernández-de-las-Peńas C, Alonso-Blanco C, Cuadrado ML, Pareja JA.
Forward head posture and neck mobility in chronic tension-type headache:
a blinded, controlled study.
Cephalalgia. 2006 Mar;26(3):314-9.
doi: 10.1111/j.1468-2982.2005.01042.x.Weber Hellstenius SA (2009)
Recurrent Neck Pain and Headaches in Preadolescents Associated
with Mechanical Dysfunction of the Cervical Spine:
A Cross-Sectional Observational Study
with 131 Students
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 625—634Fernández-de-Las-Peńas C, Cuadrado ML, Pareja JA.
Myofascial trigger points, neck mobility and
forward head posture in unilateral migraine.
Cephalalgia 2006;26(9):1061-70.
doi: 10.1111/j.1468-2982.2006.01162.x.Jull G, Amiri M, Bullock-Saxton J, Darnell R, Lander C.
Cervical musculoskeletal impairment in frequent intermittent headache.
Part 1: Subjects with single headaches.
Cephalalgia 2007;27(7):793-802.
doi: 10.1111/j.1468-2982.2007.01345.x.Amiri M, Jull G, Bullock-Saxton J, Darnell R, Lander C.
Cervical musculoskeletal impairment in frequent intermittent headache.
Part 2: subjects with concurrent headache types.
Cephalalgia 2007;27(8):891-8.
doi: 10.1111/j.1468-2982.2007.01346.x.Kidd RF, Nelson R.
Musculoskeletal dysfunction of the neck in migraine and tension headache.
Headache 1993;33(10):566-9.
doi: 10.1111/j.1526-4610.1993.hed3310566.x.Fernández-de-las-Peńas C, Alonso-Blanco C, Miangolarra JC.
Myofascial trigger points in subjects presenting with
mechanical neck pain: a blinded, controlled study.
Man Ther 2007;12(1):29-33.
doi: 10.1016/j.math.2006.02.002.Jull G, Barrett C, Magee R, Ho P.
Further clinical clarification of the muscle dysfunction in cervical headache.
Cephalalgia 1999;19(3):179-85.
doi: 10.1046/j.1468-2982.1999.1903179.x.Shevel E, Spierings EH.
Cervical muscles in the pathogenesis of migraine headache.
J Headache Pain 2004;5(1):12-14.
doi:10.1007/s10194-004-0062-0.Bartsch T.
Migraine and the neck: new insights from basic data.
Curr Pain Headache Rep 2005;9(3):191-6.
doi: 10.1007/s11916-005-0061-0.Vernon H., Steiman I., Hagino C.
Cervicogenic Dysfunction in Muscle Contraction Headache
and Migraine: A Descriptive Study
J Manipulative Physiol Ther 1992 (Sep); 15 (7): 418—429Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV.
Spinal Manipulation vs. Amitriptyline for the Treatment of Chronic
Tension-type Headaches: A Randomized Clinical Trial
J Manipulative Physiol Ther 1995 (Mar); 18 (3): 148–154Bove G, Nilsson N.
Spinal Manipulation in the Treatment of Episodic
Tension-Type Headache: A Randomized Controlled Trial
JAMA 1998 (Nov 11); 280 (18): 1576-1579Tuchin PJ, Pollard H, Bonello R.
A Randomized Controlled Trial of Chiropractic
Spinal Manipulative Therapy for Migraine
J Manipulative Physiol Ther 2000 (Feb); 23 (2): 91–95Nilsson N..
A Randomized Controlled Trial of the Effect of Spinal
Manipulation in the Treatment of Cervicogenic Headache
J Manipulative Physiol Ther. 1995 (Sep); 18 (7): 435—440Zito G, Jull G, Story I.
Clinical tests of musculoskeletal dysfunction in the
diagnosis of cervicogenic headache.
Man Ther 2006;11(2):118-29.
doi: 10.1016/j.math.2005.04.007.
Epub 2005 Jul 18. PMID: 16027027.Hall T, Robinson K.
The flexion-rotation test and active cervical mobility--
a comparative measurement study in cervicogenic headache.
Man Ther 2004;9(4):197-202.
doi: 10.1016/j.math.2004.04.004.Martelletti P.
Inflammatory mechanisms in cervicogenic headache: an integrative view.
Curr Pain Headache Rep 2002;6(4):315-9.
doi: 10.1007/s11916-002-0053-2.Laimi K, Salminen JJ, Metsähonkala L, Vahlberg T, Mikkelsson M, Anttila P.
Characteristics of neck pain associated with adolescent headache.
Cephalalgia 2007;27(11):1244-54.
doi: 10.1111/j.1468-2982.2007.01439.x.Kidd RF, Nelson R.
Musculoskeletal dysfunction of the neck in migraine and tension headache.
Headache 1993;33(10):566-9.
doi: 10.1111/j.1526-4610.1993.hed3310566.x.Leone M, D’Amico D, Grazzi L, Attanasio A, Bussone G.
Cervicogenic headache: a critical review of the current diagnostic criteria.
Pain 1998;78(1):1-5.
doi: 10.1016/S0304-3959(98)00116-X.Moore CS, Sibbritt DW, Adams J.
A critical review of manual therapy use for headache disorders:
prevalence, profiles, motivations, communication
and self-reported effectiveness.
BMC Neurol 2017;17(1):61.
doi: 10.1186/s12883-017-0835-0.Sarchielli P, Granella F, Prudenzano MP, Pini LA, et al.
Italian guidelines for primary headaches: 2012 revised version.
J Headache Pain 2012;13 Suppl 2(Suppl 2):S31-70.
doi: 10.1007/s10194-012-0437-6.Lynge S, Dissing KB, Vach W, Christensen HW, Hestbaek L.
Effectiveness of Chiropractic Manipulation Versus Sham Manipulation
for Recurrent Headaches in Children Aged 7-14 Years -
A Randomised Clinical Trial
Chiropractic & Manual Therapies 2021 (Jan 7); 29: 1Global Burden of Disease Headache Collaborators
Global, Regional, and National Burden of Migraine and Tension-type Headache,
1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016
Lancet Neurol. 2018 (Nov); 17 (11): 954–976Loughman A, Quinn T, Nation ML, Reichelt A, et al.
Infant microbiota in colic: predictive associations with
problem crying and subsequent child behavior.
J Dev Orig Health Dis 2021;12(2):260-270.
doi: 10.1017/S2040174420000227.Miceli Sopo S, Arena R, Greco M, Bergamini M, Monaco S.
Constipation and cow’s milk allergy: a review of the literature.
Int Arch Allergy Immunol 2014;164(1):40-5.
doi: 10.1159/000362365.Piazza F; Chiappedi M, Maffioletti E; Galli F; et al.
A clinical study on medication overuse headache in childhood and adolescence.
The Journal of Headache and Pain 2013 14(Suppl 1):P27.Slater SK, Powers SW, O’Brien HL.
Migraine in children: presentation, disability and response to treatment.
Curr Opin Pediatr 2018;30(6):775-779.
doi: 10.1097/MOP.0000000000000694.Onofri A, Necozione S, Tozzi E.
Complementary and alternative medicine (CAM) in headache
of children and adolescents: open-label Italian study.
Clin Ter 2020;171(5):e393-e398.
doi: 10.7417/CT.2020.2246.Yamanaka G, Suzuki S, Takeshita M, Go S, et al.
Effectiveness of low-dose riboflavin as a prophylactic agent
in pediatric migraine.
Brain Dev 2020;42(7):523-528.
doi: 10.1016/j.braindev.2020.04.002.Pakalnis A, Heyer GL.
Seasonal Variation in Emergency Department Visits
Among Pediatric Headache Patients.
Headache. 2016 Sep;56(8):1344-7.
doi: 10.1111/head.12888.Kedia S, Ginde AA, Grubenhoff JA, Kempe A, Hershey AD, Powers SW.
Monthly variation of United States pediatric headache
emergency department visits.
Cephalalgia. 2014 May;34(6):473-8.
doi: 10.1177/0333102413515346.Bronfort G, Haas M, Evans R, Leininger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Chaibi A, Benth JS, Tuchin P, et al.
Chiropractic Spinal Manipulative Therapy For Migraine: A Three-Armed,
Single-Blinded, Placebo, Randomized Controlled Trial
European Journal of Neurology 2017 (Jan); 24 (1): 143–153Chaibi A, Tuchin PJ, Russell MB.
Manual Therapies for Migraine: A Systematic Review
J Headache Pain. 2011 (Apr); 12 (2): 127–133Maduro De Camargo VM, Alburquerque-Sendin F, Berzin F, et al.
Immediate effects on electromyographic activity and pressure pain
thresholds after a cervical manipulation in mechanical neck pain:
a randomized controlled trial.
J Manipulative Physiol Ther 2011;34:211–20.Haque B, Rahman K, Hoque A, et al.
Precipitating and relieving factors of migraine versus tension type headache.
BMC Neurology 2012;12:82.Charles JA, Peterlin BL, Rapoport AM, et al.
Favorable outcome of early treatment of new onset child and
adolescent migraine-implications for disease modification.
J. Headache Pain 2009;10, 227–233.Falsiroli Maistrello L, Rafanelli M, Turolla A.
Manual Therapy and Quality of Life in People with Headache:
Systematic Review and Meta-analysis of Randomized Controlled Trials
Curr Pain Headache Rep 2019 (Aug 10); 23 (10): 78Daenen L, Varkey E, Kellmann M, Nijs J.
Exercise, not to exercise, or how to exercise in patients
with chronic pain? Applying science to practice.
Clin J Pain 2015;31(2):108-14.
doi: 10.1097/AJP.0000000000000099.
Return to PEDIATRICS
Return to MIGRAINE HEADACHE
Since 2-05-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |