

Factors Associated with Early Magnetic Resonance
Imaging Utilization for Acute Occupational Low
Back Pain: A Population-based Study From
Washington State Workers' CompensationThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine (Phila Pa 1976) 2012 (Sep 1); 37 (19): 1708–1718 ~ FULL TEXT
OPEN ACCESS Janessa M. Graves, MPH, PhD, Deborah Fulton-Kehoe, PhD, MPH, Diane P. Martin, MA, PhD,
Jeffrey G. Jarvik, MD, MPH, and Gary M. Franklin, MD, MPH
Harborview Injury Prevention and Research Center,
Department of Pediatrics, School of Medicine,
University of Washington,
Seattle, WA 98104, USA.
FROM: Am Fam Physician 2012Study design: A population-based, prospective cohort study.
Objective: To identify demographic, job-related, psychosocial, and clinical factors associated with the use of magnetic resonance imaging (MRI) within 6 weeks from injury (early MRI) among workers' compensation claimants with acute occupational low back pain (LBP).
Summary of background data: Early MRI may be associated with increased use of services for treatment and costs. To understand utilization and most appropriately apply guidelines, it is important to identify factors associated with early imaging use for occupational LBP.
Methods: Workers (N = 1830) were interviewed 3 weeks (median) after submitting a workers' compensation claim for a back injury. Demographic, work, health, clinical, and injury characteristics were ascertained from interviews, medical records, and administrative data. Modified Poisson regression analyses identified factors associated with early MRI use.
Results: Among respondents, 362 (19.8%) received an early MRI. Multivariable regression showed that male workers were 43% more likely to receive an early MRI than female workers (incident rate ratio [IRR]: 1.43, 95% confidence interval [CI]: 1.12-1.82). Initial visit type with a surgeon was associated with 78% greater likelihood of receiving an early MRI than that with a primary care physician (IRR: 1.78, 95% CI: 1.08-2.92). Having a chiropractor as the initial provider was associated with a reduced likelihood of early MRI (IRR: 0.53, 95% CI: 0.42-0.66). Workers with elevated work fear-avoidance, higher Roland scores, or increased injury severity were more likely to receive early MRI than counterparts with lower levels or scores.
Conclusion: Nearly 20% of the injured workers with LBP receive early MRI, a rate similar to that reported elsewhere. Early MRI may lead to greater subsequent interventions, potentially poorer outcomes, and increased health care expenditures. On the basis of the characteristics of patients with uncomplicated occupational LBP, providers may be able to provide tailored care, and providers and policy makers may better understand the utilization of imaging and adherence to clinical guidelines.
Keywords: low back pain, workers’ compensation, diagnostic imaging, early imaging, clinical practice guidelines, MRI, population-based
From the FULL TEXT Article:
Background
Approximately one-quarter of working adults are affected by low back pain (LBP) during their career and 10% to 20% with a work-related low back injury do not return to work. [1–3] Occupational LBP accounts for approximately 30% of the workers’ compensation (WC) claims, and these claims constitute a disproportionately higher percentage of total WC costs. [4, 5]
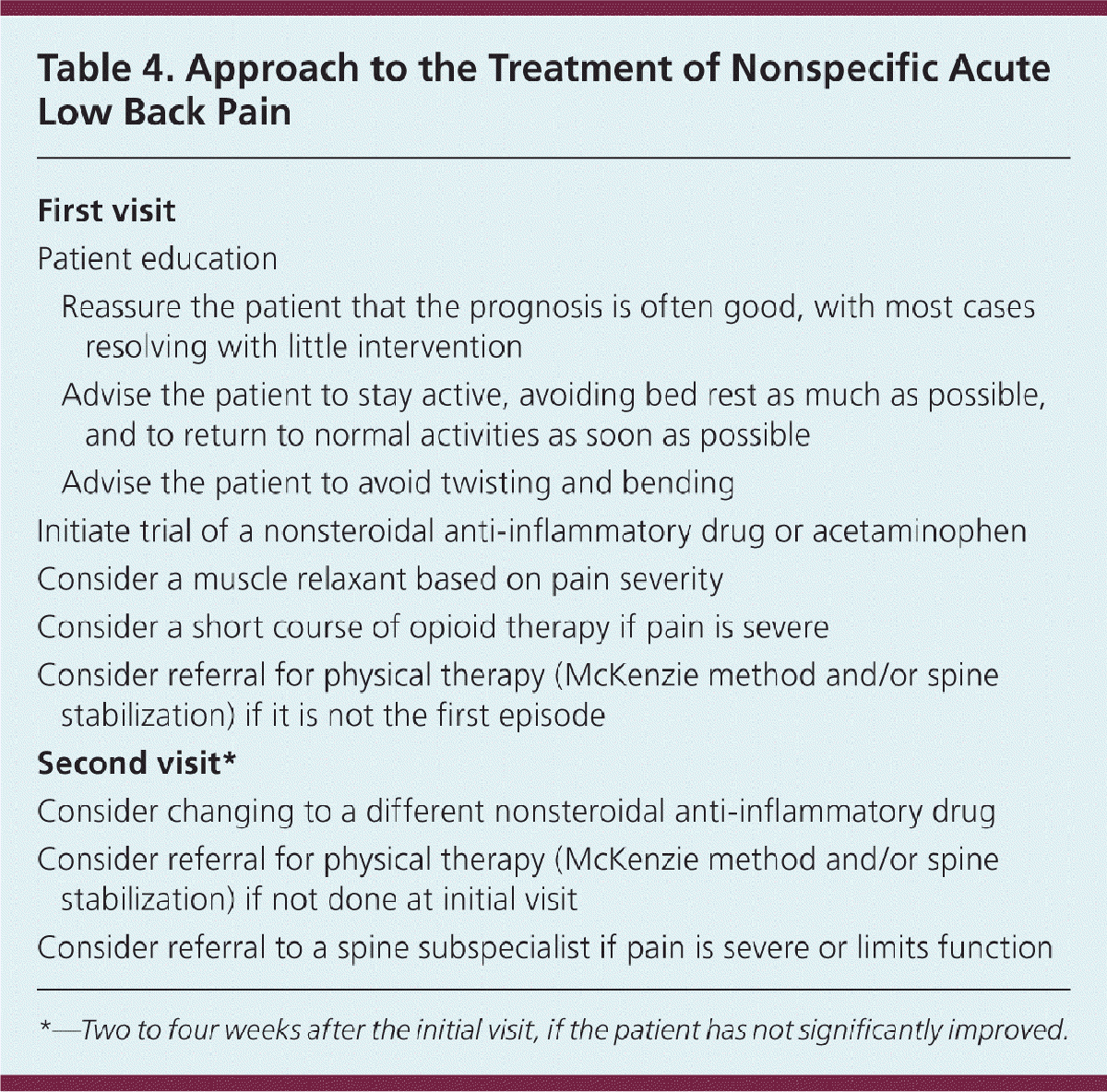
Clinical practice guidelines for acute LBP recommend a conservative approach for nontraumatic cases avoiding routine spinal imaging within the first 4 to 6 weeks of symptoms (during the acute phase of LBP). [6–10] Exceptions include patients with the following red flags: age younger than 20 years, infection, history of cancer, intravenous (IV) drug use, prolonged use of corticosteroids, osteoporosis, older age (older than 50 or 70 yr, depending on the guideline), or focal neurological deficit with progressive or disabling symptoms. [9, 11]
Although magnetic resonance imaging (MRI) for LBP within the first 6 weeks of symptoms is not recommended except in cases with red flags, approximately 20% receive MRI within first 4 to 6 weeks. [12] Early MRI may be associated with increased use of services for treatment and costs [13, 14] and may have deleterious effects on patient’s well-being, without providing additional benefit of diagnostic insight or improved health. [15] To our knowledge, no study has yet evaluated the factors associated with early MRI for occupational LBP.
Our objective was to identify demographic, job-related, psychosocial, and clinical factors associated with use of early MRI among a population-based cohort of WC claimants with acute LBP.
MATERIALS AND METHODS
Data Sources
Data were obtained from the Washington Workers’ Compensation Disability Risk Identification Study Cohort (D-RISC), a population-based study designed to identify risk factors for chronic disability among workers with acute back injury (details reported elsewhere). [16–18] D-RISC combined administrative claims and medical billing data provided by the Washington State Department of Labor and Industries (L&I), which operates a WC program that provides no-fault industrial insurance and covers two-thirds of all nonfederal Washington workers (the remaining one-third workers are employed by large, self-insured companies, for whom detailed data are not available).
D-RISC study participants were limited to workers older than 18 years with a back sprain/strain, an accepted WC claim, received compensation for missing 4 or more days from work, and not hospitalized in the acute period after injury. [19]
Trained personnel conducted computer-assisted telephone interviews with participants approximately 3 weeks (median: 18 d, range: 10–58 d) after filing the claim with L&I. Interviews included questions regarding overall and injury-specific health, personal, and work characteristics. The University of Washington institutional review board approved the study, and participants provided informed consent and were paid $10.
VARIABLE DEFINITIONS
Variables were selected a priori, informed by health services utilization models and current literature. [20, 21] The primary outcome variable for all analyses was receipt of early MRI (yes/no), defined as receiving a lumbar MRI 42 or less days after injury date. Dates of procedures from the WC medical bill payment database were used to calculate the duration between injury and MRI.
Interviews were completed approximately 1 month after injury (median: 30 d, range: 14–90 d). To account for the time lag between injury and interview, a lag variable (number of days after injury) was calculated for each worker.
Demographics
Participants provided demographic information that included race, ethnicity, education, income, and marital status.
Health Status
Workers provided self-reported health status (aside from injury) for the year before injury and concurrent with the interview (current), categorized on a Likert scale. Body mass index was categorized as normal (<25), overweight (25–29), obese (30–34), and very obese (>34). Catastrophizing, a psychosocial health measure of coping response, was categorized into 3 levels: low (<1), moderate (1–2.9), and high (3–4). [22] Work fear-avoidance was assessed by averaging responses to 2 items from the Fear-Avoidance Beliefs Questionnaire and categorized as very low (<3), low-moderate (3.1–4.9), high (5–5.9), and very high (6). [23] Mental health status was measured using the 36-Item Short Form Health Survey version 2 (SF-36 v2) (1-wk time frame) and scored on the basis of US population norms: 2 or more standard deviations (SD) below the general population mean (<30), 1–2 SD below (30–39.9), 1 SD below (40–49.9), and at/above the mean (≥50). [24, 25]
Employment
L&I administrative claims data were used to determine whether the worker had a previous compensable back claim. Workers reported overall job satisfaction and whether their employer offered accommodations for the injury (e.g., change in physical environment, tasks, work-schedule, job positions, or part-time work). Employment industry was determined according to the North American Industry Classification System. [26] Physical demands were self-reported as sedentary/light, medium, heavy, or very heavy, based on the amount of lifting, carrying, pushing, or pulling loads associated with typical work activities. [17]
Type of First Medical Visit
The type of first office visit was obtained from the WC medical bill payment database. This variable was categorized as primary care physician, occupational health physician, chiropractor, surgeon, emergency department, or other provider (including specialists and physical medicine).
Injury Characteristics
Measures describing the worker’s back injury included both self-report and clinical characteristics. Pain intensity refers to any pain in the last week, either from injury or from other causes, on a 0 to 10 scale, categorized as no/low pain (0–3), moderate pain (4–6), and high pain (7–10). [27] The Roland-Morris disability questionnaire assesses disability due to LBP and was categorized in 4 groups on the basis of scores 0 to 24: 0 to 6, 7 to 13, 14 to 18, and 19 to 24 (higher scores reflecting higher levels of disability). [28, 29] Medical record review by occupational health nurses provided a clinical estimate of injury severity and was categorized as moderate sprain/strain, major sprain/strain, or substantial immobility/radiculopathy. [30]
STATISTICAL ANALYSIS
Workers whose medical claim reported lumbar MRI 42 or fewer days after injury date were considered to have received an early MRI. This cutoff value reflects clinical guidelines, which recommend up to 6 weeks before imaging. [6–10] Rates of radiography and computed tomography (CT) were calculated for comparison. Descriptive and inferential analyses were performed using STATA/IC 10.1 for Macintosh (Stata Corp., College Station, TX).
Univariate analyses of demographic, health status, employment, provider, and injury variables were conducted using Pearson chi-square tests. Bivariate relationships evaluated the association between each variable and early MRI. Because the prevalence of the outcome was greater than 10%, a modified Poisson approach with robust error variance was used. [31] Multivariable models estimated the likelihood of receiving an early MRI for each factor while controlling for covariates (including a lag variable for time between injury and interview). The results of analyses were presented as incident rate ratios (IRRs) with 95% confidence intervals (CIs); IRR is the inverse of natural logarithm of β (or eβ) and demonstrates the multiplicative influence of 1 unit change in exposure on the rate of the outcome. Here, IRRs can be interpreted as relative risk of early MRI.
Chi-square analyses were used to assess multicollinearity by testing associations between pairs of related categorical variables. For pairs that were strongly associated (P < 0.05), each was removed sequentially from the full model to evaluate the effect on coefficients.
Seventeen percent (N = 322) received an MRI before completing the D-RISC questionnaire, which could have influenced responses to interview questions. To address this issue, a separate model excluded interview questions that may exhibit bias (e.g., health status, mental health measures, pain intensity).
To evaluate whether the early MRI may be attributed to planning of subsequent spinal injection procedures, we calculated the proportion of workers who received a spinal injection in 30 days after the early MRI. Injections included caudal, facet lumbar/sacral, transforaminal lumbar/sacral, or sacroiliac joint injections.
RESULTS
From July 2002 to April 2004, 4,354 workers were identified, of whom 49% agreed to participate in the D-RISC study, 27% could not be contacted, 3% were ineligible due to language limitations, and 21% declined to participate. Of the 2,147 subjects who agreed to participate, 240 were excluded for lacking work disability compensation, and 22 others were excluded for other reasons. The final D-RISC sample of 1,885 workers, compared with nonparticipants (N = 1776), was slightly older (age: mean [SD] 39.4 [11.2] vs. 38.2 [11.1] yr, P < 0.001) and included more women (32% vs. 26%, P < 0.001). [17] The majority of workers filed a claim within 2 months after injury (97%). Among those who did not (N = 55), claims were filed up to 9 months after injury and interviews were conducted up to a year after injury. For this study, these workers were excluded; the final study sample consisted of 1,830 workers.

Table 1 The median time from injury to the first medical appointment was 2 days (mean = 5, SD = 7). Among the 1,830 workers, 362 (19.8%) received an MRI within 42 days of the injury (early MRI) (Table 1). Of all workers, 34.4% (N = 630) received an MRI at any time in 1 year after injury. Overall, the mean time to MRI was 60 days (SD = 67). Among those who received an early MRI, the mean time to MRI was substantially less: 21 days (SD = 11, P < 0.001). Compared with MRI, more workers (N = 1002, 54.8%) received at least 1 lumbar radiograph in the year after injury (884 underwent radiography within the first 6 wk of injury). Far fewer workers received a lumbar CT in 1 year (N = 64, 3.5%); 27 received CT within the first 6 weeks of injury.
Table 2 The following variables were not associated with early MRI bivariately or in multivariate analyses: marital status, body mass index, past or current health status, and job satisfaction. Age, race, education, catastrophizing, job accommodations, previous compensable back claims, and self-reported pain intensity were associated with early MRI in bivariate analyses (Table 1) but were not significant in multivariate model after adjusting other covariates (Table 2).
Multivariable regression showed that male workers were 43% more likely to receive an early MRI than female workers (IRR: 1.43, 95% CI: 1.12–1.82), and workers whose initial visit type was with a surgeon were 78% more likely to receive an early MRI than those who visited a primary care physician initially (IRR: 1.78, 95% CI: 1.08–2.92) (model 1, Table 2). Workers with a chiropractor as the initial provider were half as likely to receive an early MRI compared with workers with the same demographic and injury characteristics whose initial provider was a primary care physician (IRR: 0.53, 95% CI: 0.42–0.66). Compared with workers with Roland scores below 6, workers with scores more than 18 were nearly 6 times more likely to receive an early MRI, holding all other covariates constant (IRR: 5.87, 95% CI: 3.16–10.89). Similarly, controlling for all other factors, the risk of early MRI was 3 times higher for workers with radiculopathy than for workers with mild sprains (IRR: 3.04, 95% CI: 2.44–3.79).
Regarding potential red flags and characteristics suggesting that the workers may be at greater risk for severe LBP, 51 workers (2.8%) were younger than 20 years, 373 workers (20.4%) were older than 50 years, and 6 workers were older than 70 years. Among workers who received an early MRI, 39.8% (N = 144) received at least 1 injection in the year after injury. The mean time between MRI and injection was 105 days (SD = 84 d). Within 30 days of the early MRI, 13.5% (N = 49) received an injection.
Analyses for multicollinearity showed that the following pairs of variables were strongly associated P < 0.05): pain intensity/Roland, injury severity/Roland, pain intensity/injury severity, past/current health status, catastrophizing/SF-36 mental health, fear-avoidance/catastrophizing, catastrophizing/SF-36 mental health, and Roland with each of the mental health measures (catastrophizing, fear-avoidance, and SF-36 mental health). Removal of each variable from the full model did not materially change the model associations or conclusions.
The multivariable model was run with and without the lag variable, representing time between injury and interview; the model associations and conclusions did not change upon exclusion of the lag variable. Model 2 (Table 2) excluded variables that could be biased because of the timing of the interview. Risk estimates exhibit patterns similar to model 1; magnitudes of the associations did not differ substantially.
DISCUSSION
This research identifies factors associated with receiving an early lumbar MRI among workers with nonspecific, acute uncomplicated LBP. Multivariable results indicate that male sex, type of first medical visit, functional status, medically documented injury severity, and fear-avoidance are strongly associated with receiving early MRI for occupational LBP.
Although injury severity is associated with an increased likelihood of receiving advanced imaging for LBP, [32] guidelines discourage early imaging unless patients have signs, symptoms, or characteristics suggestive of an underlying red flag condition, such as infection, tumor, or serious neurological impairment. [6, 8] We found that workers with radiculopathy or more severe neurological impairments were more likely to receive early imaging. It is possible that a small minority of early MRI recipients in this group may have borne definite red flag elements that justify early imaging; however, only 21.2% of the cohort was either younger than 20 years or older than 50 years, and individuals in these age groups were not disproportionately at risk for early MRI (results not shown). Although data on history of cancer, infection, IV drug use, or human immunodeficiency virus were not available, the prevalence of these conditions is likely to be very low in a relatively young working population. Among workers who received an early MRI, fewer than 15% underwent an injection procedure within 30 days of receiving the MRI, suggesting that many early MRIs may not have been used for injection planning purposes.
Studies have shown that neurosurgeon, neurologist, [33] and orthopedic surgeon [32, 34] providers are associated with increased likelihood of receiving advanced imaging (though not necessarily early). Although we were unable to assess each provider type individually due to sample sizes, our research shows that workers with an initial office visit with a surgeon provider (general, neurological, or orthopedic surgery) were highly likely to receive early MRI, independent of injury severity, suggesting that initial visit type also plays an important role in the utilization of early imaging. Early imaging should be considered a supplemental diagnostic tool for patients with red flags after the completion of a detailed medical history and physical examination. [7, 35] Some providers, especially those who typically see patients with severe injuries, such as surgeon providers, may routinely image most or all patients. This may result in patients without red flags, or with less severe injuries, receiving early MRI, and these providers having higher likelihood of early MRI than others.
Chiropractic initial visits were associated with a nearly 50% lower likelihood of MRI within the first 6 weeks of LBP symptoms. Chiropractic providers are actually more likely to use radiographs [32]; however, this utilization may be less costly to L&I, because the cost of radiographs is substantially less than MRIs (L&I 2009 reimbursement rates $85 vs. $1,131) and clinical outcomes do not differ by imaging modality. [14] Research suggests that initial chiropractic care results in significantly lower costs [36] and greater patient satisfaction. [37]
Fear-avoidance beliefs are an important psychosocial factor in the recovery of acute LBP, causing patients to avoid activities that are anticipated to cause or exacerbate pain (e.g., work). [23, 38] Research shows that holding elevated fear-avoidance beliefs is associated with increased health care use. [39] Our finding that workers with higher fear-avoidance beliefs were more likely to receive an early MRI than workers with low fear-avoidance beliefs is consistent with the literature. The use of early imaging may be particularly concerning for patients with elevated fear-avoidance beliefs, because they may be more predisposed to feel threatened by diagnostic labels, [40] develop chronic LBP, [41, 42] be prescribed narcotics, [39] or remain on disability. [38, 43]
The population-based design, large sample size, and the availability of detailed independent variables contribute to the strength and unique nature of this research. This study has several limitations. First, this cohort includes cases with 4 or more days of compensated lost work time, so results may not be generalizable to workers with less severe or noncompensable injuries. Second, 17% of the workers received imaging before the interview was conducted (N = 322), potentially introducing bias to the study. However, eliminating potentially biased covariates did not substantially change the study results. Third, information regarding a workers’ history of cancer, IV drug use, and human immunodeficiency virus status was not available for this analysis; for these red flags, early MRI would have been appropriate. Fourth, the purpose, scope, and design of this study limited its ability to assess several factors that warrant future research. This study did not incorporate information from physicians regarding the reason for ordering an MRI. It was also not possible to ascertain the appropriateness of the imaging received or whether the imaging was truly necessary for a particular patient. Finally, early imaging may influence outcomes, such as utilization, costs, health, or disability, but that analysis was beyond the scope of this study. These are important aspects in evaluating the potential overutilization of imaging and should be addressed by suitably designed, future research.
CONCLUSION
To our knowledge, this is the first study to evaluate individual-level factors, including self-reported pain and functioning, associated with early MRI for acute LBP. Results show that early MRI for LBP is a common practice, which may contribute to increased resource utilization and costs. [14, 44] It is prudent for providers to be aware of clinical practice guidelines and follow recommendations to limit advanced imaging in the first 4 to 6 weeks of LBP symptoms. Given the results of this study, providers could provide more customized care, based on the characteristics of patients with uncomplicated occupational LBP, and policy makers may seek to direct patients to certain types of providers early in the course of their LBP.
Key Points
Among workers with occupational LBP, male sex, elevated fear-avoidance, greater Roland-Morris disability scores, greater injury severity, and type of first visit were associated with increased likelihood of receiving MRI within the first 6 weeks of injury (after controlling for confounders).
Workers accessing chiropractic care initially were substantially less likely to receive an early MRI.
Understanding factors that are associated with early MRI use will help inform providers and policy makers about current utilization patterns and potential strategies for addressing guideline adherence.
Acknowledgments
This research was supported by Centers for Disease Control and Prevention National Institute for Occupational Safety and Health grants 1 R0 OH04069 and 1 T42 OH008433 and Agency for Healthcare Research and Quality grant R01 HS019222-01.
Federal funds were received to support this work.
Footnotes
The manuscript submitted does not contain information about medical device(s)/drug(s).
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
References:
Hestbaek L, Leboeuf-Yde C, Engberg M, et al.
The Course of Low Back Pain in a General Population.
Results From a 5-year Prospective Study
J Manipulative Physiol Ther. 2003 (May); 26 (4): 213–219Manchikanti L Singh V Datta S Cohen SP Hirsch JA
American Society of Interventional Pain P.
Comprehensive review of epidemiology, scope, and impact of spinal pain.
Pain Phys. (2009) 12:E35–70.
doi: 10.36076/ppj.2009/12/E35Sanders SH, Harden RN.
Medicolegal issues in acute and chronic low back pain.
In: Rucker KS, Cole AJ, Weinstein SM, eds. Low Back Pain:
A Symptom-Based Approach to Diagnosis and Treatment.
Boston, MA: Butterworth Heinemann; 2001:363–79.Frank JW, Kerr MS, Brooker AS, et al.
Disability resulting from occupational low back pain. Part I:
What do we know about primary prevention? A review of the
scientific evidence on prevention before disability begins.
Spine 1996;21:2908–17.Hashemi L, Webster BS, Clancy EA, et al.
Length of disability and cost of workers' compensation low back pain claims.
J Occup Environ Med 1997;39:937–45.American College of Occupational and Environmental Medicine.
Low Back Disorders. Occupational Medicine Practice Guidelines:
Evaluation and Management of Common Health Problems and
Functional Recovery in Workers. 2nd ed.
Elk Grove Village, IL:
American College of Occupational and Environmental Medicine; 2007.Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr., Shekelle P, Owens DK:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline
from the American College of Physicians and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491North American Spine Society Clinical Guidelines Committee.
Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis
In: North American Spine Society, ed. North American Spine Society.
Clinical Guidelines for Multidisciplinary Spine Care.
Burr Ridge, IL: North American Spine Society; 2007: 264.Davis PC, Wippold FJ II, Brunberg JA, et al.
ACR Appropriateness Criteria low back pain.
J Am Coll Radiol 2009;6:401–7.National Institute for Health and Clinical Excellence (NICE).
Low Back Pain: Early Management of Persistent Nonspecific Low Back Pain
London: National Institute for Health and Care Excellence; 2009.
[Report No.: Clinical guideline 88].Dagenais S, Tricco AC, Haldeman S.
Synthesis of Recommendations for the Assessment and Management
of Low Back Pain From Recent Clinical Practice Guidelines
Spine J. 2010 (Jun); 10 (6): 514–529Webster BS, Cifuentes M.
Relationship of early magnetic resonance imaging for work-related
acute low back pain with disability and medical utilization outcomes.
J Occup Environ Med 2010;52:900–7.Gilbert FJ, Grant AM, Gillan MG, et al.
Low back pain: influence of early MR imaging or CT
on treatment and outcome—multicenter randomized trial.
Radiology 2004;231:343–51.Jarvik JG, Hollingworth W, Martin B, et al.
Rapid magnetic resonance imaging vs radiographs for
patients with low back pain: a randomized controlled trial.
JAMA 2003;289:2810–8.Modic MT, Obuchowski NA, Ross JS, et al.
Acute low back pain and radiculopathy: MR imaging findings
and their prognostic role and effect on outcome.
Radiology 2005;237:597–604.Turner JA, Franklin G, Fulton-Kehoe D, et al.
Prediction of chronic disability in work-related
musculoskeletal disorders: a prospective, population-based study.
BMC Musculoskelet Disord 2004;5:14.Turner JA, Franklin G, Fulton-Kehoe D, et al.
ISSLS prize winner: early predictors of chronic work disability:
a prospective, population-based study of workers with back injuries.
Spine 2008;33:2809–18.Turner JA, Franklin G, Fulton-Kehoe D, et al.
Worker recovery expectations and fear-avoidance predict work disability
in a population-based workers’ compensation back pain sample.
Spine 2006;31:682–9.Franklin GM, Stover BD, Turner JA, et al.
Early opioid prescription and subsequent disability among workers
with back injuries: the Disability Risk Identification Study Cohort.
Spine 2008;33:199–204.Andersen RM.
Revisiting the behavioral model and access to medical care: does it matter?
J Health Soc Behav 1995;36:1–10.Pransky G, Benjamin K, Hill-Fotouhi C, et al.
Work-related outcomes in occupational low back pain: a multidimensional analysis.
Spine 2002;27:864–70.Sullivan M, Bishop S.
The pain catastrophizing scale: development and validation.
Psychol Assess 1995;7:524–32.Waddell G, Newton M, Henderson I, et al.
A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of
fear-avoidance beliefs in chronic low back pain and disability.
Pain 1993;52:157–68.Ware JE Jr, Sherbourne CD.
The MOS 36-item short-form health survey (SF-36).
I. Conceptual framework and item selection.
Med Care 1992;30:473–83.Ware JE Jr, Kosinski M, Dewey JE.
How to Score Version 2 of the SF-36 Health Surveyed.
Lincoln, RI: Quality Metric; 2000.US Census Bureau.
North American Industry Classification System (NAICS), 2002. Available at:
http://www.census.gov/epcd/naics02
Accessed May 25, 2011.Von Korff M, Ormel J, Keefe FJ, et al.
Grading the severity of chronic pain.
Pain 1992;50:133–49.Roland M, Morris R.
A study of the natural history of back pain. Part I: development of a
reliable and sensitive measure of disability in low-back pain.
Spine 1983;8:141–4.Turner JA, Fulton-Kehoe D, Franklin G, et al.
Comparison of the Roland-Morris Disability Questionnaire and generic
health status measures: a population-based study of
workers’ compensation back injury claimants.
Spine 2003;28:1061–7.Stover BD, Turner JA, Franklin G, et al.
Factors associated with early opioid prescription
among workers with low back injuries.
J Pain 2006;7:718–25.Zou G.
A modified Poisson regression approach to prospective studies with binary data.
Am J Epidemiol 2004;159:702–6.Carey TS, Garrett JM.
Patterns of ordering diagnostic tests for patients with acute low back pain.
Ann Intern Med 1996;125:807–14.Cherkin DC, Deyo RA, Wheeler K, et al.
Physician variation in diagnostic testing for low back pain.
Who you see is what you get.
Arthritis Rheum 1994;37:15–22.Carey TS, Garrett J, Jackman A, et al.
The Outcomes and Costs of Care for Acute Low Back Pain Among Patients
Seen by Primary Care Practitioners, Chiropractors, and Orthopedic Surgeons
The North Carolina Back Pain Project
New England J Medicine 1995 (Oct 5); 333 (14): 913–917Johanning E.
Evaluation and management of occupational low back disorders.
Am J Ind Med 2000;37:94–111.Stano M, Smith M:
Chiropractic and Medical Costs of Low Back Care
Medical Care 1996 (Mar); 34 (3): 191–204Baldwin ML, Cote P, Frank JW, et al.
Cost-effectiveness Studies of Medical and Chiropractic Care for
Occupational Low Back Pain. A Critical Review of the Literature
Spine J. 2001 (Mar); 1 (2): 138–147Fritz JM, George SZ, Delitto A.
The role of fear-avoidance beliefs in acute low back pain:
relationships with current and future disability and work status.
Pain 2001;94:7–15.Wideman TH, Sullivan MJ.
Differential predictors of the long-term levels of pain intensity,
work disability, healthcare use, and medication use in
a sample of workers’ compensation claimants.
Pain 2011;152:376–83.Boston A, Sharpe L.
The role of threat-expectancy in acute pain: effects on attentional
bias, coping strategy effectiveness and response to pain.
Pain 2005;119:168–75.Fritz JM, George SZ.
Identifying psychosocial variables in patients with acute work-related
low back pain: the importance of fear-avoidance beliefs.
Phys Ther 2002;82:973–83.Al-Obaidi SM, Nelson RM, Al-Awadhi S, et al.
The role of anticipation and fear of pain in the persistence of
avoidance behavior in patients with chronic low back pain.
Spine (Phila Pa 1976) 2000;25:1126–31.Flynn TW, Smith B, Chou R.
Appropriate use of diagnostic imaging in low back pain—
a reminder that unnecessary imaging may do as much harm
as good [published online ahead of print June 3, 2011].
J Orthop Sports Phys Ther 2011;41:838–46.Lurie JD, Birkmeyer NJ, Weinstein JN.
Rates of advanced spinal imaging and spine surgery.
Spine 2003;28:616–20.
Return to WORKERS' COMPENSATION
Since 8-11-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |