

Developing Integrative Primary Healthcare Delivery:
Adding a Chiropractor to the TeamThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Explore (NY). 2008 (Jan); 4 (1): 18–24 ~ FULL TEXT
Michael J. Garner, MSc, Michael Birmingham, PhD, Peter Aker, MSc, DC, David Moher, PhD, Jeff Balon, DC, MD, Dirk Keenan, DC, and Pran Manga, PhD
Carlington Community and Health Services,
Ottawa, Ontario, Canada.
michaelgarner@gmail.com

BACKGROUND: The use of complementary and alternative medicine has been increasing in Canada despite the lack of coverage under the universal public health insurance system. Physicians and other healthcare practitioners are now being placed in multidisciplinary teams, yet little research on integration exists.
OBJECTIVE: We sought to investigate the effect of integrating chiropractic on the attitudes of providers on two healthcare teams.
DESIGN: A mixed methods design with both quantitative and qualitative components was used to assess the healthcare teams. Assessment occurred prior to integration, at midstudy, and at the end of the study (18 months).
SETTING: Multidisciplinary healthcare teams at two community health centers in Ottawa, Ontario, participated in the study.
PATIENTS/PARTICIPANTS: All physicians, nurse practitioners, and degree-trained nurses employed at two study sites were approached to take part in the study.
INTERVENTION: A chiropractor was introduced into each of the two healthcare teams.
MAIN OUTCOME MEASURES: A quantitative questionnaire assessed providers' opinions, experiences with collaboration, and perceptions of chiropractic care. Focus groups were used to encourage providers to communicate their experiences and perceptions of the integration and of chiropractic.
RESULTS: Twelve providers were followed for the full 18 months of integration. The providers expressed increased willingness to trust the chiropractors in shared care (F value = 7.18; P = .004). Questions regarding the legitimacy (F value = 12.33; P < .001) and effectiveness (F value = 11.17; P < .001) of chiropractic became increasingly positive by study end.
CONCLUSION: This project has demonstrated the successful integration of chiropractors into primary healthcare teams.
Key words: Primary care, chiropractic, community health centers
From the FULL TEXT Article:
Introduction
Complementary and alternative medicine (CAM) usage has been increasing in the general Canadian population, despite the fact that most CAM treatments fall outside the standard coverage of the publicly financed health insurance system. [1] Scientific evidence demonstrating the potential role of CAM in primary healthcare is also increasing. [2, 3] These changes have resulted in courses on CAM being included in the curricula of many North American medical schools. [4, 5] Despite the increase in utilization, evidence for its use, and education in CAM, the integration of CAM into primary healthcare settings and teams is rare.
One type of integration that has been examined previously is that of nurse practitioners into primary care practices. [6, 7] The creation of an educational environment within the primary care setting is important for increasing the use of nurse practitioners. [6] Practitioners feel less anxiety about role overlap when a collaborative treatment approach is used, [8] although physicians continue to find it difficult to work as members of a team with other kinds of practitioners. [9] Even with these difficulties in collaborating and concerns about liability and responsibility, referrals to CAM providers from physicians are increasing in the United States, [10] Canada, [11] and the United Kingdom. [12]
In Ontario, providers who were once able to work independently are being positioned within multidisciplinary teams. It is important to understand how physicians work and integrate with nonconventional healthcare providers. Community health centers (CHCs) currently care for clients by using multidisciplinary healthcare teams. These teams serve as a readily available location for the exploration of the integration of nonconventional practitioners with conventional healthcare providers. In both the United States and Canada, CHCs are mandated to treat marginalized populations who have limited access to health services, including services not subsidized by the provincial healthcare plan. [13, 14] Just before the start of the study, chiropractic was delisted from the provincial healthcare plan, making this treatment inaccessible to the majority of CHC clients who do not have private healthcare insurance and who could not afford to attend otherwise. Previously, the provincial healthcare plan partially covered the cost of this service. Although chiropractors and medical doctors work concurrently in the Ontario healthcare system, there has yet to be a meaningful integration of these two professions. The present study was undertaken to investigate introducing chiropractic care, and the effect this integration had on the practice and attitudes of multidisciplinary primary care teams in Ottawa, Canada.
METHODS
Study Population
This project was implemented in two CHCs in Ottawa, Ontario, Carlington Community and Health Services and South-East Ottawa Centre for a Healthy Community, from July 2004 until March 2006. All physicians, nurse practitioners and degree-trained nurses employed at the two study sites were approached to participate in the study. Each center hired a chiropractor, who was integrated as a part-time member of the healthcare team and received salary and full benefits. Chiropractic services were available to all clients of either center free of charge. The chiropractors were selected on a variety of criteria, both to ensure a similar practice philosophy as that found at CHCs as well as personalities that would be a good fit with the other members of the healthcare team. Ethics approval for the study was obtained from the Ottawa Public Health Department Ethics Review Board.
Design
This study used a mixed methods design with quantitative and qualitative components, using questionnaires and focus groups to assess the healthcare teams. Providers were assessed at baseline (prior to integration), nine months later, and at study end (18 months) by using focus groups and quantitative questionnaires. Focus groups were used to broaden and complement the information gathered by the quantitative questionnaires. Focus group sessions and questionnaire administration were performed on the same morning. After the first two focus group sessions, educational sessions were run to expose providers to chiropractic treatment by demonstrations and presentations of the published evidence on chiropractic. These sessions were run by members of the research team (J.B., P.A., M.J.G.) and the chiropractors hired for the integration.
Provider Questionnaire
The questionnaire was developed to ascertain providers’ opinions, experiences with collaboration, and perceptions of chiropractic care. Each question used a seven-point Likert scale, ranked from strongly agree to strongly disagree for response. The questionnaire used was designed specifically for use in this study because the integration of chiropractors into medical settings had not been evaluated previously. The questionnaire was pilottested before the study began with providers at a CHC in Ottawa, similar to the two study CHCs, to insure clarity of the questions.
Provider Focus Groups
One member of the research team (M.J.G.) moderated the focus groups, which lasted between 60 and 90 minutes. Group sessions were recorded using nonconcealed microphones. The focus groups served as a forum for providers at both centers to communicate their experiences and perceptions of the integration and of chiropractic. At the initial session, we discussed chiropractic and its role in primary healthcare, along with perceptions and concerns about the study and the introduction of a new provider into the CHC. The second and final focus groups centered on how the providers’ views had or had not changed regarding chiropractic and how this influenced clinical practice and the success (or failure) of the integration. At the end of the study period, face-to-face interviews were performed with each of the chiropractors to assess the success of the collaboration from their point of view.
Statistical Analysis
Change in response over the three time periods was assessed by repeated measures analysis of variance, with the general linear model procedure in SAS version 9.1 (SAS Institute Inc., Cary, NC). Post hoc analyses were performed on all statistically significant main effects. Quantitative questionnaires were based on those used elsewhere. [7] The focus group audiotapes were transcribed for analysis. The Spencer and Ritchie qualitative framework served as a guide for the qualitative analysis. [15] Analysis involved an initial search for recurrent themes, focusing on the impact of the integration. This process involved familiarization with the data, identification of themes, then examining changes in provider’s perceptions and attitudes over the course of the study. This study was done in accordance with the Ottawa Public Health Ethics Review Board and received ethics approval in August 2003.
RESULTS
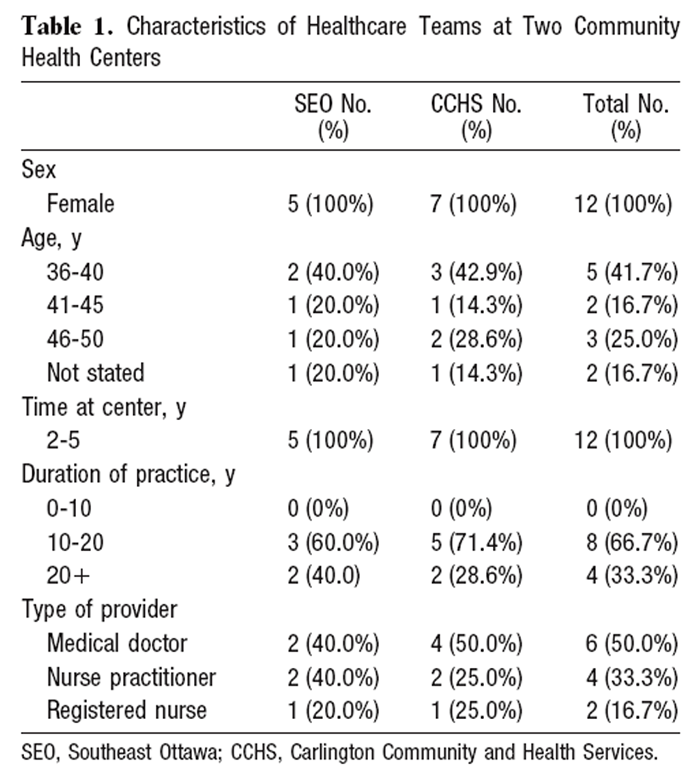
Table 1 Twelve providers were followed for the full 18 months of integration. Eight other providers were eligible for inclusion at the beginning of the study: three left their job; four took new positions at the centers, and one nurse refused involvement in the study. The results reported only pertain to the twelve providers followed for the full 18-month integration. The mean age of the providers was 44.1 years, and they all had worked at their centers between two and five years (Table 1). Each chiropractor had been in practice more than 5 years and had prior experience working in at least one multidisciplinary medical setting.
Collaboration
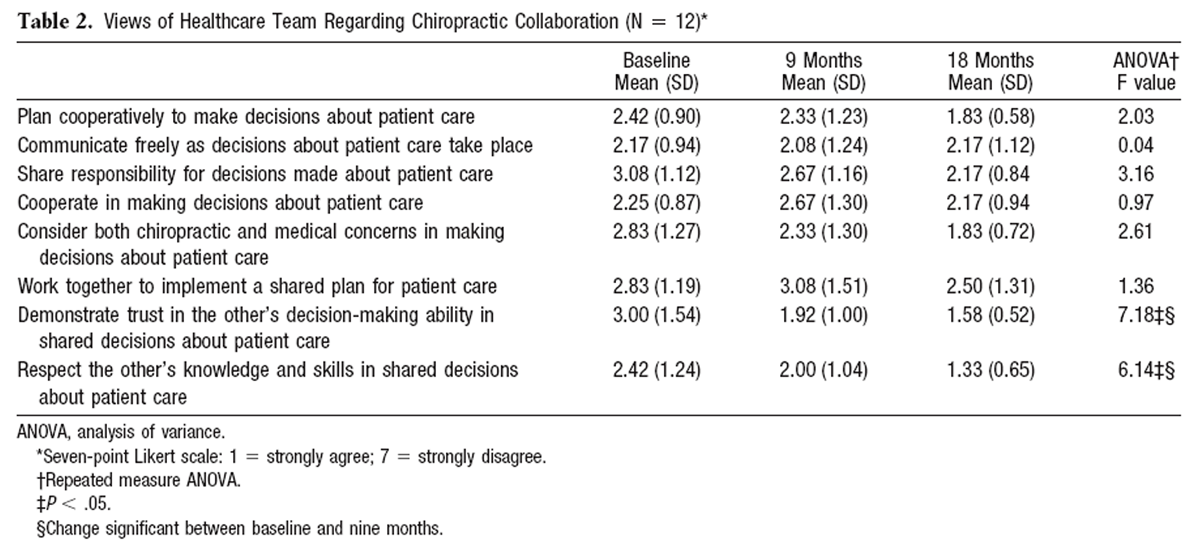
Table 2 Provider attitudes toward collaboration with the chiropractor changed over time (Table 2). The healthcare team expressed increased willingness to trust the chiropractor in shared-care cases (F-value = 7.18; P = .004) and had greater respect for the chiropractor’s knowledge and skills (F-value = 6.14; P = .008). For other questions of collaboration, the providers were generally neutral in their attitudes at baseline, and there were no significant changes over the study period.
Attitudes Toward Chiropractic
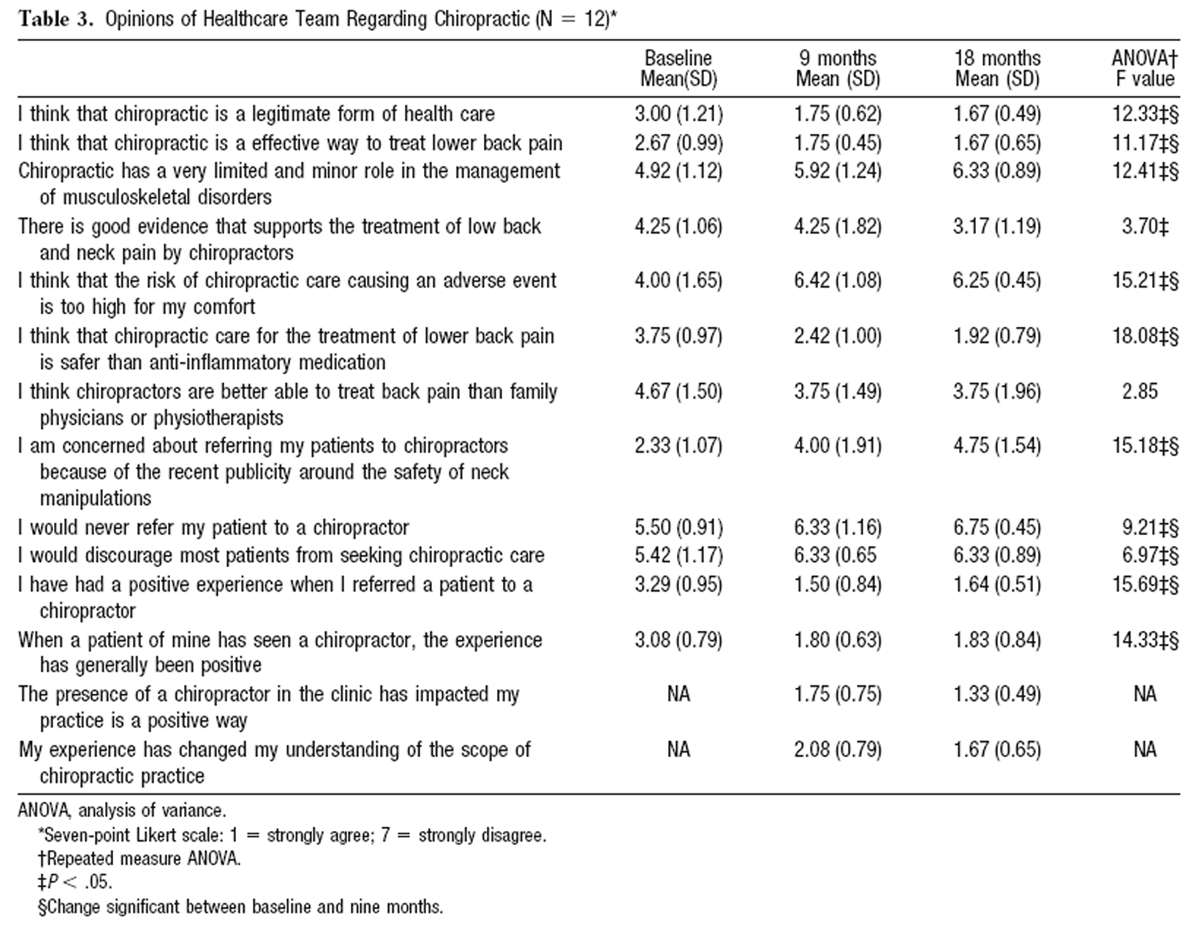
Table 3 We observed a shift during the integration in the attitude of healthcare providers toward chiropractic (Table 3). General questions regarding both the legitimacy of chiropractic as a form of healthcare (F value = 12.33; P < .001) and the effectiveness of chiropractic (F value = 11.17; P < .001) moved from neutral responses to increasingly more positive responses. By study end, the providers were indicating that chiropractic care for low back pain was safer than anti-inflammatory medication (F value = 18.08; P < .001). Initial skepticism about the efficacy and safety of chiropractic dissipated by the end of the study (F value = 15.21; P = .001). Questions regarding experiences with the chiropractor and patient outcomes moved from neutral to positive over the course of the study (F value = 15.69; P = .001). The providers also indicated that the presence of the chiropractor on the healthcare team impacted their practice in a positive way and influenced their understanding of chiropractic (mean response at 18 months, 1.33). Post hoc analysis of variables that changed significantly over the study revealed that the most of the change occurred between baseline and nine months, as opposed to the second half of the study.
Focus Group
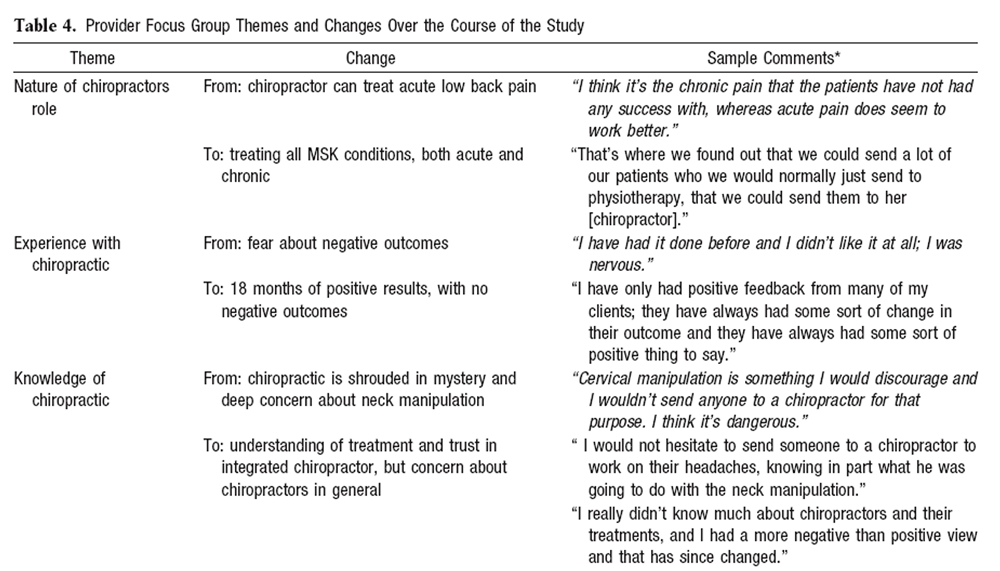
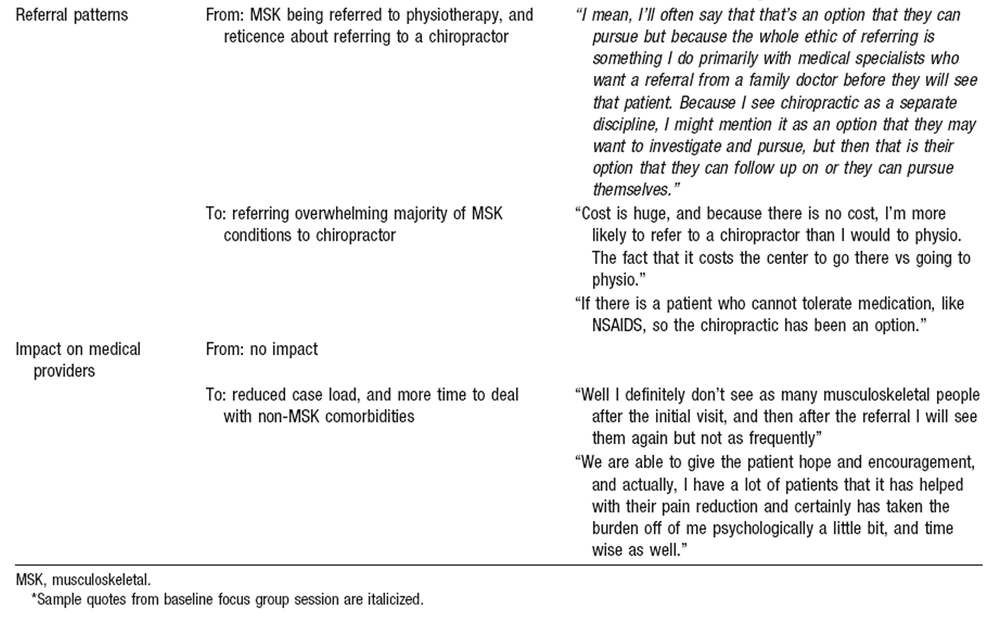
Table 4 A
Table 4 b Analysis of the focus group data revealed a shift within the medical teams from negative and limited views of chiropractic to a generally positive attitude toward having a chiropractor on the healthcare team (Table 4). The providers’ understanding of the scope of the chiropractor’s role increased markedly over the course of the study. The providers at both sites referred conditions of increasing complexity over the study, particularly the referral of chronically disabled individuals; a typical comment was “Well, I definitely don’t see as many musculoskeletal people after the initial visit.” The healthcare team expressed that patient response to chiropractic care was almost always positive. It is noteworthy that there were no negative outcomes observed in the study at either center, as seen in the following representative comment: “I have only had positive feedback from many of my clients; they have always had some sort of change in their outcome and they have always had some sort of positive thing to say.”
Providers’ understanding of chiropractic changed over the course of the study period, from seeing it as a largely unknown practice to understanding both the science and the actual practice of chiropractic. Initially, the providers did not think the introduction would impact their practice. By the end of the study period, the change in caseload because of the additional treatment option chiropractic provided, and relief to the healthcare team stemming from referring difficult cases — those for whom the conventional medical treatment options had been ineffective — to the chiropractor proved to have a positive impact on the providers’ individual and group practice. A representative comment was “We are able to give the patient hope and encouragement, and actually, I have a lot of patients that it (chiropractic) has helped with their pain reduction and certainly has taken the burden off of me psychologically a little bit and time wise as well.” It is important to note that the providers remained skeptical about chiropractors in general and would only consider referring to other chiropractors if they were demonstrated to be similar in skill and practice methodology to the integrated chiropractor.
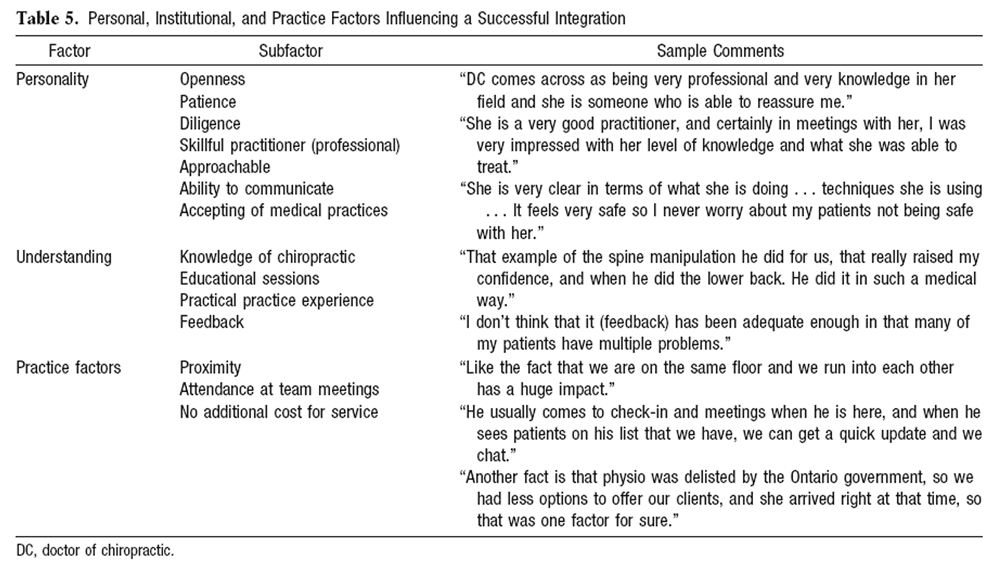
Table 5 The focus groups also elucidated the factors that were important to the successful integration of a chiropractor into a multidisciplinary healthcare team (Table 5). The main factors were the personality of the chiropractor, the healthcare provider’s understanding of chiropractic care, and the practice characteristics, such as team meetings and how the clinic is physically set up.
Chiropractor Interviews
Post-integration interviews with the chiropractors revealed that the integration was ultimately a success. Both chiropractors remarked that the length of time and amount of effort to gain the trust of the doctors and nurses on the healthcare team was large. However, once interpractitioner trust had been established, the collaborative practice that ensued was beneficial to the chiropractor as a professional and increased the scope of care provided to his/her patients.
DISCUSSION
Our results indicate that integrating chiropractic care into an established conventional medical setting, specifically a CHC, can be achieved with a high degree of comfort, as reported by healthcare providers and patients alike. These data are in sharp contrast to other published opinions. Kelner and colleagues [11] saw the integration of CAM as a distant possibility that would be extremely difficult to achieve. They did not favor this kind of integration and raised doubts about the competence of the CAM providers as well as the feasibility of working together. The collaboration observed in this study involved referrals back and forth between the chiropractor and the medical doctors, case collaboration on the treatment of certain patients, and seeking advice and diagnostic opinions from each other.
During the initial assessment, we observed the providers’ doubts about the competence of the chiropractors and the concerns about collaboration. Over the course of the study, these concerns dissipated and were replaced by a largely positive view of collaboration and working with chiropractors as equal team members. Although concern about chiropractic in general remained, the providers did state that they would be comfortable with a different chiropractor who shared the same abilities and practice methodology as the integrated chiropractor.
We found that interprofessional education was useful in reducing both the concerns about chiropractic and the team’s reluctance to collaborate with the chiropractor. The providers indicated that presentation of peer-reviewed research on chiropractic and the demonstrations of chiropractic treatments were useful in dispelling misconceptions and concerns toward the safety and efficacy of chiropractic and manipulation. The importance of interprofessional education has been previously stated as very important for addressing collaboration problems. [16]
Additional factors influencing the success of the integration were positive clinical outcomes for the patients referred to the chiropractor and the provision of chiropractic as a free service to the clients of each CHC; these factors were significant because many other treatments (eg, physiotherapy and massage therapy) for musculoskeletal disorders were inaccessible by this patient population because of cost. Also, communication between the chiropractor and the healthcare team was facilitated by the inclusion of the chiropractor in weekly team meetings and other team development activities.
The post hoc analysis performed on the change in provider’s opinions of chiropractic and collaboration revealed that the majority of the change occurred in the first nine months of the project. This suggests that integration of nonconventional healthcare workers into multidisciplinary teams can occur in less than a year, given sufficient educational and logistic support. Previous studies indicated that a minimum of 18 months is required for team formation. [17]
Negative attitudes and differences in ideology between professions have been cited as a barrier to team functioning. [18, 19] Previous studies have observed that the attitude toward chiropractors in the conventional medical community is generally poor, with only 23% considering chiropractors legitimate healthcare providers, whereas 95% considered physiotherapists legitimate. [20] The same study found that only 35% of general practitioners surveyed thought it ethical to deal with a chiropractor. [20] Although the concern related to chiropractic in the present study was not as great as that observed previously, the providers at both sites were generally concerned about this integration. The results of the study suggest that access to in-house chiropractic care may improve provider perception, and that chiropractors can be successfully integrated in a multidisciplinary primary care setting.
There are several limitations to this study. The sample of providers is small (N = 12) and only includes two multidisciplinary healthcare teams. There may be unique aspects to these teams that would prevent the results of the integration from being generalized to other healthcare teams. In particular, healthcare teams at CHCs collaborate as part of their inherent culture, and they are accustomed to working with new practitioners and treatment modalities. The sample of medical providers was all female, which may influence the generalizability of the results to male practitioners. The current setting provides both chiropractic and medical care free of charge to the client. It is unclear if the integration would be more or less difficult in situations with different financial agreements. In addition, the tool used for the quantitative study was unvalidated.
The two integration sites in this study were quite similar, with two important differences. First, the Carlington site used an integrated medical chart where both the chiropractic records and the medical records were in the same nonelectronic file. At the Southeast Ottawa site, the medical and chiropractic charts were separately maintained with limited accessibility to other team members. This meant progress attributable to chiropractic was difficult to ascertain, and this was identified by healthcare team members as a barrier to integration.
The second important difference was the presence of a volunteer chiropractic clinic at Carlington for the five years prior to the start of this study. [21] This clinic operated with a high turnover of chiropractor volunteers, with the resulting negative opinions due to a lack of continuity of care. This created a situation where the chiropractor being integrated at that site had to overcome and demonstrate the differences in clinic practices between the integrated practice and the volunteer clinic. This caused a delay in the process, but over the first few months as the healthcare team interacted with the chiropractor and experienced initially positive outcomes from patients, the integration proceeded in a similar way to the other site.
The success of the integration of chiropractors into multidisciplinary healthcare teams that was observed in this study should help provide a framework for future sites attempting similar integrations. For successful integration, it is important to first choose a professional who is willing to put significant effort into building relationships with the healthcare team and endure initial skepticism. We also found that having an experienced chiropractor (minimum of five years practice) was important to the integration, because their practice experience and ability created an environment where the healthcare team could be confident in the chiropractic care given. There should also be involvement of healthcare team members in the selection of the chiropractor so communication styles and personality traits are such to facilitate working with the existing team.
CONCLUSION
This project demonstrated the importance of structuring and scheduling interactions between the established healthcare team and the chiropractors to facilitate a successful integration. We used formal education sessions to help dispel misconceptions about chiropractic and had the chiropractor scheduled into weekly clinical rounds. This integration had a positive impact on providers’ individual practices and changed opinions and views of healthcare practitioners toward chiropractic, resulting in conventional and nonconventional healthcare providers working together on a collaborative healthcare team. However, given the small sample size and other limitations, the results may not be generalizable to other healthcare settings.
References:
So, J. (1997)
Utilization of alternative therapies by the Canadian population.
The Report of the Conference on Taking Charge of Health:
Exploring Alternative Health Care.
Peterborough, Ontario: Trent University; 1997.Barnes J, Abbot NC, Harkness EF, Ernst E.
Articles on complementary medicine in the mainstream medical literature:
an investigation of MEDLINE, 1966 through 1996.
Arch Intern Med. 1999;159:1721-1725.van Haselen RA, Reiber U, Nickel I, Jakob A, Fisher PA.
Providing complementary and alternative medicine in primary care: the primary care
workers’ perspective.
Complement Ther Med. 2004;12:6-16.Ruedy J, Kaufman DM, MacLeod H.
Alternative and complementary medicine in Canadian medical schools: a survey.
CMAJ. 1999; 160:816-817.Wetzel MS, Eisenberg DM, Kaptchuk TJ.
Courses Involving Complementary and Alternative Medicine at US Medical Schools
JAMA. 1998 (Sep 2); 280 (9): 784-787Huang PY, Yano EM, Lee ML, Chang BL, Rubenstein LV.
Variations in nurse practitioner use in Veterans Affairs primary care practices.
Health Serv Res. 2004;39(4 pt 1):887-904.Way D, Jones L, Baskerville B, Busing N.
Primary health care services provided by nurse practitioners and family physicians
in shared practice.
CMAJ. 2001;165:1210-1214.Booth J, Hewison A.
Role overlap between occupational therapy and physiotherapy during in-patient
stroke rehabilitation: an exploratory study.
J Interprof Care. 2002;16:31-40.Shuval JT, Mizrachi N, Smetannikov E.
Entering the well-guarded fortress: alternative practitioners in hospital settings.
Soc Sci Med. 2002;55:1745-1755.Kessler RC, Davis RB, Foster DF, et al.
Long-Term Trends in the Use of Complementary and Alternative Medical Therapies
in the United States
Annals of Internal Medicine 2001 (Aug 21); 135 (4): 262–268Kelner M, Wellman B, Boon H, Welsh S.
Responses of established healthcare to the professionalization of complementary
and alternative medicine in Ontario.
Soc Sci Med. 2004;59:915-930.Thomas KJ, Carr J, Westlake L, Williams BT.
Use of non-orthodox and conventional health care in Great Britain.
BMJ. 1991;302:207-210.Association of Ontario Health Centres.
Available at: www.aohc.org
Accessed February 17, 2006.Forrest CB, Whelan EM.
Primary care safety-net delivery sites in the United States: a comparison of
community health centers, hospital outpatient departments, and physicians’ offices.
JAMA. 2000;284: 2077-2083.Ritchie J, Spencer L.
Qualitative data analysis for applied policy research.
In: Bryman A, Burgess RG, eds.
Analyzing Qualitative Data.
London, England: Routledge; 1995:174-194.Reeves S, Freeth D, McCrorie P, Perry D.
‘It teaches you what to expect in future . . . ’: interprofessional learning on
a training ward for medical, nursing, occupational therapy and physiotherapy students.
Med Educ. 2002;36:337-344.Nancarrow S.
Dynamic role boundaries in intermediate care services.
J Interprof Care. 2004;18:141-151.Dalley J, Sim J.
Nurses’ perceptions of physiotherapists as rehabilitation team members.
Clin Rehabil. 2001;15:380-389.Bradford R.
Obstacles to collaborative practice.
Nurs Manage. 1989; 20:72I, 72L-72M, 72P.Simpson JK.
A study of referral patterns among Queensland general medical practitioners
to chiropractors, osteopaths, physiotherapists and others.
J Manipulative Physiol Ther. 1998;21:225-231.Baskerville N, Keenan D.
How chiropractors began working in a community health centre in Ottawa.
J Can Chiropr Assoc. 2005;49: 13-20
Return to INTEGRATED HEALTH CARE
Since 6-20-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |