

Chiropractic Services in the Active Duty Military Setting:
A Scoping ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2019 (Jul 15); 27: 45 ~ FULL TEXT
OPEN ACCESS Silvano Mior, Deborah Sutton, Daphne To, Carolina Cancelliere, Simon French, Anne Taylor-Vaisey & Pierre Côté
UOIT-CMCC Centre for Disability Prevention and Rehabilitation,
University of Ontario Institute of Technology (UOIT) and
Canadian Memorial Chiropractic College (CMCC),
6100 Leslie Street,
Toronto, Ontario M2H 3J1 Canada
FROM: Nahin ~ Pain 2017BACKGROUND: Musculoskeletal injuries are one of the most prevalent battle and non-battle related injuries in the active duty military. In some countries, chiropractic services are accessed to manage such injuries within and outside military healthcare systems; however, there is no recent description of such access nor outcomes. This scoping review aimed to synthesize published literature exploring the nature, models, and outcomes of chiropractic services provided to active duty military globally.
METHOD: We employed scoping review methodology. Systematic searches of relevant databases, including military collections and hand searches were conducted from inception to October 22, 2018. We included peer-reviewed English literature with qualitative and quantitative designs, describing chiropractic practice and services delivered to active duty military worldwide. Paired reviewers independently reviewed all citations and articles using a two-phase screening process. Data from relevant articles were extracted into evidence tables and sorted by study type. Results were descriptively analyzed.
RESULTS: We screened 497 articles and 20 met inclusion criteria. Chiropractic services were commonly provided on-base only in the US. Services were accessed by physician referral and commonly after initiation or non-response to other care. Use of scope of practice was determined by the system/facility, varying from intervention specific to comprehensive services. Back pain with and without radiculopathy accounted for most complaints. Treatment outcomes were reported primarily by case reports. However, two recent randomized trials reported improved pain, disability, and satisfaction when adding chiropractic care to usual medical care compared to usual medical care alone in management of low back pain. Specific reaction time measures in special operation forces military did not improve after chiropractic care compared to wait-list control.
There is more like this at our
CHIROPRACTIC CARE FOR VETERANS PageCONCLUSIONS: Our scoping review found the majority of published articles described chiropractic services in the active duty military in the US setting. Recent RCTs suggest a benefit of including chiropractic care to usual medical care in managing back pain in active duty military. Yet despite reported benefits in Australia, Canada, and the US, there is a need for further qualitative, descriptive, and clinical trial data worldwide to inform the role of chiropractic services in active duty military.
KEYWORDS: Active duty; Chiropractic; Military medicine; Military personnel
From the FULL TEXT Article:
Background
Musculoskeletal injuries significantly affect the health and operational readiness of active military personnel. They are one of the most prevalent battle and non-battle related injuries in theatre. [1, 2] Analysis of United States (US) Navy Physical Evaluation Board data between February 2005 and February 2006 indicated that musculoskeletal diagnoses were frequent (43%), with back pain (29%) being the most common musculoskeletal diagnosis. [3] Musculoskeletal injuries are also one of the most common reasons for Canadian Armed Forces (CAF) personnel not being deployed [4], and were responsible for 42% of all medical releases in 2013. [5] In addition, neck pain is an important aeromedical problem. Fifty-one percent (51.7%) of Swedish Air Force aviators reported experiencing neck pain [6], while 53.3% of rotary-wing crew and 69% of fast-jet crew reported neck pain in the Royal Air Force. [7]
In the active military setting, musculoskeletal conditions are associated with lost productivity due to sick parade attendance, lost duty days [1, 8, 9], and impact the ability to deploy. [5] The probability of returning to full duties decreases with time spent away from duties [10], and the potential long term sequelae include limited duty assignment or early termination of service. [8] In addition to related costs for treatment interventions, medical discharge increases resource expenditures resulting from the recruitment and training of replacement recruits. [2]
Evidence-based interventions for musculoskeletal injuries include a focus on active versus passive treatment, structured education, exercise, and manual and cognitive behavioural therapies. [11] Musculoskeletal programs of care in the military setting are frequently delivered in a multidisciplinary healthcare environment. Access to these programs of care by military personnel most often occurs through a traditional gatekeeper physician referral [12], or through a non-traditional gatekeeper such as a physical therapist [13]; personnel are referred to other musculoskeletal healthcare providers, or to team assessment and management. [14, 15]
Available reviews have compared or described chiropractic services within both military and veteran healthcare systems in combination [16–18]. A 2009 review described chiropractic services in military and veteran healthcare systems in the US and Canada, but concluded that there was a need to evaluate the processes, policies, practices, and effectiveness of chiropractic services in these settings. [17] However, no recent knowledge syntheses have summarized the integration of chiropractic services in global military healthcare systems solely within an active duty military population. In particular, to our knowledge there is no current review of the literature describing chiropractic services and its utilization, scope of practice, and policies in the active duty military worldwide. Such a review can assist in informing the role of chiropractic services in this population.
Therefore, the objective of this scoping review was to document the current global state of knowledge related to chiropractic services in the active duty military setting with respect to:1) access of chiropractic services;
2) chiropractic scope of practice, e.g. procedures, processes, and actions;
3) service model and location; and
4) type of condition treated, duration, and outcomes of treatment provided to active duty military members.
Methods
We employed scoping review methodology to collect and organize relevant information to synthesize the available evidence addressing our broad research question. [19] We applied the scoping review framework of Arksey and O’Malley [19] and successive recommendations [20–22] for conducting and reporting scoping reviews. Consistent with this framework, we did not critically appraise the methodology of reviewed articles [19–21]. This review is reported against the PRISMA extension for scoping reviews (PRISMA-ScR). [22]
Stage 1: identifying the research question
Our scoping review was guided by the following broad research question: What is published in the peer-reviewed literature regarding the access, scope of practice, service models, conditions treated and outcomes related to chiropractic care for active duty military members?
Stage 2: identifying relevant articles
Our search strategy was developed in consultation with a health sciences librarian, and a second librarian reviewed the search for completeness using the Peer Review of Electronic Search Strategies (PRESS) Checklist. [23, 24] The search strategy was first developed in MEDLINE (Ovid®) and subsequently adapted to the other databases. The search terms included subject headings specific to each database (e.g., MeSH in MEDLINE) [25] and free text words relevant to utilization of chiropractors and chiropractic services were combined with terms relevant to the army and active duty military (see Additional file 1 for full MEDLINE search strategy).
We searched MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, PsycINFO, Cochrane Central Register of Controlled Trials, and Embase, through Ovid Technologies, Inc.; CINAHL Plus through EBSCOhost from inception to September 15, 2018; and the Military & Government Collection through EBSCOhost; and the Military Database through ProQuest from inception to October 22, 2018. The reference lists of relevant articles were hand searched for additional articles not identified from the electronic database search. We used the PRISMA-ScR [22] flow chart to track the number of articles at each stage of the review. The results from the database searches were combined and imported to EndNote X6. [26] We did not register this review prior to undertaking it.
Stage 3: article selectionInclusion and exclusion criteria Eligible studies met the following criteria: 1) published in the peer-reviewed literature; 2) written in the English language; 3) were any primary qualitative or quantitative designs, including qualitative studies, randomized controlled trials, quasi-randomized trials, cohort, cross-sectional, case report and case series designs; 4) described chiropractic services; and 5) the study population included active duty military personnel, the National Guard, or reservists. Study exclusion criteria included: narrative and systematic reviews, letters, editorials, commentaries, unpublished manuscripts, dissertations, government reports, books and book chapters, conference proceedings, meeting abstracts, lectures and addresses, consensus development statements, informal communication, e.g. blogs, podcasts, email, cadaveric or animal studies, and non-active military members, e.g. veterans.
Screening and agreement Eligible articles were selected through a two-phase screening process. In Phase 1, two of the authors (DS, DT) independently screened titles and abstracts to determine eligibility. Articles were classified as relevant, possibly relevant, or irrelevant. In Phase 2, the same reviewers independently reviewed full text manuscripts of relevant and possibly relevant articles to make a final determination of eligibility. Reviewers met to solve disagreements and reach consensus in both phases. We involved a third independent reviewer (SM) if consensus could not be reached. We contacted authors when additional information was needed to confirm article relevance.
Stage 4: data charting
We extracted the following data from the relevant articles (when available): 1) study description (study design, country of origin, service model and branch, and study population); 2) type of condition and duration; 3) chiropractic services provided; and 4) study findings (e.g. utilization of chiropractic services, patient outcomes, satisfaction). One review author (DS) extracted the data which were independently checked by a second review author (SM) to minimize error.
Stage 5: collating, summarizing, and reporting the results
We employed a ‘descriptive-analytical’ method within the narrative tradition to summarize the data and include the following [27]: Descriptive numerical analysis: The nature and distribution of the articles were examined with respect to the total number of articles, year of publication, country where studies were conducted, study population, and study design.
Narrative summary of included study findings: We classified the studies according to our review objectives: 1) access to chiropractic services; 2) chiropractic scope of practice, e.g. procedures, processes, and actions; 3) service model and location of delivery; and 4) type of condition treated, duration and outcomes of treatment provided for active duty military members globally. Where relevant and where possible, we extracted the 95% confidence intervals around any point estimates provided.
Implication of results: We reported the findings according to our objective of describing the published literature on utilization, scope of practice, and policies related to chiropractic services for active duty military members globally.
Results
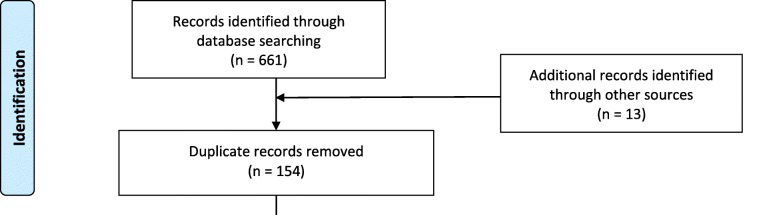
Figure 1

Table 1 Our search yielded 674 citations. We removed 154 duplicates and screened 520 articles (Figure 1). During Phase I screening, we excluded 461 articles, and a further 39 articles following Phase II screening. We contacted two authors for clarification, one regarding military status of participants and one to clarify treatment specifics of chiropractic care provided. However, neither author responded; these two articles were excluded. Twenty articles were included in this review. [12, 16, 28–45]
Descriptive numerical analysis
Table 1 summarizes the key findings from the relevant articles. Research on the utilization, scope of practice, and policies related to chiropractic services for active duty military members globally is a small and relatively recent body of literature, with the earliest included study published in 2006. The studies were most commonly conducted in the United States (n = 17) [16, 28–32, 34–43, 45], with one conducted in Australia (n = 1) [33], and two in Canada (n = 2). [12, 44] Most studies were cross-sectional (n = 9) [12, 28, 31–37], six were case reports [38–43], three were randomized controlled trials [29, 30, 45], and two were qualitative designs. [16, 44]
Location and access to chiropractic services
Six case reports [38–43], three randomized controlled trials [29, 30, 45], and one cross-sectional study [12] described chiropractic services provided to active duty military personnel worldwide. In North America, chiropractic services were reported as initiated through referral from a primary care provider (gatekeeper) following initial assessment, except in the randomized controlled studies where access was predetermined by study design. [29, 30, 45]
As reported in the included articles, patients typically accessed chiropractic services through a gatekeeper, and were seen primarily for musculoskeletal conditions. [16, 44] The referral for chiropractic services may occur after the initial assessment, but most often occurred after initiation and non-response from other interventions. [16, 41, 44] Such other interventions included prescribed medication, diagnostic imaging, e.g. radiographs, magnetic resonance imaging, physical therapy, and referral to other healthcare services, e.g. pain clinic, specialist consultation. Direct access by active duty military personnel to chiropractic care was not reported in any included study.
Dunn et al. [16] in their qualitative study noted that chiropractic care was initiated into the US Department of Defense (DoD) in response to legislative action (1993–2009), and service has grown to 49 Military Health System commands. A survey to identify complementary and alternative medicine use at fourteen Military Treatment Facilities reported 92% of these facilities offered chiropractic services in 2005 compared to 85% in 2009. [34] Additionally, the Military Health System Complementary and Alternative Medicine survey identified 55% of US Military Treatment Facilities offered chiropractic services in 2013. [31] However, in 2005, 54% of active duty personnel resided in areas served by chiropractic clinics, with the remainder not served because of living overseas (14%), in remote areas (5%), or on bases with no chiropractic clinics (28%). [28]
In one Canadian study [12], chiropractic care was provided on-base in one location; however, this is no longer the case. Currently in Canada, chiropractic care is an eligible health benefit to CAF personnel and is accessed off-base, outside the military health system. [44]
Chiropractic scope of practice
The practice of chiropractic is the assessment of conditions related to the spine, nervous system, and joints and the diagnosis, prevention, and treatment of these conditions. [14] However, in Military Treatment Facilities, chiropractic scope of practice is established by the system/facility and may include comprehensive services (e.g. spinal manipulative therapy (SMT), mobilizations, modalities, rehabilitation), utilization of guidelines, and in some instances the performance of administrative tasks. [16]
The chiropractic scope of practice described in the included articles consisted of both assessment and treatment. The chiropractic assessment included a focused history, physical examination, clinical impressions, disability, prognosis, and treatment plan elements. The interventions described in the articles included the following physical techniques and modalities: joint manipulation and mobilization of the spine and extremities [12, 29, 30, 38–42], soft tissue massage [12, 29], stretching/proprioceptive neurological facilitation maneuvers [12, 38–41], cryotherapy [30, 42], moist heat [42], superficial heat [30], McKenzie exercises [29], exercise [12, 29, 30, 38–42], interferential current [12, 30, 42], ultrasound [30], acupuncture [12], myofascial release [38], ischemic compression [38], advice on activities of daily living [29], postural/ergonomic advice [29, 39, 40], as well as nutritional and psychosocial aspects of treatment. [42]
Delivery model and benefits
In the US, active duty military personnel predominantly attended an on-base clinic [16, 29, 30, 38–43]. Care was described as interdisciplinary; however, healthcare providers typically provided services in physical isolation from other care providers. Case discussions occurred most often when prompted by a referral. In this healthcare model, the service member’s first point of contact is with a primary care provider who refers to chiropractic care if deemed necessary.
Chiropractors in the Military Health System are either contractors or employees of contractors, typically without healthcare and other benefits as part of their employment contract. [16] The chiropractor’s employment period is limited to the contract period. A decentralized leadership Military Health System structure may challenge the integration of chiropractic service into the Military Health System. Chiropractic care is a TRICARE benefit available to active duty service personnel but not their dependents. [16]
Challenges to collaboration
Challenges to collaboration were identified in two qualitative studies. Mior et al. described barriers to the integration of chiropractic services within the Canadian Forces Health Services (CFHS). [44] Challenges to the integration of chiropractic services within the CFHS included base-to-base variation in referral procedures, which were associated with clinician preference and experience rather than a systematic approach. Mior et al. also reported that inter-professional communication varied by base and typically lacked standardized reporting. [44] The minimal reported interaction between chiropractors and CFHS healthcare providers apparently impeded the development of a positive inter-professional relationship. Chiropractic care was perceived as a duplication of physical therapy services, often considered more as a single intervention, that is spinal manipulative therapy, rather than as a profession.
Dunn et al. [16] identified that untimely access, unavailable services, and unobtained referrals could affect the integration of chiropractic services in the Military Health System. Despite the legislative mandates in the US, Dunn et al. argued that continued acceptance and integration will depend upon the chiropractors adding measurable value to service delivery. [16]
Both qualitative reports suggested that improved collaboration and/or integration was not possible without service availability at military treatment facilities. Also, ensuring care provided was consistent with the needs of the patients, while being respectful of the roles and responsibilities of others, was argued as important to ensure sustainable integration. [16, 44]
Opportunities
Opportunities to include chiropractic services within the active duty military were identified in several articles. [6, 31, 44]These opportunities included providing clinical, cost effective evidence-based care for musculoskeletal conditions within an environment of inter-professional collaborative care. Specifically, within this environment the delivery of care would be based on clinical practice guidelines that draw upon the full scope of chiropractors’ practice rather than solely the delivery of a specific intervention.
Utilization of chiropractic services
The utilization rate of chiropractic services by active duty military members was reported in seven cross-sectional surveys. [28, 32–37] The reported utilization rate of chiropractic services over the preceding 12?months was consistent over time (2000–2011) in the United States but then decreased in 2013. Specifically, the utilization rate ranged between 5.2 and 10.5% among active duty military personnel [28, 32, 35–37] and 14.8% in the Reserve/National Guard in 2007 [35], to a low of 2.9% in 2013 among services in the Military Health System. [49] In Australian military aircrew, 12% sought chiropractic services for flight-related neck pain [66], which is higher than the 12-month chiropractic service utilization in the US in the period 2008-2011.
Type of conditions treated and duration of treatment period
Back pain with or without radiculopathy accounted for the majority of presentations [12, 29, 30, 38, 39]. In a US cross-sectional study, 42.7% of respondents reported using chiropractic services for low back pain (LBP), 27.3% for headaches, and 10.9% for general health, wellness, and prevention. [31] In a Canadian cross-sectional survey, 97% of patients reported spine-related musculoskeletal complaints, of which 52% were LBP, and 3% involved conditions of the extremities. [12]
Neck pain was reported as the reason for chiropractic consult in several articles [12, 33, 40, 41, 43]. In a survey of Australian air force personnel, 12% of the respondents sought chiropractic care for neck pain. [33] Neck pain with radiating symptoms was reported in one cross-sectional study. [12] Aside from one of the included randomized controlled trials [29], most articles reported patients presenting with chronic musculoskeletal conditions. [12, 30, 31, 40, 43]
Chiropractic treatment duration was reported in nine articles and varied considerably between articles [12, 29, 30, 38–43]. In their cross-sectional study, Boudreau et al. [12] reported the average number of chiropractic visits as 5.7 ± 4.1 (mean ± SD), ranging from one to 25 visits. Goertz et al. [29] in their randomized control trial (RCT) scheduled up to two chiropractic visits weekly (eight visits) for a period of 4 weeks, and reported participants attended an average of seven visits. In another randomized controlled trial, patients were allocated to up to 12 visits over 6 weeks [30], with patients utilizing a much smaller number than the available number of visits. Patients who attended at least one visit to a chiropractor reported a mean number of chiropractic visits (mean ± SD) which varied across study sites and ranged from 2.3 ± 1.4 (San Diego), 4.7 ± 2.5 (Walter Reed), to 5.4 ± 2.6 (Pensacola). [30] In a survey of US Military Treatment Facilities offering chiropractic services, the average number of patient visits to a chiropractor was 5.4, the highest reported patient visits of any complementary and alternative medicine provider in 2013. [31]
Case report participants reported the greatest number of chiropractic visits. The number varied from 16 visits over 30?weeks with an aviator instructor with acute LBP [38], a military officer with C3–5 anterior longitudinal ligament heterotopic ossification and ankyloses received 34 visits over 47 weeks [43], and a Naval Petty Officer with low back and radicular pain attended 11 visits over 72 days. [52]
Outcomes of care
Reported outcomes of chiropractic care were predominantly positive. Favourable outcomes following chiropractic care were reported in each of the case reports, however in one case report the patient improved but did not return to duty. [43] In a Canadian cross-sectional study, active duty military reported satisfaction with care (94.2%). [12] Further, all physicians in this study identified a perceived demand for chiropractic services, and the majority (80.6%) were satisfied with chiropractic services. [12]
In a RCT, Goertz et al. [29] reported a mean difference favouring chiropractic manipulative therapy (CMT) in addition to standard medical care (SMC) over SMC alone for each of the primary outcomes at 2 and 4 weeks in acute LBP subjects. A greater percentage of participants in the SMC plus CMT group (73%) rated their global improvement as pain completely gone, much better, or moderately better, compared with 17% in the SMC group. Similarly in another RCT, Goertz et al. [30] reported mean differences favouring usual medical care (UMC) with chiropractic care (CC) over UMC alone for each of the primary outcomes at 6 and 12 weeks, although the magnitude of difference decreased at 12 weeks. Additionally, secondary outcomes of worst LBP intensity and symptom bothersomeness also favoured UMC + CC over UMC. Overall, UMC + CC identified better global perceived improvement, satisfaction with care, and used less pain medication.
The DeVocht et al. [45] RCT assessed if a short course (4 visits) of CMT improved reaction and response time outcomes in special operation forces military compared to wait-list control. Despite observing an immediate effect after the first session on complex response task, no significant between group differences were reported for any of the outcome measures at 2 weeks.
Adverse events
Adverse events were reported in three articles, all RCTs. [29, 30, 45] Although there were no serious adverse events reported, two studies reported 6 minor events of which 5 were unrelated to trial procedures and 1 related to SMT. [45] In a large RCT [33], there were 62 events reported, where 19 were in the usual care group and 43 in the usual care and chiropractic care group. The majority (49/62) were reported as muscle or joint stiffness related to either chiropractic care, physiotherapy care or self-care.
Discussion
We found 20 articles that described chiropractic services within the active military worldwide. The majority of articles (n = 17) were from the US, with additional information provided from articles from Canada (n = 2) and Australia (n = 1). The majority were cross-sectional studies assessing utilization or access of chiropractic services or case reports highlighting common or unique conditions managed; there were only three RCTs evaluating chiropractic as an intervention in this setting. The majority of included articles were published between 2006 and 2010 (n = 9) but the more robust designed clinical studies were published in the last 2 years. There is less research related to chiropractic services in active military personnel compared to that involving veterans. [16, 47]
We found that chiropractic services are provided to active duty military in on-base clinical facilities in only one country, the US; this is driven by US legislation. [16] Regardless of location, services are typically accessed through a gatekeeper, usually a medical physician. [16, 44] Care delivery models vary but the extent of integration of chiropractic services within the US Military Health System remains unclear. In the US and Canada, chiropractic services are available to active duty military; however, they are delivered by paid contracted chiropractors in the US, as opposed to a third party insured military personnel benefit in Canada. It is unclear what service delivery models exist in countries other than the US and Canada as we located no articles describing this. However, it appears that the inherent gatekeeper referral processes influence the access to chiropractic services.
Reported 12-month utilization of chiropractic services in the US ranged from 2.9 to 10.5% between 2000 and 2013. [28, 32, 36, 37] Outside of the US, we found only one study reporting a 12% utilization of chiropractic services among Australian military aircrew. [33] The reported utilization seems similar to that reported in the general population. [48]
Aside from one randomized controlled trial which included acute LBP patients, most articles reported patients presenting with chronic musculoskeletal conditions. These findings are similar to those seen in the general population, where musculoskeletal conditions are the predominant reason for consulting chiropractors. [48] The frequency of chiropractic visits reported in cross-sectional studies ranged from a mean of 5.4 in a survey of US Military Treatment Facilities [31] to 5.7 in a single Canadian base [12]. In Canada, limits to covered benefits and policy may influence visit frequency.
Outcomes of care provided by chiropractors was positive in most of the reported clinical studies; however, six of these were case report designs that cannot evaluate effectiveness. In two included RCTs, outcomes favoured usual medical care and chiropractic care compared to standard medical care alone. These findings are consistent with recent LBP guidelines supporting the use of manual and conservative care. [49–51] However, in the larger LBP pragmatic trial [30], treatment included interventions of questionable effectiveness [51]; suggesting further clinical trial data are required to assess if practice is consistent with current guidelines.
In another RCT, the use of a short course (4 visits over 2 weeks) of chiropractic manual therapy to improve select measures of performance in special operations military personnel was no different from wait-list control. [45] Despite empirical evidence of performance enhancement following manual therapy, the immediate but not statistically significant longer-term effect reported in this study is consistent with findings in systematic reviews assessing the impact of manual therapy on performance. [52, 53]
Our review adds to a previous review examining the integration of chiropractic services in military and veteran health care facilities. [47] We add new information assessing chiropractic services in active duty military from articles in the US, Canada, and Australia. Unfortunately, we found no evidence of chiropractic services provided to active duty military in other countries. The majority of the articles emanated from the US where chiropractic services were included in the Military Health System since 1995. [47] Little is known about the nature of integration of chiropractic services in the US Military Health System, but evidence suggests that it varies from base-to-base. [16, 47] We add new information from Canada highlighting the challenges and opportunities of the inclusion of chiropractic services in active duty military. [44] Given utilization data is limited to the US and Australian Air Force, further descriptive studies are required to fill this gap worldwide.
Understanding the characteristics of chiropractic services provided is important in assessing and maximizing quality of care. [54] The significant expansion of chiropractic services within the US Military Health System has been largely driven by legislative directives, which in themselves may challenge the nature and extent of system integration. [16] If value of services is measured by system needs rather than that of the providers [16], then system and care-based outcomes are important assessment metrics required to ensure continued success. Our scoping review suggests little is known about the clinical and quality metrics of chiropractic services in active duty military globally. Qualitative studies could provide the necessary understanding of the system and resource barriers and potential opportunities for inclusion or expansion of chiropractic services worldwide.
Strengths and limitations
A strength of our scoping review was the systematic process used to collect and summarize the evidence from this diverse body of literature. A scoping review is the most appropriate method to collect and organize diverse information and to develop a picture of the existing evidence base when a broad research question is asked. [55] Our health sciences librarian conducted a broad and methodologically rigorous literature search, which was reviewed by a second librarian. Further, we searched two military specific databases in an effort to capture all discipline specific relevant articles. Study selection was based upon detailed inclusion and exclusion criteria to ensure that consensus between paired independent reviewers was transparent and reproducible.
There are limitations in this review. In keeping with the scoping review framework we collated the evidence on chiropractic care in the military and did not critically appraise the methodology of the reported articles. [19] Future systematic reviews focusing on the specific factors discussed in this review should include an appraisal of the study methods. We restricted our search to include articles in the English language, which may have excluded some relevant articles. However, chiropractic journals publish in English, which is recognized as the standard language of science, thereby reducing this risk. [56]
Conclusion
Our scoping review explored the available evidence related to chiropractic services within active duty military. The majority of the articles emanated from the US and were cross-sectional in nature. Two recent RCTs provide evidence of comparative effectiveness of adding chiropractic care to usual medical care. Despite the reported use of chiropractic services in Australia, Canada, and the US, there is little available published evidence related to the nature, use, and outcomes of chiropractic care in active duty military. Our review suggests the need for further qualitative, descriptive, and clinical trial data worldwide to inform the role and value of chiropractic services in active duty military globally.
Additional files
Acknowledgements
The authors would like to acknowledge the invaluable contributions to this scoping review by Kent Murnaghan.
Authors’ contributions
Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data;-DS, SM, DT, CC, ATV. Been involved in drafting the manuscript or revising it critically for important intellectual content-DS, SM, DT, CC, SF, ATV, PC. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content; and-DS, SM, DT, CC, SF, ATV, PC. Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved-DS, SM, DT, CC, SF, ATV, PC. All authors read and approved the final manuscript.
Funding
This research was undertaken, in part, thanks to funding from the Canadian Chiropractic Association and the Ontario Chiropractic Association to the Centre for Disability Prevention and Rehabilitation at the University of Ontario Institute of Technology. The funding sources had no role in the design, execution, analyses or interpretation of the data, or decision to submit results.
Competing interests
DS, SM, CC, PC and SF have received research funding from the Canadian national and provincial chiropractic organizations, either as salary support or for research project funding. SF is Deputy-Editor-in-Chief for Chiropractic and Manual Therapies; however, he did not have any involvement in the editorial process for this manuscript and was blinded from the editorial system for this paper from submission to decision.
References:
Spooner SP, Tyner SD, Sowers C, Tsao J, Stuessi K.
Utility of a sports medicine model in military combat concussion and musculoskeletal restoration care.
Mil Med. 2014;179:1319–1324. doi: 10.7205/MILMED-D-14-00191Rowe P, Hébert LJ.
The impact of musculoskeletal conditions on the Canadian forces.
In: Aiken A, Bélanger S, editors. Shaping the future: military and veteran health research.
Kingston: Canadian Defence: Academy Press; 2011. p. 377–91.Litow CD, Krahl PL.
Public health potential of a disability tracking system: analysis of U.S. navy and marine corps
physical evaluation boards 2005-2006.
Mil Med. 2007;172:1270–1274. doi: 10.7205/MILMED.172.12.1270Born J, Hawes R, Whitehead J.
Regular Force version: your health speaks volumes.
Ottawa: Government of Canada; 2010.
Results from health and lifestyle information survey of Canadian forces personnel 2008/2009Canadian Forces Health Services Group .
Surgeon General's Report 2014: Consolidation, Innovation, Readiness.
Ottawa: Government of Canada, Department of National Defence; 2014Ang B, Harms-Ringdahl K.
Neck pain and related disability in helicopter pilots: a survey of prevalence and risk factors.
Aviat Space Environ Med. 2006;77:713–719Wickes S, Scott J, Greeves J.
Epidemiology of flight-related neck pain in Royal air Force (RAF) aircrew.
Aviation, space, and environmental medicine. 2006. p. 298Hiebert R, Campello MA, Weiser S, Ziemke GW, Fox BA, Nordin M.
Predictors of Short-term Work-related Disability Among Active Duty
US Navy Personnel: A Cohort Study in Patients with
Acute and Subacute Low Back Pain
Spine J. 2012 (Sep); 12 (9): 806–816Smith Laurel, Westrick Richard, Sauers Sarah, Cooper Adam.
Underreporting of Musculoskeletal Injuries in the US Army:
Findings From an Infantry Brigade Combat Team Survey Study
Sports Health. 2016 (Nov); 8 (6): 507–513Canada Parliament House of Commons .
Standing Committee on National Defence. Ottawa: Government of Canada; 2014.
Caring for Canada's Ill and Injured Military Personnel (June 2014)
41st Parliament, 2nd Session; pp. 1–93Cote P, Wong JJ, Sutton D, Shearer HM, Mior S, Randhawa K, et al.
Management of Neck Pain and Associated Disorders: A Clinical Practice Guideline
from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration
European Spine Journal 2016 (Jul); 25 (7): 2000–2022Boudreau LA, Busse JW, McBride G.
Chiropractic Services in the Canadian Armed Forces: A Pilot Project
Military Medicine 2006 (Jun); 171 (6): 572–576McGee JC, Bise CG, Stevens JM.
An orthopedic performance improvement initiative at a small military treatment facility.
Mil Med. 2017;182:18–25. doi: 10.7205/MILMED-D-16-00141Brawley S, Fairbanks K, Nguyen W, Blivin S, Frantz E.
Sports medicine training room clinic model for the military.
Mil Med. 2012;177:135–138. doi: 10.7205/MILMED-D-11-00331Kelly EW, Bradway LF.
A team approach to the treatment of musculoskeletal injuries suffered by navy recruits:
a method to decrease attrition and improve quality of care.
Mil Med. 1997;162:354–359. doi: 10.1093/milmed/162.5.354Dunn AS, Green BN, Gilford S.
An Analysis of the Integration of Chiropractic Services Within
the United States Military and Veterans' Health Care Systems
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 749–757Green BN, Johnson CD, Lisi AJ, Tucker J.
Chiropractic Practice in Military and Veterans Health Care:
The State of the Literature
J Can Chiropr Assoc. 2009 (Aug); 53 (3): 194–204Lisi AJ, Brandt CA.
Trends in the Use and Characteristics of Chiropractic Services
in the Department of Veterans Affairs
J Manipulative Physiol Ther. 2016 (Jun); 39 (5): 381–386Arksey H, O'Malley L.
Scoping studies: towards a methodological framework.
Int J Soc Res Methodol. 2005;8:19–32. doi: 10.1080/1364557032000119616Levac D, Coquhoun H, O'Brien K.
Scoping studies: advancing the methodology.
Implement Sci. 2010;5:1–9. doi: 10.1186/1748-5908-5-69O'Brien KK, Colquhoun H, Levac D, et al.
Advancing scoping study methodology: a web-based survey and consultation of perceptions on terminology,
definition and methodological steps.
BMC Health Serv Res. 2016;16:305. doi: 10.1186/s12913-016-1579-zTricco AC, Lillie E, Zarin W, et al.
PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation.
Ann Intern Med. 2018;169:467–473. doi: 10.7326/M18-0850McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C.
PRESS peer review of electronic search strategies: 2015 guideline statement.
J Clin Epidemiol. 2016;75:40–46. doi: 10.1016/j.jclinepi.2016.01.021Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C.
An evidence-based practice guideline for the peer review of electronic search strategies.
J Clin Epidemiol. 2009;62:944–952. doi: 10.1016/j.jclinepi.2008.10.012US National Library of Medicine. MeSH.
Thomas Reuters. ENDNOTE.
Pawson R.
Evidence-based policy: the promise of 'realist synthesis'.
Evaluation. 2002;8:340–358. doi: 10.1177/135638902401462448Goertz C, Marriott BP, Finch MD, et al.
Military Report More Complementary and
Alternative Medicine Use Than Civilians
J Altern Complement Med. 2013 (Jun); 19 (6): 509–517Goertz CM, Long CR, Hondras MA, Petri R, Delgado R, Lawrence DJ, et al.
Adding Chiropractic Manipulative Therapy to Standard Medical Care
for Patients with Acute Low Back Pain: Results of a Pragmatic
Randomized Comparative Effectiveness Study
Spine (Phila Pa 1976). 2013 (Apr 15); 38 (8): 627–634Goertz CM, Long CR, Vining RD, Pohlman KA, Walter J, Coulter I.
Effect of Usual Medical Care Plus Chiropractic Care vs Usual Medical Care
Alone on Pain and Disability Among US Service Members With
Low Back Pain. A Comparative Effectiveness Clinical Trial
JAMA Network Open. 2018 (May 18); 1 (1): e180105 NCT01692275Herman PM, Sorbero ME, Sims-Columbia AC.
Complementary and Alternative Medicine Services in the Military Health System
J Altern Complement Med. 2017 (Nov); 23 (11): 837–843Jacobson IG, White MR, Smith TC, et al.
Self-reported health symptoms and conditions among complementary and alternative medicine users
in a large military cohort.
Ann Epidemiol. 2009;19:613–622. doi: 10.1016/j.annepidem.2009.05.001Netto K, Hampson G, Oppermann B, Carstairs G, Aisbett B.
Management of Neck Pain in Royal Australian Air Force Fast Jet Aircrew
Military Medicine 2011 (Jan); 176 (1): 106–109Petri RP, Jr, Delgado RE.
Integrative medicine experience in the U.S. Department of Defense.
Med Acupunct. 2015;27:328–334. doi: 10.1089/acu.2014.1067Ryan MA, Smith TC, Smith B, et al.
Millennium cohort: enrollment begins a 21-year contribution to understanding the impact of military service.
J Clin Epidemiol. 2007;60:181–191. doi: 10.1016/j.jclinepi.2006.05.009Smith TC, Smith B, Ryan MA.
Prospective investigation of complementary and alternative medicine use and subsequent hospitalizations.
BMC Complement Altern Med. 2008;8:19. doi: 10.1186/1472-6882-8-19White MR, Jacobson IG, Smith B, et al.
Health care utilization among complementary and alternative medicine users in a large military cohort.
BMC Complement Altern Med. 2011;11:27. doi: 10.1186/1472-6882-11-27Green BN, Sims J, Allen R.
Use of Conventional and Alternative Treatment Strategies
for a Case of Low Back Pain in a F/A-18 Aviator
Chiropractic & Osteopathy 2006 (Jul 4); 14: 11Green BN, Schultz G, Stanley M.
Persistent synchondrosis of a primary sacral ossification center in an adult with low back pain.
Spine J. 2008;8:1037–1041. doi: 10.1016/j.spinee.2007.04.003Green BN, Browske LK, Rosenthal CM.
Elongated Styloid Processes and Calcified Stylohyoid Ligaments in a Patient with Neck Pain:
Implications for Manual Therapy Practice
Journal of Chiropractic Medicine 2014 (Jun); 13 (2): 128–133B.N. Green, A.S. Dunn, S.M. Pearce, et al.,
Conservative Management of Uncomplicated
Mechanical Neck Pain in a Military Aviator
J Can Chiropr Assoc. 2010 (Jun); 54 (2): 92–99Lillie GR.
Resolution of Low Back and Radicular Pain in a 40-year-old Male United States Navy
Petty Officer After Collaborative Medical and Chiropractic Care
J Chiropractic Medicine 2010 (Mar); 9 (1): 17–21Morgan WE, Morgan CP.
Chiropractic care of a patient with neurogenic heterotopic ossification of the anterior longitudinal
ligament after traumatic brain injury: a case report.
J Chiropr Med. 2014;13:260–265. doi: 10.1016/j.jcm.2014.08.001Mior SA, Vogel E, Sutton D, et al.
Exploring Chiropractic Services in the Canadian Forces Health Services -
Perceptions of Facilitators and Barriers Among Key Informants
Military Medicine 2019 (May 1); 184 (5-6): e344–e351DeVocht J.W., Vining R., Smith D.L., Long C., Jones T., Goertz C.
Effect of Chiropractic Manipulative Therapy on Reaction Time
in Special Operations Forces Military Personnel:
A Randomized Controlled Trial NCT02168153
Trials. 2019 (Jan 3); 20 (1): 5College of Chiropractors of Ontario.
Scope of Practice and Authorized Acts. 2018.Green BN, Johnson CD, Daniels CJ, Napuli JG, Gliedt JA, Paris DJ.
Integration of Chiropractic Services in Military and Veteran Health Care Facilities:
A Systematic Review of the Literature
J Evid Based Complementary Altern Med. 2016 (Apr); 21 (2): 115–130Beliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussieres AE, Mior SA, et al.
The Chiropractic Profession: A Scoping Review of Utilization Rates,
Reasons for Seeking Care, Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35Chou R, Cote P.
The Global Spine Care Initiative: Applying Evidence-based Guidelines on the Non-invasive
gement of Back and Neck Pain to Low- and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 851–860Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM.
Prevention and Treatment of Low Back Pain: Evidence, Challenges, and Promising Directions
Lancet. 2018 (Jun 9); 391 (10137): 2368–2383Wong JJ, Cote P, Sutton DA, et al.
Clinical Practice Guidelines for the Noninvasive Management of Low Back Pain: A Systematic Review
by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration
European J Pain 2017 (Feb); 21 (2): 201–216Botelho MB, Alvarenga BAP, Molina N, Ribas M, Baptista AF.
Spinal manipulative therapy and sports performance enhancement: a systematic review.
J Manip Physiol Ther. 2017;40:535–543. doi: 10.1016/j.jmpt.2017.03.014Miners AL.
Chiropractic treatment and the enhancement of sport performance: a narrative literature review.
J Can Chiropr Assoc. 2010;54:210–221Lisi AJ, Khorsan R, Smith MM, Mittman BS.
Variations in the Implementation and Characteristics of Chiropractic Services in VA
Medical Care 2014 (Dec); 52 (12 Suppl 5): S97–104Armstrong R, Hall BJ, Doyle J, Waters E, Update C.
Scoping the scope' of a cochrane review.
J Public Health (Oxf) 2011;33:147–150. doi: 10.1093/pubmed/fdr015Green BN.
Improvements in the Journal of Chiropractic Education for 2013.
J Chiropr Educ. 2013;27:1–4. doi: 10.7899/JCE-13-100
Return to CHIROPRACTIC CARE FOR VETERANS
Since 8-09-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |