

The Diagnosis and Treatment of Chronic Back Pain by
Acupuncturists, Chiropractors, and Massage TherapistsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Clinical J Pain 2006 (Mar); 22 (3): 227-234 ~ FULL TEXT
OPEN ACCESS Karen J. Sherman, PhD, MPH • Daniel C. Cherkin, PhD • Richard A. Deyo, MD, MPH
Janet H. Erro, RN, MN, PNP • Andrea Hrbek • Roger B. Davis, ScD • David M. Eisenberg, MD
Center for Health Studies,
Group Health Cooperative,
Seattle, Washington 98101, USA.
![]()
Objectives: To describe the diagnostic and therapeutic content of visits for chronic back pain to acupuncturists, chiropractors, and massage therapists.
Methods: Randomly selected acupuncturists, chiropractors, and massage therapists in two states were surveyed, and then eligible providers collected data on consecutive patient visits. The authors analyzed information on diagnosis, treatment, and self-care recommendations for chronic back pain patients collected during consecutive patient visits to these complementary and alternative medicine (CAM) providers.
Results: Back pain was the most common reason for visits to each of these providers, with chronic back pain representing about 10% of visits to acupuncturists, 20% of visits to chiropractors, and 12% of visits to massage therapists.Diagnosis by acupuncturists included traditional questioning and inspecting the patient as well as pulse and tongue assessment and palpation of the acupuncture meridians. Treatments usually included acupuncture needling, heat of some sort, and other modalities, such as East Asian massage, herbs, and/or cupping (application of suction cups to the skin). Lifestyle recommendations were common, particularly exercise and dietary counseling.
Visits to chiropractors usually included spinal and muscle/soft tissue examinations and spinal manipulation. Soft tissue techniques (eg, "active release"), stretch or strength training, and home exercise recommendations were much less common.
Massage therapists usually performed a tissue assessment and commonly assessed range of motion. They emphasized Swedish, deep tissue, and trigger point massage techniques and usually made self-care recommendations, particularly increased water intake, hot/cold therapy, exercise, and body awareness.Conclusion: Information on the care patients routinely receive from CAM providers will help physicians better understand these increasingly popular forms of care.
Key Words: acupuncture, chiropractic, massage, office visits, low back pain
From the FULL TEXT Article:
Background
Despite the long-standing major public health impact of chronic back pain, there are still few proven treatments for this condition. [1] As a result, patients are often frustrated with conventional care for back pain, [2] and they are turning increasingly to complementary and alternative medicine (CAM). Chiropractors, massage therapists, and acupuncturists are the most common CAM providers treating patients with back pain in the United States, [3, 4] but there is little reliable information about the care they provide. Moreover, back pain is the most common condition these providers treat. [5] This paper describes the types of diagnostic and assessment techniques, treatment modalities, and self-care recommendations used during consecutive visits for chronic back pain to randomly selected samples of licensed acupuncturists, chiropractors, and massage therapists in each of two states.
METHODS
Study Goals
The data presented in this paper were collected as part of a larger study of four CAM professions (acupuncture, chiropractic, massage, and naturopathy) and their practices. We focused on chronic back pain because these analyses were conducted in the course of developing protocols for clinical studies of chronic back Due to limited resources, we were unable to analyze the data for acute back pain. The methods in the original study, previously described in detail, [5, 6] are summarized below for acupuncture, chiropractic, and massage. We surveyed each of the CAM professions in one Western and one Northeastern state: acupuncturists in Massachusetts and Washington; chiropractors in Arizona and Massachusetts; and massage therapists in Connecticut and Washington. Our goal was to obtain data on 20 consecutive visits from 50 randomly selected providers from each profession in both states who saw at least a minimal number of patients per week. Thus, acupuncturists seeing at least 10 patients per week, chiropractors seeing at least 30 patients per week, and massage therapists seeing at least 5 patients per week were eligible for this study. These criteria represented more than 98% of visits to these professions in each state. [5] While we met our goals of obtaining at least 1000 visits for acupuncturists, chiropractors, and massage therapists in each state, analyses in this report were restricted to those visits where the patient’s primary complaint was back pain, the provider indicated that the major reason for the visit was a "chronic problem," and all of the provider’s care during the visit was provided as part of his or her acupuncture, chiropractic, or massage license.
Sampling and Eligibility of Licensed Providers
Initially, we randomly sampled providers from state licensure lists in 1998 (Washington) or 1999 (Arizona, Connecticut, Massachusetts) and confirmed they were practicing in those states and had identifiable phone numbers. The proportion of licensed providers who were found to be ineligible ranged from 6% for Massachusetts chiropractors to 47% for Connecticut massage therapists. Lack of an identifiable phone number was the predominant reason for ineligibility of acupuncturists in Massachusetts (34%) and massage therapists in Connecticut (39%), while not being in practice was more common in the other samples. Sampled providers were sent letters signed by local leaders in their professions inviting them to participate in a phone interview about their training, demographic profile, and practice characteristics. The response rate for interviews was only 61% for Arizona chiropractors but ranged between 84 and 91% for the other professions and states. [6]
We asked all survey participants with high weekly visit volumes (ie, acupuncturists: 20+ visits per week; chiropractors: 60+ visits per week; massage therapists: 10+ visits per week) and a sample of those with low weekly visit volumes (ie, acupuncturists: 10–19 visits per week; chiropractors: 30–59 visits per week; massage therapists: 5–9 visits per week) to collect data on 20 consecutive patient visits. Sampling weights were used to adjust final estimates to reflect the actual distribution of visits in each state (see Analysis section below).
Data Collection
After approval from the Group Health, University of Washington, and Beth Israel Deaconess Institutional Review Boards, we collected visit data in 1998 (Washington) and 1999 (Arizona, Connecticut, and Massachusetts). We gave practitioners blank visit forms marked with unique identification codes and asked them to record data on 20 consecutive visits (even if the same patient was seen more than once). We asked practitioners to begin data collection on a randomly assigned weekday and to continue until all 20 forms had been completed.
We modeled the one-page visit data forms on those used in the National Ambulatory Medical Care Survey (NAMCS). Copies are available from the authors upon request. Whenever possible, questions were identical to those in the NAMCS form (eg, demographic characteristics, smoking status, reason for visit, referral source, source of payment, visit duration, visit disposition). Practitioners were asked to record up to five "complaints, symptoms, or other reasons for this visit" using the patient’s own words, listing the most important complaint or reason first. These data were classified using the NAMCS Reason for Visit Classification System, [7] which distinguishes among symptoms, diseases, diagnostic/screening/preventive interventions, treatments, and injuries. New questions asked if the patient was receiving care from a conventional medical provider for the primary problem and if the CAM practitioner had discussed the patient’s care with the treating conventional provider. Questions about diagnoses, assessments, treatments, and self-care recommendations were customized for each profession based on advice from practitioners.
Analysis
Each visit in the sample was weighted by the inverse of the sampling probability, which reflected both the chance a specific provider participated and the proportion of that provider’s annual visits sampled during data collection. For example, an individual chiropractor included in a 10% random sample of chiropractors in a state might report 5,000 patient visits in a year. In this case, each of the 20 visits for which he or she recorded data for the study would represent 250 visits for the year (ie, the inverse of 20/5000). Furthermore, because every chiropractor had a 10% chance of being included in the sample, his or her visits contributed to 10% of the total visits to chiropractors in that year. Thus, to estimate the contributions of each of that chiropractor’s 20 visits to the total number of visits in the state, one would multiply the inverse of the sampling probability (ie, the inverse of 1/10 = 10) by the annual number of visits represented by each of the 20 visits reported (ie, 250). Hence, in this example, each of this chiropractor’s 20 visits would represent 2500 (ie, 10 X 250) of all chiropractor visits in the state for the year and would be weighted accordingly.
Consequently, reported results reflect the total of all visits made to each provider category in each state, except for the 2% of visits made to providers below the minimum visit volume threshold. To correct for the two-stage sampling design, we used SUDAAN software (version 7.5; Research Triangle Institute, Research Triangle, NC) to calculate standard errors and confidence intervals using Taylor series linearization. We assessed statistical significance at the 0.05 level.
RESULTS
Demographic Characteristics and Visit Duration

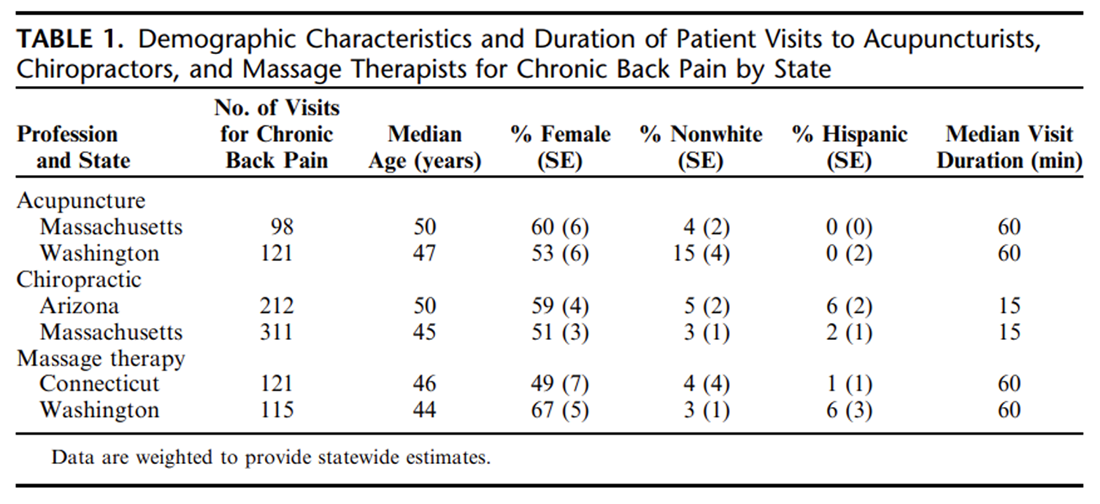
Table 1 This study included a total of 219 visits to 123 acupuncturists, 523 visits to 130 chiropractors, and 236 visits to 126 massage therapists for chronic back pain (Table 1). About 20% of all visits to chiropractors were for chronic back pain, compared with 12–13% of all visits to massage therapists and about 10% of all visits to acupuncturists. Chiropractic visits for chronic back pain lasted a median of 15 minutes, compared with 60 minutes for both acupuncture and massage.
Initial back pain visits to chiropractors were slightly longer (medians of 20 minutes in Arizona and 25 minutes in Massachusetts). Visits for chronic back pain represented about half of all back pain visits to chiropractors and about two thirds of visits to acupuncturists and massage therapists, with the remainder of back pain visits for acute back pain. The median age of patients making these back pain visits ranged from 44 for massage therapy in Washington to 50 for acupuncture in Massachusetts and chiropractic in Arizona. Children represented 1% to 2% of visits for each profession (data not shown). The proportion of visits made by women ranged from 49% for massage therapy patients in Connecticut to 67% for massage therapy patients in Washington. Whites made over 95% of visits, except for acupuncture in Washington (where Asians made 8% of visits). Hispanics made 6% of the visits to chiropractors in Arizona and massage therapists in Washington but only 0% to 3% of visits in the other samples.
Acupuncture
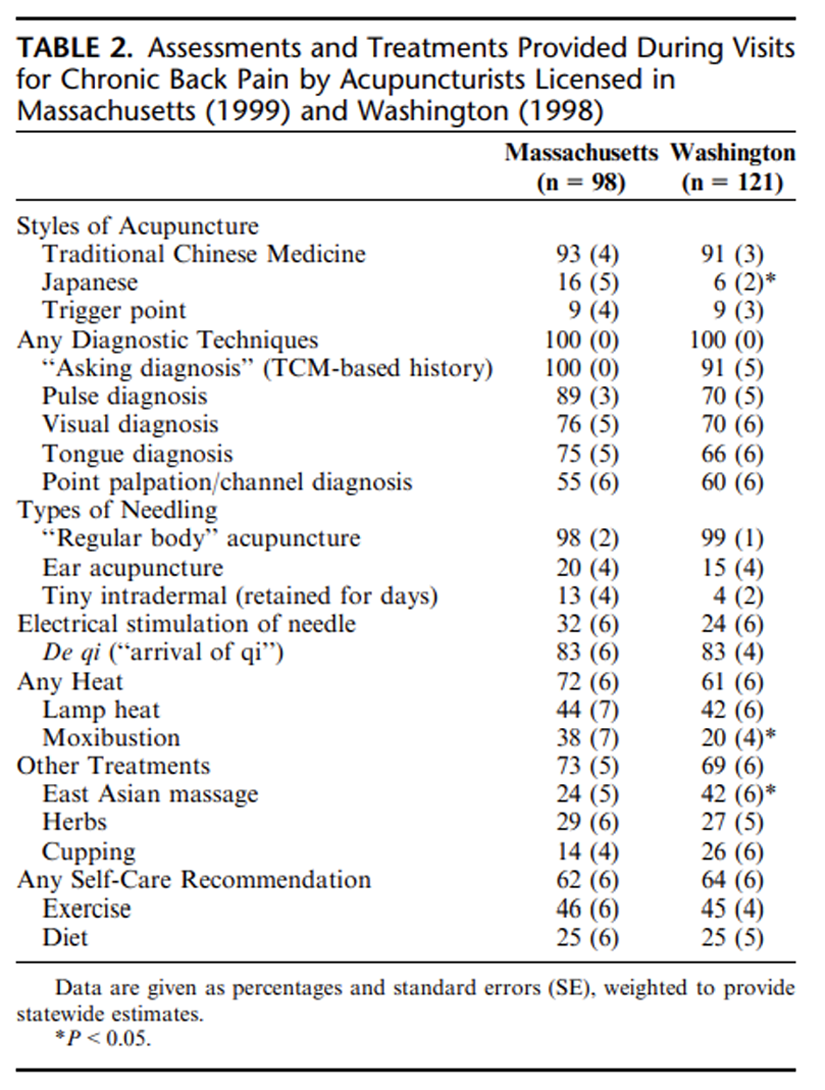
Table 2 Traditional Chinese Medicine was by far the most common style of acupuncture used, although some visits included use of several styles (Table 2). Japanese acupuncture was used significantly more often in Massachusetts than in Washington (P<0.05). Traditional acupuncture diagnostic techniques were used in all visits. These usually included traditional questioning (‘‘Asking Diagnosis’’), taking the radial pulse, inspecting the patient visually (eg, looking at skin color, changes of skin texture, tone of musculature), inspecting the tongue color, shape, and coating, and palpating points along the classic acupuncture meridians (see Appendix for a definition of meridians).
Virtually all visits included "regular body" acupuncture (defined in the Appendix), usually with an attempt to obtain the characteristic de qi sensation in one or more needle locations. Less than one third of all visits included electrical stimulation of the needles. Most visits also included use of additional modalities, especially heat and, in Washington, East Asian massage. Heat lamp use was similar in both states, but moxibustion (defined in the Appendix) was more commonly used in Massachusetts (P<0.05 for moxibustion). Herbs were used in almost 30% of all visits in both states, and in Washington, cupping (defined in the Appendix) was used almost as often. Two thirds of the visits included self-care recommendations, with exercise being the most common recommendation.
Chiropractic
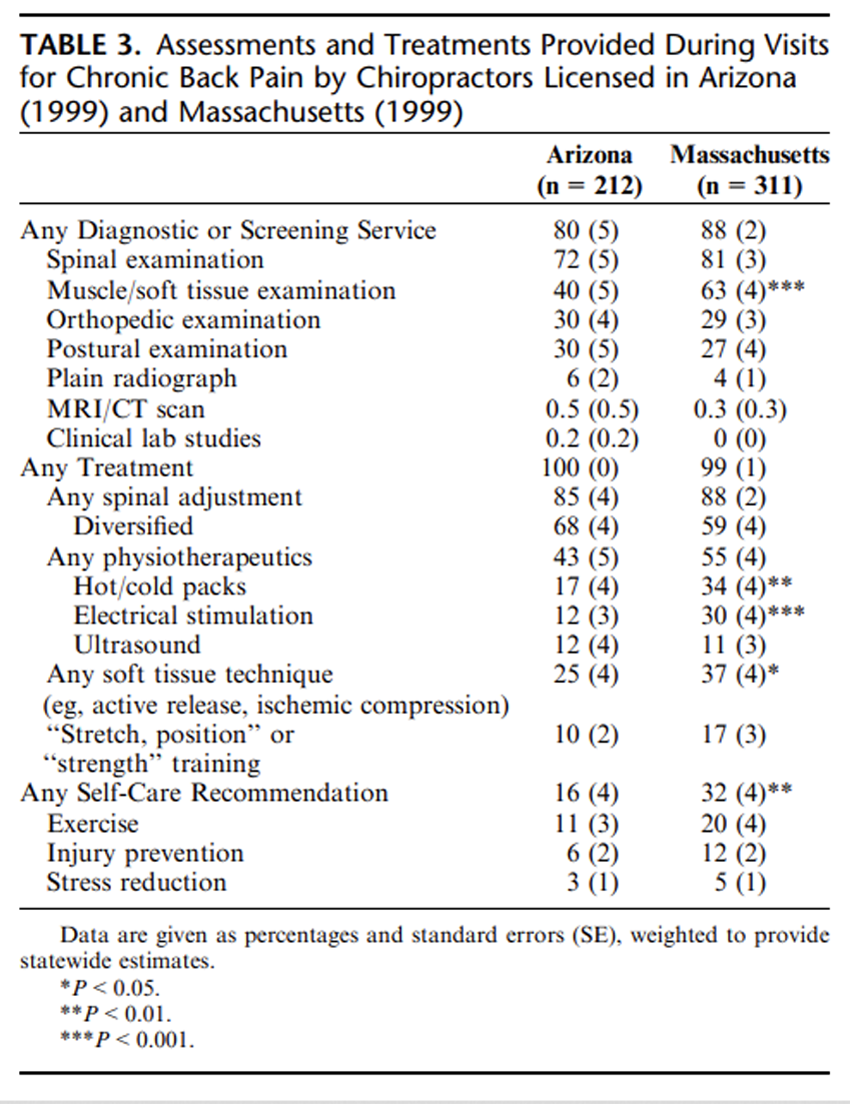
Table 3 About 85% of visits for chronic back pain included one or more diagnostic or screening examinations, most often spinal examinations and, especially in Massachusetts, soft tissue examinations (Table 3). About one third of visits included orthopedic and postural examinations. Surprisingly few radiographs were taken (ie, 12 and 20% of initial visits). MRI/CT scans were extremely rare and laboratory testing was almost never reported.
Visits virtually always included treatments, with 85% to 88% involving a spinal adjustment. Although a variety of adjustment techniques were used, the diversified technique was the most common and was used in about 60% of visits. Physiotherapeutic treatments were used in roughly half of the visits. Of these physiotherapeutics, hot/cold packs and electrical stimulation were twice as likely to be used in Massachusetts as in Arizona. Soft tissue techniques, such as "active release" (defined in the Appendix), were used in about one third of visits. "Stretch or strength" training was substantially less common. Finally, one sixth (Arizona) to one third (Massachusetts) of visits included self-care recommendations, with exercise being the most common.
Massage
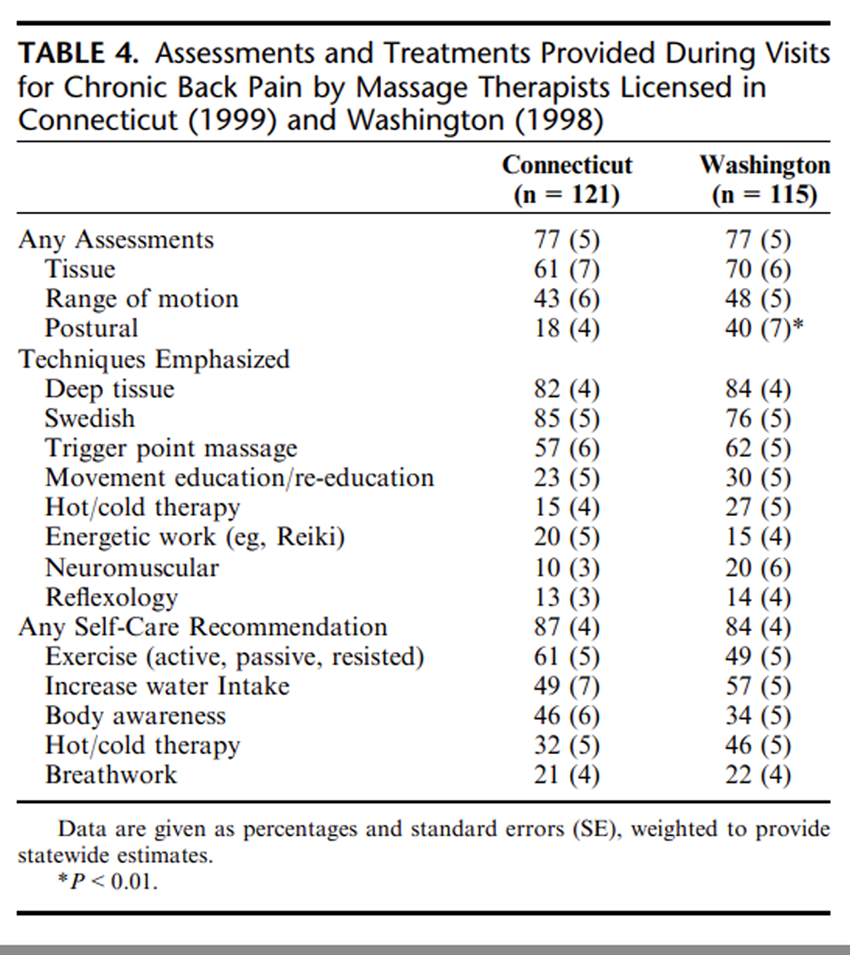
Table 4 Three quarters of the visits included at least one physical assessment, most commonly tissue assessments and range of motion (Table 4). Massage therapists in Washington were more than twice as likely as those in Connecticut to use postural assessments (P<0.01).
Visits to massage therapists emphasized multiple massage techniques, especially deep tissue, Swedish, and trigger point massage. Movement education/re-education (defined in the Appendix) was emphasized in 23% to 30% of all visits, and other techniques were emphasized less often. Finally, about 85% of all visits included self-care recommendations, particularly exercise, increased water intake, body awareness, and hot/cold therapy.
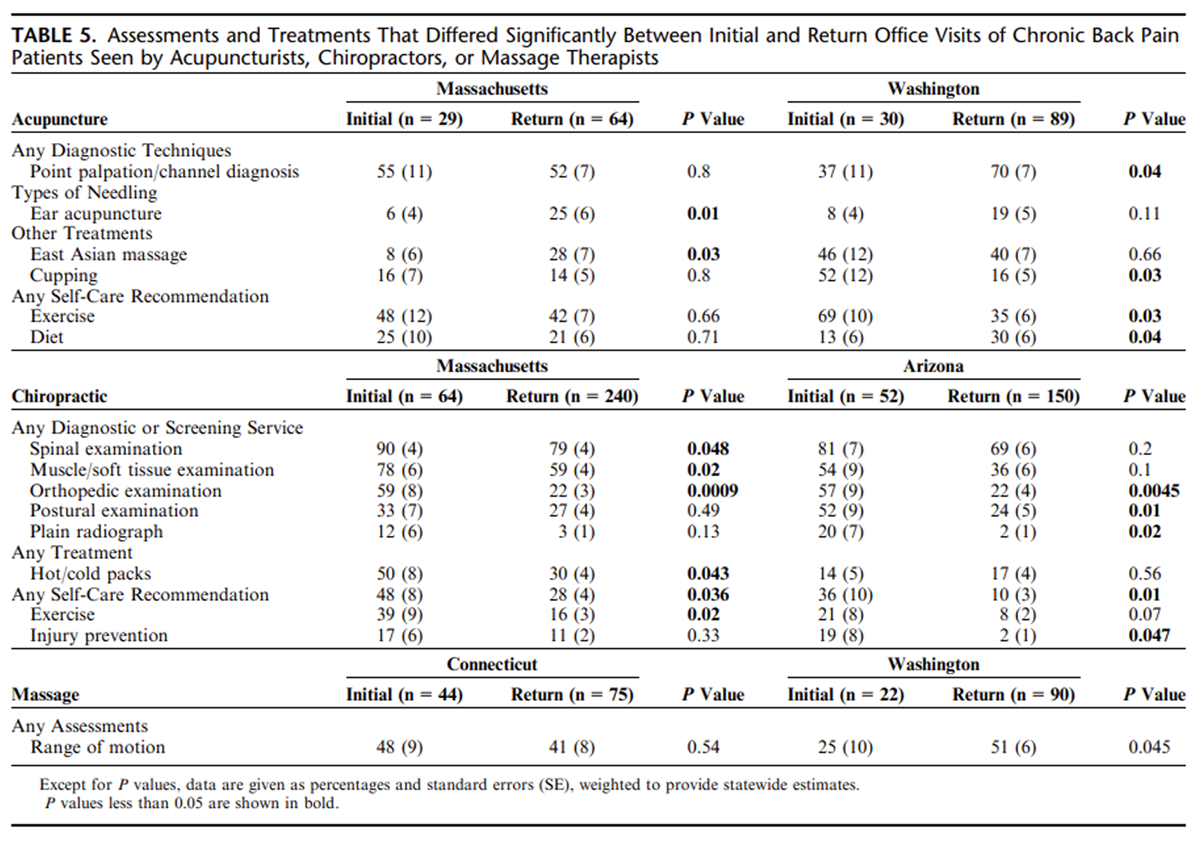
Differences Between First and Return Visits
Table 5 There were numerous differences in the characteristics of initial and return visits to CAM providers for chronic back pain (Table 5). However, few of these differences (and none for visits to acupuncturists or massage therapists) were statistically significant in both states. Specifically, several chiropractic diagnostic and screening services were more common at the first office visit. Plain radiographs were much more likely to be taken at initial visits (12% in Massachusetts, 20% in Arizona) than at follow-up visits (3% in Massachusetts, 2% in Arizona). In both states, self-care recommendations were substantially more common at first office visits than at follow-up visits.
DISCUSSION
Chronic back pain is a common reason that people seek care from acupuncturists, chiropractors, and massage therapists, representing between 10% and 20% of the visits to these providers. Treatments given by each of these professions share certain similarities. Each has a hands-on technique at the core of its treatments (ie, needling the body, manipulating the spine, or massaging the soft tissues), although many different variations of these techniques are used. These techniques are repeatedly used during successive visits, often in conjunction with various adjunctive modalities. Each profession has a prototypical approach. For acupuncture, the typical approach includes assessments that are foreign to the biomedical community (eg, tongue diagnosis), regular body acupuncture using the approach of Traditional Chinese Medicine, and heat. Chiropractic typically includes spinal and soft tissue examinations at the first office visit followed by spinal adjustment, most often using the "diversified technique." Massage therapy usually includes tissue assessment and a massage involving three major treatment styles: deep tissue, Swedish, and trigger point.
Self-care recommendations are also a standard part of acupuncture and massage practice, occurring during almost 65% of visits to acupuncturists and 85% of visits to massage therapists. Chiropractic visits, which are much shorter (15 minutes vs. 60 for the other professions), tend to emphasize in-office treatment. Most self-care recommendations by acupuncturists and chiropractors involve exercise, while massage therapists also emphasize body awareness, heat and cold therapy, and increased water intake. Our finding that few chiropractors prescribed self-care recommendations, even at the first visit, is surprising given the importance of wellness as part of chiropractic philosophy and the findings from previous studies. More than two thirds of the chiropractors surveyed by Christensen and Morgan [9] reported counseling patients about nutrition and exercise in their practices. Hawk and Dusio [10] found that almost 70% of the chiropractors in their survey counseled patients about exercise. In a prospective study of chiropractic care for 842 chronic low back patients, Nyiendo et al [11] found that half of all patients received self-care education and 57% received an education plan. Even though some of the study findings could be due to differences in the way data were collected in each of the studies (ie, single visit per patient for our study vs. all visits per patient for the Nyiendo study vs. surveys of providers for the other studies), our data suggest that chiropractors may not be taking full advantage of the potential benefits of self-care recommendations.
Each of the professions offers an explanation for the cause of back pain that differs somewhat from that normally provided by a medical doctor, and the treatments they provide are designed to directly remove such causes. For example, traditional acupuncture treatments for back pain might "move the stagnant qi or energy and nourish the Kidney" [8] and chiropractic treatments might correct the "subluxation" (see Appendix for a definition). [12] The safety profile of these treatments for back pain is reassuring. [13] Finally, each of these professions acknowledges the importance of the patient-provider relationship as well as patient self-care in contributing to the healing process (eg, acupuncture [14, 15]; chiropractic [16, 17]; massage [18]).
Although the primary treatment modality differs among acupuncture, chiropractic, and massage, there is some overlap in treatment between the professions. For example, chiropractors in some states use acupuncture needles, if only rarely. During the time frame of the study, 19 states, including Arizona, permitted chiropractors to use acupuncture needles as part of their scope of practice, many requiring additional training, most commonly 100 hours. [19, 20] Some states, including Massachusetts, required all chiropractors who used acupuncture needles to also be trained and licensed as an acupuncturist. Meridian-based massage techniques are used more often by acupuncturists than by massage therapists. All three professions make self-care recommendations, with exercise being part of those recommendations for all professions.
In general, there were few significant between-state differences in how each type of CAM provider treated patients for chronic back pain. There were also few consistent differences in care provided during first and return visits. A notable exception was that first visits to chiropractors were more likely to include various diagnostic or screening exams, including radiographs, than were return visits. Interestingly, radiographs were relatively uncommon (12% to 20%) even at first visits. Whether this reflects more conservative use of radiographs by chiropractors than has been reported in the past [21] or whether many chiropractic patients already had radiographs during previous episodes of chiropractic care is unknown.
Strengths and Limitations
Strengths of this study include the random sampling of providers from two geographically diverse states for each profession, the relatively high participation rates, and the comprehensive information collected on assessments and treatments. This study has several limitations. Since data were collected for each profession from only two states, we do not know how representative the findings are of the entire United States, due to variation in state licensing laws for these professions. These data are cross-sectional, including a mix of initial and follow-up visits.
Although we found that some diagnostic features of the visits (eg, chiropractor’s use of radiographs and self-care recommendations) were more common at the first visit, we had limited ability to detect significant differences due to small sample sizes. Our data collection form did not distinguish between the care provided for primary complaints (ie, chronic back pain) and for secondary complaints, so some of the care provided may not have been for a back problem. Finally, we restricted our analyses to back pain visits where the provider indicated that the condition was "chronic," but providers may not have defined such visits consistently.
Implications for Future Research
To date, studies of both acupuncture and spinal manipulation have evaluated the core technique of acupuncturists and chiropractors but have rarely studied these techniques as part of the package of care delivered by acupuncturists and chiropractors. [22, 23] Pragmatic trials that test therapies resembling what patients with chronic back pain receive in practice are critical to evaluate the effectiveness of the types of treatments that patients are most likely to get. Massage studies are in their infancy but will also need to test protocols broad enough to mirror the care that patients actually receive.
Implications for Physicians
In advising patients about the use of CAM therapies, physicians should be guided by evidence on effectiveness and safety. [24] The amount and quality of evidence on effectiveness varies for these therapies. Spinal manipulation appears to be superior to sham and known ineffective therapies but not superior to effective conventional treatments for chronic low back pain. [13] Previous acupuncture studies are generally of poor quality, so the effectiveness of acupuncture for treating low back pain is unclear. [13] Although only three studies have evaluated massage for back pain, all three studies were positive. [13]
The literature suggests that, in general, the care given to back pain patients by these CAM providers is safe. [13] While no information was collected on the source of the herbal medicines prescribed by acupuncturists during a substantial minority of their visits, there is some concern that Chinese "patent" remedies manufactured overseas may be adulterated with various contaminants, including medications and toxic metals. [24] As such, patients should be cautioned in this regard.
While there is some variability in the treatment provided to chronic back pain patients by acupuncturists, chiropractors, and massage therapists, physicians may be reassured by our data that the treatments used by these practitioners are relatively well characterized and "mainstream" for these professions and rarely include modalities that can be dangerous. Individualization is a hallmark of CAM treatments, even though the effect of such variability on outcomes is unknown. In any event, data from this study will be helpful to physicians whose patients seek or wish to seek CAM care for back pain and who may want advice from an informed physician.
Supplementary Material
Acupuncture Terms
Traditional Chinese Medicine (TCM): Although TCM traces its roots to ancient China, it has undergone much change over the centuries. Currently, the system includes a variety of traditional diagnostic approaches as well as numerous therapeutic modalities, including herbal medicine, acupuncture, moxibustion, cupping, and Tui Na (Chinese massage). TCM acupuncture often involves heavy manipulation of the acupuncture needles and a strong de qi sensation. [25]
Japanese Acupuncture: Although many different styles of Japanese acupuncture exist, all tracing their roots to different interpretations of an ancient Chinese acupuncture text, they are characteristically subtler than TCM, with shallower needle insertion and no emphasis on eliciting the de qi sensation. They also seem to concentrate much more on putative root causes of a condition rather than symptom reduction per se. [25]
Meridian: In traditional forms of acupuncture, meridians are the invisible channels that carry energy or qi throughout the body. Health is thought to depend partially on the unobstructed flow of this energy through the meridians. There are 12 major meridians and numerous minor "collaterals" that connect these meridians. [25]
De qi: The characteristic de qi sensations (a dullness, achiness, or pain) elicited by some acupuncture needling techniques occurs when needling activates type II, III, and IV afferent nerve fibers in the muscle. [26]
Regular Body Acupuncture: Regular body acupuncture involves using acupuncture points located on the traditional acupuncture channels (ie, meridians) that traverse the body, as well as classically described "extra" points.
Moxibustion: Moxibustion is burning of the mugwort plant Artemesia vulgaris near or on the surface of the body at specific locations. It is thought to influence the flow of "qi and blood." [25]
Cupping: Cupping is the application of suction cups to the skin to induce a vacuum. Cupping is thought to clear local "stagnation" (common in pain conditions) by stimulating the flow of "qi and blood." [25]
Point Palpation/Channel Diagnosis: Palpation of acupuncture points and acupuncture channels to help in identifying the Chinese medical diagnosis
Chiropractic TermsDiversified Technique: The term refers to a variety of chiropractic spinal and extremity manipulation procedures as developed and taught in chiropractic colleges. It is the most commonly used chiropractic manipulation procedure, typically involving low-amplitude, high-velocity thrust procedures applied to articulations determined to be dysfunctional. Other chiropractic techniques have been developed as part of a "comprehensive diagnostic and treatment package" by private practitioners and are frequently given "brand names."
Subluxation: When used as a diagnosis in chiropractic care, the term typically refers to mechanical dysfunction (eg, aberrant motion, muscle spasm, local inflammatory responses, pain radiation) of joints and associated soft tissues in the anatomic region where it is diagnosed. [27]
Active Release: A soft tissue myofascial and manipulation procedure aimed at locating adhesions and fibrosis in musculotendinous structures. The technique uses specially designed instruments and procedures to break up adhesions and restore greater mobility and pliability to the affected tissues.
Massage TermsMovement Education/Re-education: Movement re-education uses movement to enhance body awareness and movement for the patient. Some styles of movement re-education emphasize active exercises (eg, Alexander technique) to teach healthier ways of moving. Others emphasize tablework in which the practitioner induces, assists, or resists movement for a patient (eg, Proprioceptive Neuromuscular Facilitation, positional release, passive and active assisted or resisted exercise and stretch). A third group of movement therapies offers a combination of tablework and exercises (eg, Trager, Feldenkrais). [18]
Energetic Work: Subtle energy techniques (also called energy work or body-mind therapies) attempt to assist the flow of energy in the body through either very light touch or holding the hands just above the skin. [18]
Reflexology: Reflexology is the physical act of applying pressure to the feet (or hands) based on the idea that there are reflex points in these areas that correspond to other areas of the body and/or organs.
ACKNOWLEDGMENTS
The authors thank the original "NAMACS Team" for data collection and Kristin Delaney and John Ewing for help with data analysis and manuscript preparation
References:
van Tulder MW, Koes BW, Bouter LM.
Conservative treatment of acute and chronic nonspecific low back pain.
A systematic review of randomized controlled trials
of the most common interventions.
Spine. 1997;22:2128-2156.How is your doctor treating you?
Consumers Reports. 1995;81-88.Eisenberg DM, Davis RB, Ettner SL, et al.
Trends in Alternative Medicine Use in the United States,
from 1990 to 1997: Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Wolsko PM, Eisenberg DM, Davis RB, et al.
Patterns and Perceptions of Care for Treatment of
Back and Neck Pain: Results of a National Survey
Spine (Phila Pa 1976) 2003 (Feb 1); 28 (3): 292–297Cherkin DC, Deyo RA, Sherman KJ, et al.
Characteristics of Visits to Licensed Acupuncturists,
Chiropractors, Massage Therapists, and Naturopathic Physicians
J Am Board Fam Pract 2002; 15 (6):463-480Cherkin DC, Deyo RA, Sherman KJ, et al.
Characteristics of licensed acupuncturists, chiropractors,
massage therapists, and naturopathic physicians.
J Am Board Fam Pract. 2002;15:378-390.Schneider D, Appleton L, McLemore T.
National Center for Health Statistics:
a reason for visit classification for ambulatory care.
In: DHEW Pub No Public Health Service (PHS), ed.,
Vital and Health Statistics.
Washington, DC: U.S. Government Printing Office; 1979; 79/1352.Maciocia G, ed.,
The Practice of Chinese Medicine.
New York: Churchill Livingstone; 1997.Christensen M, Morgan D, eds.
Job Analysis of Chiropractic: A Project Report, Survey Analysis,
Summary of the Practice of Chiropractic
in the United States
Greeley, CO: National Board of Chiropractic Examiners. 2005Hawk C, Dusio ME.
Chiropractors’ attitudes toward training in prevention:
results of a survey of U.S. chiropractors.
J Manipulative Physiol Ther. 1995;18:135-140.Nyiendo J, Haas M, Goldberg B, et al.
Patient Characteristics and Physicians' Practice Activities for
Patients with Chronic Low Back Pain: A Practice-based
Study of Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther 2001 (Feb); 24 (2): 92–100Kaptchuk TJ, Eisenberg DM.
Chiropractic: Origins, Controversies, and Contributions
Archives of Internal Medicine 1998 (Nov 9); 158 (20): 2215–2224Cherkin DC, Sherman KJ, Deyo RA, et al.
A review of the evidence for the effectiveness, safety, and cost of
acupuncture massage therapy, and spinal manipulation for back pain.
Ann Intern Med. 2003;138:898-906.Cassidy CM.
Chinese medicine users in the United States. Part II:
Preferred aspects of care.
J Altern Complement Med. 1998;4:189-202.Kaptchuk TJ.
Acupuncture: theory, efficacy, and practice.
Ann Intern Med. 2002;136:374-383.Meeker WC, Haldeman S.
Chiropractic: A Profession at the Crossroads
of Mainstream and Alternative Medicine
Annals of Internal Medicine 2002 (Feb 5); 136 (3): 216–227Cooper RA, McKee HJ.
Chiropractic in the United States: trends and issues.
Milbank Q. 2003;81:107-138.Levine AS, Levine VJ.
The Bodywork and Massage Sourcebook.
Los Angeles: Lowell House; 1999.Lamm LC, Wegner E, Collord D.
Chiropractic scope of practice: what the law allows—update 1993.
J Manipulative Physiol Ther. 1995;18:16-20.Ergil KV.
Acupuncture licensure, training, and certification in the US.
NIH Consensus Development Conference on Acupuncture, November 1997:31-38.Cherkin DC, MacCornack FA, Berg AO.
Managing low back pain: a comparison of the beliefs and
behaviors of family physicians and chiropractors.
West J Med. 1988;149:475-480.Sherman KJ, Cherkin DC.
Challenges of acupuncture research: study design considerations.
Clin Acupuncture Oriental Med Int J. 2003;3:200-206.Assendelft WJ, Morton SC, Yu EI, et al.
Spinal manipulative therapy for low back pain. A meta-analysis
of effectiveness relative to other therapies.
Ann Intern Med. 2003;138:871-881.Eisenberg DM.
Advising Patients Who Seek Alternative Medical Therapies
Annals of Internal Medicine 1997 (Jul 1); 127: 61-69Birch SJ, Felt RL.
Understanding Acupuncture.
New York: Churchill Livingstone; 1999.Wang KM, Yao SM, Xian YL, et al.
A study on the receptive field of acupoints and the relationship between
characteristics of needling sensation and groups of afferent fibres.
Sci Sin. 1985;28:963-971.Triano JJ.
The Functional Spinal Lesion: An Evidence-Based Model of Subluxation
Topics In Clinical Chiropractic 2001 (Dec); 8 (1): 16–28
Return to ACUPUNCTURE
Return to LOW BACK PAIN
Since 9-23-2025
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |