

Selecting a Dietary Supplement with Appropriate
Dosing for 6 Key Nutrients in PregnancyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Am J Clin Nutr 2023 (Apr); 117 (4): 823–829 ~ FULL TEXT
OPEN ACCESS Katherine A. Sauder • G Lance Couzens • Regan L. Bailey • Christine W. Hockett • Karen M. Switkowski • Kristen Lyall • Jean M. Kerver • Dana Dabelea • Luis E. Maldonado • Thomas G. O’Connor • Sean CL. Deoni • Deborah H. Glueck • Diane J. Catellier, on behalf of program collaborators for Environmental influences on Child Health Outcomes.
Lifecourse Epidemiology of Adiposity and Diabetes (LEAD) Center,
University of Colorado Anschutz Medical Campus,
Aurora, CO, USA.
Department of Population Medicine,
Harvard Medical School and
Harvard Pilgrim Health Care Institute,
Boston, MA, USA.
Editorial Commentary:
Like Shaklee's Landmark Studies, this paper is another Landmark of a sort, in which scientists from 10 different medical institutions pooled their resources to review 28,307 dietary supplements, to find out how many of them contained the proper dosage all 6 of the key nutrients that support a healthy pregnancy.
Guess what? Shaklee's Life Strip with Iron was the ONLY supplement to pass their test! Once again, Shaklee science prevails, and this study irrefutably puts Shaklee at the top of the nutrition industry.

Background: Most pregnant women in the United States (US) are at risk of inadequate intake of key nutrients during pregnancy from foods alone. Current dietary supplement practices reduce risk of inadequacy for only some nutrients and induce excessive intake of other nutrients.
Objectives: Our study aimed to estimate the doses of supplementation needed to help most pregnant women achieve the recommended intake without exceeding upper limits for key prenatal nutrients and to identify US dietary supplements providing these doses.
Methods: We conducted 24–h dietary recalls in 2450 pregnant participants aged 14–50 y from 2007 to 2019. We estimated the usual intake of vitamins A and D, folate, calcium, iron, and ω-3 FAs (omega-3 fatty acids) from foods alone. We calculated the target doses of supplementation needed to shift 90% of participants to consume above the estimated average requirement and keep 90% below the tolerable upper limit. We identified products in the Dietary Supplement Label Database (DSLD) providing these target doses of supplementation.
Results: The target dose for supplementation was≥198 mcg retinol activity equivalents of total vitamin A
(with ≤2063 mcg preformed retinol);
7–91 mcg vitamin D;
169–720 mcg dietary folate equivalents of folic acid;
383–943 mg calcium;
13–22 mg iron; and
≥59 mg ω-3 FAs (omega-3 fatty acids) .
NOTE: ≥ means "greater than or equal to", as in 5 ≥ 4
≤ = less than, or equal to, as in 4 ≤ 5Out of 20,547 dietary supplements (including 421 prenatal products), 69 products (33 prenatal) contained all 6 nutrients; 7 products (2 prenatal) contained target doses for 5 nutrients. Only 1 product (not a prenatal) contained target doses for all 6 nutrients, but it currently costs ~USD200/mo and requires 7 tablets per daily serving.
Conclusions: Almost no US dietary supplements provide key nutrients in the doses needed for pregnant women. Affordable and convenient products that fill the gap between food-based intake and estimated requirements of pregnancy without inducing excess intake are needed to support pregnant women and their offspring.
Keywords: calcium; dietary supplements; folic acid; iron; pregnancy; vitamin A; vitamin D; ω-3 FAs.
From the Full-Text Article:
Introduction
Inadequate and/or excessive intake of nutrients during pregnancy is associated with adverse maternal and offspring health outcomes. [1–8] More than half of pregnant women in the United States (US) are at risk of inadequate intake of vitamin D, folate, and iron from foods alone, and one-third of them are at risk of inadequate intake of vitamin A and calcium. [9] Dietary supplement use is common (>70% of pregnant women), but it does not eliminate risk of inadequate intake of all nutrients and causes >25% of pregnant women to consume more than the maximum intake levels of folic acid and iron, which is likely to cause adverse health effects. [9, 10]
This suggests that formulations of commonly used dietary supplements are not appropriately addressing the gap between food-based intake and estimated requirements in pregnancy. Additional constraints of out-of-pocket costs, insurance-approved formularies, and payer reimbursements render choosing a specific product challenging for patients and healthcare teams alike.
To address this knowledge and practice gap, we aimed to identify the doses of key nutrients that pregnant women should consume from dietary supplements to bridge the gap between food-based intake and estimated requirement. Our analysis considered 6 nutrients with the strongest evidence for a potential benefit for maternal-child health outcomes: vitamin A [11], vitamin D [12], folate/folic acid [13, 14], calcium [15, 16], iron [14], and ω-3 FAs. [17] Our goals were to provide target doses for supplementation of these key nutrients and generate a list of products currently available in the US that provide these target doses.
Methods
We analyzed the dietary intake data collected from pregnant participants of the NIH Environmental influences on Child Health Outcomes (ECHO) program. [18] ECHO is a consortium of 69 observational cohorts of mothers and offsprings established to understand the effects of early life exposures on child health and development. We included dietary data from 2450 participants from 6 cohorts across 5 states (Supplemental Table 1). All cohort-specific protocols were approved by the institutional review boards with jurisdiction, and participants provided informed consent. Sociodemographic-, pregnancy-, and weight-related participant data were collected via self-report at enrollment and/or medical records.
Dietary intake data
Dietary intake was assessed with interviewer- or self-administered 24–h recalls that query all foods and beverages consumed in the prior 24 h or the full day before using standardized and validated methods. [19, 20] We excluded dietary supplement data as our goal was to understand the intake from food alone. Participants completed >1 24–h dietary recall from ≥6–week gestation until delivery. Cohorts processed dietary data locally using appropriate databases for nutritional content at the time of data collection. For each recall, cohorts provided the intake data for vitamins A (total retinol activity equivalents and preformed retinol only), vitamin D (total), folate (total dietary folate equivalents (DFEs) and synthetic folic acid only), calcium (total), iron (total), and ω-3 FAs (total eicosapentaenoic acid + docosapentaenoic acid + DHA).
DRI (Dietary Reference Intakes)
We defined target intake with the estimated average requirement (EAR) and tolerable upper limit (UL) for pregnant women specified by the dietary reference intakes (DRIs). [21] The EAR reflects the average daily nutrient intake level estimated to meet the requirements of half of the healthy individuals in a group. The UL is the highest daily nutrient intake that is likely to pose no risk of adverse health effects in most individuals. As exact nutrient requirements for any specific individual cannot be defined, risk of inadequacy for a population can be estimated with the cut-point method whereby the percentage of individuals with intake below the EAR or above the UL reflects the percentage at a risk of inadequate or excessive intake, respectively. [22] For ω-3 FAs, the EAR and UL are not defined. We selected a target of 100 mg/d on the basis of a recent meta-analysis reporting the benefits of long-chain ω-3 FAs for perinatal outcomes. [17]
Dietary supplement data
Dietary supplements are regulated by the FDA as a food rather than a drug [23]; thus, there is no official listing of all available products. [24] To our knowledge, the most complete listing in the US is the NIH Dietary Supplement Label Database. [25] This database was created in 2008 to provide researchers and consumers with information on dietary supplement nutrient composition. Composition data are derived from product labels, as laboratory verification of data on all available dietary supplement products is not feasible and the FDA does not require third-party verification of contents for “foods”. [26] As of December 13, 2022, the database contained composition data on >136,000 products currently or previously available in the US, including ~800 products specifically marketed for pregnant and/or lactating women. [27] We abstracted composition data for all products classified as “on market” that contained ≥1 of the 6 nutrients of interest. We did not restrict our search to prenatal products specifically because products advertised for populations or other conditions could contain the target doses needed for pregnant women. We also confirmed that the prescription prenatal products (n = 39) indexed by DailyMed (the database of label information submitted by manufacturers to the FDA) as of December 13, 2022 were included. Thus, our dietary supplement list includes all prescription and nonprescription prenatal dietary supplements, in addition to nonprescription dietary supplements for all other populations.
For all products, we converted units as needed to facilitate comparison with the DRI [for example, international units (IU) to micrograms]. [28] For vitamin A, the UL applies only to preformed retinol. We calculated the amount of preformed retinol separately from provitamin A (that is, β-carotene) on the basis of the label details. When relative amounts were not specified on the label, we assumed that 100% of the vitamin A was retinol to avoid underestimating the potential retinol intake. For folic acid, labeling requirements changed from specifying folic acid in micrograms to micrograms of DFE (mcg DFE) beginning in 2016. When labels did not specify DFE in the units for folic acid, we applied a conversion factor of 1.7 to estimate mcg DFE. [28] For selected products, we consulted manufacturer and distributor websites to confirm that the product was still available in the market with the same nutrient composition as recorded in the database and to ascertain current cost.
Statistical analyses
Cohorts transferred individual level data to the ECHO Data Analysis Center for analysis, including nutrient data for ≥1 repeated observations (that is, days) for each participant. Dietary intake analyses were conducted separately for participants aged 14–18 y compared with 19–50 y because the DRIs for pregnancy vary by age. [21] We used macros developed to implement the NCI method to produce the mean and standard error for a given usual intake, as well as the percentiles of intake using the probability approach. [29] The statistical model fit using this procedure incorporated covariate adjustment for the day of the week of the dietary recall (weekend/weekday) and a random effect accounting for the clustering of participants within ECHO cohorts. This model produces population point estimates by partitioning out the within-person random variation (that is, day-to-day) when estimating the distributions of intakes. This method has been shown to be valid for obtaining usual intake distributions even when not all participants have repeated recalls. [30, 31]
We defined the lower limit for target supplementation by calculating the difference between the EAR (or 100 mg/d for ω-3 FAs) and the intake at the 10th percentile for each nutrient. Similarly, we defined the upper limit for target supplementation by calculating the difference between the UL and the intake at the 90th percentile for each nutrient. The resulting range indicates the supplementation dose needed to reduce the proportion of participants with intake below the EAR to ≤10% while simultaneously maintaining the intake of ≥90% of participants below the UL. For simplicity, we defined the overall target range as the one that would provide sufficient (but not excessive) intake for both age groups. We then classified each dietary supplement as that providing target doses (within the range) and that providing too little (below the range) or too much (above the range) of each nutrient, and counted the number of nutrients provided in target doses.
Results
Participants

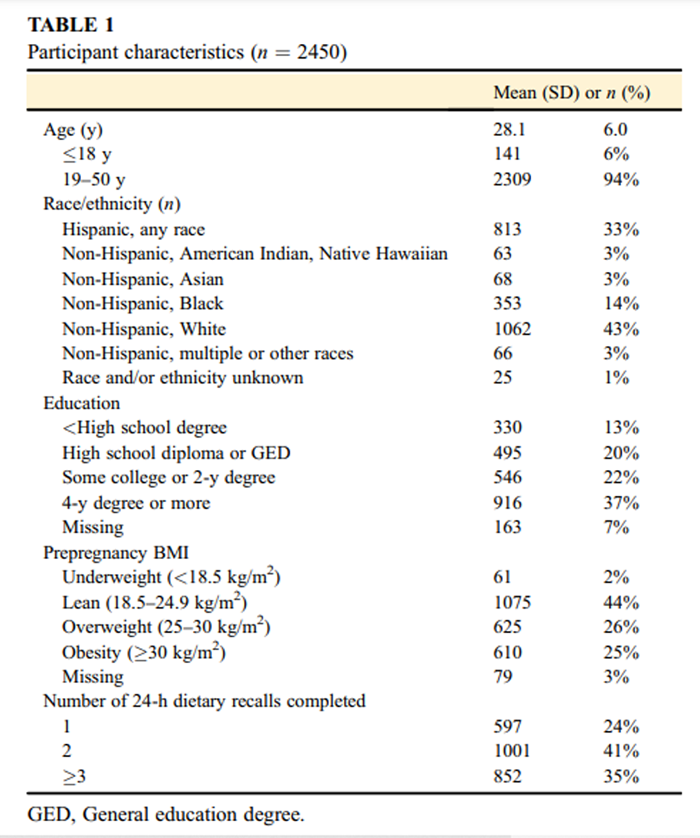
Table 1 The characteristics of the 2450 participants are presented in Table 1. Our sample was diverse in terms of race and ethnicity (43% identified as non-Hispanic White), education (33% had high school degree or less; 37% had a 4–y college degree or a higher qualification), and weight (44% of lean weight, 51% being overweight or obese). Participants completed 6106 recalls (76% completed ≥2 recalls).
Dietary intake
Table 2
page 4The intakes of vitamin A (all forms), retinol only, vitamin D, folate (all forms), folic acid only, calcium, iron, and ω-3 FAs from food sources alone at selected percentiles are reported in Table 2, with the full distributions presented graphically in Supplemental Figure 1. Risk of inadequate intake was the greatest for vitamin D and iron (83%–96% at risk for both age groups), followed by ω-3 FAs (67% of younger participants at risk and 50% of older participants at risk), calcium (55% of younger participants at risk and 30% of older participants at risk), folate/folic acid (45% of younger participants at risk and 34% of older participants at risk), and then vitamin A (42% of younger participants at risk and 26% of older participants at risk). Risk of excessive intake based on food intake alone was 0% for retinol and vitamin D (both age groups), and <0.1% for folic acid (both age groups), calcium (older participants), and iron (older participants). The target supplementation for 90% of participants to exceed the average requirement (or 100 mg/d for ω-3 FAs) while limiting the intake of 90% of participants to below the upper limit for each nutrient within each age group and overall is reported in Table 2. Supplementary Figure 1 includes a graphical depiction of how the minimum dose of this target range of supplementation would impact the intake relative to recommendations. Supplemental Figure 2 is a simplified reference card with the target ranges for each nutrient in units commonly used on product labels, which is provided as a resource to guide patient and healthcare team evaluation of dietary supplements.
Dietary supplements
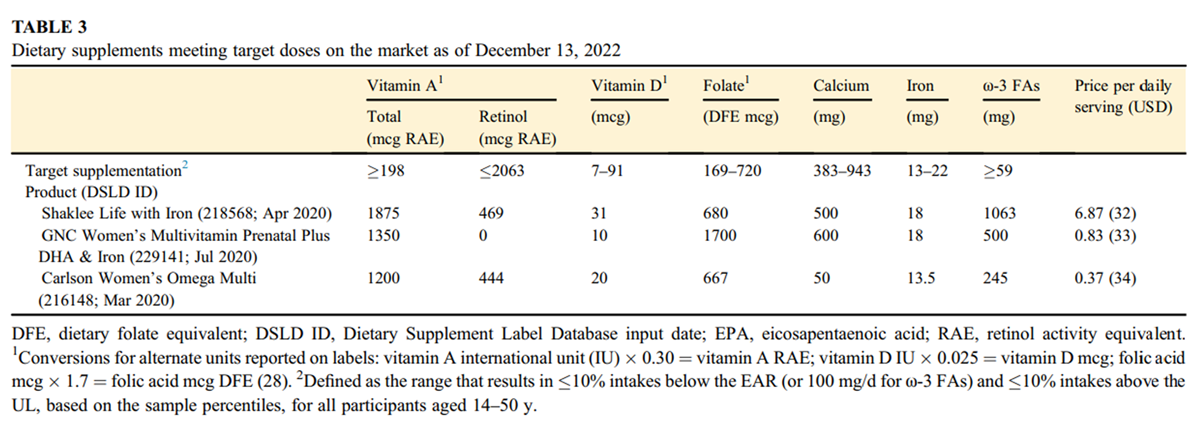
Table 3 We abstracted 28,307 products from the Dietary Supplement Label Database (Supplemental Figure 3). Of these, 21,536 contained ≥1 nutrient of interest (n = 989 were indexed as having ≥1 nutrient of interest but actually contained 0 levels); 20,547 represented unique products (n = 6305 were duplicates, typically because the same product was indexed multiple times with differing container quantities), of which 421 were labeled as prenatal products. The percent of products containing target doses of each key nutrient is presented in the Supplemental Figure 4 (overall) and Supplemental Figure 5 (those marketed as prenatals).
Of the 20,547 unique products, 69 [0.3%; 33 prenatal (0.3%)] did contain all 6 nutrients,
but only 1 [0.005%; (and not even a prenatal !)] contained target doses of all 6 nutrients
(Shaklee Life Strip with Iron; Table 3).
This product consists of 7 tablets per daily serving and costs USD 6.87 per day (~USD1850 for 9–mo supply). [32] Another 7 products (2 prenatal) contained all 6 nutrients but target doses for only 5 nutrients. By consulting the manufacturer and retail websites in May 2022, we determined that 5 of these (one prenatal) were no longer available and/or had changed formulation since entry into the database (Supplemental Table 2), whereas 2 (one prenatal) were available in the same formulation (Table 3). One of these would put 100% of our participants at risk of excessive intake of folic acid (GNC Women’s Multivitamin Prenatal Plus DHA & Iron) [33], and the other would put 46% of participants aged 14–18 y and 13% of participants aged 19–50 y at risk of inadequate intake of calcium (Carlson Women’s Omega Multi). [34] All products containing target doses of 5 or more nutrients (n = 100; 2 prenatal) are presented in Supplemental Table 3. The majority (n = 74) did not contain any ω-3 FAs, whereas some (n = 18) did not contain any iron. Few products contained too little calcium (n = 3), too little iron (n = 2), or too much folic acid (n = 2).
Discussion
We report wide targets of supplementation that are sufficient to achieve a minimum recommended intake of 6 nutrients during pregnancy. We determined that >12,000 US dietary supplements (including ~400 prenatal products) contain target doses of 1 + nutrient, <100 products contained target doses for 5 nutrients, and just 1 product contained target doses for all 6 nutrients. We posit the large US dietary supplement market is not meeting the nutrient needs of pregnant women.
Prior reports indicate that inadequate and excessive nutrient intake occurs during pregnancy, even with dietary supplements. [9, 10, 35–38] Although prior studies reported mean intakes from foods alone [9, 37, 38], they did not provide guidance on how much supplementation is needed to achieve the recommended intake without exceeding the limits. The recommendations by Adams et al. [37, 38] did not account for food-based intake, did not restrict supplementation based on upper safety limits, and called for supplementation of vitamins A and D and iron of 2–3 times the total (food + supplement) intake necessary per the DRIs. [38] Applied to our population, such supplementation would cause 100% of participants to exceed the iron UL, although other nutrient doses are within our recommended target. Regardless, Adams et al. [38] affirm that no US prenatal products supply appropriate doses for pregnancy.
Ninety percent contain more than the UL for folic acid, fostering concerns about over-supplementation of folic acid that can potentially induce adverse maternal/offspring outcomes. [39] About 50% contain >27 mg iron, which would induce excessive intake in ~30% of our participants. Differing intake recommendations stimulate further challenges. The Cochrane reviews affirm the potential benefit of supplementation for these nutrients, do not recommend specific doses [11–17], and include studies from populations in which food intake differs substantially from that of the US. Furthermore, the American College for Obstetrics and Gynecologists endorses the Recommended Dietary Allowance for minimum intake targets at the individual level [40], given their goal to minimize risk of inadequate intake without knowledge of individual requirements. However, these higher intakes may be unnecessary for most individuals and thus are not recommended for determining a population’s risk of inadequacy nor setting individual intake targets. [22, 41] With >70% of pregnant women using dietary supplements [9], often at the recommendation of their healthcare provider [42], formalization of evidence-based targets for supplementation for this population is urgently needed.
We acknowledge the limitations of our population-based approach, as personalized recommendations are appealing in general and clinically necessary for pregnant women with known medical conditions [for example, history of neural tube defects warrants 4000 (compared with 400) mcg folic acid]. [43] However, busy healthcare teams are not equipped to assess individual dietary intake (which varies day by day) and the individual’s physiological need (which varies across pregnancy) to provide individualized advice. [44] Instead, healthcare teams prescribe a “default” dietary supplement to most patients or give general advice for patient self-selection, but this is done without the knowledge of usual intake in pregnancy and thus may not resolve inadequacies or induce excessive intake. Additionally, such choices may require compromises between nutrients (given no optimal options are available); especially, availability, payer reimbursement, and out-of-pocket cost must be considered with nutrient content. Healthcare teams and patients can consult the reference card provided herein to select the best option among products available. This might require the use of multiple products, such as an individual ω-3 supplement alongside a multivitamin/multimineral, or individual iron or calcium supplements to achieve the intake targets. These strategies could address concerns about calcium interfering with iron absorption [45] and commonly-reported gastrointestinal side effects of supplemental iron [45]; however, it may be harder for patients to achieve high compliance with multiple products. Healthcare teams should be prepared to discuss strategies with patients to identify the best option for individual circumstances.
Further research is needed to determine the appropriate doses for diverse populations. Additional research is particularly needed for the intake of ω-3 FAs during pregnancy, as scientific evidence is not sufficient to establish an EAR. [47] A long-chain ω-3 FA supplementation of 100–1000 mg/d has been shown to reduce risk of preterm and early preterm birth, but a preferred dose has not been defined. [17] We used 100 mg/d as our total intake target, but acknowledge that 100 mg/d for supplementation specifically may be more appropriate.
We also note that other authoritative bodies such as the 1999 Workshop on the Essentiality of and Recommended Dietary Intakes for ω-6 and ω-3 FA and the WHO recommend an even higher intake: ≥200–500 mg/d during pregnancy. [48–50] Regardless, the mean intake is much lower, herein and nationally [51], suggesting that most pregnant women would benefit from a ω-3 FA supplementation. Evaluation of differing doses of these nutrients within randomized clinical trials is needed to clarify supplementation targets and, in turn, for the development of dietary supplements to support meeting such targets. Fortunately, among the top 100 products we presented in the Supplemental Table 3, all of those that contained ω-3 FAs included ≥245 mg of it, which would facilitate meeting intake targets higher than a minimum of 100 mg/d as recommended by the Cochrane review.
Our work has strengths and limitations. Dietary data were collected across the US for over 15 y of mandatory food fortification. Our sample had notable diversity and intakes were similar to nationally representative prenatal data, limiting concerns about selection bias. [9] Our adolescent sample was relatively small, warranting replication in larger cohorts. We selected nutrients on the basis of supporting Cochrane reviews, which concluded that these nutrients likely or potentially benefit maternal or offspring outcomes based on pooled clinical trial data. We acknowledge that other nutrients are also important and should be explored in future analyses; however, the number of dietary supplement products containing target doses for a larger number of nutrients is likely less than that reported here. Participants self-reported intake, limiting the accuracy of estimates [52], and cohorts utilized various dietary recall methods and 2 nutrient databases, which could increase variability in the estimates of nutrient intake. We did not examine bioavailability or circulating concentrations of these nutrients, which is critical to determining the actual deficiency or excessive concentrations. Manufacturers self-reported the dietary supplement content for the Dietary Supplement Label Database. As actual content is unknown but should be ≥80% of the labeled amount per FDA guidance [53], priority should be given to products with verified third-party testing. Our goal of shifting the intake of 90% of participants above the EAR and below the UL was arbitrary; higher percentage goals would require narrower ranges (for example, 286–443 mcg DFE of folic acid to achieve 99% above the EAR and 99% below the UL, compared with 169–720 to achieve 90% above the EAR and 90% below) and would further reduce the number of products providing target doses.
This study provides practical guidance for clinicians and pregnant women seeking to achieve the recommended nutrient intake to support maternal/offspring health. Nearly all pregnant participants were at risk of inadequate intake of ≥1 key nutrients from foods alone and thus may benefit from a carefully selected dietary supplement. Clarification of the upper and lower dosing thresholds associated with specific health outcomes is needed. Reformulation or development of products that maximize the number of pregnant women receiving enough (but not too much) vitamin A, vitamin D, folic acid, calcium, iron, and ω-3 FAs is needed.
The authors thank their ECHO colleagues; the medical, nursing, and program staff; and the children and families participating in the ECHO cohorts. The authors also acknowledge the contribution of the following ECHO Program collaborators: ECHO Components—Coordinating Center: Smith PB, Newby KL, and Benjamin DK from Duke Clinical Research Institute, Durham, North Carolina; Data Analysis Center: Jacobson LP from Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland; Parker CB and Catellier DJ from Research Triangle Institute, Durham, North Carolina.
Appendix A. Supplementary dataAdditional file 1: Appendix A. (DOCX 78 MB)
Author Contribution
The authors’ responsibilities were as follows–
KMS, KL, JMK, DD, TGO, and SCLD: designed cohort-level research;
KAS, CWH, KMS, KL, JMK, DD, LEM, TGO, and SCLD: conducted research;
KAS, GLC, RLB, and DJC: designed the pooled research question and analysis;
KAS, GLC, and DJC: conducted the pooled analysis;
KAS and DJC: wrote the article;
KAS: had primary responsibility for final content;
and all authors: read and approved the final manuscript.
Conflict Of Intrest
RLB has served as a consultant in the past to the NIH Office of Dietary Supplements, Nestlé, the General Mills Bell Institute, RTI International, and Nutrition Impact; is a trustee of the International Food Information Council; is a former board member of International Life Sciences Institute–North America; is a member of Schiff Scientific Advisory Board; and in the past has received travel support to present her research on dietary supplements. Dr. Switkowski is a paid consultant of prenatal nutrition to Modern Fertility. All other authors report no conflicts of interest.
Funding
Research reported in this publication was supported by the Environmental influences on Child Health Outcomes Program, Office of the Director, NIH, under award numbers U2COD023375 (Coordinating Center); U24OD023382 (Data Analysis Center); UG3/UH3OD023248 (to KAS, DD, and DHG); UG3/UH3OD023279 (to CWH); R01HD-034568, R01HD096032, and UG3/UH3OD023286 (to KMS); UG3/UH3OD023342 and R01ES016443 (to KL); UG3/UH3OD023285 (to JMK); UG3/UH3OD023287 (to LEM); UG3/UH3OD023349 (to TGOC); and UG3/UH3OD23313 (to SCLD) and by Autism Speaks under award number AS5938 (to KL).
The sponsors had no role in in the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the report for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
References:
MRC Vitamin Study Research Group
Prevention of neural tube defects:
results of the Medical Research Council Vitamin Study.
Lancet. 1991; 338: 131-137Clagett-Dame M. DeLuca H.F.
The role of vitamin A in mammalian reproduction and embryonic development.
Annu Rev Nutr. 2002; 22: 347-381Prado E.L. Dewey K.G.
Nutrition and brain development in early life.
Nutr Rev. 2014; 72: 267-284Korsmo H.W. Jiang X. Caudill M.A.
Choline: exploring the growing science on its benefits for moms and babies.
Nutrients. 2019; 11: 1823Waterland R.A. Dolinoy D.C. Lin J.R. Smith C.A. Shi X. Tahiliani K.G.
Maternal methyl supplements increase offspring DNA methylation at Axin fused.
Genesis. 2006; 44: 401-406
Szeto I.M. Aziz A. Das P.J. Taha A.Y. Okubo N. Reza-Lopez S. et al.
High multivitamin intake by Wistar rats during pregnancy results in increased
food intake and components of the metabolic syndrome in male offspring.
Am J Physiol Regul Integr Comp Physiol. 2008; 295: R575-R582Dominguez-Salas P. Moore S.E. Baker M.S. Bergen A.W. Cox S.E. Dyer R.A. et al.
Maternal nutrition at conception modulates DNA methylation
of human metastable epialleles.
Nat Commun. 2014; 5: 3746Caffrey A. Irwin R.E. McNulty H. Strain J.J. Lees-Murdock D.J. McNulty B.A. et al.
Gene-specific DNA methylation in newborns in response to folic acid
supplementation during the second and third trimesters of pregnancy:
epigenetic analysis from a randomized controlled trial.
Am J Clin Nutr. 2018; 107: 566-575Bailey R.L. Pac S.G. Fulgoni III, V.L. Reidy K.C. Catalano P.M.
Estimation of total usual dietary intakes of pregnant women in the United States.
JAMA Netw Open. 2019; 2e195967Sauder K.A. Harte R.N. Ringham B.M. Guenther P.M. Bailey R.L. Alshawabkeh A. et al.
Disparities in risks of inadequate and excessive intake
of micronutrients during pregnancy.
J Nutr. 2021; 151: 3555-3569McCauley M.E. van den Broek N. Dou L. Othman M.
Vitamin A supplementation during pregnancy for maternal and newborn outcomes.
Cochrane Database Syst Rev. 2015; (2015): CD008666Palacios C. Kostiuk L.K. Peńa-Rosas J.P.
Vitamin D supplementation for women during pregnancy.
Cochrane Database Syst Rev. 2019; 7: CD008873De-Regil L.M. Peńa-Rosas J.P. Fernández-Gaxiola A.C. Rayco-Solon P.
Effects and safety of periconceptional oral folate
supplementation for preventing birth defects.
Cochrane Database Syst Rev. 2015; (2015): CD007950Keats E.C. Haider B.A. Tam E. Bhutta Z.A.
Multiple-micronutrient supplementation for women during pregnancy.
Cochrane Database Syst Rev. 2019; 3: CD004905Hofmeyr G.J. Manyame S. Medley N. Williams M.J.
Calcium supplementation commencing before or early in pregnancy,
for preventing hypertensive disorders of pregnancy.
Cochrane Database Syst Rev. 2019; 9: CD011192Buppasiri P. Lumbiganon P. Thinkhamrop J. Ngamjarus C. Laopaiboon M. Medley N.
Calcium supplementation (other than for preventing or treating hypertension)
for improving pregnancy and infant outcomes.
Cochrane Database Syst Rev. 2015; (2015): CD007079Middleton P. Gomersall J.C. Gould J.F. Shepherd E. Olsen S.F. Makrides M.
Omega-3 fatty acid addition during pregnancy.
Cochrane Database Syst Rev. 2018; 11: CD003402Gillman M.W. Blaisdell C.J.
Environmental influences on child health outcomes,
a research program of the National Institutes of Health.
Curr Opin Pediatr. 2018; 30: 260-262U.S. Department of Agriculture, Agricultural Research Service,
USDA Food and Nutrient Database for Dietary Studies 2019–2020.
2022 (Food Surveys Research Group Home Page)
http://www.ars.usda.gov/nea/bhnrc/fsrgSubar A.F. Kirkpatrick S.I. Mittl B. Zimmerman T.P. Thompson F.E. Bingley C. et al.
The automated self-administered 24-hour dietary recall (ASA24):
a resource for researchers, clinicians, and educators
from the National Cancer Institute.
J Acad Nutr Diet. 2012; 112: 1134-1137Institute of Medicine
Dietary reference intakes: the essential guide to nutrient requirements.
The National Academies Press, Washington, D.C.2006Murphy S.P. Guenther P.M. Kretsch M.J.
Using the dietary reference intakes to assess intakes of groups: pitfalls to avoid.
J Am Diet Assoc. 2006; 106: 1550-1553103D Congress (Public Law 103–417)
Dietary Supplement Health and Education Act of 1994.Saldanha L.G. Dwyer J.T. Andrews K.W. Brown L.L. Costello R.B. Ershow A.G. et al.
Is nutrient content and other label information for prescription
prenatal supplements different from nonprescription products?
J Acad Nutr Diet. 2017; 117: 1429-1436Dwyer J.T. Bailen R.A. Saldanha L.G. Gahche J.J. Costello R.B. Betz J.M. et al.
The dietary supplement label database: recent developments and applications.
J Nutr. 2018; 148 (35S): 1428SSaldanha L.G. Dwyer J.T. Bailen R.A. Andrews K.W. Betz J.W. Chang H.F. et al.
Characteristics and challenges of dietary supplement databases
derived from label information.
J Nutr. 2018; 148 (7S): 1422SUS Department of Health and Human Services,
National Institutes of Health, Office of Dietary Supplements.
Dietary Supplement Label Database (DSLD). [Internet].
[cited December 13, 2022]. Available from:
https://dsld.nlm.nih.gov/dsld/US Department of Health and Human Services
Food and Drug Administration, Center for Food Safety and Applied Nutrition.
Converting units of measure for folate, niacin, and vitamins A, D,
and E on the nutrition and supplement facts labels: guidance for industry.
Food and Drug Administration,
College Park, Maryland2019Kipnis V. Midthune D. Buckman D.W. Dodd K.W. Guenther P.M. Krebs-Smith S.M. et al.
Modeling data with excess zeros and measurement error:
application to evaluating relationships between
episodically consumed foods and health outcomes.
Biometrics. 2009; 65: 1003-1010Thompson F.E. Kirkpatrick S.I. Subar A.F. Reedy J. Schap T.E. Wilson M.M. et al.
The National Cancer Institute’s dietary assessment primer:
a resource for diet research.
J Acad Nutr Diet. 2015; 115: 1986-1995Luo H. Dodd K.W. Arnold C.D. Engle-Stone R.
A new statistical method for estimating usual intakes of nearly-daily
consumed foods and nutrients through use of only one 24-hour dietary recall.
J Nutr. 2019; 149: 1667-1673Life-Strip: The Best, Most Comprehensive Nutrition System [Internet].
Shaklee [cited December 13, 2022].
https://us.shaklee.com/Nutrition/Essential-
Nutrition/Multivitamins/Life-Strip%C2%AE/p/21294.GNC Women’s Multivitamin Prenatal Formula
with DHA & Iron [Internet]. GNC [cited December 13, 2022].
https://www.gnc.com/prenatal/286721.html.Carlson Labs–, Women’s Omega Multi–60 Softgels
Formerly Right 1 Daily [Internet]. Carlson Labs [cited April 25, 2022].
https://www.walmart.com/ip/Carlson-Labs-Women-s-Omega-Multi-
60-Softgels-Formerly-Right-1-Daily/44161932.Dubois L. Diasparra M. Bédard B. Colapinto C.K. Fontaine-Bisson B. Morisset A.S. et al.
Adequacy of nutritional intake from food and supplements in a cohort
of pregnant women in Quebec, Canada: the 3D cohort study
(Design, Develop, Discover).
Am J Clin Nutr. 2017; 106: 541-548Brunst K.J. Wright R.O. DiGioia K. Enlow M.B. Fernandez H. Wright R.J. et al.
Racial/ethnic and sociodemographic factors associated with micronutrient
intakes and inadequacies among pregnant women in an urban US population.
Public Health Nutr. 2014; 17: 1960-1970Adams J.B. Kirby J.K. Sorensen J.C. Pollard E.L. Audhya T.
Evidence based recommendations for an optimal prenatal supplement
for women in the US: vitamins and related nutrients.
Matern Health Neonatol Perinatol. 2022; 8: 4Adams J.B. Sorenson J.C. Pollard E.L. Kirby J.K. Audhya T.
Evidence-based recommendations for an optimal prenatal
supplement for women in the U.S., Part two: minerals.
Nutrients. 2021; 13: 1849Lamers Y. MacFarlane A.J. O’Connor D.L. Fontaine-Bisson B.
Periconceptional intake of folic acid among low-risk women in Canada:
summary of a workshop aiming to align prenatal folic acid
supplement composition with current expert guidelines.
Am J Clin Nutr. 2018; 108: 1357-1368Nutrition During Pregnancy [Internet]
(American College of Obstetricians and Gynecologists [cited June 7, 2022])
https://www.acog.org/womens-health/faqs/nutrition-during-pregnancyInstitute of Medicine
Food and Nutrition Board, Subcommittee on Interpretation
and Uses of Dietary Reference Intakes.
in: Standing Committee on the Scientific Evaluation of Dietary Reference Intakes.
DRI Dietary Reference Intakes: Applications in Dietary Assessment.
The National Academies Press, Washington, D.C.2000Jun S. Gahche J.J. Potischman N. Dwyer J.T. Guenther P.M. Sauder K.A. et al.
Dietary supplement use and its micronutrient contribution
during pregnancy and lactation in the United States.
Obstet Gynecol. 2020; 135: 623-633American College of Obstetricians and Gynecologists
Practice Bulletin No. 187: neural tube defects.
Obstet Gynecol. 2017; 130: e279-e290Lucas C. Charlton K.E. Yeatman H.
Nutrition advice during pregnancy:
do women receive it and can health professionals provide it?
Matern Child Health J. 2014; 18: 2465-2478Hurrell R. Egli I.
Iron bioavailability and dietary reference values.
Am J Clin Nutr. 2010; 91 (–7S): 1461STolkien Z. Stecher L. Mander A.P. Pereira D.I. Powell J.J.
Ferrous sulfate supplementation causes significant gastrointestinal
side-effects in adults: a systematic review and meta-analysis.
PLOS ONE. 2015; 10e0117383Trumbo P. Schlicker S. Yates A.A. Poos M.
Food, Nutrition Board of the Institute of Medicine, The National Academies.
Dietary reference intakes for energy, carbohydrate, fiber,
fat, fatty acids, cholesterol, protein and amino acids.
J Am Diet Assoc. 2002; 102: 1621-1630Kris-Etherton P.M. Grieger J.A. Etherton T.D.
Dietary reference intakes for DHA and EPA.
Prostaglandins Leukot Essent Fatty Acids. 2009; 81: 99-104Diet, Nutrition and the Prevention of Chronic Diseases
World Health Organization, Geneva, Switzerland 003Simopoulos A.P. Leaf A. Salem Jr., N.
Workshop statement on the essentiality of and recommended
dietary intakes for Omega-6 and Omega-3 fatty acids.
Prostaglandins Leukot Essent Fatty Acids. 2000; 63: 119-121Zhang Z. Fulgoni V.L. Kris-Etherton P.M. Mitmesser S.H.
Dietary intakes of EPA and DHA omega-3 fatty acids among US childbearing-age
and pregnant women: an analysis of NHANES 2001-2014.
Nutrients. 2018; 10: 416Subar A.F. Freedman L.S. Tooze J.A. Kirkpatrick S.I. Boushey C. Neuhouser M.L. et al.
Addressing current criticism regarding the value
of self-report dietary data.
J Nutr. 2015; 145: 2639-2645Center for Food Safety and Applied Nutrition
Guidance for Industry:
Guide for Developing and Using Data Bases for Nutrition Labeling.
([Internet]) Food and Drug Administration,
Washington, D.C 1998
https://www.fda.gov/regulatory-information/search-fda-guidance-documents/
guidance-industry-guide-developing-and-using-data-bases-nutrition-labeling
Return to SHAKLEE STUDIES
Since 4-21-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |