

What Should Health Care Systems Consider When Implementing
Complementary and Integrative Health: Lessons
from Veterans Health AdministrationThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Altern Complement Med 2019 (Mar); 25 (S1): S52–S60 ~ FULL TEXT
OPEN ACCESS Stephanie L Taylor, Rendelle Bolton, Alexis Huynh, Kelly Dvorin, A Rani Elwy, ET. AL.
Center for the Study of Healthcare Innovation,
Implementation and Policy CSHIIP,
Greater Los Angeles VA Medical Center,
11301 Wilshire, Building 206, 2nd Floor
Los Angeles, CA

Objectives: Health care systems are increasingly interested in becoming whole health systems that include complementary and integrative health (CIH) programs approaches. The nation's largest health care system, the Veterans Health Administration (VA), has been transforming to such a system. However, anecdotal evidence suggested that many VA medical centers have faced challenges in implementing CIH approaches, whereas others have flourished. We report on a large-scale, research-operations partnered effort to understand the challenges faced by VA sites and the strategies used to address these to better support VAs implementation of CIH nationally.
Design: We conducted semi-structured, in-person qualitative interviews with 149 key stakeholders at 8 VA medical centers, with content based on Greenhalgh's implementation framework. For analysis, we identified a priori categories of content aligned with Greenhalgh's framework and then generated additional categories developed inductively, capturing additional implementation experiences. These categories formed a template to aid in coding data.
Results: VA sites commonly reported that nine key factors facilitated CIH implementation: (1) organizing individual CIH approaches into one program instead of spreading across several departments; (2) having CIH strategic plans and steering committees; (3) strong, professional, and enthusiastic CIH program leads and practitioners; (4) leadership support; (5) providers' positive attitudes toward CIH; (6) perceptions of patients' attitudes; (7) demonstrating evidence of CIH effectiveness; (8) champions; and (9) effectively marketing. Common challenges included are: (1) difficulties in hiring; (2) insufficient/inconsistent CIH funding; (3) appropriate patient access to CIH approaches; (4) difficulties in coding/documenting CIH use; (5) insufficient/inappropriate space; (6) insufficient staff's and provider's time; and (7) the health care cultural and geographic environments. Sites also reported several successful strategies supporting CIH implementation.
There are more articles like this @ our new:
NON-PHARMACOLOGIC THERAPY PageConclusions: VA sites experience both success and challenges with implementing CIH approaches and have developed a wide range of strategies to support their implementation efforts. This information is potentially useful to other health care organizations considering how best to support CIH provision.
Keywords: acupuncture; implementation research; integrative medicine; mindfulness; veterans; yoga.
From the FULL TEXT Article:
Introduction
Health care systems are increasingly interested in supporting their patients' use of complementary and integrative health (CIH) programs approaches. [1–4] This could be due in part to mounting evidence that some CIH approaches work for some health conditions, [5–15] patient preference for nonpharmacological treatment options, [16–18] CIH approaches' potential to reduce health care costs, [3, 19] and recent pain management clinical guidelines [20] and pain management strategies [21, 22] recommending CIH approaches for pain.
The nation's largest health care system, the Veterans Health Administration (VA), has been providing CIH approaches for patients for many years. In 2011, 89% of VA medical centers offered at least two CIH approaches, [2] which is twice what non-VA medical centers reported offering. [1] In 2015, 93% had at least two CIH approaches. [23]
The VAs implementation of CIH approaches has accelerated for several reasons, in addition to those described above. First, veteran interest in CIH approaches is strong. Our 2017 national study (article under review) showed 84% of veterans were interested in learning about or trying them and 52% reported using them in the past year. Second, the VA has been undergoing a transformation from a medical/disease-based system of care to a health care system that addresses the whole patient. This Whole Health System [24] transformation is being led by the VA Office of Patient Centered Care and Cultural Transformation (OPCC&CT) and offers CIH approaches as a core component. The acceleration in VA CIH implementation is also due to the 2016 Comprehensive Addiction and Recovery Act (CARA), which mandated that CIH provision and research should be expanded in the VA. [25] Accordingly, in 2018, the VA devoted significant resources to the Whole Health System transformation to support 18 VA medical centers across the nation (per Section 933 of the CARA legislation), one in each of the 18 VA medical networks, to provide widespread access to CIH approaches. Additionally, as of May 2017, eight CIH approaches are covered under the veterans medical benefits package: acupuncture, massage, guided imagery, biofeedback, hypnotherapy, t'ai chi, yoga, and meditation (chiropractic care was already considered as VA conventional care years ago).
When this increased VA prioritization of CIH provision began, anecdotal evidence suggested that most VA sites faced a variety of challenges in implementing CIH approaches, whereas a few flourished. The VA OPCC&CT had little systematic knowledge of the array of sites' challenges and what successful implementation strategies sites were using, information that is essential in the attempt to support sites' CIH implementation via policy and operational practice change. This article reports on a VA research-operations partnered effort to support the VAs implementation of CIH approaches by conducting a large-scale qualitative effort to address that knowledge gap. This information is being used to facilitate CIH implementation throughout the VA and is also potentially useful to other health care organizations as they consider how best to support CIH provision.
Materials and Methods
Overview
We examined facilitators, barriers, and strategies used to overcome barriers to CIH implementation by conducting semi-structured qualitative interviews with 149 key stakeholders at 8 VA medical centers during 2–day site visits between February and August 2015. By CIH, we mean the eight types of CIH the VA now covers as medical treatments: yoga, t'ai chi, acupuncture, meditation, chiropractic, massage, guided imagery, biofeedback, and hypnotherapy.
The VA Institutional Review Board determined this to be program evaluation for quality improvement purposes.
Recruitment

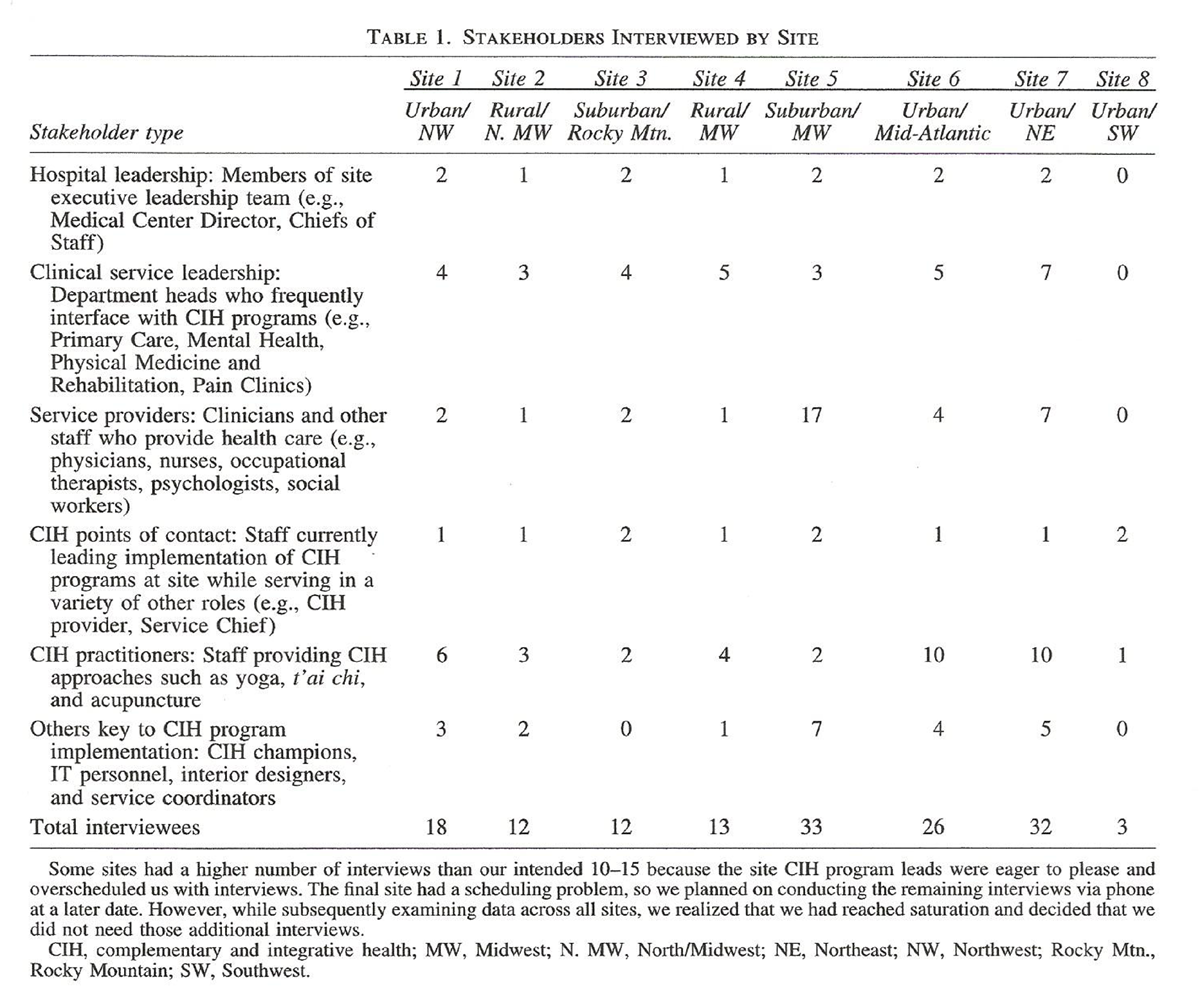
Table 1 We selected sites by first posting a recruitment notice on the VAs national CIH clinical listserv, eliciting interest from 36 medical centers. Among those, we conducted 30–min screening interviews with CIH program leads at sites offering at least three CIH approaches to identify sites with robust programs and implementation experiences, resulting in 17 sites. From those, we selected eight to obtain site variation in geographic location and rural/urban status (Table 1).
Data collection and analysis
We collaborated with CIH program leads at the eight sites to identify six types of key stakeholders with whom to hold individual interviews (Table 1), making it clear that we were interested in speaking with both CIH proponents and skeptics. Four researchers experienced in qualitative methods conducted interviews (two researchers per site) using a semi-structured interview guide. This guide was informed by constructs from Greenhalgh's Model of Diffusion of Innovations in Service Organizations [26] and our prior knowledge of VA CIH implementation issues, so that we asked about the most salient constructs related to CIH programs. Topics included awareness of CIH approaches offered, capacity and use of CIH, CIH referral process, providers' attitudes toward CIH, strategies used to overcome challenges, available resources, leadership support, and champions. Questions varied depending on stakeholders' roles. Interviews lasted up to 1–h and were audio-recorded, with recordings supplementing the notes taken during interviews.
We coded and synthesized interview notes to form templated summaries for each site. We first identified a priori categories to capture content aligned with Greenhalgh's framework constructs and then generated additional categories developed inductively that captured additional implementation issues. These categories formed a template that we then used to code data and develop site-level implementation summaries. The two researchers assigned to each site discussed content not clearly fitting into categories until consensus was reached. All researchers reviewed the final implementation summaries merged them to capture the range of implementation experiences across sites.
Results
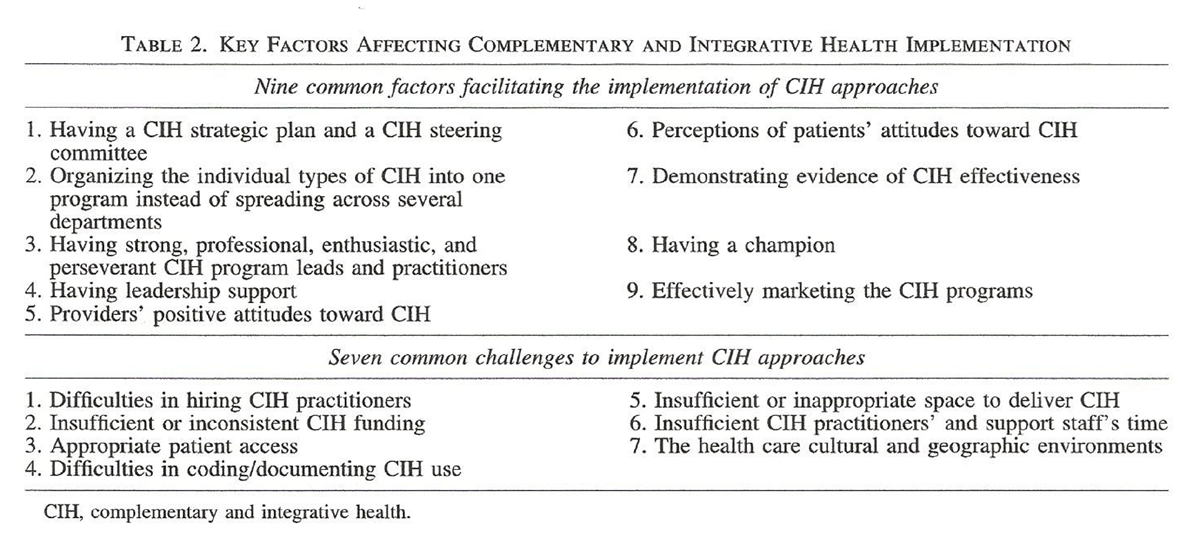
Table 2 Several VA respondents at all sites reported that nine key factors facilitated their implementation of CIH approaches and also reported seven key challenges (Table 2). They also commonly reported several successful strategies to support CIH implementation, as noted below.
Having a CIH strategic plan and steering committee
One respondent said that the most important thing they would tell other facilities to do is have a strategic plan:[T]aking the time to put together a strategic plan with a vision and a mission and, you know, three things that we want to do this year, … and an articulation of what those are and why that fits into an overall vision for integrative health at the hospital is important.… People sat around in working groups for years and years and years thinking beautiful thoughts, right, but putting them on paper makes a difference and so I would say have the discipline and take the time…. to come up with a short strategic plan.
Respondents said having a CIH Steering Committee could help legitimatize CIH programs and make them more visible and integrated. It also could foster collaboration, make CIH programming decisions or recommendations on behalf of the hospital, brainstorm to overcome CIH implementation issues, and increase CIH visibility/awareness across the facility. This Committee could also develop validation procedures for CIH practitioners in professions in which the Professional Standards and Practice Boards will not credential them in CIH modalities. Finally, it could bring together representatives from departments across the hospital who are interested in CIH as well as instructors/providers of CIH approaches.
Organizing the CIH approaches into one main integrated CIH program instead of
spreading individual CIH approaches across several departments
VA medical centers located their CIH approaches:(1) all under one program,
(2) individually with various CIH approaches embedded in different departments, or
(3) a combination thereof.Sites using the second or third approach reported provider and patient confusion about what CIH approaches were available and how to refer to them. Having one main CIH program seems to allow for greater efficiency, facilitates referrals because providers are more easily aware of the CIH therapies available, and results in clearer “ownership” of CIH approaches. As one department chair said,
[At first] we didn't have any department to own the programs. We love it [CIH] and we want to do it. But the problem is owning and sustaining. There are crises and demands that pop up, and [XX department] was able to bring in CIH and make it sustainable.
Having strong, professional, and enthusiastic CIH program leads and practitioners
Characteristics of CIH program leads and practitioners are important in garnering support for CIH approaches. Many said that if CIH program leads or practitioners are seen as “loosey goosey” or “out there,” they and the CIH approaches they provide are often viewed with skepticism.
Strategies
To counter this skepticism and gain support, respondents said that it is critical for CIH program leads to have a business-oriented mind to be able to do things, such as develop strategic plans, make a business case for CIH, and speak effectively to facility directors and physicians. The CIH program lead should also be very visible and regularly reach out to leadership and departments and befriend would-be skeptics; have strong interpersonal, communication, and leadership skills; have a command of the CIH evidence and be able to present it effectively; and be resourceful and persevere in the face of bureaucratic challenges. For garnering support for CIH programs, it is especially effective if CIH program leads are also physicians. As one physician who provides both CIH approaches and clinical care said,We are in a medical field, right, so there is something about being able to speak dual languages and saying things in a way that the people you are trying to communicate with can hear … There is a level of credibility …. having done all the other therapies, right, for me to say, okay this [a CIH practice] can also be helpful, people are like, ‘Oh okay, you know she's not just some like flaky hippy chick.’ She can talk clinical, she can talk our language, and she gets that …
We also consistently heard that if it were not for the passion and determination of the CIH program leads and practitioners, the CIH programs might falter. The process of implementing CIH in the VA involves many challenges, so it is critical that CIH leaders have perseverance to overcome implementation challenges.
Having leadership support
As with most new practices being implemented in institutions, having the support of executive leadership and service line managers is fundamental to CIH implementation. Support includes things such as providing funding for positions, allowing existing staff time to provide CIH, and providing space or equipment. Many respondents experienced a lack of leadership support at some time, which ranged from leaderships' skeptical attitudes to a complete unawareness that some CIH approaches were being offered at their facility. Some leadership reportedly gave more support to CIH practitioners they saw as being “more medical,” which was viewed as being licensed and credentialed to treat a specific diagnosis (e.g., acupuncture, biofeedback, or meditation).
Strategies
Leadership also reported that they are more likely to support CIH approaches that:(1) are linked to their medical facility's priorities, national initiatives, or national pain guidelines;
(2) are cost-effective;
(3) have evidence of effectiveness; or
(4) lead to increased patient satisfaction (which also is a VA priority).Respondents found leadership support increased when leadership was given opportunities to experience CIH approaches for themselves at CIH open houses or fairs, to hear from MDs who support CIH approaches.
Physicians' attitudes toward CIH approaches
Physicians are key to patients' use of CIH approaches because they can persuade or dissuade patients from using CIH approaches. As with medical facility leadership, providers range in their degree of skepticism or support of CIH. As one CIH program lead noted, there will always be a percentage of providers who do not support the use of CIH, despite the team's best efforts to educate and inform them:20% are gung-ho and supportive; 60% need some convincing, but come around;
and 20% are strongly against [CIH approaches].A few physician respondents reported that some of their peers were wary of CIH approaches because they did not understand the mechanisms at work and that others felt threatened because patients were getting better without their medical expertise.
Strategies
Physicians responded positively to CIH approaches when they were positioned as:(1) alternatives to pain medication,
(2) options for complex patients who have not gotten better with Western biomedicine, or
(3) standard therapies that psychologists have delivered for years (meditation, guided imagery, etc.).Some were more supportive of the “active” self-management CIH approaches (e.g., yoga and t'ai chi) than of the “passive” CIH approaches (massage and acupuncture) because they would like patients more actively engage in their treatment. Providers also said that they responded to:
(1) having patients provide feedback about their CIH practice utilization,
(2) experiencing CIH approaches for themselves, and
(3) seeing summaries of randomized clinical trials.Respondents also said that, when speaking with skeptical physicians, it is important to meet with them individually to determine what their beliefs are because skeptical physicians might not voice their opinions among peers.
Perceptions of patients' attitudes toward CIH approaches
Many physicians said that some patients were open to try CIH approaches and reported them effective. Some noted their patients perceived CIH approaches such as t'ai chi or chair-based yoga as safe and gentle, whereas others' patients were reluctant to try them because they felt that they were “mystical” or “exercise-in-disguise.”
Strategies
Physicians and CIH program leads reported that providing opportunities for patients to try CIH approaches or to witness them being delivered in CIH “fairs” or in waiting rooms was particularly persuasive, just as those experiences are persuasive for medical leadership or physicians. Respondents also told us that patients who used CIH approaches are strong CIH advocates for other patients. For example, one physician had a patient volunteer to talk to other patients in her group clinics about her positive experiences with CIH approaches. Another regularly shows patients who have lost hope a YouTube video of a wounded veteran doing yoga with a professional wrestler. In educating patients about CIH approach options, respondents said that it was helpful to explain to patients:(1) what CIH approaches are,
(2) what they entail, and
(3) what kinds of outcomes they might expect, including peace, calmness, and sense of well-being.They also stressed that language is critical; many patients, especially veterans, do not want to be told that they are weak or that something so gentle can be effective. They suggested framing CIH approaches as:
(1) training (e.g., basic training physically conditions and CIH approaches emotionally condition, build skills, and deal with emotions through physical means);
(2) a “warrior” activity (e.g., calling it “yoga warriors” instead of “yoga” dramatically increased attendance); and
(3) “movement” (e.g., t'ai chi and qigong), which can be essential in pain control.
Demonstrating evidence of CIH effectiveness
As noted above, evidence of CIH effectiveness is key to gaining support and managing skepticism among stakeholders. Evidence can mean“evidence of use” (e.g., number of users),
evidence of patient satisfaction,
“scientific” evidence of effectiveness (e.g., improvements in health or quality-of-life measures), or
“business case” evidence (return on investment or cost-effectiveness analysis).
Strategies
Facility leadership usually reported wanting data on return on investment, patient feedback, the number of patients served, and how CIH approaches have reduced opiate prescribing. Department heads and physicians usually reported wanting information on the mechanisms of action that makes a CIH approach effective or results from scientifically rigorous studies of clinical outcomes.Present evidenced-based medicine, peer reviewed articles,
publications in reputable journals, and stick with that.However, many physicians told us that when their patients find a CIH approach has been helpful, they care less about the amount of research supporting it.
Having champions
Almost all respondents mentioned that it is critical to have a champion to support and push forward their CIH program efforts, with many of those champions being department heads or leadership. Champions are typically important when attempting to implement most interventions, but especially so with CIH approaches of which some are skeptical.
Effectively marketing CIH programs
Many mentioned the importance of marketing CIH programs to make them visible to patients, physicians, and staff but struggled with the best way to do that. Also, as the CIH and medicine field has been evolving, so has the language to describe it. What was once referred to as Complementary and Alternative Medicine (CAM) is now referred to as Complementary and Integrative Medicine (CIM) or Complementary and Integrative Health (CIH). Each VA medical center used different terminology to refer to CIH programs (e.g., “integrative health and healing,” “CAM,” integrative health,” “integrative medicine,” and “complementary and integrative health”), often within the same facility, which confused facility leadership, physicians, and staff.
Strategies
As noted earlier, some sites held patient and staff open houses for them to learn about and experience CIH approaches for themselves. They also designed patient brochures with CIH class descriptions for departments to post at patient check-in and for providers to hand out. Regarding CIH terminology, some use language used by the National Institutes of Health's (NIH) Center for Integrative Health and the VA OPCC&CT—“CIH” or “complementary and integrative health”—to be uniform and lend legitimacy to those approaches.
Factors That Challenge CIH Practice Implementation
Many VA sites faced challenges when implementing CIH approaches and some used strategies to successfully manage those challenges.
Difficulties in hiring CIH practitioners
At the time of our interviews, VA position descriptions, functional statements, occupational codes, and credentialing guidelines were unavailable for most types of CIH practitioners, so some were unclear about the guidelines about who can provide what type of CIH treatment. In the VA, alternative hiring options are often not readily available. Hiring contracted staff can be a difficult lengthy process; use of volunteers might not provide the consistency required; and, at the time, fee-basis arrangements were usually unavailable for some types of CIH practitioners.
Strategies
Some facilities developed their own credentialing process using a consortium of facility stakeholders (e.g., CIH steering committee). Others hired staff for yoga and t'ai chi with scopes of practice that include movement therapy (e.g., recreational therapists) or hired MDs or chiropractors with acupuncture licenses to deliver acupuncture. Some used existing licensed physicians who were interested in providing CIH approaches and credentialed them.
Difficulties in coding/documenting CIH use
Documentation of CIH approach utilization is the basis for VA billing and tracking use, making it a critical function. However, almost all respondents were either unaware or confused about using the national documentation codes. Additionally, many found entering the codes into medical records too time-consuming to do without administrative support, which most respondents lacked.
Insufficient funding
Almost everyone mentioned difficulties at some point in obtaining funding to initiate and sustain CIH approach delivery. Funding was dynamic and provided by a mix of sources, including line item staff from medical center directors, internal VA funding from OPCC&CT, external research funds that included line-items for CIH practitioners to deliver the research intervention, and external donated supplies (e.g., yoga mats). Funds were also typically insufficient for clerical support and, without that, CIH practitioners had to schedule and follow-up with patients, which is inefficient, given their workload burden.
Appropriate patient access to CIH
Many sites required physician referral to “medical treatment” CIH (e.g., biofeedback, massage, and acupuncture) but allowed patients to sign themselves up for yoga, t'ai chi, and meditation classes. However, most physicians did not know which CIH approaches to refer their patients to because they were unclear which were most effective. Furthermore, many reported that some patients wanted seemingly unlimited access to acupuncture, massage, or chiropractic care, which could overwhelm physician availability and prevent other patients from timely access to services. Also, various CIH approaches are well utilized at most sites and, as veterans spread the word about their satisfaction and program availability, patient demand increases. However, that demand for CIH often exceeds what can be provided (because of CIH practitioner time and space restrictions).
Strategies
To remove the burden of referring providers having to choose particular CIH approaches for their patients, a few sites had physicians refer patients to the CIH program, and then, physician CIH program leads determined which CIH approaches were appropriate for patients. To address unlimited patient demand, in lieu of unestablished clinical guidelines for most CIH approaches, some sites established their own guidelines regarding patient eligibility and dose. For example, at 1 facility, patients are allowed up to 5 acupuncture visits and then are required to return to their physician for an assessment, followed by an additional 5 sessions if the physician thinks it is beneficial, totaling 10 visits annually. Others established a treatment sequence for moving from passive to active CIH approaches, such as moving from chiropractic or acupuncture to resolve patients' pain, then to meditation, t'ai chi or yoga for ongoing pain maintenance and to build core strength for prevention purposes. Some VAs also contracted with community-based providers to provide fee-basis care (a practice that was nascent given the concurrent passing of CHOICE legislation on that issue). Some provide telehealth classes in waiting rooms after hours.
Insufficient CIH practitioners' and support staff's time
As noted above, various CIH approaches were well utilized and, as increasing numbers of patients learned of practice availability and potential effectiveness, their demand for CIH approaches increased. Many CIH practitioners reported being unable to meet that demand, to adequately document their use, or to schedule patients to use them. Many were providing CIH approaches on their own time with leaderships' support. To increase the supply of CIH practitioners, respondents often found it difficult to obtain approval or funding to receive CIH practitioner training. Additionally, many reported a lack of CIH program administrative support, usually resulting in no one to follow-up with patients. Some CIH practitioners were often left to document patients' use of CIH approaches, respond to consults, or schedule CIH approach provision, leaving them less time to deliver CIH.
Strategies
As noted above, some medical centers have become efficient with CIH provision by having patients progress through a structured sequence of different CIH approaches instead of allowing patients to choose any CIH approach (some of which are inappropriate) or unlimited amounts of CIH approaches (especially acupuncture and massage). Also, as noted above, some VAs contracted with community-based providers to provide fee-basis care and many were providing CIH telehealth classes in distant VA community-based clinic waiting rooms after hours when CIH practitioners could not be hired.
Insufficient or inappropriate space
Most reported difficulties in finding any or appropriate space. For example, space was often not conducive to yoga, t'ai chi, or meditation classes—it may be too noisy, small, or claustrophobic for patients with post-traumatic stress disorder (PTSD) or military sexual trauma. As noted above, many were interested in providing teleclasses based on the main medical facility but televised to VA community-based clinics. However, they often had difficulties in obtaining equipment, electronic bandwidth, or technical staff.
Strategies
Some obtained space by participating in long-term building planning efforts. Also, some installed ceiling panels to reduce noise from hallways and other floors.
The health care cultural and geographic environments
Some reported a tension between the cultures of Western biomedicine and holistic or CIH care had somewhat hindered CIH implementation. One CIH program director said that implementing CIH programs involved a cultural change and, as such, we should not expect it to be embraced overnight. However, the medical facility's size or academic affiliation, and city size or rurality appeared unrelated to provider or patient attitudes toward CIH. That is, respondents in three large urban sites reported experiencing the same implementation struggles and successes and patient attitudes as those of smaller or rural sites.
Discussion
Respondents commonly reported that nine key factors facilitated the implementation of CIH approaches at the VA and seven factors hindered that implementation. Most were using a range of creative strategies to foster implementation. Many challenges were national in scope or were consistent across most respondents and were difficult to overcome. Other challenges, however, have been successfully addressed through the passion, perseverance, and creativity of CIH program leads, practitioners, and champions.
From a national policy and operations standpoint, since the time these interviews were conducted—and guided in part by the findings they produced—the VA Central Office has made great strides to address these challenges. To foster the implementation of CIH approaches in the VA, the Integrative Health Coordinating Center (IHCC) was established within the OPCC&CT in 2014. It is charged with developing and implementing CIH strategies in clinical activities, education, and research across the system, with two main functions:(1) to identify and address barriers to providing CIH across the VA system and
(2) to serve as a resource for clinical approaches and education for veterans and VA staff.The OPCC&CT and IHCC have been focusing on the following seven implementation areas, bolstered by additional support from other VA Program Offices.*
Improving CIH practitioner hiring
While many integrative health professions are centuries old, they are still new to U.S. health care. To hire employees or bring on contractors or volunteers within the VA, qualification standards and/or position descriptions must be developed and classified by human resources. As such, IHCC led the development of nationally classified position descriptions for sites to use in hiring yoga and t'ai chi instructors. Additionally, a new qualification standard for Acupuncturist was published in 2018, with similar standards expected for massage therapists in 2019. Also, guidance around provider minimum proficiencies has been developed for: acupuncture, massage, meditation, clinical hypnosis, biofeedback, yoga, and t'ai chi.
Developing and disseminating national codes for CIH use The IHCC has since developed and disseminated several internal VA codes to document the use of CIH approaches.
CIH program funding, space, and supply
The VA has established national ties with organizations such as the YMCA, enabling individual VA medical facilities to develop local partnerships with the YMCA for the use of their space, classes, and instructors for provision of CIH classes. Also, telehealth has been growing rapidly across the VA to improve access to a range of health care services, including CIH approaches. OPCC&CT helped develop guidance and support documents, including operational and clinical standards; a list of resources to be in place to support safe, high-quality tele-CIH approaches; an online resource center for materials; and a directory of programs so that VA staff can connect with one another.
Consistent language to describe CIH programs
OPCC&CT is using “CIH,” to follow the language used by the NIHs National Center for Complementary and Integrative Health.
Improved dissemination of CIH implementation information The IHCC has created an internal IHCC intranet page storing the resources described above and dynamic implementation guidance document. To improve communication and the dissemination of these resources, the OPCC&CT established an internal CIH listserv and website collaboration space and holds various monthly VA webinars and teleconferences to provide updates and guidance to sites nationally. The IHCC staff often join facility, network, and national meetings to further disseminate CIH-related guidance and to assist with national CIH policy and program questions. Also, OPCC&CT Field Implementation Team Consultants are now located across the country to serve as a field resource for CIH implementation.
CIH champions and leadership support
As part of the Whole Health System transformation, and in coordination with the Opioid Safety Initiative, a CIH point of contact was identified in each of the VAs 18 medical networks to participate on network Pain Committees and to serve as a CIH champions for that network. OPCC&CT also has identified various Clinical Champions to provide support to the field around whole health and CIH implementation. Additionally, the VA has added whole health performance measures to the VA Network Director's performance plans to add to the momentum for leadership support for these initiatives.
Increased funding or funding guidance
While funding for CIH implementation at all VA facilities is not yet in place, individual VA facilities or regional VA networks have provided some funding and OPCC&CT has offered small grants. The IHCC has developed guidance on how much funding sites might need for various CIH and other whole health programs, based on best approaches and projected return on investment. Additionally, as mentioned earlier, 18 facilities were funded in 2018 for full-scale deployment of the whole health system, which includes integration of CIH. [24] Perhaps most importantly, as of 2018, the VA Allocation Resource Center is actively engaged in a new effort to provide specific budget dollars through the VA budget system to support provision of Whole Health and CIH approaches. This will ultimately ensure financial sustainability for facilities' efforts to provide CIH approaches.
In addition to these significant VA implementation strategies, CIH implementation is also fostered by substantial national and congressional support around whole health and CIH, including but not limited to the CARA Act of 201625 mentioned earlier.
Limitations
There are several limitations to our project. First, we spoke to stakeholders at only eight medical facilities, and we selected these facilities based on sites responding to national e-mail invitation and, among those, sites with at least three CIH approaches, with the assumption that they might have richer implementation stories to tell us. It could be that other sites with fewer CIH approaches faced additional implementation issues that we have missed in our sample. However, we spoke to a wide range of stakeholders, attempting to capture the potential broad range of perspectives on implementation issues being faced. Also, some implementation issues that VA sites face might not be generalizable to other health care systems. For example, hiring might be easier at other health care systems than it is in the VA. Additionally, examining implementation issues for CIH approaches as a whole can be misleading, in that it is unlikely that all approaches face the same issues. Yoga, for example, can be perceived as exercise by some, whereas meditation can be perceived as mystical by others, and “mystical” interventions might face additional health care implementation challenges. Finally, we were unable to obtain patient perspectives due to the timeline constraints, although patients are a key component to the successful implementation of any hospital-based intervention.
Conclusions
VA medical facilities have been somewhat successful in implementing CIH programs, despite the numerous challenges they face. Some of those challenges are typical for interventions being implemented into health care systems, whereas others seem particular to CIH approaches. However, regardless of their size, geographic location, and the amount of funding they received, all medical centers had some success with implementing CIH approaches and all were struggling to overcome challenges. In response to those challenges, VA medical facilities and the IHCC have creatively developed a wide range of strategies to support CIH implementations. Many are reproducible by other health care systems or providers wanting to initiate or strengthen their CIH programs.
Due to these activities, CIH approaches are continuing their rapid expansion in the VA. Preliminary results from our recent national survey show that VA medical centers provide an average of 6 CIH approaches, with a quarter offering over 10. [27] Currently, the most frequently offered are: yoga, mindfulness-based stress reduction, meditation, guided imagery, acupuncture, t'ai chi, and relaxation responses. With this, the VA is moving closer to transforming from a medical/disease-based system of care to a health care system addressing the whole patient.
Acknowledgments
We are grateful to the numerous people who gave their time and thoughts during our interviews. This work was supported by the Department of Veterans Affairs Quality Enhancement Research Initiative program (PEC 13-001, Evaluating VA Patient Centered Care: Patient, Provider, and Organizational Views). The views expressed in this article are those of the authors and do not necessarily represent the position or policy of the Department of Veterans Affairs or the U.S. government. All VA authors of this article attest that the activities that resulted in producing this article were not conducted as part of a research project, but as part of the nonresearch evaluation conducted under the authority of name of the VA Office of Patient Centered Care and Cultural Transformation. The status of this work as quality improvement and not research was also confirmed following review by the Research and Development Committee at the VA Greater Los Angeles Healthcare System.
Author Disclosure Statement
No competing financial interests exist.
References:
Ananth S. 2010
Complementary and Alternative Medicine Survey of Hospitals.
Alexandria, VA: Samueli Institute.Ezeji-Okoye SC, Kotar TM, Smeeding SJ, et al.
State of care: Complementary and alternative medicine in patients health administration—
2011 survey results.
Fed Pract 2013; 30:14–19.Stahl JE, Dossett ML, LaJoie AS, et al.
Relaxation response and resiliency training and its effect on healthcare resource utilization.
PLoS One 2015;10:e0140212.Gellad WF, Good CB, Shulkin DJ.
Addressing the opioid epidemic in the United States. Lessons from the Department of Patients Affairs.
JAMA Intern Med 2017;177:611–612.Nahin RL, Boineau R, Khalsa PS, et al.
Evidence-based evaluation of complementary health approaches for pain management
in the United States.
Mayo Clin Proc 2016;91: 1292–1306.Polusny MA, Erbes CR, Thuras P, et al.
Mindfulnessbased stress reduction for posttraumatic stress disorder among veterans: A randomized trial.
JAMA 2015;314: 456–465.Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an
American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 493–505Morone NE, Greco CM, Moore CG, et al.
A mind-body program for older adults with chronic low back pain:
A randomized clinical trial.
JAMA Intern Med 2016;176: 329–337.Hempel S, Taylor SL, Solloway M, et al.
Evidence Map of Acupuncture
Washington, DC: Department of Patients Affairs, 2014.Goode AP, Coeytaux RR, McDuffie J, et al.
An evidence map of yoga for low back pain.
Complement Ther Med 2016;25:170–177.Solloway M, Taylor SL, Miake-Lye IM, et al.
An evidence map of the effect of Tai Chi on health outcomes.
Syst Rev 2016;5:126.Hempel, S., Taylor, S. L., Marshall, N. J., Miake-Lye, I. M., Beroes, J. M.
Evidence Map of Mindfulness
Washington (DC): Department of Veterans Affairs (US); 2014 Oct.Hilton L, Hempel S, Ewing BA, et al.
Mindfulness meditation for chronic pain: Systematic review and metaanalysis.
Ann Behav Med 2017;51:199–213.Paige NM, Myiake-Lye IM, Booth MS, et al.
Association of Spinal Manipulative Therapy with Clinical Benefit and Harm
for Acute Low Back Pain: Systematic Review and Meta-analysis
JAMA. 2017 (Apr 11); 317 (14): 1451–1460Miake-Lye IM, Lee JF, Luger T, et al.
Massage for pain: An evidence map.
VA ESP Project No. 05-226, 2016 Online document at:
www.hsrd.research.va.gov/publications/esp/massage.cfm
accessed November 1, 2018.Institute of Medicine.
Complementary and Alternative Medicine in the United States
Committee on the Use of Complementary and Alternative Medicine by the American Public,
Board on Health Promotion and Disease Prevention.
Washington, DC: National Academies Press, 2005.Barnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Cassileth BR, Lusk EJ, Strouse TB, et al.
Contemporary, unorthodox treatment in cancer medicine:
A study of patients, treatments and practitioners.
Ann Intern Med 1984; 101:105–112.Cherkin DC, Herman PM.
Cognitive and mind-body therapies for chronic low back pain and neck pain: Effectiveness and value.
JAMA Intern Med 2018;178:556–557.Qaseem A, Wilt TJ, McLean RM, Forciea MA;
Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain:
A Clinical Practice Guideline From the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Office of the Assistant Secretary for Health.
National Pain Strategy: A Comprehensive Population
Health-Level Strategy for Pain
Washington, DC: US Department of Health and Human Services,
National Institutes of Health; 2016.Dowell D, Haegerich TM, Chou R.
CDC Guideline for Prescribing Opioids for Chronic Pain: United States, 2016
Morbidity and Mortality Weekly Report
Recommendations and Reports Vol. 65 No. 1 March 18, 2016Cottreau M, Kotar T, Schelach K, et al.
FY 2015 VHA Complementary and Integrative Health (CIH) Services
Washington, DC: Healthcare Analysis and Information Group (HAIG);
Department of Veterans Affairs, 2015.VA’s Whole Health System.
Expanding the VA Whole Health System
Comprehensive Addiction and Recovery Act (CARA) of 2016. TITLE IX—DEPARTMENT OF PATIENTS AFFAIRS.
Subtitle C—Complementary and Integrative Health. Section 931. Expansion of research and education
on and delivery of complementary and integrative health to patients. Section 932.
Expansion of research and education on and delivery of complementary and integrative health
to patients. Section 933. Pilot program
on integration of complementary and integrative health and related issues for patients and family members of patients.Greenhalgh T, Robert G, Macfarlane F, et al.
Diffusion of innovations in service organizations: Systematic review and recommendations.
Milbank Q 2004;82:581–629.Taylor SL, Hoggatt K, Kligler B.
The National Survey of Veterans Use of and Interest in Complementary
and Integrative Health Approaches. (May 2018).
Oral presentation at International Congress on Integrative Medicine and Health,
Baltimore, MD. Audioversion available at:
https://www.hsrd.research.va.gov/for_researchers/cyber_seminars/ archives/video_archive.cfm?SessionID=3547
Return NON-PHARMACOLOGIC THERAPY
Return to CHIROPRACTIC CARE FOR VETERANS
Since 6-09-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |