

When Boundaries Blur - Exploring Healthcare Providers'
Views of Chiropractic Interprofessional Care
and the Canadian Forces Health ServiceThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2021 (Apr); 65 (1): 14–31 ~ FULL TEXT
OPEN ACCESS Ellen Vogel, PhD, Silvano A Mior, DC, PhD, Deborah Sutton, MEd, MSc, Pierre Côté, DC, PhD, Simon French, BAppSc(Chiro), MPH, PhD, Margareta Nordin, Dr. Med. Sci, PT, Audrey Laporte, PhD
Faculty of Health Sciences,
Ontario Tech University.

Introduction: Musculoskeletal (MSK) conditions are primary reasons prohibiting Canadian Armed Forces (CAF) personnel from being deployed, with back pain the second most common activity-limiting condition. CAF provides a spectrum of services, including chiropractic care. There is a paucity of data related to chiropractic interprofessional care (IPC) within CAF healthcare settings.
Methods: A qualitative study, using an Interpretative Phenomenological Analysis (IPA) approach, involving 25 key informant interviews explored factors that impact chiropractic IPC. We used a systematic but not prescriptive process, based on a thematic analysis, to interconnect data to develop meaning and explanation. Initially, we explained and interpreted participant's experiences and meanings. Next, we used extant literature and theory, together with expert knowledge, to explain and interpret the meanings of participants' shared accounts.
Results: We present findings central to the domain, Role Clarity, as described in the IPC Competency Framework. Our findings call for strengthening IPC specific to MSK conditions in the CAF, including an examination of gatekeeping roles, responsibilities and outcomes.
Conclusion: It is timely to investigate models of care that nurture and sustain inter-provider relationships in planning and coordinating evidence-based chiropractic care for MSK conditions, within the CAF, and its extended referral networks.
Keywords: Chiropractic; Health Services; Interpretative Phenomenological Analysis; Interprofessional Collaboration; Military Medicine; Military Personnel; Role Clarity.
From the FULL TEXT Article:
Introduction
Musculoskeletal (MSK) conditions have a significant impact on the health and operational readiness of Canadian Armed Forces (CAF) personnel. [1] MSK conditions are primary reasons prohibiting CAF personnel from being deployed and back pain is the second most common activity-limiting condition. [2, 3] Moreover, in the 2014 Surgeon General’s Report, MSK injuries were identified as responsible for 42% of all medical releases. [4] The CAF recognizes that evidence-based and cost-effective management of MSK conditions is an important issue for members and the CAF as a whole. [5]
The Canadian Forces Health Services (CFHS) provides a spectrum of healthcare services in managing members’ health needs, including healthcare provided in civilian off-base facilities when services are not available on-base. [5] In Canada, chiropractic care is an eligible CAF health practitioner benefit when prescribed by a physician, and accessed off-base, outside the military healthcare system. Chiropractic care is authorized with a 10-visit limit per condition, after which a physician’s review is required to determine if further treatment is necessary. [6] Within the CFHS, strengthening the integration and coordination of care in primary care settings is an envisaged priority, with significant investments currently made in some areas, including mental health. [5]
However, the inclusion of multiple services in an integrated healthcare delivery model is a complex process requiring in-depth knowledge of professionals’ distinct roles, responsibilities, skills, scopes of practice, and understandings of their practice settings. [7] Exploring how these components interact in an interprofessional collaborative manner (i.e., triaging and referring patients, appropriateness of care, and ensuring continuity of care), requires attention. Chiropractors are increasingly participating as active members of interdisciplinary teams, in both primary care and hospital-based settings. [8–10] Currently, there is a paucity of data about interprofessional collaboration (IPC) within the CFHS’s unique healthcare environment and its community-based referral networks, related to diagnosing and treating MSK conditions.
Purpose and aim
Our national study used an Interpretative Phenomenological Analysis (IPA) approach to describe and interpret how integrated chiropractic services could be designed, implemented and evaluated within the CFHS. In this manuscript we expand on our previous work that explored key informants’ perceptions of opportunities and barriers, in a variety of complex and diverse domains, related to introducing interprofessional collaborative chiropractic services in the CFHS. [11]

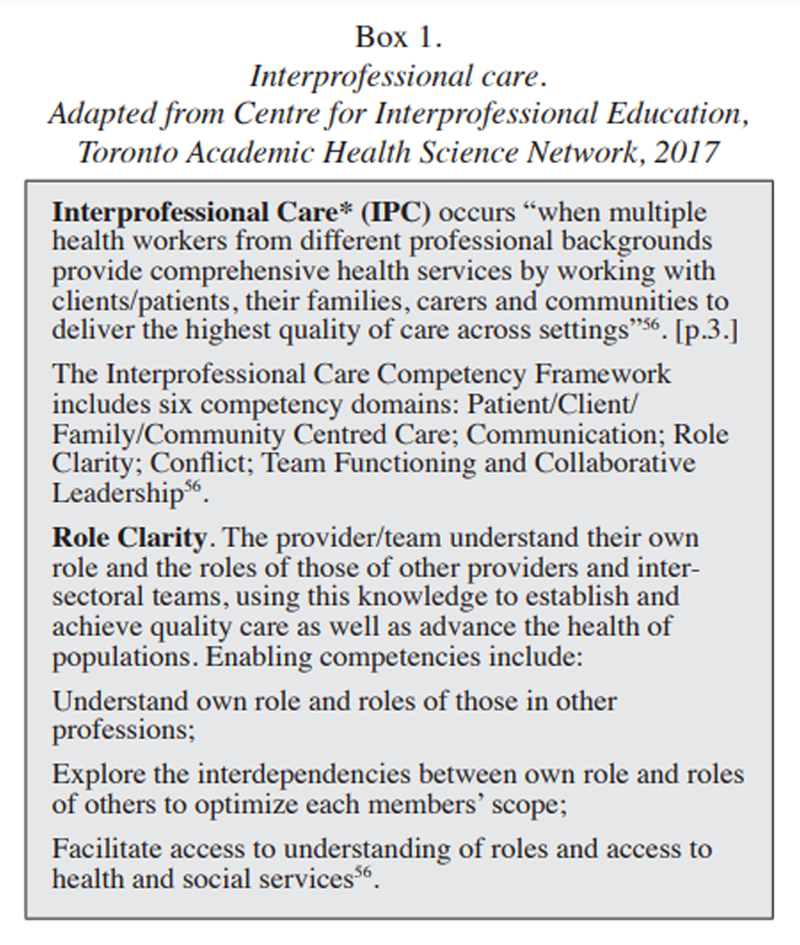
BOX 1 Our aim in this manuscript is to focus on one aspect of the study (i.e., IPC in the CFHS), explicit to MSK conditions. Specifically, we examined emergent themes to elucidate the factors that foster or hinder chiropractic IPC within the CFHS. While recognizing that all six IPC competency domains are important, we described and interpreted findings related to the domain Role Clarity (see Box 1). Our rationale was two-fold: brevity requirements, together with robust, previously unreported data, in the form of rich, situated, and detailed narratives that expand on our earlier analysis and discussion. We hope that our findings resonate with readers on the basis of their experiences and that ongoing reflection leads to deeper and original insights. [12]
Methods
We employed an IPA approach whereby we explained and interpreted key informants’ perspectives on how an interprofessional collaborative chiropractic service could be designed, implemented and evaluated wthin the interdisciplinary CFHS. IPA is an approach to qualitative research concerned with exploring and understanding the lived experiences of a specified phenomemon. [13, 14]
One of the hallmarks of an IPA approach is that data analysis progresses from making sense of the participant’s experience, to a focus on the shared experience of participants, and from the descriptive to the interpretative. [15] When applying findings, readers critically reflect to see whether published findings resonate with their experiences, perhaps nudging a re-evaluation of what was considered known or understood about the phenomena being explored. [16] The onus is on IPA researchers to discuss findings through the lens of the extant literature and theory and to debate the congruence and dissonance between the findings of the study and the prevailing discourse or evidence. [13]
Approvals
Ethical approval was received from the Research Ethics Boards at the University of Ontario Institute of Technology (Ontario Tech University) (# 15-049) in Oshawa, and the Canadian Memorial Chiropractic College (CMCC) (#152019) based in Toronto. Agreement to conduct the study was provided by the Canadian Deputy Surgeon General, CFHS (7 June 2016). All participants were provided with an overview of the purpose of the study prior to providing informed consent. A regional Commander of the CFHS introduced the study and provided background information through an e-mail communication emphasizing that participation was voluntary.
Recruitment
We used purposeful sampling [17] to recruit key informants. Inclusion criteria included: English-speaking health care professionals, military personnel, and researchers with experience and in-depth understandings of healthcare delivery and interprofessional collaborative practice within the military setting in Canada. Additional key informants with knowledge and/or experience related to the delivery of health care within the CFHS, with emphasis on MSK conditions, were identified using a snowball sampling technique. [17] Of the individuals approached only one person declined to participate in the study, referring researchers to individuals seen as more highly qualified to address the key research questions.
Interview schedule and procedures
Semi-structured telephone interviews were conducted employing an interview guide with open-ended questions. [7, 18–20] The interview guide was informed by expert opinion, as well as health, social [21, 22] and behavioral [23] theories addressing facilitators and barriers to accessing chiropractic care. [21–23] After the first eight interviews, additional probes were developed and questions slightly revised (See Appendix A). Interviewing continued until the research team ascertained that saturation of responses to key questions was achieved. [24–26] As data saturation is not generally a goal of the IPA approach [27], researchers focused on obtaining robust and rich personal accounts from participants, in order to describe and interpret the experiences, concepts and commonalities across the group.
All interviews were conducted by two members of the research team, both healthcare professionals, who were not physicians, chiropractors nor physiotherapists, thereby mitigating potential researcher bias. [20] The lead interviewer, an experienced qualitative researcher, was assisted by a team member who served as a note-taker and timekeeper while providing logistical support in setting-up and audio-recording; neither had prior knowledge of study participants. The interviews were conducted between September 2016 and February 2017 and were 45-to 60-minutes in duration. Interviews were audio-recorded, exported to an encrypted USB key and transcribed verbatim by an experienced transcriptionist. All transcripts were reviewed for accuracy against the recorded sessions. Content errors were corrected and any potential identifying information removed prior to coding.
Participants were invited to review the transcript (member checking) and make any necessary additions or deletions. Member checking involves taking data (e.g., verbatim transcripts) back to participants so that they can judge the accuracy of the account and is “the most critical technique for establishing credibility” [28] (p.314). In qualitative research, member checking or seeking participant feedback remains an important validation strategy. [12] Twelve of 25 key informant interviews completed member-checking. Five key informants accepted the transcript with no changes, while seven made minor changes. In situations where key informants declined to be audio-recorded (n=3), both interviewers kept field notes and post-interview memos to the self; this information was subsequently included in data analysis. [29] Researchers did not conduct repeat interviews with any of the participants.
Data analysis
Several approaches to analyzing phenomenological data are described in the literature. Smith and colleagues (2009) proposed a distinct, systematic and flexible structure, based on thematic analysis, and consisting of several phases, for analyzing IPA data. Data analysis necessitates that researchers be open and willing to “dwell in the data,” consistent with the IPA approach taken to data collection.
In our study, dual interpretation occurred during data analysis whereby the participant made sense of a phenomenon by explaining and interpreting their own experience and the researchers used extant literature and theory, together with expert knowledge and experiences to explain and interpret the meaning of participants’ shared accounts. [14, 15] Described as the “double hermeneutic,” Smith et al. (2009) underscored the circularity of the process (questioning, uncovering meaning and further questioning) involved in interpreting and understanding a phenomena. [15]
In IPA research, the final account offers a layered analysis of the phenomena, where the first descriptive phenomenological layer conveys a thoughtful understanding of participant’s experience. In the second layer, a probing critical analysis is conducted based on deeper interpretative work. [30] The findings should be plausible, indicative and provisional given that researchers, despite their best efforts, cannot fully abstract themselves from the contextual basis of their own experience. [30] In our earlier work11, data analysis proceeded in an iterative and inductive manner in which thematic analysis of early interviews informed later data collection. After the first three interviews were completed and transcribed, each verbatim transcript was independently read and re-read by three research team members (i.e., the two individuals who facilitated or participated in all interviews and a third team member with extensive experience in qualitative approaches and topics central to the study.)
Initial notes and observations were made in the margin of the texts, and key descriptive comments and phrases were highlighted. Additionally, researchers began to make more interpretative comments, in some cases questioning what the comments revealed about the participant’s understanding of the phenomenon.
Next, the three researchers met regularly to begin the process of developing emergent themes, partly informed by their initial margin notes and observations. Discussion focused on reviewing and reaching consensus on coding, examining and defining codes, and developing a referent codebook. The coding structure and the related transcript reference data were entered into qualitative data analysis software (NVivo Pro Version 11.4.1 for Windows, QSR International (Americas) Inc., Burlington, MA, USA). This final step was helpful in illuminating the connections between themes and sub-themes, and served to highlight differences and similarities, leading in some cases to renaming themes as researchers acquired a deeper understanding of the data. [15]
As data analysis progressed, and building on our earlier work, we further examined participants’ experiences to explore and interpret findings relevant to Role Clarity of the IPC framework. Specifically, we organized and interpreted themes into major and minor components, supported by an intensive line-by-line analysis of the texts. Again, researchers’ formative thoughts and reflections were noted, with ideas and developing interpretations brought forward and debated. Theoretical sensitivity was strengthened by repeatedly comparing and verifying themes to the actual texts. [31] We used our knowledge of the available literature and theory, including the IPC framework, to interpret salient themes further. Although researchers attempted to bracket themselves out of the study by acknowledging values and biases on a regular basis, in interpretative (hermeneutic) phenomenology, it is widely accepted that researchers’ values affect the object of study. [32, 33]
The Interprofessional Care Competency Framework (Box 1) offered a theoretical lens for researchers to manage, organize and ultimately interpret findings, specific to Role Clarity. With Role Clarity emerging as a central phenomenon underpinning recent work, we used an IPA approach to return to our database, reviewing the published literature and theoretical frameworks, to explore and interpret facilitators and barriers to Role Clarity, as well as specific contextual and intervening conditions. This approach, consistent with the dual interpretation described earlier in the manuscript, also reflected the circularity of the process vis-ŕ-vis interpreting and understanding a phenomenon. [15]
Results
Participants
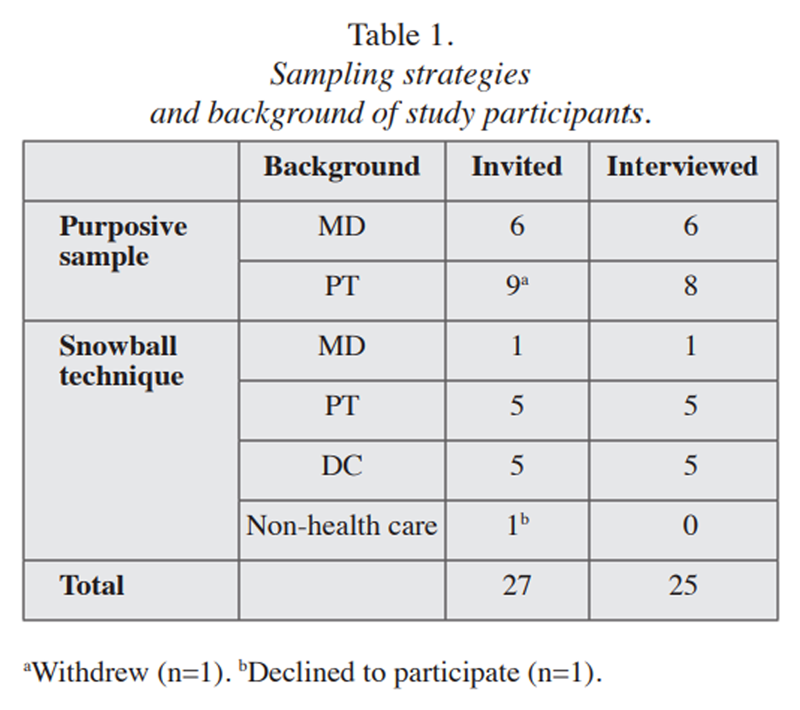
Table 1 Table 1 provides information on study participants’ professional backgrounds. They included military personnel (52%), public servants and contractors employed by the CAF (24%), and civilians (24%), distributed across Canada. Military participants included ranks of Chief Warrant Officer, Lieutenant, Captain, Lieutenant Colonel, and Colonel. Slightly more than half of the CAF key informants were deployed at least once over the course of their career. Participants self-identified as medical doctors (MD), physiotherapists (PT), and chiropractors (DC). The chiropractors, all situated off-base, provided care to CAF members. Of the study participants, the majority were male (n = 76%).
Our findings focussed upon the competency domain of Role Clarity. We organized our findings under a series of sub-headings based on the Interprofessional Care Competency Framework And Team Assessment Toolkit (See Box 1) and supported them using salient verbatim quotes. nbsp; Knowledge gaps related to role clarity
We found little evidence to suggest that within the CFHS, healthcare professionals involved with managing MSK conditions, were interested, or motivated, to explore the interdependencies between their own roles and the roles of others, in an effort to optimize each members’ scope. Some CFHS physiotherapists discussed their role limitations and the need for consultation with other members of the healthcare team. This was based on their perceptions of knowledge, skills, roles, scopes, and sometimes on lengthy wait-lists for physiotherapy services on-base. Although the referral processes for MSK conditions varied from base-to-base, they were largely contained within their intra-professional networks (i.e., physiotherapist to physiotherapist).
A chiropractor working in an off-base multidisciplinary clinic, offered the following perspective on the lack of role clarity specific to the treatment of spinal pain:Essentially in our healthcare system if you have a heart condition you go to a cardiologist, if you have cancer you go to an oncologist, but if you have back pain who do you go to? You can go to a chiro, a physio, a massage therapist, an osteopath. You can go to any of those people and with any of those people you have no idea what kind of care you are getting because within each of those professions there is a huge spectrum of peoples expertise in dealing with spinal pain. And all kinds of philosophical approaches... From a consumers point of view, there is no portal of entry into the healthcare system for someone with spinal pain. It is a wide-open door and you can go anywhere you want and get any kind of care that anyone wants to give you. (DC, K20)
Blurring of boundaries
We found strong evidence on the blurring of boundaries relative to the roles that physiotherapists and chiropractors play in the treatment of MSK conditions within the CFHS. This emerged as a key factor hindering role clarity as explicated by a chiropractor below:The line between what a physio does and what a chiro does at this point is so grey, it is difficult to decide, ‘Well, should somebody see a chiropractor or a physiotherapist?’ Because physiotherapists provide manipulation, they are licensed to diagnose. The only difference in their (physiotherapists’) scope of practice is that they don’t have the ability to order and interpret x-rays. Outside of that, their scope of practice is very similar. (DC, K20)
A CFHS physician addressed the lack of role clarity, concurring with the majority of key informants on the perceived “overlap” between MSK service providers. In part, the problem was attributed to a lack of knowledge pertaining to unique professional roles: “The problem is, and we are never taught as to when would a chiropractor be more beneficial than a physio, or vice versa, or if they are both the same.” Elaborating further, the physician stated:When I was seeing patients in a Care Delivery Unit setting, I would have patients who either didn’t respond to physiotherapy, who I would refer to a chiropractor, or vice versa, in fact... So, I think it is just part of the treatment options as such. (MD, KI4)
A CFHS physiotherapist shared perspectives on changing scopes of practice for physiotherapists and chiropractors, including the confusion among patients and healthcare providers with respect to the unique role each provider can play. In the quote, the key informant explains the confusion, through the professional lens of a military physiotherapist, who has been deployed. The reference to decreasing numbers of referrals to off-base chiropractors supports the perspectives expressed by other non-military key informants who were located off-base:...So the difference that we used to see between the two professions is now a lot more blurred and there is a lot more shades of grey... So, if someone comes in, where before twenty years ago and said, ‘I want to see a chiropractor’, essentially what they were asking for is manipulation. Now, if they come-in and say, ‘I want to see a chiropractor’, it’s not necessarily what they are asking for. Their friend could be seeing a really good therapist that is treating them not with manipulation, but more of myofascial techniques, exercise therapy, which would be the exact same sort of treatment that they would end up receiving from a physiotherapist onbase... We see our outsourcing, not just for chiropractic, but for manipulation of any kind, to be very low in the (XXX) region because we actually have those expertise right on-base. (PT, K25)
In discussing the blurring of boundaries between physiotherapists and chiropractors, an off-base chiropractor introduced the notion of the “primary spine practitioner,” suggesting that both professional groups, on the basis of their current scopes of practice, could fulfill the role. In the second quote, the chiropractor clarifies that at this point in time the notion of a primary spine practitioner has not been fully explored by key stakeholders, including healthcare professionals and provides a brief description of the role:So physiotherapists are capable within their scope of practice of taking on the role of primary spine practitioner, as are chiropractors. The difference I see is that chiropractors are more focused in training and in their expertise, and in their experience, in everything really, to take on that role straight out of school... So, again, both are licensed to diagnose, but chiropractors, straight out of school, can perform manipulation. So, there is a lot of understanding and there is a lot of knowledge that I think chiropractors have straight out-of-school that physios don’t necessarily have... They can go in that direction and they can build that scope of practice but it is not as much as let’s call it the ‘academic culture of physiotherapy’ as it is in chiropractic. (DC, K20)
That primary spine practitioner is somebody who should be able to provide that conservative care for general musculoskeletal disorders and spinal disorders, but also know how to screen for red flags, refer when appropriate, identify yellow flags, and be able to refer to appropriate imaging in order to further their diagnosis. That entity does not exist in our healthcare system right now.” (DC, K20)
Reflecting on deployment as a barrier to the integration of non-uniformed healthcare professionals in the CFHS, a physician emphasized the need to clarify perceptions of “redundancy,” referring to the overlapping roles of physiotherapists and chiropractors. The physician’s comments also address resource limitations associated with offering post-graduate training and skill development opportunities to physiotherapists employed by the CAF:Let’s just be clear on what it is that they (chiropractors) are going to be doing because otherwise there is that perception of redundancy. The physios are telling me, ‘Well, why not just train more physios in manual therapy,’ because those are expensive courses and because we expect our physios to be deployable and go to wherever the country asks them to go, which wouldn’t be the case for chiropractors. (MD, K11)
Knowledge gaps re: unique contributions of each profession
Findings with respect to participants’ knowledge of the unique contributions of both physiotherapists and chiropractors were mixed. For example, a CFHS physiotherapist replied to a question asking under what conditions would referral to a chiropractor be appropriate:I would say no (conditions for referral). I would say there is specific need for evidence-based management of musculoskeletal conditions. That is what I demand of the on-base physios and all outsourced providers. Because that is what the Surgeon General expects... There is nothing that chiro offers that is both unique and evidence-based, so for me it is about getting access to evidence-based care for MSK issues. (PT, K6)
We have developed very good partnerships with some chiropractors in the area and I think they are phenomenal therapists. But I hesitate to say that the care that they provide differs greatly from (care delivered) by the very experienced physios that we also outsource to... (PT, K25)
Despite opinions posited by participants, there is evidence of favorable outcomes of chiropractic care of active duty military. In particular two randomized controlled trials comparing standard medical care (usual care, medications, physical therapy, pain clinic) and standard medical care with the addition of chiropractic care, favoured the latter for each primary outcome in the short term for patients with low back pain. [6]
In other situations, participants clearly identified the unique strengths and particular expertise of other healthcare professionals involved in the management of MSK conditions, recognizing their own role and its limitations. A chiropractor stated:So, what I end up referring to physiotherapists for is for the treatment of conditions that are within their area of expertise and outside of my area of expertise. We have a physiotherapist who does a lot of pre- and postnatal care, pelvic floor rehabilitation, and things like that. That is completely outside my expertise... Same thing for concussion, which is not my expertise. (DC, K20)
A CFHS physiotherapist contemplated the conditions under which referral to an off-base healthcare professional would be recommended, emphasizing the importance of trust, respect and a successful track-record in treating CAF members for MSK conditions.It is kind of a development of trust in the community with certain clinicians, where you know the paperwork has been done well, the patient has been well looked after... So, it is all about track-record, personal and/or professional interactions... If I wanted to see a chiro, who would I want to go and see? Well, I want to see someone with really good credentials, and a really good track-record, and where we have had that in the past (PT, K16)
Reflecting on the confusion regarding professional roles and scopes, a chiropractor cautioned that while interprofessional collaboration and communication is important, having “too many cooks stirring the pot” can be detrimental to patient care. For example:...If someone (a patient) is seeing too many healthcare practitioners, you tend to get protracted or an over abundance of care. Patients get confused with information: the conditions are medicalized... So, there are two sides to care and that is giving the patient clear messaging and not over-treating them and not over-medicalizing their condition and not subjecting them to too much passive care, but at the same time ensuring that what you are offering them is optimal care. (DC, K20)
A CFHS physiotherapist stated that perceptions of role confusion between physiotherapists and chiropractors were important to address, partly to contain healthcare costs: “Chiropractors cost way more; their salary is way higher than a physio. You could get two physios for one chiropractor (laughs).” In the following quote, the physiotherapist emphasized patient confusion issues, Policymakers need to look at the bigger picture and use the resources that we have to collaborate better with the people that are already in the CFHS... My biggest fear of bringing a chiropractor into the military service is replication of service when other needs are clearly a priority... (PT, K18)
Describing personal experiences working with chiropractors, the physiotherapist’ comments mirror the notion expressed above by a chiropractor that, in some situations, interprofessional MSK care can be detrimental when patients are caught in the middle:There wasn’t a heck a lot of difference in what the chiro was doing and what the physiotherapist was doing, and in some cases, the patient kind of kept going in a little bit of a circle between the two professions. (PT, K18)
Optimizing scopes of practices as a necessary next step
Our findings on role clarity suggest that the majority of CFHS key informants (physiotherapists, physicians, policymakers) viewed chiropractors more as a therapy (i.e., manipulation), rather than as a profession working within a full scope of practice. This perspective can potentially limit access to chiropractic care.
The following quotes, from a mix of participants (physiotherapist, physician, chiropractor), supported the notion of chiropractors being viewed as an intervention rather than as a profession offering a full scope of service:So the most specific criteria to determine if someone is a good candidate for chiropractic care is your ability to determine if there is some form of joint restriction that needs manipulation. (PT, K9)
I think every chiropractor is slightly different, their manipulation technique... So, some will use an instrument to manipulate joints, some will use manual [approaches], there are many different techniques. Some of them, the osteopaths, use muscle energy, as far as I understand, to manipulate joints into the right position. You would have to ask the physios; some physios have been trained... to perform some type of manipulation techniques which are oddly very similar to what a chiropractor offers, as well. (MD, K14)
I have heard physiotherapists say, ‘Well, we can do everything that a chiropractor can do.’ And that is becoming more of an issue now, especially with these manual therapy training sessions where physiotherapists are learning how to manipulate joints. It is for that reason that I specialized in doing a lot of the flexion decompression, because that is strictly a chiropractic technique. (DC, K15).
With this convergence of the professions, whether they go to one or the other it ends up almost being the same... If someone needs manipulation, they can get manipulation from a physio or a chiropractor; if they need acupuncture they can get acupuncture from a physio or a chiropractor. They need active release therapy... that can be done by a physio or chiropractor. So, really there is no one modality of treatment..., that you would say, ‘OK, well, a physio just does this and a chiro just does that.’ If you said to me, ‘We can give you an extra chiropractor, or you can give me an extra physio,’ I would say, ‘OK, well, essentially, in the end, it ends up being the same. (PT, K25).
In contrast, a minority of CFHS key informants, reflecting on their professional and personal experiences (i.e., seeking chiropractic treatment for themselves or family members) with patients with MSK conditions, emphasized the unique assessment and therapeutic skills of chiropractors. Such thoughts have been highlighted in other reports suggesting how health policies define complementary and alternative professions (including chiropractic) as individual therapies, rather than as a profession with a wider scope of practice. [34]
Findings suggested that within the CFHS it was not uncommon for key stakeholders to equate chiropractic care with spine care. There was consistency amongst most participants that access to services within the spectrum of care is for a specific intervention, rather than for the profession’s full scope of practice. In other words, consideration for referral for chiropractic services was made primarily for spinal manipulation to treat a particular spinal disorder, most commonly chronic low back pain. A CFHS physician stated:...We’re not making a good usage of chiropractic practitioners in our organization... I’m looking more at quality than quantity. I don’t think we need to do more but I think we can do better in referring the right individuals at the right time instead of doing what we do now which is paying a lot of money for chronic low back pain with very little results. (MD, KI)
However, a minority of participants, particularly physicians who had established both personal and professional relationships with chiropractors, considered also accessing chiropractors for their expert clinical opinion.‘Who ultimately is the spine care specialist?’ because we lump all kinds of people in that domain. I think given the nature of the speciality, and how much time chiropractors spend on the spine, I would have to agree that... chiropractors, ...come closest to a spine care specialist. (MD, K11)
Exploring how chiropractors can be involved, the majority of participants called for an integrated team, consistent with a patient-centred spine care model. In this model, providers are respected and distinguished for their uniqueness, with care provided together with others, rather than in isolation. In this scenario, providers do not become the intervention. Rather, collaboration is developed through relationships built on trust, respect and shared decision-making, taking advantage of differing complementary skills in multiple settings across the continuum of care. According to experts in collaboration:“...It involves sharing knowledge, perspectives and responsibilities, and a willingness to learn together. This requires understanding the roles of others, pursuing common goals and outcomes, and managing differences.”
(CANMEDS 2015, p. 7) [35]
Facilitating access to health services
Chiropractic services within active duty military healthcare settings is typically accessed through a gatekeeper. [6] Our findings suggested the gatekeeper role with respect to off-base referrals was a major barrier to the access of chiropractic services with the CFHS.
Typically, the gatekeeper was identified as a lead physiotherapist and/or the Base Surgeon. Frequently, the decision to refer was predicated on the clinician’s individual preferences and experiences, rather than a systematic approach.
Consistent with the work of others [36, 37], our findings suggest that the diversity within the chiropractic profession limits referrals and creates significant barriers to IPC. Below, we provide additional perspectives on the gatekeeper role in the CFHS, with the goal of elucidating turf issues, professional biases and, possibly role discrimination.The current way that it works... is that a Medical Officer can make the recommendation to the physiotherapy department, but it is ultimately the physiotherapy department that makes the ‘yes’ or ‘no’ call. [regarding the need for referrals off-base]
(PT, K15)
A CFHS physician described the delivery of healthcare services on-base as interprofessional, emphasizing “That is the outset; that is the theory.” He explained further:In practice, as with all things whether it is medicine or any other profession, whether people talk to each other is more a matter of personality and previous life experience then it has to do with either the profession or organization they work in.
Although we can tell people how they should practice, ultimately we are not micromanaging... So, in a perfect world they would all be exchanging, collaborating and talking to each other, but knowing from experience, this is not always the case. This is the first caveat... theory and practice are two very distinct entities. (MD, K11)
A CFHS physiotherapist reflected on past and present military postings, concluding: “We haven’t really seen a significant need for chiropractic referral to an external healthcare provider.”
A second physiotherapist elaborated further, stating: “We [physios] are able to provide every skill set and every possible intervention that a CAF member may require as part of their treatment plan...”
A third physiotherapist considered a hypothetical situation, described as an “odd case,” where a referral to a chiropractor might be authorized:The odd case where a spinal manipulation is indicated for a particular condition such as fixated facet joint, something of that nature, where they have a mechanical obstruction that has a low amplitude, high velocity mobilization may be beneficial for, we have the flexibility to refer to a chiropractor, as they specialize in this technique. (PT, K3)
A CFHS physiotherapist shared views on the gatekeeping process and the factors motivating some CAF members to pursue chiropractic care. The assumptions made explicit in the following quote may appear paternalistic and the perception may raise questions surrounding gatekeepers’ motivations and lack of transparency in outsourcing decisions:So, what typically happens, the patient comes in and says, ‘I want chiropractic care’ and the doctor says, ‘Well, have you done any physio?’ This is where the patient and the physician can be in a little bit of a position of power. They may say something like, ‘No, I have tried physio and it doesn’t work.’ In my experience, a large portion of these patients have come once or twice for physio and have stopped doing their exercises and have basically been non-compliant.
There are a percentage of patients that have done physio, have done their due diligence, have worked hard but have not gotten the results they want, there are some of those patients and those patients are very few and there is just not that many out there... So very seldom is that choice of chiropractic care based on a biomechanical assessment and sound assessment findings. (PT, K9)
Facilitating access to understanding of roles
When discussing issues associated with role clarity, and the perceived duplication of services between physiotherapists and chiropractors relative to MSK conditions, one physiotherapist (PT, K9) espoused critical questions: “Is there any reason to send anyone for chiropractic care? What is the scientific evidence to suggest that chiropractors can do a better job than our physiotherapists and what is the determining factor for this?” Importantly, another CFHS physiotherapist posed the same questions, but in a slightly different manner:What would the difference be? What would be the net overall benefit of having a chiropractor in the clinic when the services provided are essentially going to be the same? ...If you really want to look at how a chiropractor would function in a military setting just look at how a physiotherapist is functioning in a military setting and it would be the same. (PT, K25)
A CFHS physiotherapist with managerial experience, emphasized organizational barriers, including current labour-management relations, to the integration of chiropractic services into CDUs across the country.
For example, “The public service union is an extremely strong union right now... If somebody else comes into this clinic that provides the exact same services as our physiotherapists provide but are getting paid substantially more, the union would have something drastic to say about that.” (PT, K25)
A physician addressed interprofessional care in the CFHS with emphasis on the complexities of bringing healthcare professionals together for the common good of a patient: “The scopes of practice, collegiality, respect, and everyone has to know their ‘arcs of fire,’ how to engage...” (MD, K14).
Referring more specifically to the possibility of including off-base chiropractors as members of the healthcare team, the physician asked:Who gets involved when its physio and chiropractor that are both involved with one patient? I think at the moment we try physio with similar physio, similar [same thing with] chiropractor, and not mix-and-match. Obviously some patients are very complex; maybe there is a case of having both specialities providing care simultaneously. (MD, 14)
A CFHS physician began his interview by stating, “MSK and mental health are my two largest presenting complaints.” Later on, he addressed barriers associated with the blurred roles of physiotherapists and chiropractors in the delivery of MSK services. The key informant posits that within both professional groups there are significant inconsistencies in approach, services and patient outcomes that complicates referral and outsourcing decisions.We find chiropractors, some of them are excellent, right, provide such great advice, they provide modalities, they are effective, patients are satisfied. And others that are missing the mark and tell me that their spine has something to do with diabetes or their pancreas, you know. It doesn’t make any biological sense and we don’t always know that ahead of time until we try them (laugh). So there is some overlap in terms of what they provide and we are careful about that because by the time you get to 20 sessions of physio and we are considering chiropractic care, or they have done a few sessions of chiro care and you are considering some different modalities there is an overlap. (MD, K12)
In the above quote, the CFHS physician alluded to some chiropractors providing questionable services, not supported by current scientific evidence, and the questions this raises for those fulfilling gatekeeper roles within the CFHS. This observed diversity in individual chiropractic practices, reportedly raises questions of the trustworthiness of certain practices and creates uncertainty among decision-makers, which in turn negatively impacts the frequency of chiropractic referrals and their ultimate intergration. [38]
The observed diversity and competing factions within professions is common [39] but within the chiropractic profession continues to be a source of challenge in advancing the image of a unified profession [40] and promoting interprofessional collaboration. [36, 38]. The challenge is further omplicated by chiropractors holding pseudoscientific beliefs [41] and whom draw national media attention to the profession. [42] Our findings, situated within the broader public discourse surrounding the efficacy of some chiropractic practices, suggest that despite current research supporting the chiropractic profession’s well defined scope of practice and the integration of chiropractors into mainstream healthcare delivery [43], considerable confusion exists surrounding the scope and unique value-added contributions of the profession within the CFHS, and Canadian society, at large.
When discussing issues associated with diagnosing and treating MSK conditions in the CAF, a CFHS physician emphasized “having the right providers at the right time for the patient (MD, K1).
When explaining critical knowledge gaps, the physician does not distinguish between chiropractic and manipulation therapy:“The majority of the members that we refer out [for chiropractic care] have developed chronic musculoskeletal and low back pain disorders... I think the benefit of doing manipulative therapy and other types of chiro approaches on these people is very limited. I am not sure that we have the outcomes desired either, by referring them out at that late stage in the process... It’s important on our side to educate more of our prescribers or providers about what can chiropractic or manipulation therapy bring to an individual based on their condition and what are the most likely conditions that will respond to chiropractic or manipulative care?” (MD, K1)
The physician concluded the interview by providing a fairly recent and positive example related to mental health. In the following quote, he described how the CFHS strengthened IPC and enhanced role clarity, with emphasis on communication, education and outreach:“We’ve been able to develop better ways of communicating with external mental health clinicians... We do a lot internally, but we outsource a significant portion of mental healthcare, as well... We’ve been able, through local communication and outreach, to educate... clinicians in the community about the specific needs of the military and what we need from them in return from our consultation.” (MD, K1).
The physician (MD, K1) stated that although the military had yet to come-up with a standardized approach or a national strategy, local initiatives, involving off-base mental health clinicians, demonstrated the positive outcomes associated with “better outreach and better communication with external providers.”
Discussion
Currently, CAF members have access to chiropractic services within the spectrum of care and at the discretion of CFHS providers. Within this context, our overall findings inform health policies, practices and applied research that could address existing barriers to effective referrals and improve quality of care. [37] However, it is simplistic to suggest that barriers can be addressed and opportunities fully realized without an in-depth understanding of the factors underpinning IPC related to MSK conditions, at multiple levels: CAF member, healthcare professional, healthcare team, organization, profession, and civil society.
Interprofessional practice is often discussed in the literature from the perspective of key and enabling competencies. Recognizing the complexities of IPC practice and the limitations of current theoretical underpinnings informing our understanding of ‘competencies,’ Flood et al. (2019) call for expanding the discourse. [44] Utilizing a phenomenological hermeneutic approach, the authors conclude that “working in the ‘spirit’ of interprofessional practice goes beyond competencies... [It] cannot be reduced to separate aspects, it is about everything” (p. 493). [44] This finding has relevance to our work, with special emphasis on the barriers we identified related to role clarity and interprofessional communication. For example, in the Communication domain, efforts to evaluate IPC competencies related to interpersonal skills, using current assessment tools/ resources, are limited in their ability to “capture the spirit” – that is, the “comportment the person brings, shaped by culture, history, life experience, influenced by mood, time and challenge...” [41]
In consideration of our findings of the perspective of a limited chiropractic scope of practice, if one is to advance an ontological approach to IPC and Interprofessional Education (IPE), according to Flood et al. each individual must “strip oneself of the professional mask, to be revealed as ‘human’, a person with feelings, ideas, history and hope” (p.498). [44]
The development of interprofessionality (i.e., the field of interprofessional practice and interprofessional education) implies a better understanding of the determinants and processes that influence both IPC and IPE. [45] This emerging concept is grounded in the notion that silo-like division of professional responsibilities “is rarely naturally nor cohesively integrated in a manner which meets the needs of both the clients and the professionals” (p. 9). [45] Our findings suggesting limited understanding of the role of chiropractors beyond providing manipulaton supports the notion that practitioners are often limited in their abilities to recognize professional values, stereotypes or misconceptions of other healthcare professionals. Such limited abilities may be grounded in neoliberalism, where professions focus on their autonomy, services and entrepreneurial competitive interests rather than on professionalism, where the best interest and concern of the patient are foremost considered. [46]
Ultimately, in order to address factors that hinder chiropractic IPC within the unique culture of the CFHS, strategies need to be developed with the goal of establishing more cohesive and less fragmented practices. Similar barriers have been identified in other settings wherein insider groups’ subordination of outsider groups close access to opportunities and resources and use demarcationary strategies to monitor, create and control boundaries, thus securing a priviledged access to markets. [21, 39] To this end, our work calls for increased attention to the role of gatekeeper in model design and testing. In addition, we need to further explore the patients, CAF service members, lived experience to capture their perspective and opinion of such a collaborative role.
Increasingly, Canadian experts in IPC emphasize the need to move from an emphasis on individual competencies to an examination of competencies at the team-level. This requires an increased understanding of and respect for professional roles, their complex interactions, and the facilitators and barriers to interprofessional teamwork. Lingard et al. (2012) employed the theoretical lens of activity theory to explore the inherent complexities associated with IPC and IPE. [47] The findings challenge two historical premises: the notion that stable professional roles exist, and the ideal of a unifying objective of ‘caring for the patient’ (p. 876). [47]
Our conclusions support the notion that amongst MSK service providers, roles and scopes of practice are increasingly fluid and often blurred, perceived to vary from base-to-base, and are often context-specific. We support the conclusions of Lingard et al. that collaborative expertise involves being attuned and responsive to this fluidity” (p. 875). [47] Further, although “patient-centred care” was earlier identified as a key facilitator to integrating chiropractic care in the CFHS [11], we concur with Lingard et al. (2012), that this ideal is shared widely among diverse professional groups. [47] Therefore, “as a motivation for collaborative action it is in constant tension with other relative motives, such as appropriate resource allocation and trainee education” (p. 876). [47]
Given the ongoing re-design of healthcare systems, integrating aligning institutions with organization-specific missions and work cultures will be a priority. Within this context, interprofessional co-managing will be expected, requiring new ways of working and enhanced capacities for managers and team leaders in relationship development. According to Clausen et al., based on an integrative review of educational interventions to enhance competencies for IPC among nurse and physician managers, competencies for collaborative management practice have yet to be addressed. [48] Novice managers will need to build strategic and effective partnerships to increase productivity, mobilize knowledge across teams and settings, and eliminate perceptions of systemic overlap or role duplication in order to ensure positive impact for patients.
Our findings reinforce the significance of strengthening IPC specific to MSK conditions in the CFHS, including an examination of gatekeeping roles, role clarity and responsibilities and outcomes of care. We propose that it is timely to investigate models of care that nurture and sustain inter-provider and inter-team relationships to plan and coordinate care for MSK conditions, within the CFHS, and its extended referral networks. Rather than considering professions as an intervention with competing interests, consider their full scope of practice and differing views as complementary instead of exclusionary to be applied for the benefit of patient care.
Our findings emphasize the significance of professional cultures as barriers to effective IPC. We are reminded of the pioneering work of Hall (2005) who addressed the increasing specialization of healthcare professions. [49] This has led to the “further immersion of learners into the knowledge and culture of their own professional group.” We have seen through our work that constantly defining and redefining professional roles and/or boundaries visŕ-vis MSK conditions, increases the risks inherent in one professional group excluding or forcing out their rivals – often with the propensity of describing rival groups as “frauds, amateurs, or incompetents” (p. 189). [49]
Given the unique environment of the CFHS, coupled with other distinguishing characteristics of military culture anchored in rules, norms, values and traditions [50], there may be a danger in ‘insiders’ seeking scapegoats from within its external referral networks when faced with complex patient care challenges. According to Hall (2005), this can exempt members of a group from taking full responsibility for the consequences of their work (p. 189). [49] The notion of interprofessional cultural competence is especially important when healthcare teams are involved in internships and work placements, charged with ensuring that students have the requisite knowledge and skills to collaborate effectively in the real world. [51]
An examination of factors that foster or prevent interprofessional team working in primary and community care concluded that team structure (team premises) and team process were key considerations. [6, 52] For example, shared team premises may enhance information transaction, facilitate communication, and increase personal familiarity. In contrast, members with separate bases or work settings were less integrated with the team, which may limit team functioning and effectiveness. [53]
The stability of the team was also deemed important in fostering IPC. Our findings suggest that from the perspectives of off-base contractors, workplace isolation and the dynamic composition of CFHS healthcare teams, due to military transfers, deployment and other internal factors, are contributing to IPC barriers. In addition, evidence suggests that the vast majority of providers outside of military facilities do not demonstrate military cultural competency, which impacts not only patient care but impedes effective communication and formation of alliances. [54] Thus, ensuring military cultural competence of civilian healthcare providers through appropriately structured IPE and ensuring its implementation into practice is another essential component successful IPC.
In summary, our findings illuminate a central question for the CFHS that has yet to be addressed: “Is there any reason to send anybody for chiropractic care?” Although stakeholders (CFHS policymakers, practitioners, and off-base service providers) articulate a common goal, that is, achieving and maintaining healthy spines in CAF members, our findings suggest that they construct their professional roles, scopes of practice and work cultures very differently. Where the edges of their scopes or “territories” meet, the underlying conditions become “boundary objects” that must be negotiated. [55]
We posit that the CFHS and its extended MSK referral networks, offers an information-rich “case” to explicate promising practices in IPC, with the potential to bring down the walls imposed by professional silos, for the benefits of policymakers, managers, healthcare professionals, educators, society, but most importantly CAF patient members.
Limitations
In presenting results in this manuscript we focus on one of six IPC domains (i.e., role clarity). To further explore issues central to this work, additional publications should include an in-depth examination of other IPC competency domains relative to key patterns or over-arching themes. Our efforts to obtain detailed documentation related to CFHS referrals to chiropractors and physiotherapist located off-base (e.g., numbers, location, diagnoses, etc.), were not successful during the time that data was being analyzed and final reports prepared.
Our study consisted of military personnel, public servants and contractors of the Canadian Armed Forces and civilians. Participants were from different CAF bases, healthcare services, and geographic regions across Canada. Military personnel were of different ranks and military experience. It is possible that individuals who were not invited to participate may have expressed different views. We also did not explore patients’ perspectives of care delivered within the CFHS nor their experiences when requesting or being referred for chiropractic services.
Conclusions and recommendations
Our study provides the first qualitative analysis of barriers and opportunities for the collaboration of chiropractic within the unique CFHS environment. This manuscript, exploring IPC relative to MSK conditions in the CFHS, elucidated barriers and opportunities to potentially inform a series of next steps involving key stakeholders. Further, findings reinforce the importance of bringing CAF members’ voices to this important work.
Based upon our qualitative analysis, the research team posits the following recommendations gleaned from the over-arching experiences, perceptions, meanings and interpretations shared by key informants, together with reflexivity of the researchers, and an in-depth description and interpretation of the research problem. Our recommendations are:
Given the prevalence of MSK conditions in the CAF, and demonstrated interest in exploring cost-effective, evidence-based and sustainable changes to the delivery of care, design a pilot project to explore the interdependencies between the role of the physiotherapist and those of other professionals to optimize each members’ scope.
In collaboration with academic partners and funding agencies, carry out research to increase understandings of the CAF members’ experiences in seeking treatment for MSK conditions, both on-and-off the military base. This could include information-rich case studies, evaluative studies and quality care initiatives.
In partnership with educational partners, develop a suite of interactive IPE tools and resources, including military cultural competence and simulations, to depict the complexities associated with IPC in the treatment of MSK conditions and how best to mitigate these barriers in the real world of military healthcare.
Within the CFHS, expand continuing education sessions, and other knowledge dissemination and training activities focused on MSK conditions, to include, where feasible, broad representation of professionals from across the continuum of care, and respectful of the unique military culture and its environment.
MSK service providers must ensure that practices are professional, evidence-based, carried out with competence, with emphasis on clear and respectful communication strategies to strengthen care, coordination, collaboration and common understandings of care.
Appendix A. Interview Guide
Can you share an example of a positive collaborative experience that you have experienced, or have observed? This can be related to musculoskeletal pain, but not necessarily so...
Probe: What are the observed benefits of collaboration in the example that you provided?In a collaborative setting within the CAF, for example, if a patient walks in with back pain can you describe what would happen?
Probe: How is choice of treatment determined? What role does the patient play? Which providers are accessed? When and why?
Probe: Collaborative practice within the CAF is evolving. How does staff mobility, e.g. posting changes, affect the establishment of collaborative practice?We understand that chiropractic services are included in the CAF spectrum of care. How would you describe the military spectrum of care?
Probe: How would you describe the chiropractic spectrum of care within the CAF? How do CAF patients access chiropractic services? How does the process work, e.g. direct referral from base health care provider; patient requested; only after limited treatment response, etc.For what conditions would you see chiropractic care being accessed? Is there a need in the CAF?
Probe: nature of condition; duration of condition (acute vs chronic)What are your suggestions for the research team as we explore the issue of chiropractic care collaborations within the CAF health care system?
Probe: Can you elaborate on chiropractic care on-base? Off-base? Current challenges and opportunities of such access? Impact on patient care? If collaboration with chiropractic care in the CAF health care system is not necessary, why is it not necessary?What is nature of communication between chiropractors and CAF health care providers?
Probe: does communication exist, in what form? How can it improve, if so how?What criteria would you use to assess the impact of collaborative practices in the CAF between medical, physiotherapy and chiropractic services?
Probe: what are the indicators? What are the outcomes?Of everything we have spoken about today, what would be the key messages or key points you would use to summarize this discussion?
Who else, or which organization, do you recommend we speak to on this topic? Could you please provide us with the contact information? Can we use your name when we contact them?
Probe: Could you recommend a physician, physician assistant (PA), nurse, physiotherapist, chiropractor or others who we should speak to on this topic?Funding
The study was funded by a grant from the Canadian Chiropractic Association and the Ontario Chiropractic Association. The funders did not have a role in study design, analysis or preparation of this manuscript. The views expressed are solely those of the authors and do not reflect the official policy or position of the Canadian Armed Forces, the Department of Defense, or the Canadian Government.
References:
Aiken A, Bélanger S, editors.
Shaping the future: Military and veteran health research
Kingston: Canadian Defence. Academy Press; 2011.Born J, Hawes R, Whitehead J.
Results from Health and Lifestyle INformation Survey of Canadian Forces personnel 2008/2009:
Regular Force version: Your health speaks volumes.
Ottawa: Government of Canada; 2010Directorate of Force Health Protection.
Canadian Forces Health and Llifestyle Information Survey – 2008/2009.
Ottawa: Department of National Defence; 2010Canadian Forces Health Services Group.
Surgeon General’s Report 2014 Consolidation, Innovation, Readiness.
Ottawa: Government of Canada, Department of National Defence; 2014.Caring for our own.
A Comprehensive approach for the care of CF ill and injured members and their families.
Ottawa: National Defence; 2012Mior S, Sutton D, et al., Daphne To.
Chiropractic Services in the Active Duty Military Setting: A Scoping Review
Chiropractic & Manual Therapies 2019 (Jul 15); 27: 45Way D, Jones L, Busing N.
Implementation Strategies: Collaboration in Primary Care – Family Doctors
& Nurse Practitioners Delivering Shared Care.
Toronto: The Ontario College of Family Physicians; 2000Branson RA.
Hospital-Based Chiropractic Integration Within a Large
Private Hospital System in Minnesota: A 10-Year Example
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 740–748Johnson C, Baird R, Dougherty PE, et al.
Chiropractic and public health: current state and future vision.
J Manipulative Physiol Ther. 2008;31:397–410Kopansky-Giles D, Walker B, Borges S.
Integration of chiropractic into multidisciplinary and hospital-based settings.
In: Haldeman S, editor. Principles and practic of chiropractic. 3rd ed.
New York: McGraw-Hill; 2005. pp. 1165–1179Mior SA, Vogel E, Sutton D, et al.
Exploring Chiropractic Services in the Canadian Forces Health Services -
Perceptions of Facilitators and Barriers Among Key Informants
Military Medicine 2019 (May 1); 184 (5-6): e344–e351Creswell J, Poth C.
Qualitative Inquiry & Research Design Choosing Among Five Approaches. 4th ed.
Thousand Oaks: SAGE Publications; 2018Smith JA.
Reflecting on the development of interpretative phenomenological analysis
and its contribtuion to qualitative research in psychology.
Qual Res Psychol. 2004;I:39–54Smith JA, Osborn M.
Qualitative psychology: A practical guide to research methods.
UK: Sage; 2003.Smith JA, Flowers P, Larkin M.
Interpretative Phenomenological Analysis: Theory, Method and Research.
Los Angeles: Sage; 2009.Johnson JL.
Completing a Qualiltative Project: Details and Dialogue.
Thousand Oaks, CA: SAGE; 1997Robinson O.
Sampling in interview-based qualitative research: a theoretical and practical guide.
Qual Res Psychol. 2014;11:25–41Dorflinger L, Moore B, Goulet J, et al.
A partnered approach to opioid management, guideline concordant care
and the stepped care model of pain management.
J Gen Intern Med. 2014;29(Suppl 4):870–876.Christine M. Goertz, Cynthia R. Long, Robert D. Vining, Katherine A. Pohlman,
Bridget Kane, Lance Corber, Joan Walter, and Ian Coulter
Assessment of Chiropractic Treatment for Active Duty, U.S. Military Personnel
with Low Back Pain: Study Protocol for a Randomized Controlled Trial
Trials. 2016 (Feb 9); 17 (1): 70Pope C, Mays N.
Qualitative Resesarch in Health Care. 3rd ed.
Hoboken, NJ: Blackwell; 2007Hollenberg D.
Uncharted ground: patterns of professional interaction among complementary/
alternative and biomedical practitioners in integrative health care settings.
Soc Sci Med. 2006;62:731–744Shuval JT, Gross R, Ashkenazi Y, et al.
Integrating CAM and biomedicine in primary care settings:
physicians’ perspectives on boundaries and boundary work.
Qual Health Res. 2012;22:1317–1329Hirschkorn KA, Bourgeault IL.
Conceptualizing mainstream health care providers’ behaviours
in relation to complementary and alternative medicine.
Soc Sci Medicine (1982) 2005;61:157–170Glaser B, Strauss A.
The Discovery of Grounded Theory Strategies for Qualitative Research.
Chicago, Illinois: Aldine Publishing; 1967Strauss A, Corbin J.
Basics of Qualitative Research: Techniques and Procedures for Developinng Grounded Theory.
Thousand Oaks, CA: Sage; 1998Fusch PI, Ness LR.
Are we there yet? Data saturation in qualitative research.
The Qualitative Report. 2015;20:1408–1416Hale ED, Treharne GJ, Kitas GD.
Qualitative methodologies II: A brief guide to applying
Interpretative Phenomenological Analysis in musculoskeletal care.
Musculoskeletal Care. 2008;6:86–96Lincoln Y, Guba EG.
Naturalistic inquiry.
Newbury Park, CA: Sage; 1985Denzin N, Lincoln Y.
Handbook of Qualitative Research. 5th ed.
Thousand Oaks, CA: SAGE Publications; 2018Larkin M, Watts S, Clifton E.
Giving voice and making sense in interpretative phenomenological analysis.
Qual Res Psychol. 2006;3:102–120Michie S, Hendy J, Smith J, et al.
Evidence into practice: a theory based study of achievieng national targets in primary care.
J Eval Clin Pract. 2004;10:447–456van Manen M.
Writing qualitatively, or the demands of writing.
Qual Health Res. 2006;16:713–722van Manen M.
Phenomenology of practice: Meaning-giving methods in
phenomenological research and writing.
Walnut Creek, CA: Left Coast Press; 2014Herman PM, Coulter ID:
Complementary and Alternative Medicine: Professions or Modalities?
Policy Implications for Coverage, Licensure, Scope of Practice,
Institutional Privileges, and Research.
RAND Corporation, Santa Monica, California: (2015. pp. 1–76)Richardson D, Calder L, Dean H, et al.
CanMEDS 2015 Physician Competency Framework
Frank J, Snell L, Sherbino J, editors.
Ottawa: Royal College of Physicians and Surgeons of Canada; 2015Busse JW, Jim J, Jacobs C, et al.
Attitudes Towards Chiropractic: An Analysis of Written Comments
From a Survey of North American Orthopaedic Surgeons
Chiropractic & Manual Therapies 2011 (Oct 4); 19: 25Dunn AS, Green BN, Gilford S.
An Analysis of the Integration of Chiropractic Services Within
the United States Military and Veterans' Health Care Systems
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 749–757Triano JJ, McGregor M.
Core and Complementary Chiropractic:
Lowering Barriers to Patient Utilization of Services
J Chiropractic Humanities 2016 (Sep 15); 23 (1): 1-13Saks M.
Inequalities, marginality and the professions.
Curr Soc Rev. 2015;63:850–868McGregor M, Puhl A, Reinhart C, Injeyan H, Soave D.
Differentiating Intraprofessional Attitudes Toward Paradigms
In Health Care Delivery Among Chiropractic Factions:
Results From A Randomly Sampled Survey
BMC Complementary and Alternative Medicine 2014 (Feb 10); 14: 51Côté P, Bussičres A, Cassidy JD, et al.
A united statement of the global chiropractic research community
against the pseudoscientific claim that chiropractic care boosts immunity.
Chiropr Man Therap. 2020;28:21.Benedetti P, MacPhail W.
Chiropractors at a crossroad: The fight for evidence-based treatment and profession’s reputation.
The Globe and Mail. 2018 Nov 1;Chapin D.
Despite the Tired Narratives, Chiropractic is Backed by Evidence
The Globe and Mail. 2019 Feb 16;Flood B, Smythe L, Hocking C, et al.
Interprofessional practice: beyond competence.
Adv Health Sci Educ. 2019;24:489–501.D’Amour D, Oandasan I.
Interprofessionality as the field of interprofessional practice
and interprofessional education: an emerging concept.
J Interprof Care. 2005;19(Suppl 1):8–20Gliedt JA, Holmes BD, Nelson DA.
The Manchurian candidate: chiropractors as propagators of
neoliberalism in health care.
Chiropr Man Therap. 2020;28Lingard L, McDougall A, Levstik M, et al.
Representing complexity well: a story about teamwork,
with implications for how we teach collaboration.
Med Educ. 2012;46:869–877Clausen C, Cummins K, Dionne K.
Educational interventions to enhance competencies for interprofessional
collaboration among nurse and physician managers: An integrative review.
J Interprof Care. 2017;31:685–695Hall P.
Interprofessional teamwork: professional cultures as barriers.
J Interprof Care. 2005;19(Suppl 1):188–196Sturgeon-Clegg I, McCauley M.
Military psychologists and cultural competence: exploring implications
for the manifestation and treatment of psychological trauma in the British armed forces.
J R Army Med Corps. 2019;165:80–86Doll J, Haddad A, Laughlin A, et al.
Building interprofessional cultural competence: reflections of
faculty engaged in training students to care for the vulnerable.
Int Public Health J. 2015;7:131–138Xyrichis A, Lowton K.
What fosters or prevents interprofessional teamworking in
primary and community care? A literature review.
Int J Nurs Stud. 2008;45:140153Riva JJ, Muller GD, Hornich AA, et al.
Chiropractors and Collaborative Care:
An Overview Illustrated with a Case Report
J Can Chiropr Assoc. 2010 (Sep); 54 (3): 147–154Meyer EG, Writer BW, Brim W.
The importance of military cultural competence.
Curr Psychiatry Rep. 2016;18:26Akkerman S, Bakker A.
Boundary crossing and boundary objects.
Rev Educ Res. 2011;81:132–169Toronto Academic Health Science Network Practice Committee and
University of Toronto Centre for Interprofessional Education.
Interprofessional Care Competency Framework and Team Assessment Toolkit
Toronto: 2017
Return to INTEGRATED HEALTH CARE
Return NON-PHARMACOLOGIC THERAPY
Return to CHIROPRACTIC CARE FOR VETERANS
Since 9-26-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |