

The Effectiveness of Manual and Exercise Therapy on
Headache Intensity and Frequency Among Patients
with Cervicogenic Headache: A Systematic
Review and Meta-analysisThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2022 (Nov 23); 30 (1): 49 ~ FULL TEXT
OPEN ACCESS Pietro Bini, David Hohenschurz-Schmidt, Vincenzo Masullo, Diana Pitt, Jerry Draper-Rodi
University College of Osteopathy,
275 Borough High Street,
London, SE1 1JE, UK
Background: Cervicogenic headache is a secondary headache, and manual therapy is one of the most common treatment choices for this and other types of headache. Nonetheless, recent guidelines on the management of cervicogenic headache underlined the lack of trials comparing manual and exercise therapy to sham or no-treatment controls. The main objective of this systematic review and meta-analysis was to assess the effectiveness of different forms of manual and exercise therapy in people living with cervicogenic headache, when compared to other treatments, sham, or no treatment controls.
Methods: Following the PRISMA guidelines, the literature search was conducted until January 2022 on MEDLINE, CENTRAL, DOAJ, and PEDro. Randomized controlled trials assessing the effects of manual or exercise therapy on patients with cervicogenic headache with headache intensity or frequency as primary outcome measures were included. Study selection, data extraction and Risk of Bias (RoB) assessment were done in duplicate. GRADE was used to assess the quality of the evidence.
Results: Twenty studies were included in the review, with a total of 1439 patients. Common interventions were spinal manipulation, trigger point therapy, spinal mobilization, scapulo-thoracic and cranio-cervical exercises. Meta-analysis was only possible for six manual therapy trials with sham comparators. Data pooling showed moderate-to-large effects in favour of manual therapy for headache frequency and intensity at short-term, small-to-moderate for disability at short-term, small-to-moderate for headache intensity and small for headache frequency at long-term. A sensitivity meta-analysis of low-RoB trials showed small effects in favor of manual therapy in reducing headache intensity, frequency and disability at short and long-term. Both trials included in the sensitivity meta-analysis studied spinal manipulation as the intervention of interest. GRADE assessment showed moderate quality of evidence.
Conclusion: The evidence suggests that manual and exercise therapy may reduce headache intensity, frequency and disability at short and long-term in people living with cervicogenic headache, but the overall RoB in most included trials was high. However, a sensitivity meta-analysis on low-RoB trials showed moderate-quality evidence supporting the use of spinal manipulation compared to sham interventions. More high-quality trials are necessary to make stronger recommendations, ideally based on methodological recommendations that enhance comparability between studies. Trial registration The protocol for this meta-analysis was pre-registered on PROSPERO under the registration number CRD42021249277.
Keywords: Exercise therapy; Meta-analysis; Musculoskeletal manipulation; Post-traumatic headache; Randomized controlled trial; Systematic review.
From the FULL TEXT Article:
Introduction
Background
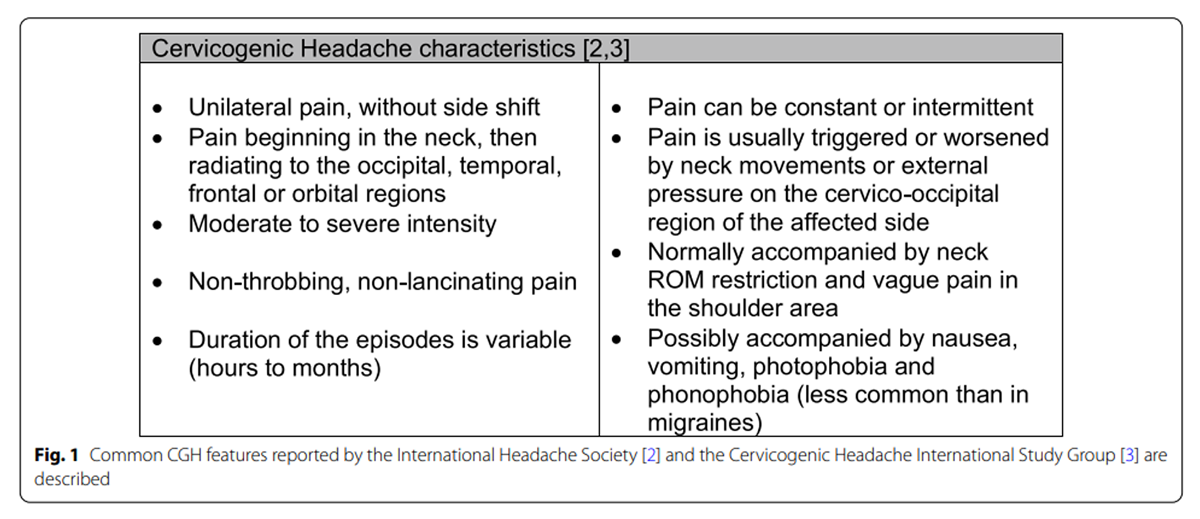
Figure 1 Cervicogenic Headache (CGH) is a secondary headache, with a prevalence of 1–4% among people experiencing headaches. [1] The pathophysiological mechanism underlying this condition is referred pain, and the currently accepted theory is that structures in the upper cervical spine supplied by the first three spinal nerves can refer pain to the occipital, frontal or temporal regions. Specific features which tend to characterize CGH and are considered in the diagnostic process are presented in Figure 1. [1, 2] Several sets of criteria have been proposed. Most widely used are the criteria proposed by the International Headache Society (IHS) in the International Classification of Headache Disorders-3rd version (ICHD) [2], and the ones proposed by the Cervicogenic Headache International Study Group (CHISG). [3] Despite the presence of features characteristic of CGH, different headaches with similar phenotypes can co-exist, posing further obstacles to the diagnostic process. [5]
Manual therapy is among the most common treatment choices for headaches in Australia, Europe and in the USA, provided to about a third of patients in headache clinics. [5] Recent guidelines on the management of CGH [6] support the use of exercise therapy and spinal manipulation to reduce CGH pain intensity, frequency, and disability. Based on the current literature, an initial 8–10 sessions of manual or exercise therapy (i.e. low-load endurance exercise, spinal manipulation or mobilization) over 6 weeks are recommended in isolation. [6]
While this recommendation is supported by three trials, the guideline authors highlight the lack of high-quality studies studying the efficacy of non-pharmacological interventions compared to sham or no treatment. [6] Two systematic reviews and meta-analyses [7, 8] in this field evaluated the effectiveness of spinal manipulation (alone or combined with mobilization) for CGH and tension-type headache. One systematic review [8] found no evidence in favour of spinal manipulation compared to other conservative interventions for headache intensity or disability. This review compared manipulation and mobilization to other forms of manual therapy and various forms of exercise, but it did not assess the effectiveness of other interventions commonly used by manual therapists (i.e. massage, exercise, and acupuncture), nor the efficacy of manual therapy compared to no treatment or sham. The second systematic review [8] did include sham-controlled randomized controlled trials (RCTs), but grouped sham interventions with “other forms of manual therapy''. RCTs using sham and other manual therapy interventions as comparisons were incorporated into the same meta-analysis, not allowing for a separate appraisal of RCTs with sham-controls only. The review reported spinal manipulation as more effective in the short-term for headache intensity, frequency and disability, and in the medium-term for headache frequency, but it did not allow for conclusions on comparisons to sham controls.
Our systematic review has a broader scope than the previous reviews, comparing the effectiveness of interventions commonly used in a manual therapy setting to other conservative interventions, as well as to sham or no treatment. This allows for the assessment of intervention efficacy against control interventions that ideally account for expectancy effects, rather than basing recommendations solely on comparative effectiveness studies, which can lead to bias. [9] Such recommendations would help to inform patients and clinicians on the appropriateness of choosing manual and exercise therapy for the management of CGH in general, and against or alongside other possible treatment options.
Objectives
The objective of this systematic review was to systematically review the effectiveness and efficacy of manual and exercise therapy for CGH intensity and frequency when compared to placebo, no treatment or other interventions.
Methods
The systematic review was performed following the PRISMA guidelines. [10]
Literature search
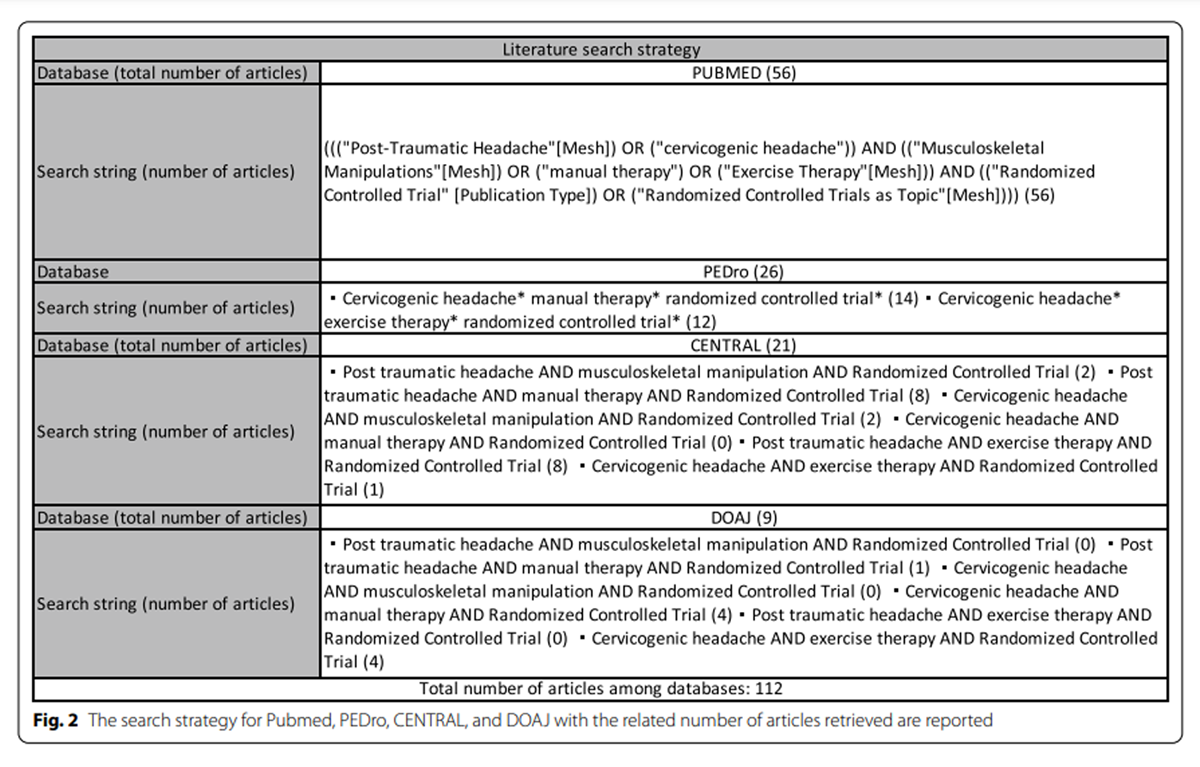
Figure 2 A computerized search was conducted for the following electronic databases: MEDLINE (via PubMed), CENTRAL, DOAJ, and PEDro. EMBASE, MEDNAR and SAGE databases were not consulted due to access limitation, deviating from the protocol of this systematic review. The search was from inception to December 2020, and was updated in January 2022 to include trials published after December 2020. No language restrictions were applied during the search, but studies were excluded if English, German, Italian, Spanish or Portuguese language versions were not available in the literature. References of the included studies were searched manually, and content experts consulted to ensure that no relevant literature was missed. The complete search strategy is provided in Figure 2.
Eligibility criteria
The research question and eligibility criteria were designed following the PICOS (Participant, Intervention, Comparator, Outcomes, Study design) method. [11]
Participants
Trials with people diagnosed with CGH according to the IHS [2] or the CHISG [3] diagnostic criteria were included, regardless of participants’ age, gender or symptoms duration. Trials using modified versions of the aforementioned criteria were also included, in line with previous Cochrane reviews. [12] Nonetheless, for transparency reasons and to allow potential secondary analyses on the impact of diagnostic criteria on trial results, studies that did not state the diagnostic criteria used for CGH were excluded.
Intervention(s)
Manual therapy is defined as any techniques administered manually by a trained practitioner for therapeutic purposes. [13] For the scope of this systematic review, manual therapy techniques of interest included massage, trigger point therapy, kinesio-taping, manipulation, mobilization, acupuncture (including dry needling) or a combination of such techniques. Exercise therapy involves movement prescribed to correct impairments, restore muscular and skeletal function, and/or maintain a state of well-being. Therapeutic exercise modalities considered for inclusion by this systematic review were: endurance training (i.e. low-load endurance exercises), resistance training (isotonic, isometric and isokinetic exercises), flexibility training (static and dynamic mobility exercises, stretching exercises). [14] Studies which included a combination of manual and exercise therapy interventions (i.e. spinal manipulation and stretching exercises; trigger point therapy and low-load endurance exercises) were included. Trials using reflexology, acupressure, wellness massage or Reiki as the experimental intervention of interest were excluded.
Comparator(s)/control conditions
Eligible comparators were sham and placebo controls, no treatment, and other active interventions.
Main outcome(s)
Headache intensity, disability, frequency and duration are commonly used outcomes for headaches [15, 16] and have been considered by previous guidelines. [6] The primary outcome measures of interest were headache intensity and frequency, and trials not including these outcome measures were considered ineligible for the systematic review. Secondary outcomes of interest were disability and headache duration.
Study design
Only prospective randomized controlled trials were included. Case reports and case series, observational studies, and crossover studies were not eligible.
Screening and eligibility assessment
The literature search and de-duplication were carried out by a single researcher (PB). Search results were imported to Endnote© and duplicates removed using the Endnote tool. Subsequent screening performed in Covidence [17], an online platform for systematic reviews.
The study selection was performed in duplicate by two independent reviewers (PB and VM), initially based on study titles and abstracts, and followed by full-text screening, using a pre-defined study eligibility form on an offline spreadsheet in conjunction with Covidence, where decisions on inclusion/exclusion of trials were made. Disagreements were discussed by the two reviewers, and mediated by a third party if necessary. Screening procedures were pre-tested by calculating a Kappa score on a sub-sample of retrieved studies. [18]
Data extraction
Two independent reviewers (PB and VM) extracted data using a predefined data extraction form on an offline spreadsheet, and consensus was reached by discussion and mediation in case of disagreements. Data were extract for: author and date of the trial, experimental and control interventions studied, primary and secondary outcome measures considered, duration and frequency of the intervention, and follow-up measurements times. For the primary and secondary outcome measures of interest for this review, values were extracted for all reported time points and groups. Where necessary, data were extracted from figures using the Adobe Reader© measurement tool.
A description of potentially relevant studies excluded at the full-text screening stage with reasons for exclusion was provided in the results section.
Risk of bias assessment
Risk of bias (RoB) assessments were performed by two reviewers (PB and VM) using the criteria proposed by the Cochrane Back and Neck Group [19], and consensus was reached by discussion when needed. Inter-rater reliability was assessed using Kappa score. [18] As recommended by the authors of the RoB tool, trials were not categorized according to arbitrary cut-off points of the overall score. Instead, studies were considered as overall low-RoB if no individual domain was rated as “high” or “unsure” RoB. Studies which scored “unsure”, but not “high”, for one or more items, were considered as overall unsure RoB, and “high” if any individual item was rated as high RoB.
A common concern in manual and exercise therapy studies is the lack of blinding of patients, providers, or both. [20, 21] Obscuring treatment allocation from patients, and in particular therapists, is inherently difficult due to the complex and participatory nature of most interventions. [22] To avoid unduly skewing RoB assessments, and aligning with a previous meta-analysis of physiotherapy for headaches [12], the items “patient blinding”, “assessor blinding” and “therapist blinding” were considered non-applicable. Following methodology recommendations, the RoB assessment for each trial was outcome-specific. [23] Considering that the primary and secondary outcome measures of interest of this systematic review constituted of subjective outcome measures, the RoB assessment for headache intensity, frequency, duration and disability could be summarized across these outcomes. Where objective or clinically-observed outcomes were evaluated, a separate RoB assessment was provided.
Data synthesisDescriptive analysis A detailed description of study characteristics and RoB assessments was provided in the results section. For the descriptive analysis, trials were sub-grouped according to the specific experimental intervention used. Data from the included trials were presented in a summary table.
In order to determine whether statistically significant changes constituted important clinical benefits or detriments for patients, Minimal Clinical Important Differences (MCIDs) were analyzed when available from the literature for a specific outcome measure. The MCID is defined as the smallest difference in score in any outcome that patients can perceive as beneficial or harmful. MCIDs allow for the appreciation of patients’ perspectives on their health and treatments, making MCIDs an important factor in decision-making. [24] To facilitate the interpretation of the findings, RoB judgements and estimates of outcomes, as well as available data on statistical (P value) and clinical significance (MCIDs) were described in separate summary tables.
Regarding MCIDs for the outcome measures of interest in this systematic review, headache intensity is often assessed via a Visual Analogue Scale (VAS) or Numeric Pain Rating Scale (NPRS), headache frequency is often reported as “number of days with headache in last 2 or 4 weeks”, and disability as the Neck Disability Index (NDI). The aforementioned pain scales have been shown to be reliable in assessing pain intensity and disability. [7, 25, 26, 28] Nonetheless, MCIDs of these scales for CGH have only been derived for NPRS (2.5-point reduction after 4 weeks of intervention) [16], NDI (5.5-point reduction at 4 weeks) [16], and headache frequency (50% reduction of days with headache). [29] MCIDs for headache duration were not found in the literature. Throughout the Results and Discussion, findings were only contextualized with MCIDs when these were available from the literature for the respective outcome measure.
Meta-analysis The quantitative synthesis was performed using RevMan 5 (Review Manager 5 software, Version 5.4). [30] For continuous outcomes, studies were compared using standardized mean differences (SMDs) and standard deviations (SDs). In cases of missing data, study authors were contacted. If the missing data were not accessible and not imputable from other reported data, articles were excluded from quantitative analyses. Q statistics and I2 were used to assess statistical heterogeneity. Random effects models were employed to calculate overall effects, and forest plots to depict estimates. SMDs between 0.2 and 0.5 were considered as small effect sizes, SMD between 0.5 and 0.8 moderate effect sizes, and SMD > 0.8 were considered large effect sizes. [31]
Due to large differences in the designs of the included trials, the strategy for data pooling was changed from the one proposed in the protocol to allow for a more nuanced interpretation of the findings. Studies were compared only when the control interventions were comparable (i.e. grouping trials with sham or placebo controls, trials with no-treatment controls, and trials with other interventions), and pooling was divided into short-term (< 3 months) and long-term (> 3 months) endpoints, in line with previous systematic reviews on this topic. [32] When a single study reported multiple outcome assessments within the same time period (e.g. 2 or more follow-ups before 3 months), data for the time point closest to the other pooled studies were used. When trials with high or unsure RoB were included in the meta-analysis, a sensitivity analysis was also conducted, excluding the high or unsure RoB studies.
GRADE assessment The GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach [33] was used to evaluate the overall quality of the evidence for each outcome of interest. In brief, the overall quality of evidence for each pooled estimate was initially considered “high”, and could be downgraded by 1 level for each of the following 5 criteria: RoB (any of the trials included in the analysis showed “high” or “unsure” RoB [34], inconsistency (large heterogeneity among trials, I2 > 50%) [35], imprecision (< 400 participants for each comparison) [36], indirectness (indirectness of population, outcomes or intervention) [37], and publication bias (which was assessed with a funnel plot and Egger’s test if 10 or more studies were pooled). [38] Two reviewers (PB and VM) applied the criteria. A GRADE profile was completed for each pooled estimate. The following definitions of quality of the evidence were applied [39]: high quality (further research is very unlikely to change our confidence in the estimate of effect), moderate quality (further research is likely to have an important effect on our confidence in the estimate of effect and may change the estimate), low quality (further research is very likely to have an important effect on our confidence in the estimate of effect and is likely to change the estimate), and very low quality (we are very uncertain about the estimate).
Results
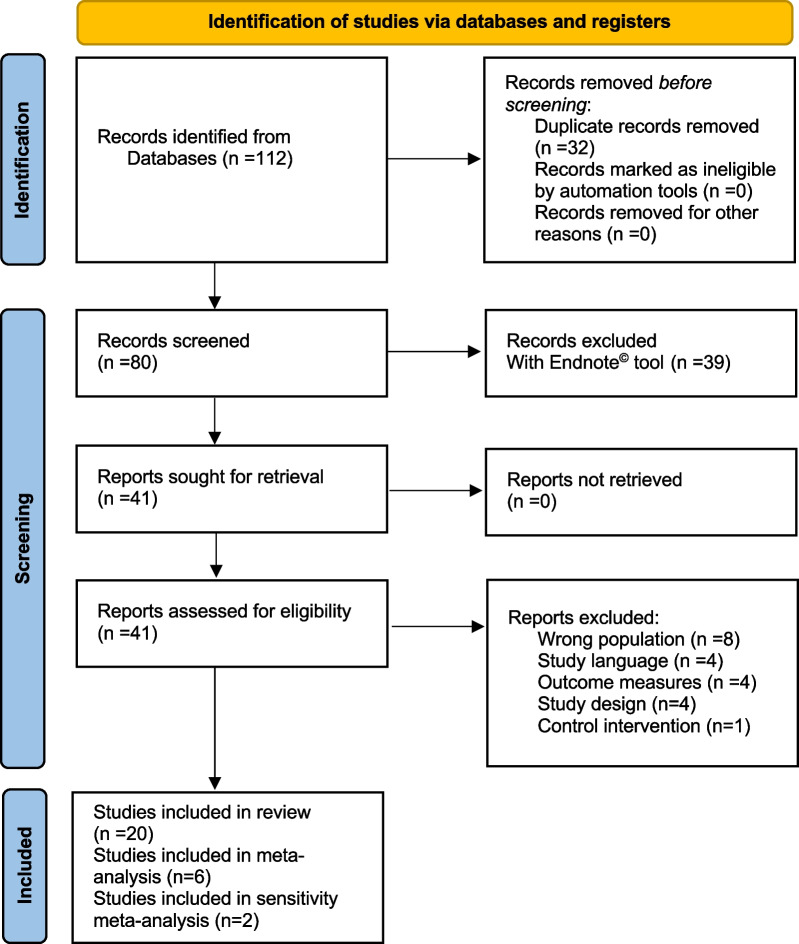
Figure 3

Table 1 The detailed process of study selection performed in January 2022 is presented in the PRISMA flow diagram (Figure 3).
After deduplication, the literature search identified 80 potentially relevant trials. Twenty studies were included in the final review, with a total of 1,439 patients. The eligibility assessment had strong inter-rater reliability (Cohen’s Kappa = 0.92).
Trials were mainly excluded during the full-text screening due to ineligible pathologies (i.e. different headaches) [10-44], outcome measures [45-48], and unclear diagnostic criteria for CGH. [49, 50] Table 1 provides the characteristics of the included trials.
As part of the inclusion criteria, all included trials described the diagnostic criteria used during their screening process. The official ICHD and CHISG diagnostic criteria [2, 3] were strictly followed by a limited number of studies, whilst the majority utilized modified versions of such criteria. In most cases, the discrepancy between the official sets of criteria and the ones used by the trials was the absence of diagnostic nerve blocks, which is a fundamental criterion for the CHISG, but not for the IHS.
Risk of Bias
Table 2
Table 3 The RoB analysis showed high inter-rater reliability (Cohen’s Kappa = 0.87). Overall RoB was low in eight trials [53, 55, 56, 60, 61, 66–68], unsure in six trials [51, 58, 62–64, 69], and high in six trials [52, 54, 57, 59, 65, 70] for the primary and secondary outcome measures. Further detail regarding the RoB of individual studies is found in Table 2.
Descriptive analysis: primary outcome measures
Among the included trials, the majority analyzed manual therapy in isolation: six focussed on spinal manipulation [52, 53, 55, 56, 61, 68], two on trigger point therapy [21, 58], two on spinal mobilization [57, 60], and one study each on kinesio-taping [54] and dry needling. [62] Seven trials used a combination of manual and exercise therapy [59, 63, 64, 66, 67, 69, 70], and two used exercise therapy alone. [59, 65] Ten studies used “other interventions” in their control groups (e.g. spinal mobilization, scapulo-thoracic exercises, trigger point therapy), nine studies used sham or placebo interventions, and four used no treatment. Nine studies had a long-term follow-up, and the last follow-ups among these studies averaged 42 weeks, ranging from 3 months to 2 years. Headache intensity was assessed with an 11 or 101-point Visual Analogue Scale (VAS), 11-point Numerical Pain Rating Scale (NPRS), 11-point Coloured Analogue Scale (CAS), and with a 100-point Modified Von Korff Scale. Composite headache questionnaires, which combined headache intensity, frequency, and other outcome measures, were used in two trials; these were not comparable to other pain intensity scales and relevant raw data could not be accessed. [57, 62]Headache frequency was assessed as the “number of days (with headache) in the previous four weeks”, “days in the previous two weeks”, or as “days in the previous week”. The following descriptive analysis is categorized according to the main study interventions and provides a brief overview of the findings from included trials. Tables 1 and 3 include further detail, list the statistical significance and MCIDs and should be referred to for a complete overview of the trials’ results.
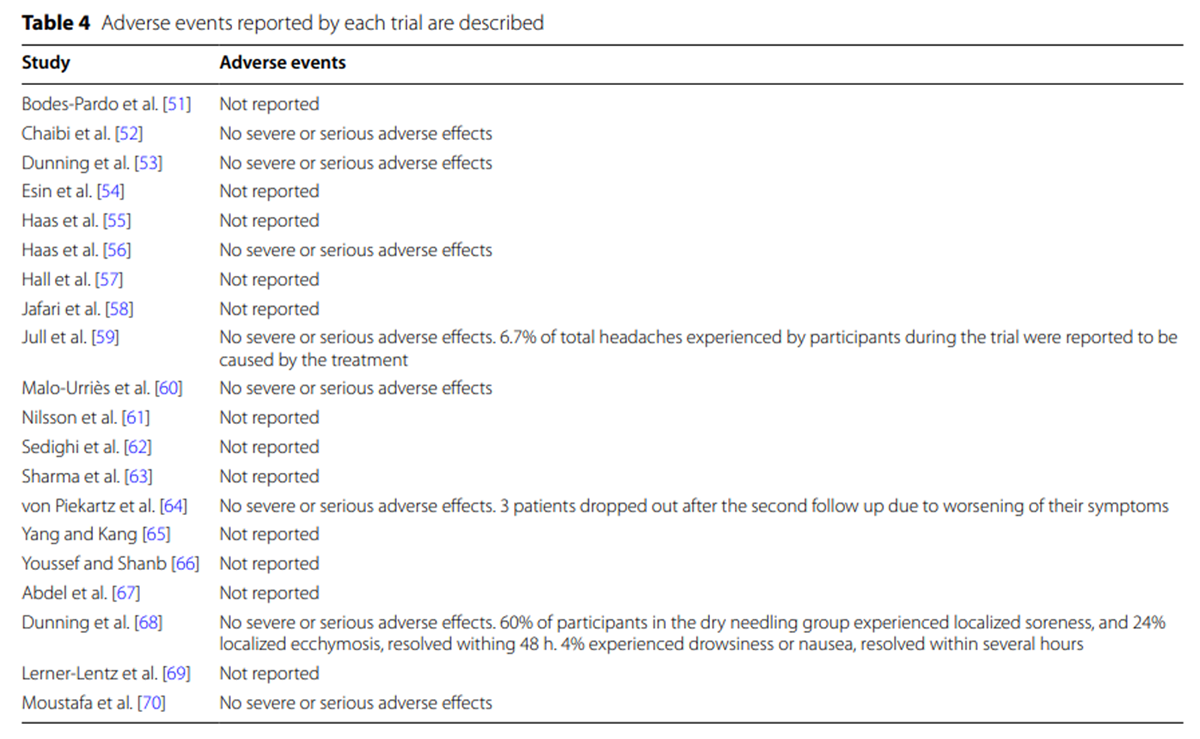
Table 4 Only 8 of the included trials reported whether adverse events were monitored. No severe adverse events were reported, but minor or transient adverse effects were noted in 3 trials [59, 64, 68], which are described in Table 4.
Spinal manipulation
Overall, 8 trials assessed the effectiveness of spinal manipulation. Two trials with low RoB [56, 57] (n = 336) compared spinal manipulation alone to sham treatments and found statistically significant changes in favor of spinal manipulation (p < 0.05) at short and long term. MCIDs for headache intensity and frequency were reached by one trial only [56], but over half of the participants receiving a higher dose of spinal manipulation achieved at least a 50% improvement in such outcomes in the second trial. [57]
Three trials with low RoB (n = 306) compared spinal manipulation to other forms of manual therapy. [53, 61, 68] Spinal manipulation was found more effective than spinal mobilization and cranio-cervical flexion exercises (p < 0.001) [53], and multimodal therapy (deep friction massage, trigger point therapy, light laser therapy) (p < 0.05) [61], and MCIDs were reached at short and long term. A combination of spinal manipulation and electrical dry needling was found more effective than spinal mobilization and cranio-cervical exercises at short and long-term. [69] Important clinical changes were also found in favor of spinal manipulation (with or without exercise therapy] for headache frequency and intensity in two high and unsure-RoB trials (n = 245) [59, 69] at short and long term.
Spinal mobilization
The effectiveness of spinal mobilization was assessed by two trials with low RoB [60, 66] (n = 120) and one study with unsure RoB [63] (n = 36). Spinal mobilization (with or without exercise therapy) was found more effective than no-treatment [60], massage and exercise therapy [66], and postural correction or exercise therapy [63] (p < 0.05) at short term. For outcome measures with MCIDs available from the literature, MCIDs were reached within four to seven weeks in all trials.
Myofascial trigger point therapy
Two trials with small sample sizes (n = 38), unsure RoB and no long-term follow-up found statistically significant superiority of sternocleidomastoid myofascial trigger point release for CGH compared to sham trigger point therapy (p < 0.001), and a no treatment control (p < 0.05). [51, 58] MCIDs for headache intensity and frequency were reached.
Dry needling
The unsure-RoB trial by Sedighi et al. [62] (n = 30) found no statistically significant changes (p > 0.05) for sub-occipital and trapezius dry needling compared to sham acupuncture at 1 week.
Temporo-mandibular joint (TMJ) treatment
One trial with unsure RoB (n = 43) [64] compared a similar set of manual and exercise therapy interventions (mobilization, trigger point release, coordination and stretching exercises depending on the therapists’ clinical decision) either directed to the TMJ area or to the cranio-cervical region in people living with CGH and showing signs of TMJ dysfunction. They found superior effects for the TMJ group (p < 0.001) at 6 months.
Kinesio-taping
Kinesio-taping was compared to sham taping and to home rehabilitation by one high-RoB trial [54] (n = 101), and statistical (p < 0.01) and clinical improvements at 4 and 8 weeks were reported. The study population consisted of teenagers aged 14–16 diagnosed with CGH and with presence of cervical “myogenic trigger zones”.
Therapeutic exercise
Two high-RoB trials (N = 140) assessed the effectiveness of therapeutic exercise in isolation. Jull et al. [59] compared low-load endurance cervico-scapular exercises to no treatment, and found statistical significant changes in headache intensity and frequency at 7 weeks and 12 months (p < 0.05). MCIDs were reached for headache frequency.
The high-RoB trial by Yang and Kang [65] (n = 30) compared cranio-cervical flexion exercises alone and manual suboccipital manual relaxation alone to a no-treatment control group. Despite between-group differences in headache intensity reported as significant (p < 0.05), the values reported in the study for the follow-up assessment were unequivocally mistaken (values of > 350 for a 0–100 VAS). The authors of the trial were contacted without success.
Self-sustained Natural Apophyseal Glide (SNAG)
Hall et al. [57] (n = 32) compared SNAG treatment to sham-SNAG. Patients were asked to perform SNAG autonomously twice daily for twelve months. A headache index was used as primary outcome measure, and significant between-group differences were found in favour of the experimental group at 4 weeks and twelve months (p < 0.05). Poor treatment compliance in the control group at four weeks, and in both groups at twelve months was reported, and the study had high RoB.
Graston technique
The low-RoB trial by Abdel et al. [67] (n = 60) compared Graston mobilization plus therapeutic exercise to exercise alone, and found between-group differences favoring Graston mobilization for headache intensity and frequency (p < 0.001) at four weeks. MCIDs for headache frequency were reached at 4 weeks.
Dennerol cervical extension traction
The high-RoB trial by Moustafa et al. [70] (n = 60) compared two groups treated with a mix of manual and exercise therapy, where the experimental group was also treated using the Dennerol traction device. The experimental group had significant improvements (p < 0.001) compared to the control group at ten weeks, one and two years for headache frequency, which also reached the MCID at all timepoints.
Descriptive analysis: secondary outcome measures
Table 5 Table 5 shows the results for the other outcome measures considered by each of the included studies, reporting levels of statistical and clinical significance when available, and the reader is invited to consult it for a more precise interpretation of the following section. The most common additional outcome measures used by the RCTs and included in this systematic review were disability (eleven trials), headache duration (eight trials) and pressure-pain-thresholds (seven trials). Cervical spine range of motion (CROM) and Medication intake were assessed in six trials, perceived change in four trials, and cervical flexors performance in three trials. A descriptive description of secondary outcome measures of interest (headache duration and disability) is provided in Table 5.
Disability
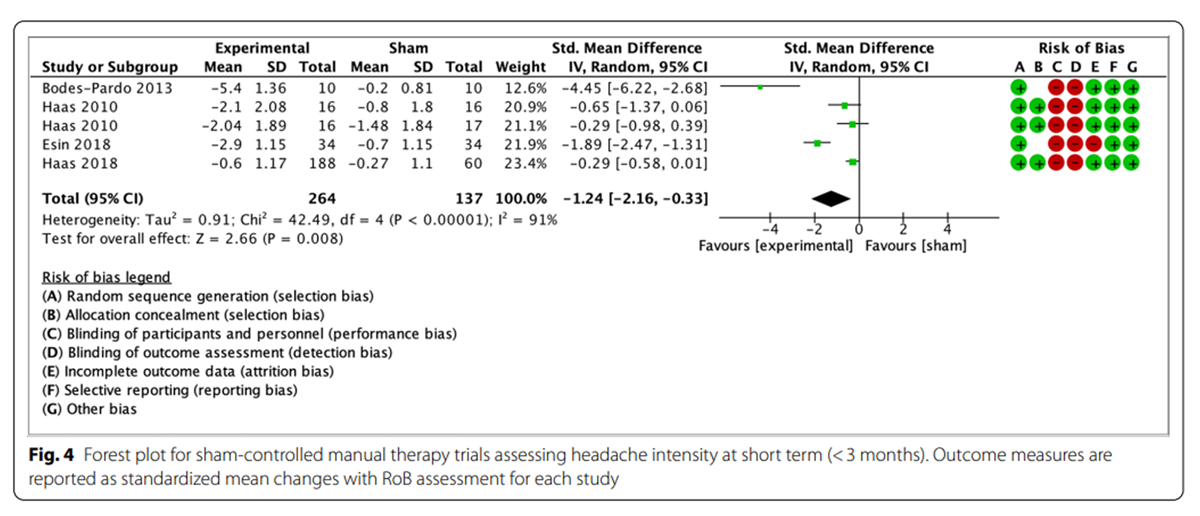
Figure 4

Figure 5
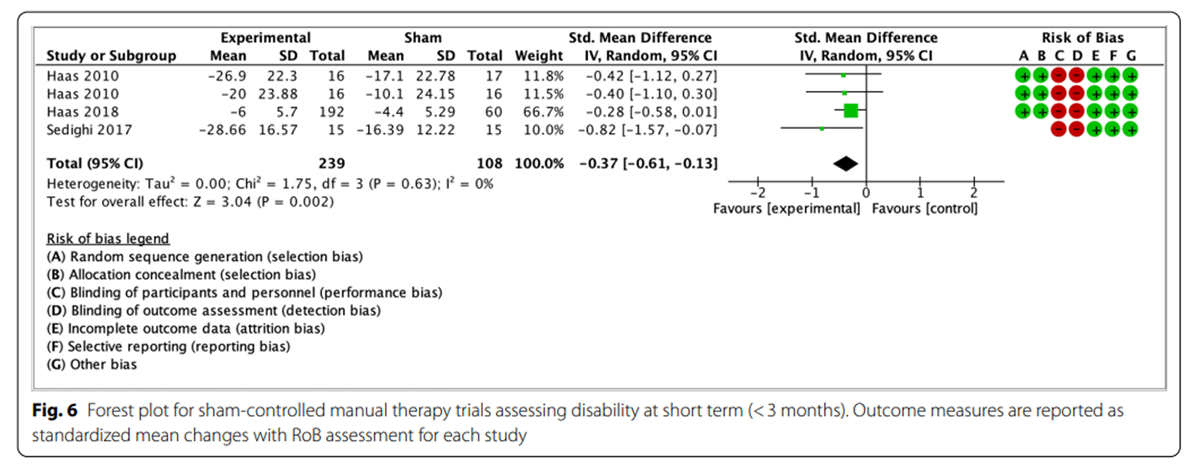
Figure 6
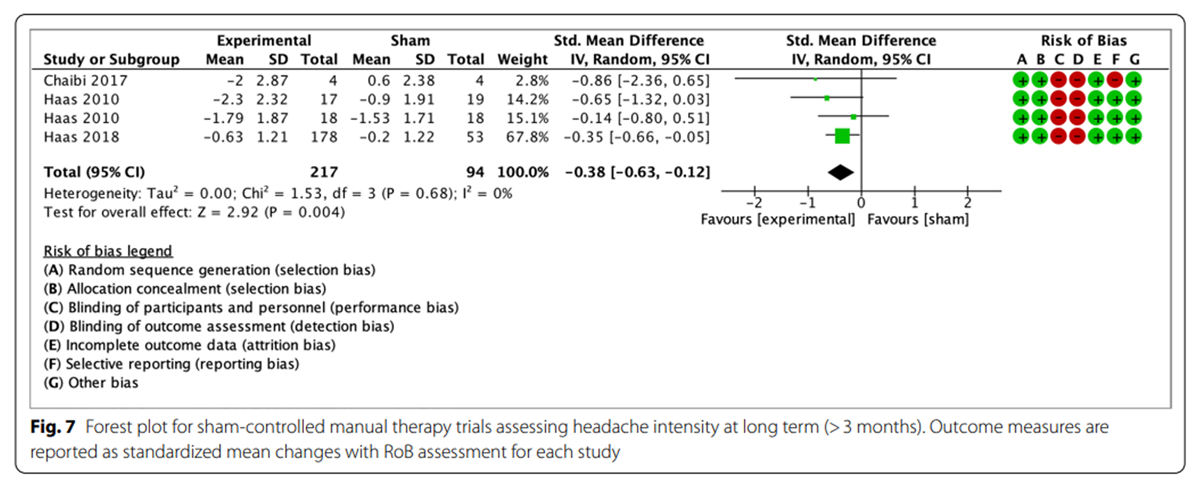
Figure 7

Figure 8
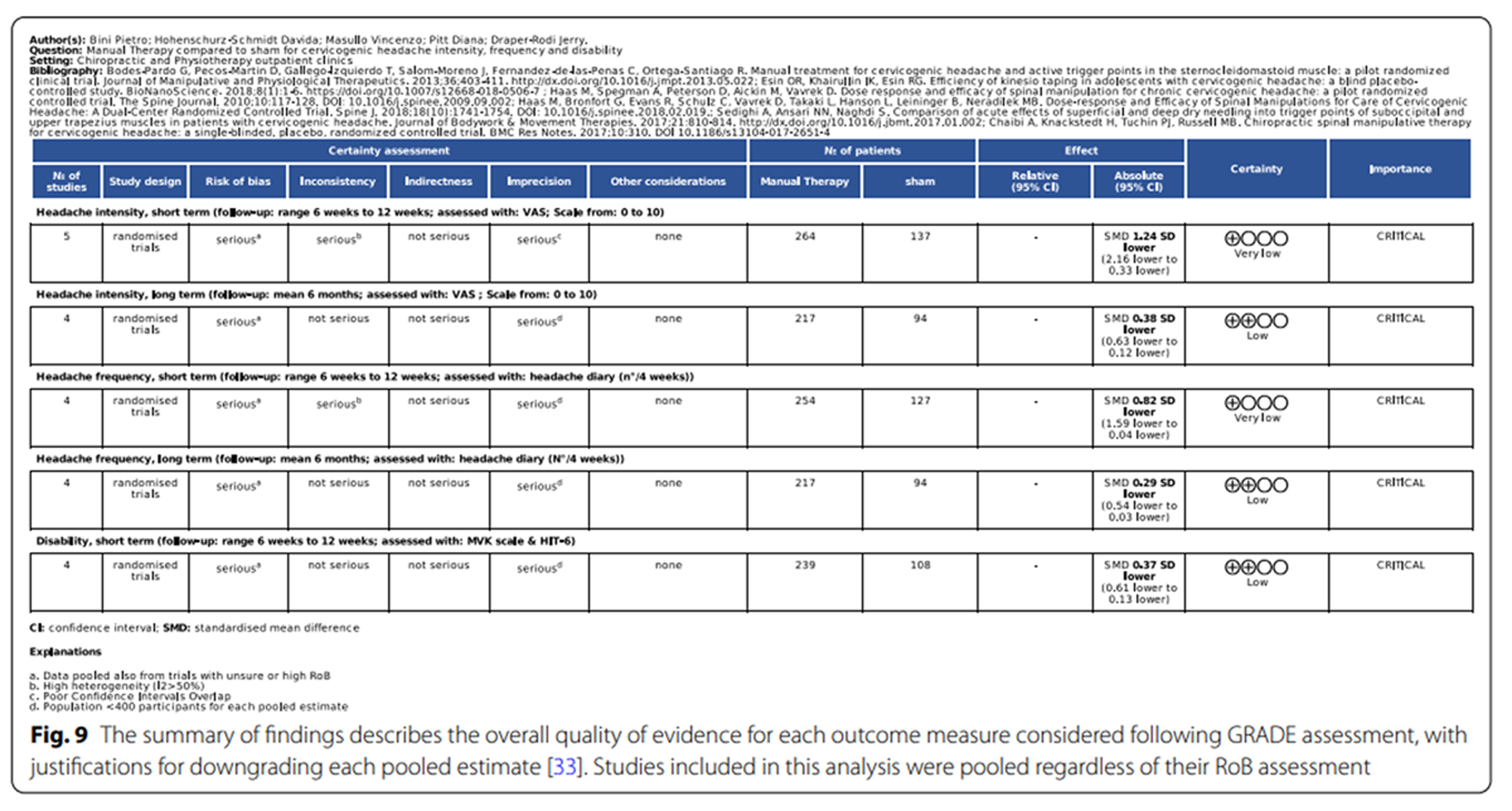
Figure 9
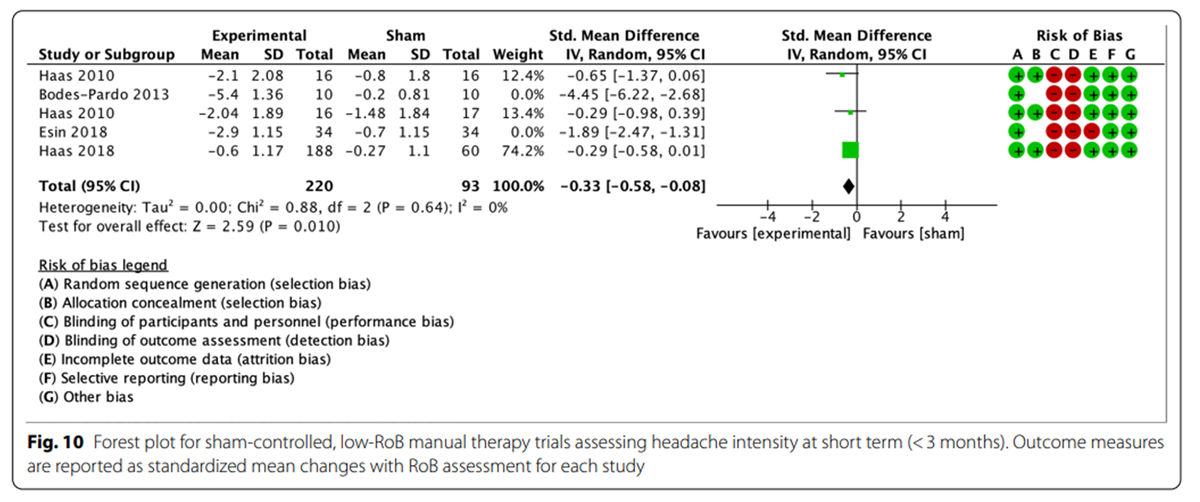
Figure 10
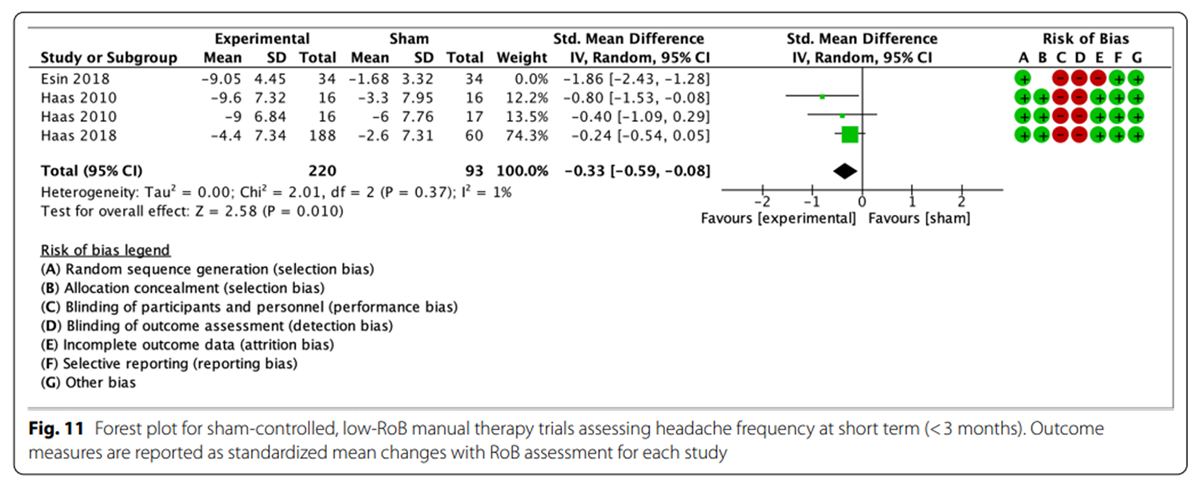
Figure 11
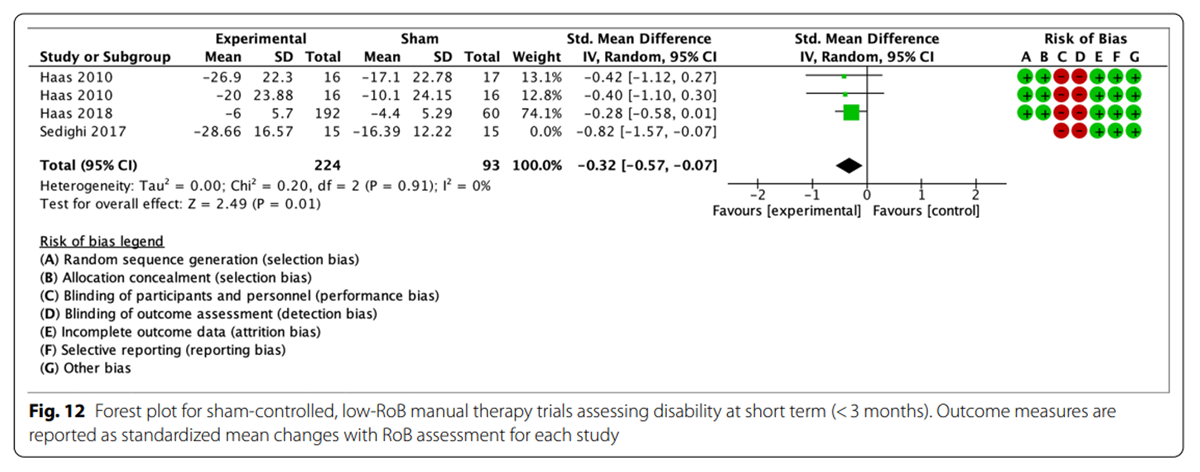
Figure 12
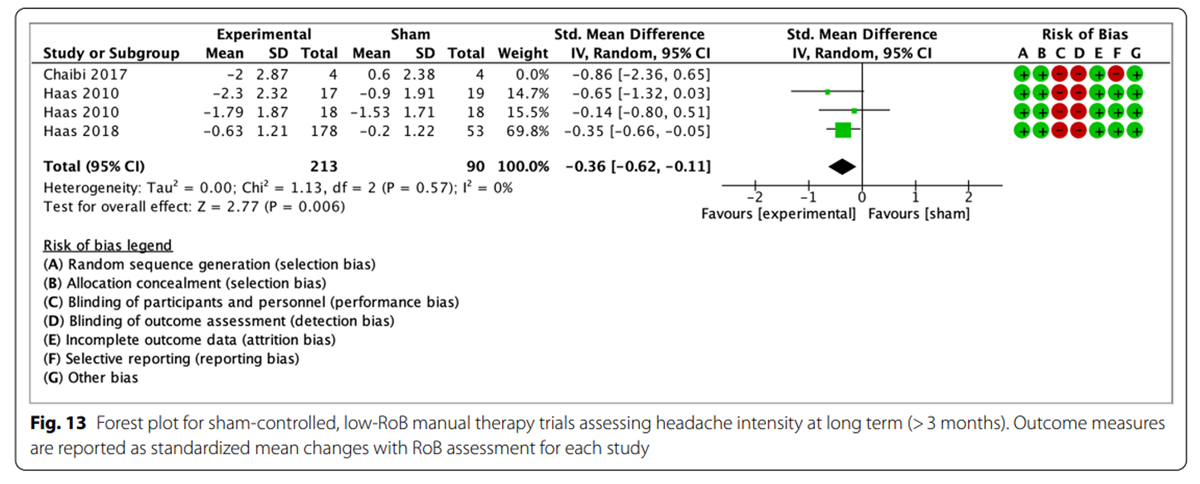
Figure 13
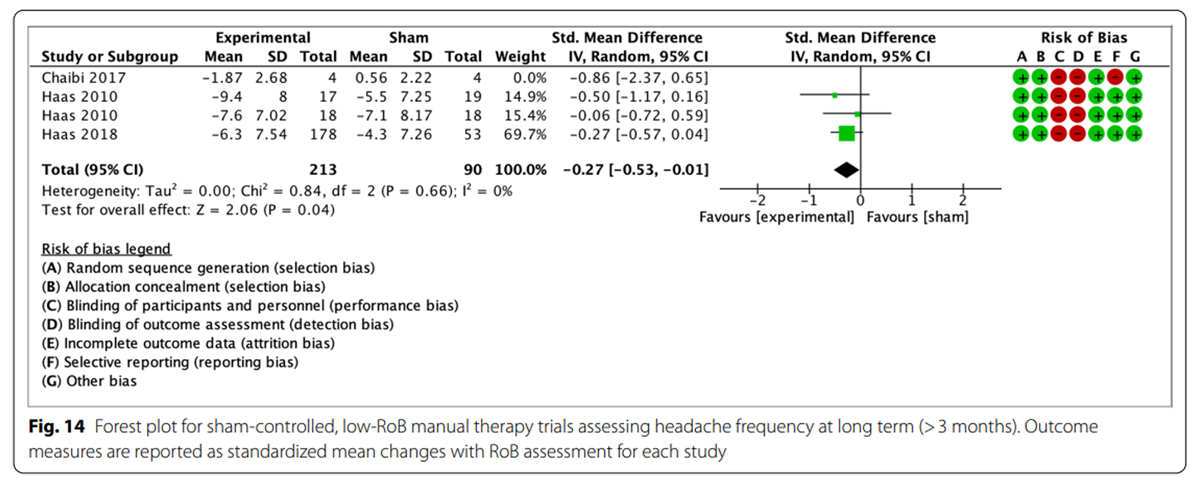
Figure 14
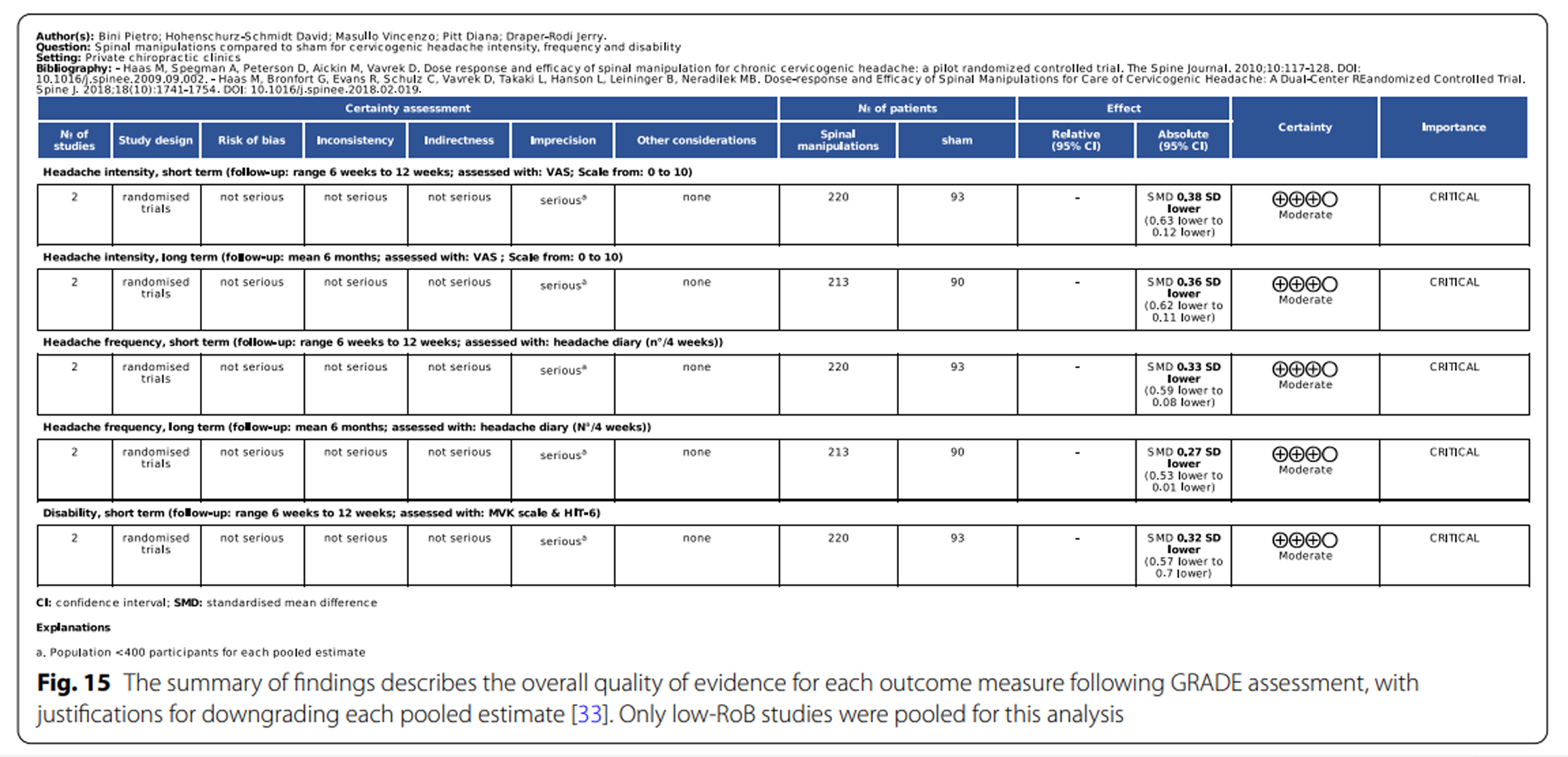
Figure 15 When disability was measured with the NDI, five studies [53, 63, 64, 67, 68] found significant within- and between-group differences favoring experimental interventions (p < 0.05) when compared to “other interventions”. MCIDs were reached in four trials [53, 64, 67, 68], whilst the absence of raw data did not permit analysis of the fifth trial. [63]
Youssef and Shanb and Lerner-Lentz et al. [66, 69] did not find significant between-group differences, although all groups involved in this study had a significant within-group improvement (p < 0.001 and p < 0.05 respectively) and reached the MCID for the NDI.
The two trials by Haas et al. [55, 56] found significant differences favouring spinal manipulation over sham manipulation at 6, 12 and 24 weeks (p < 0.05).
Sedighi et al. [62] found a greater efficacy of dry needling over sham acupuncture at one week after a single application (p < 0.001).
Headache Duration
Headache duration was measured as hours with headache per day or per week. The 2016 and 2018 trials by Dunning et al. [53, 68] found significant improvements after spinal manipulation at one week, four weeks and three months (p < 0.05). Jafari et al. [58] found effectiveness of trigger point therapy in decreasing headache duration at three weeks (p < 0.05). Jull et al. [59] found manual therapy with or without exercise therapy to be more effective than no treatment for headache duration at seven weeks and twelve months (p < 0.05), but low-load endurance exercise was not statistically more beneficial than no treatment (p > 0.05). Sharma et al. [63] found significant effects of mobilization and low-level exercise compared to postural correction and endurance exercise (p = 0.001) at four weeks. Significant improvements (p < 0.05) were also found for the experimental group by Youssef and Shanb [66], comparing cervical mobilization to massage therapy. Graston mobilization were found more effective than therapeutic exercise at four weeks for headache duration (p < 0.001) by Abdel et al. [67]
Meta-analysis
Due to the various differences in the design of included trials, only six studies were deemed comparable in a meta-analysis. [51, 52, 54–56, 62] Specifically, data pooling was only possible for trials with sham controls, as not enough studies were comparing interventions to no-treatment controls or to other active interventions. For the pooled trials, meta-analysis was feasible for headache intensity and frequency both at short and long-term, and for disability at short-term.
As illustrated by the forest plots (Figures 4, 5, 6, 7 and 8), a large effect was found in favour of manual therapy for headache intensity and moderate-to-large effects for headache frequency at short-term. For disability, there was a small-to-moderate effect at short-term. Long-term effects were small-to-moderate for headache intensity and small for headache frequency. The GRADE assessment for the quality of evidence showed very low quality of evidence for Headache Intensity and Frequency at short term (downgraded due to risk of bias, inconsistency, and imprecision), and low quality of evidence for Headache intensity, frequency and disability at long term (downgraded due to risk of bias and imprecision). As none of the comparisons included 10 or more studies, publication bias could not be assessed. [38] The summary of findings table can be found in Figure 9.
Only two trials in the meta-analysis had a low RoB for primary and secondary outcome measures, and both analyzed spinal manipulation. A sensitivity analysis including only these two studies was performed. The trials included groups with different dosages of the same intervention as parallel experimental groups. Haas et al. [55] contributed to data pooling with two comparisons: manipulation vs sham (8 sessions) and manipulation vs sham (16 sessions). For the 2018 trial by Haas et al. [56], means and standard deviations for the three experimental groups were combined, and compared to the single control group. The sensitivity analysis showed small effect sizes at short-term for headache intensity, frequency and disability (Figures 10, 11, 12). Small effects were also found at long-term for headache intensity and frequency (Figures 13, 14). The GRADE assessment [33] showed moderate quality of evidence for the sensitivity analysis results for each comparison. The GRADE evidence table for the sensitivity analysis is presented in Figure 15.
Discussion
The aim of this systematic review and meta-analysis was to assess the effects of manual and exercise therapy on headache intensity, frequency and other headache-related outcomes in patients experiencing CGHs.
Overall, this review found evidence consistently supporting the use of various manual therapy modalities for the management of CGH, based on nineteen RCTs, eight of which with a low RoB for the outcome measures of interest. In particular, there is stronger evidence favoring the use of spinal manipulation, spinal mobilization and Graston technique, while the positive effects of other interventions of interest are supported by fewer, low or unsure-RoB trials.
The meta-analysis of sham-controlled manual therapy trials showed moderate-to-large positive effects for manual therapy in reducing headache intensity, frequency and low-to-moderate positive effects on disability at short-term compared to sham. This meta-analysis also showed small-to-moderate and small positive effects for headache intensity and frequency at long-term. The GRADE assessment showed very low quality of evidence supporting manual therapy for the short-term estimates, and low quality of evidence of the long-term comparisons. A sensitivity meta-analysis including only low-RoB trials showed small effects of spinal manipulation for headache intensity and frequency at short and long-term, and for disability at short-term. The results of the GRADE assessment of the sensitivity meta-analysis showed moderate quality of evidence and can be interpreted as “the authors believe that the true effect is probably close to the estimated effect”. Considering the differences in the GRADE assessment and the resulting quality of evidence between the meta-analysis and the sensitivity analysis, the pooled estimates provide stronger evidence for the efficacy of spinal manipulation than other manual or exercise therapies. In particular, further studies are needed to allow data pooling and to assess the effectiveness of exercise therapy as a stand-alone treatment, but the integration with manual therapy appears to be effective based on relevant combinational trials included in this review. [59, 63, 64, 66–69]
When comparing the results of this systematic review with a previous systematic review that only used conservative care as control [7], we notice that the trials pooled in this previous review were different and led to different results. The lack of effectiveness of spinal manipulation and mobilization reported by the previous systematic review compared to the moderate-size positive effects found in the current meta-analysis, strengthens the importance of comparing the interventions of interest to sham interventions. Another systematic review and meta-analysis [8] found a similar direction of results, although with generally smaller effect sizes for headache intensity, frequency and disability at both short and long term. The smaller effects seen in the [8] review are explained by a different grouping of trials (which included no-treatment comparators), and different treatment of individual trials [55, 56] in its meta-analysis.
Furthermore, the sensitivity analysis included in the present manuscript allows for a more robust interpretation of the effects of spinal manipulation, and provides higher-quality evidence.
Comparing the results of the present review to the clinical indications proposed by Cote et al. in previous guidelines [6], the existing recommendations for the use of manual therapy and exercise are strengthened, especially regarding spinal manipulation and mobilization. In fact, 10 of the 11 included trials of spinal manipulation and mobilization reported clinical and statistical superior effects for the experimental group compared to controls. Contrastingly, the evidence was limited to fewer trials with high or unsure risk of bias for other manual therapy interventions (myofascial trigger point therapy, dry needling, kinesio-taping, Graston technique, Dennerol cervical traction) and for exercise therapy. The guidelines’ manual therapy recommendations are strengthened further by the results of our meta-analysis, while meta-analysis was not feasible for exercise trials. Previous guidelines discourage combinations of manual therapy and low-load endurance cervico-scapular exercise, based on a single high-risk of bias trial. [59]
The present systematic review found that the addition of Graston technique to an exercise plan provided statistical significant improvements compared to the exercise regime alone. [67] Consequently, although these findings are in line with existing guidelines, the evidence seems to suggest that clinicians could consider offering patients a mixed approach which combines manual therapy and stretching, isometric exercises and postural correction.
The Cote et al. guidelines [6] also provide indications on the dosage of such interventions, recommending a maximum of 10 manual therapy sessions. Nonetheless, one trial [56] included in our sensitivity meta-analysis reported a higher efficacy of spinal manipulation at 18 sessions, compared to 12 or 6 sessions. Consequently, although this systematic review confirms that spinal manipulation is the intervention with the greatest amount and quality of evidence available, a higher dose of interventions may be necessary to obtain statistically and clinically significant improvements, which contrasts with previous guidance.
Shared decision-making and patient education should be the basis of choosing an intervention, as per current literature and CGH guidelines. [6] To facilitate this process, the present review also considered MCIDs and adverse events wherever possible. MCIDs could be used to contextualize the review’s findings for three outcome measures (headache intensity with NPRS, headache frequency, disability measured by the NDI). To be meaningful to patients, changes in NPRS and NDI need to be at least 2.5 and 5.5 points [16], respectively, within four weeks; recognizing, however, that meaningfulness likely differs between groups of patients and that more research on context-sensitive MCIDs may be required. In the reviewed studies, MCIDs were largely reached, despite treatment intensities and dosages varying widely. Considering the context and time required to achieve the clinical benefits observed in the present review, the magnitude of the changes seems to justify the resources.
Weighing intervention risks against patient-perceived benefits, it has been reported that up to 50% of patients receiving manual therapy can experience transient mild adverse effects. These are generally self-resolving within 48–72 h, which is lower than the risk with most drug therapies. [13] The incidence of adverse events reported in the included trials is well below 50%, and no serious adverse events were reported. While such data underlines the relative safety of manual therapy for CGH, patients should be informed about the possibility of experiencing transient adverse effects. Considering the results of this systematic review, the authors recommend that practitioners discuss with patients the available evidence regarding the effectiveness of manual and exercise therapy and alternative interventions as well as their costs and risks. This will promote realistic expectations for people experiencing CGH, supporting them to make an informed decision about their health.
To the authors’ knowledge, this is the first systematic review and meta-analysis of CGH trials to assess such a wide range of interventions and to analyze trials using different control interventions, which makes it the most comprehensive review available on CGH. Furthermore, the rigorous data pooling methodology, the presence of a sensitivity analysis based on low-RoB trials only, the thorough analysis of each trial and their MCIDs as well as the various GRADE assessments for each of the pooled estimates, allow a more specific interpretation of the findings, compared to previous systematic reviews and meta-analyses on this topic. Limitations to this review were the exclusion of trials in Chinese, the limited number of published trials, small group sizes, and the prevalence of trials with unclear or high RoB. Differences in trial design (notably choice of comparators and treatment dosage) limited the number of studies that could be pooled for meta-analysis.
A notable challenge in trial design in the field of manual therapy and exercise therapy research is the intrinsic difficulty in patient and therapist blinding, and a limitation to this systematic review is that the included trials rarely evaluated the patient-blinding effectiveness. Consequently, even in sham-controlled trials it remains unclear whether the influence of patient expectations was adequately controlled. [20-22] Some of the included trials had further specific limitations. In both trials assessing trigger point therapy [51, 58], participants were included only when showing signs of a trigger point at the sternocleidomastoid muscle, which might not be representative of all people living with CGH and could limit the generalizability of these conclusions.
Similarly, the presence of TMJ dysfunction as inclusion criterion in the trial by von Piekartz et al. [64] decreases the generalizability of the findings, although the results can be considered when making treatment recommendations specific to patients with TMJ dysfunction. Considering the concerns about methodological and reporting quality of the trial by Yang and Kang [65], it is the opinion of the authors of this systematic review that no conclusions should be drawn from this study.
Furthermore, only trials on spinal manipulation were included in the sensitivity meta-analysis, restricting the relevance of the meta-analysis to this particular intervention. Another common limitation in trials on physical therapy is that the standardized treatment procedures described in the intervention groups seldom reflect common practice, where the choice of the intervention is specific to the patient, rather than being standardized across patients. This can limit the translatability of guidelines to clinical practice. [71] A further limitation is that only 11 of the included trials were excluding participants with co-existing headaches, which could have similar characteristics to CGH and confound trial results. This and the considerable overlap across headache types in various diagnostic classifications, pose a considerable limitation to the systematic review.
Nonetheless, it could be argued that due to the diagnostic challenges, this limitation might be considered inherent to headache trials. [12] In addition, 60% of the trials did not provide data on adverse events, which might keep readers unaware of possible major or minor complications experienced by participants. Considering the limitations described and the low-to-moderate quality of evidence found with GRADE, further *16 RCTs are expected and necessary to clarify the role of manual and exercise therapy, especially for interventions other than spinal manipulation. In order to generate more comparable and high-quality evidence for these interventions for CGH, future primary research on this topic should consider the limitations encountered in this systematic review.
Conclusion
Manual therapy (with or without exercise therapy) appears to be a safe and effective intervention for CGH, and should be considered in the management of this condition, as already proposed by the latest guidelines. [6] The main body of evidence favours the use of spinal manipulation to reduce headache intensity, frequency and disability, but other forms of manual therapy and exercise therapy were found to be consistently beneficial for other outcomes across the trials.
Future research with low-RoB RCTs, higher numbers of participants, better-defined headache populations, and more homogeneous trial designs is necessary to confirm these findings. The relevance for clinical practice is considerable, as reflected by the amount of clinical guidelines proposing some form of manual or physical therapy in the management of headaches, and the large number of patients seeking this type of intervention to manage their headache symptoms.
Abbreviations
CGH = Cervicogenic headache
RCT = Randomized controlled trial
PRISMA = Preferred reporting items for systematic review and meta-analysis
PICO = Population intervention comparison outcome(s)
GRADE = Grading of recommendations, assessment, development and evaluations
RoB = Risk of bias
SMD = Standard mean difference
NPRS = Numeric pain rating scale
VAS = Visual analogue scale
NDI = Neck disability index
CROM = Cervical range of motion
CAS = Coloured analogue scale
MCID = Minimal clinically important difference
SNAG = Self-sustained naural apophyseal glide
TMJ = Temporo-mandibular joint
Author contributions
PB, DP, DHS and JDR conceived the idea for the study and contributed to the design and planning of the research. PB and VM collected and analyzed the data. PB wrote the first draft of the manuscript. DP, VM, DHS and JDR had a critical role in the revision of the manuscript. All authors read and approved the final version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare that they have no competing interests.
References:
Al Khalili Y, Ly N, Murphy PB.
Cervicogenic headache.
Treasure Island (FL): StatPearls Publishing; 2020ICHD: Headache Classification Subcommitee of the International Headache Society
The international classification of headache disorders.
Cephalalgia. 2018;38(1):1–211.
doi: 10.1177/0333102417738202Sjaastad O, Fredriksen TA, Pfaffenrath V.
Cervicogenic headache: diagnostic criteria.
Headache. 1998;38(6):442–445.
doi: 10.1046/j.1526-4610.1998.3806442.xSjaastad O, Fredriksen T, Pareja JA, et al.
Coexistence of cervicogenic headache and migraine without aura (?)
Funct Neurol. 1999;14:209–218Moore CS, Sibbritt DW, Adams J.
A critical review of manual therapy use for headache disorders:
prevalence, profiles, motivations, communication and
self-reported effectiveness.
BMC Neurol. 2017;17:1–11.
doi: 10.1186/s12883-017-0835-0Cote P, Yu H, Shearer HM, Randhawa K, Wong JJ, Mior S, Ameis A, Carroll LJ, Nordin M. et al.
Non-pharmacological Management of Persistent Headaches Associated
with Neck Pain: A Clinical Practice Guideline from the
Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration
European Journal of Pain 2019 (Jul); 23 (6): 1051–1070Coelho M, Ela N, Garvin A, Cox C, Sloan W, Palaima M, Cleland JA.
The effectiveness of manipulation and mobilization on pain and disability
in individuals with cervicogenic and tension-type headaches:
a systematic review and meta-analysis.
Phys Ther Rev. 2019;24(1–2):12–28.
doi: 10.1080/10833196.2019.1572963Fernandez M, Moore C, Tan J, Lian D, Nguyen J, Bacon A, Christie B, Shen I.
Spinal Manipulation for the Management of Cervicogenic Headache:
A Systematic Review and Meta-analysis
European Journal of Pain 2020 (Oct); 24 (9): 1687–1702Freedland KE, King AC, Ambrosius WT, Mayo-Wilson E, Mohr DC, Czajkowski SM.
The selection of comparators for randomized controlled trials of
health-related behavioral interventions: recommendations
of a NIH expert panel.
J Clin Epidemiol. 2019;110:74–81.
doi: 10.1016/j.jclinepi.2019.02.011Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffman TC, Mulrow CD, et al.
The PRISMA 2020 statement: an upgraded guideline
for reporting systematic reviews.
BMJ. 2021;372:n71.
doi: 10.1136/bmj.n71Santos CMC, Pimenta CAM, Nobre MRC.
The PICO strategy for the research question construction and evidence search.
Rev Latino-Am Enfermagem. 2007;15(3):508–511.
doi: 10.1590/s0104-11692007000300023Luedtke K, Allers A, Schulte LH, May A.
Efficacy of interventions used by physiotherapists for patients with
headache and migraine-systematic review and meta-analysis.
Cephalalgia. 2016;36:474–492.
doi: 10.1177/0333102415597889Carnes D, Mars TS, Mullinger B, Froud R, Underwood M.
adverse events and manual therapy: a systematic review.
Man Ther. 2010;15:355–363.
doi: 10.1016/j.math.2009.12.006Bielecki JE, Tadi P.
Therapeutic exercise.
Treasure Island (FL): StatPearls Publishing; 2022Luedtke K, Basener A, Bedei S, Castien R, Chaibi A, Falla D, et al.
Outcome Measures for Assessing the Effectiveness of
Non-pharmacological Interventions in Frequent
Episodic or Chronic Migraine: A Delphi Study
BMJ Open. 2020 (Feb 12); 10 (2): e029855Young IA, Dunning J, Butts R, Cleland JA, Fernandez-de-las-Penas C.
Psychometric properties of the numeric pain rating scale and
neck disability index in patients with cervicogenic headache.
Cephalalgia. 2019;39(1):44–51.
doi: 10.1177/0333102418772584Covidence, https://www.covidence.org/; 2022 [accessed 10th-01–2022].
McHugh ML.
Interrater reliability: the kappa statistic.
Biomech Med. 2012;22(3):276–282Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, Bronfort G, van Tulder MW.
2015 updated method guideline for systematic reviews
in the cochrane back and neck group.
Spine. 2015;40(21):1660–1673.
doi: 10.1097/BRS.0000000000001061Hohenschurz-Schmidt D, Draper-Rodi J, Vase L, Scott W, McGregor A, et al.
Blinding and sham control methods in trials of physical, psychological,
and self-management interventions for pain (article I):
a systematic review and description of methods.
Pain. 2022
doi: 10.1097/j.pain.0000000000002723Hohenschurz-Schmidt D, Draper-Rodi J, Vase L, Scott W, McGregor A, et al.
Blinding and sham control methods in trials of physical, psychological,
and self-management interventions for pain (article II):
a meta-analysis relating methods to trial results.
Pain. 2022
doi: 10.1097/j.pain.0000000000002730Armijo-Olivo S, Fuentes J, da Costa BR, Saltaji H, Ha C, Cummings GG.
Blinding in physical therapy trials and its association with treatment effects.
Am J Phys Med Rehabil. 2017;96(1):34–44.
doi: 10.1097/PHM.0000000000000521Viswanathan M, Ansari MT, Berkman ND, Chang S, Hartling L, McPheeters M et al.
Assessing the risk of bias of individual studies
in systematic reviews of health care interventions. 2012.
In: Methods guide for effectiveness and comparative effectiveness reviews [Internet].
Rockville (MD): Agency for Healthcare Research and Quality (US); 2008-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK91433/
(Accessed 1st July 2022)Salas Apasa JA, Ariel Franco JV, Meza N, Madrid E, Loezar C, Garegnani L.
Minimal clinically importance difference: the basics.
Medwave. 2021;21(03):e8149.
doi: 10.5867/medwave.2021.03.8149Hawker GA, Mian S, Kendzerska T, French M.
Measures of adult pain: visual analog scale for pain (VAS pain),
numeric rating scale for pain (NRS Pain), McGill pain
questionnaire (MPQ), short-form McGill pain questionnaire
(SF-MPQ), chronic pain grade scale (CPGS), short form-36
bodily pain scale (SF-36 BPS), and measure of
intermittent and constant osteoarthritis pain (ICOAP)
Arthritis Care Res. 2011;63(S11):S240–S252.
doi: 10.1002/acr.20543Fleming R, Forsythe S, Cook C.
Influential variables associated with outcomes
in patients with cervicogenic headache.
J Man Manip Ther. 2007;15(3):155–164.
doi: 10.1179/106698107790819846McGrath P, Seifert CE, Speechley KN, Booth JC, Stitt L, Gibson MC.
A new analogue scale for assessing children’s pain:
an initial validation study.
Pain. 1996;64:435–443.
doi: 10.1016/0304-3959(95)00171-9Underwood MR, Barnett AG, Vickers MR.
Evaluation of two time-specific back pain outcome measures.
Spine. 1999;42(11):1104–1112.
doi: 10.1097/00007632-199906010-00010Jull GA, Stanton WR.
Predictors of responsiveness to physiotherapy
management of cervicogenic headache.
Cephalalgia. 2004;25:101–108.
doi: 10.1111/j.1468-2982.2004.00811.xReview Manager (RevMan)
[Computer program]. Version 5.4.
The Cochrane Collaboration, 2020Cohen J.
Statistical power analysis for the behavioral sciences. 2.
Hillside, NJ: Lawrence Erlbaum Associates; 1988Bronfort G, Nilsson N, Haas M, Evans RL, Goldsmith CH, Assendelft WJJ, Buter LM.
Non-invasive physical treatments for chronic/recurrent headache.
Cochrane Database Syst Rev. 2004;3:CD001878.
doi: 10.1002/14651858.CD001878.pub2Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S. et al.
GRADE guidelines: 1. Introduction-GRADE evidence profiles
and summary of findings tables.
J Clin Epidemiol. 2011;64:383–394.
doi: 10.1016/j.jclinepi.2010.04.026Guyatt G, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P. et al.
GRADE guidelines 4: rating the quality of evidence-
study limitations (risk of bias)
J Clin Epidemiol. 2011;64:407–415.
doi: 10.1016/j.jclinepi.2010.07.017Guyatt G, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M.
GRADE guidelines 7: rating the quality of evidence - inconsistency.
J Clin Epidemiol. 2011;64:1294–1302.
doi: 10.1016/j.jclinepi.2011.03.017Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, Devereaux PJ. et al.
GRADE guidelines 6: rating the quality of evidence - imprecision.
J Clin Epidemiol. 2011;64:1283–1293.
doi: 10.1016/j.jclinepi.2011.01.012Guyatt G, Oxman AD, Kunz R, Woddocock J, Brozek J, Helfand M. et al.
GRADE guidelines 8: rating the quality of evidence - indirectness.
J Clin Epidemiol. 2011;64:1303–1310.
doi: 10.1016/j.jclinepi.2011.04.014Higgins JPT, Thomas J, Chandler J, Cumpston M.
Cochrane handbook for systematic reviews of interventions. 2.
Chichester, UK: John Wiley & Sons; 2019Guyatt G, Oxman AD, Vist G, Kunz R, Falck-Ytter Y, Alonso-Coello P.
GRADE: an emerging consensus on rating quality of evidence
and strength of recommendations.
BMJ. 2008;336:924–926.
doi: 10.1136/bmj.39489.470347.ADLangevin P, Fait P, Frémont P, Roy JS.
Cervicovestibular rehabilitation in adult with mild traumatic
brain injury: a randomised controlled trial protocol.
BMC Sports Sci Med Rehabil. 2019;11:25.
doi: 10.1186/s13102-019-0139-3Svedmark A, Djupsjöbacka M, Häger C, Jull G, Björklund M.
Is Tailored treatment superior to non-tailored treatment for pain
and disability in women with non-specific neck pain?
a randomized controlled trial.
BMC Musculoskelet Disord. 2016;17(1):408.
doi: 10.1186/s12891-016-1263-9Vernon H, Borody C, Harris G, Muir B, Goldin J, Dinulos M.
A randomized pragmatic clinical trial of chiropractic care
for headaches with and without a self-acupressure pillow.
J Manip Physiol Ther. 2015;38(9):637–643.
doi: 10.1016/j.jmpt.2015.10.002Daher A, Carel RS, Tzipi K, Esther H, Dar G.
The effectiveness of an aerobic exercise training on patients with
neck pain during a short- and long-term follow-up:
a prospective double-blind randomized controlled trial.
Clin Rehabil. 2020;34(5):617–629.
doi: 10.1177/0269215520912000Ylinen J, Nikander R, Nykänen M, Kautiainen H, Häkkinen A.
Effect of neck exercises on cervicogenic headache:
a randomized controlled trial.
J Rehabil Med. 2010;42(4):344–349.
doi: 10.2340/16501977-0527Whittingham W, Nilsson N.
Active range of motion in the cervical spine
increases after spinal manipulation (toggle recoil)
J Manipulative Physiol Ther. 2001;24(9):552–555.
doi: 10.1067/mmt.2001.118979Ramezani E, Arab AM.
The effect of suboccipital myofascial release technique on cervical
muscle strength of patients with cervicogenic headache.
PTJ. 2017;7(1):19–28.
doi: 10.29252/nrip.ptj.7.1.19von Piekartz H, Hall T.
Orofacial manual therapy improves cervical movement impairment associated
with headache and features of temporomandibular dysfunction:
a randomized controlled trial.
Man Ther. 2013;18(4):345–350.
doi: 10.1016/j.math.2012.12.005Haas, M, Aickin, M, and Vavrek, D.
A Preliminary Path Analysis of Expectancy and Patient-Provider
Encounter in an Open-Label Randomized Controlled Trial of
Spinal Manipulation for Cervicogenic Headache
J Manipulative Physiol Ther 2010 (Jan); 33 (1): 5—13Borusiak P, Biedermann H, Bosserhoff S, Opp J.
Lack of efficacy of manual therapy in children and adolescents with
suspected cervicogenic headache: results of a prospective,
randomized, placebo-controlled, and blinded trial.
Headache. 2010;50(2):224–230.
doi: 10.1111/j.1526-4610.2009.01550.xKhan M, Shahzad S, Soomro RR.
Efficacy of C1–C2 sustained natural apophyseal glide (SNAG) versus
posterior anterior vertebral mobilization (PAVMs) in the
management of cervicogenic headache.
J Basic Appl Sci. 2014;10:226–230.
doi: 10.6000/1927-5129.2014.10.31Bodes-Pardo G, Pecos-Martín D, Gallego-Izquierdo T, Salom-Moreno J.
Manual Treatment for Cervicogenic Headache and Active Trigger Point
in the Sternocleidomastoid Muscle: A Pilot Randomized Clinical Trial
J Manipulative Physiol Ther. 2013 (Sep); 36 (7): 403—411Chaibi A, Knackstedt H, Tuchin PJ, Russell MB.
Chiropractic Spinal Manipulative Therapy for Cervicogenic Headache:
A Single-blinded, Placebo, Randomized Controlled Trial
BMC Res Notes. 2017 (Jul 24); 10 (1): 310Dunning JR, Butts R, Mourad F, Young I, Fernandez-de-las-Penas C.
Upper Cervical and Upper Thoracic Manipulation Versus Mobilization
Exercise in Patients with Cervicogenic Headache: A Multi-center
Randomized Clinical Trial
BMC Musculoskelet Disord. 2016 (Feb 6); 17 (1): 64Esin OR, Khairullin IK, Esin RG.
Efficiency of kinesio taping in adolescents with
cervicogenic headache: a blind placebo-controlled study.
BioNanoScience. 2018;8(1):1–6.
doi: 10.1007/s12668-018-0506-7Haas M, Spegman A, Peterson D, Aickin M, Vavrek D.
Dose Response and Efficacy of Spinal Manipulation for Chronic
Cervicogenic Headache: A Pilot Randomized Controlled Trial
Spine J. 2010 (Feb); 10 (2): 117–128Haas M, Bronfort G, Evans R, Schulz C, Vavrek D, Takaki L, Hanson L.
Dose-Response and Efficacy of Spinal Manipulation for Care of
Cervicogenic Headache: A Dual-Center
Randomized Controlled Trial
Spine J. 2018 (Oct); 18 (10): 1741–1754Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K.
Efficacy of a C1–C2 Self-sustained natural apophyseal glide
(SNAG) in the management of cervicogenic headache.
J Orthop Sports Phys Ther. 2007;37(3):100–107.
doi: 10.2519/jospt.2007.2379Jafari M, Bahrpeyma F, Togha M.
Effect of ischemic compression for cervicogenic headache and elastic
behavior of active trigger point in the sternocleidomastoid
muscle using ultrasound imaging.
J Bodyw Mov Ther. 2017;21(4):933–939.
doi: 10.1016/j.jbmt.2017.01.001Jull G, Trott P et al.
A Randomized Controlled Trial of Exercise and
Manipulative Therapy for Cervicogenic Headache
Spine (Phila Pa 1976) 2002 (Sep 1); 27 (17): 1835—1843Malo-Urričs M, Tricas-Moreno JM, Estebanez-de-Miguel E.
Immediate effects of upper cervical translatoric mobilization on cervical
mobility and pressure pain threshold in patients with
cervicogenic headache: a randomized controlled trial.
J Manip Physiol Ther. 2017;40(9):649–658.
doi: 10.1016/j.jmpt.2017.07.007Nilsson N, Christensen HW, Hartvigsen J.
The Effect of Spinal Manipulation in
the Treatment of Cervicogenic Headache
J Manipulative Physiol Ther 1997 (Jun); 20 (5): 326–330Sedighi A, Ansari NN, Naghdi S.
Comparison of acute effects of superficial and deep dry needling into
trigger points of suboccipital and upper trapezius muscles
in patients with cervicogenic headache.
J Bodyw Mov Ther. 2017;21:810–814.
doi: 10.1016/j.jbmt.2017.01.002Sharma A, Hameed UA, Grover S.
Multimodal therapy in cervicogenic headache- a randomized controlled trial.
Indian J Physiother Occup Ther. 2011;5(1):9–13Von Piekartz H, Luedtke K.
Effect of treatment of temporomandibular disorders (TMD) in patients
with cervicogenic headache: single-blind, randomized controlled study.
Cranio J Craniomandib Pract. 2011;29(1):43–56.
doi: 10.1179/crn.2011.008Yang DJ, Kang DH.
Comparison of muscular fatigue and tone of neck according to craniocervical
flexion exercise and suboccipital relaxation in cervicogenic headache patients.
J Phys Ther Sci. 2017;29(5):869–873.
doi: 10.1589/jpts.29.869Youssef EF, Shanb AA.
Mobilization versus massage therapy in the treatment
of cervicogenic headache: a clinical study.
J Back Musculoskelet Rehabil. 2013;26:17–24.
doi: 10.3233/BMR-2012-0344Abdel-Aal NB, Elsayyad MM, Megahed AA.
Short-term effect of adding Graston technique to exercise program in treatment of patients with cervicogenic headache:
a single-blinded, randomized controlled trial.
Eur J Phys Rehabil Med. 2021;57(5):758–766.
doi: 10.23736/s1973-9087.21.06595-3Dunning J, Butts R, Zacharko N, Fandry K, Young I, Wheeler K.
Spinal manipulation and perineural electrical dry needling in patients
with cervicogenic headache: a multicenter randomized clinical trial.
Spine J. 2021;21(2):284–295.
doi: 10.1016/j.spinee.2020.10.008Lerner-Lentz A, O’Halloran B, Donaldson M, Cleland JA.
Pragmatic application of manipulation versus mobilization to the upper
segments of the cervical spine plus exercise for treatment of
cervicogenic headache: a randomized clinical trial.
J Man Manip Ther. 2021;29(5):267–275.
doi: 10.1080/10669817.2020.1834322Moustafa IM, Diab A, Shousha T, Harrison DE.
Does restoration of sagittal cervical alignment improve cervicogenic
headache pain and disability: a 2-year pilot
randomized controlled trial.
Heliyon. 2021;7(3):E06467.
doi: 10.1016/j.heliyon.2021.e06467Vander Schaaf EB, Seashore CJ, Randolph GD.
Translating clinical guidelines into practice: challenges and
opportunities in a dynamic health care environment.
NCMJ. 2015;76(4):230–234.
doi: 10.18043/ncm.76.4.230.
Return to CERVICOGENIC HEADACHE
Since 11-02-2022
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |