

Do Sports Drinks Cause Kidney Stones?
This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Urological Research 2009 (Feb); 37 (1): 41–46 ~ FULL TEXT
Jeffrey W. Goodman · John R. Asplin · David S. Goldfarb
NYU School of Medicine,
New York, NY 10010, USA.
Why was this study done?
To investigate the effects of two sports drinks (“G” or “P”) and whether they produce or prevent the formation of kidney stones.
What This Study Found
“P” increased citrate excretion (by 170 mg/day) and increased urine pH (by 0.31), whereas “G” did not change citrate excretion or pH. These findings suggest that “P” may help prevent the formation of kidney stones.The Abstract
Effect of Two Sports Drinks on Urinary Lithogenicity
The effect of commercial oral rehydration solutions ("sports drinks") relative to water on risk of nephrolithiasis has not been studied previously. We studied the effect of two sports drinks, Performance (Shaklee Corp., Pleasanton, CA, USA) and Gatorade (Gatorade, Chicago, IL, USA) on urinary chemistry and measures of lithogenicity in non-stone formers.
Performance has a pH of 4.3, and contains21 mmol/L of sodium,
5.3 mmol/L of potassium,
0.8 mmol/L of calcium, and
19.5 mmol/L of citrate.Gatorade pH ranges from 2.9 to 3.2, and contains
20 mmol/L of sodium,
3.2 mmol/L of potassium,
negligible calcium, and
13.9 mmol/L of citrate.Subjects drank 946 ml (32 oz) of tap water daily for 3 days, and recorded diet history. This was followed by a second 3-day experimental period during which subjects drank 946 ml (32 oz) of sports drink daily, duplicating diets from part 1. In each 3-day period, urine was collected for 24 h during days 2 and 3.
Urine chemical analysis was performed, and supersaturations of calcium oxalate, calcium phosphate and uric acid were calculated. Nine subjects completed the study using Performance, ten used Gatorade. Urine volumes and creatinine excretions were not different during the control and experimental periods.
Performance increased mean citrate excretion by 170 mg/day (95% CI 57-284 mg/day; P = 0.01) and increased urine pH by 0.31 (95% CI 0.03-0.59; P = 0.03).
Gatorade did not significantly change urinary citrate excretion or pH. Neither drink caused significant differences in the excretion of sodium and calcium or any supersaturation value.
Ingestion of Performance, but not Gatorade, led to an increase in mean urinary citrate excretion and pH as compared to water. The increase in citrate is likely to be a clinically significant effect. pH is an important determinant of alkali load in beverages containing organic anions.
Performance, with more citrate and a higher pH than Gatorade, could represent a superior alternative to water for reducing urinary lithogenicity. Most sports drinks with significant carbohydrate content however may contain too many calories, and fructose, to be preferred beverages for stone prevention.
Keywords Beverages · Calculi, renal · Citrate · Diet · Fructose · Kidney stones · Oxalate · Rehydration solutions · Urolithiasis
From the FULL TEXT Article:
Introduction
An increase in urine volume in response to an increase in the oral intake of fluids is a well-recognized method of reducing the prevalence of recurrent kidney stones. [1, 2] Increasing fluid intake has been shown to be effective in a single randomized, controlled trial. [3] Although the optimal urine volume has not been determined in clinical trials, an often cited goal is to increase urine volume to more than 2 L/day. [4] However, in practice, the results of physician efforts to increase urine volume are at best modest, amounting to a mean increase of only 0.3 L/day in one study of 2,877 patients in 14 stone-oriented practices. [5]
Each patient’s individual preferences and perceptions of palatabililty for various beverages is presumably a factor in determining whether urine volume can successfully be increased. Patients often inquire as to the risk or benefit that would be associated with increasing intake of specific beverages. In recent years, “sports drinks”, beverages which were historically formulated as oral rehydration solutions containing both sodium and glucose to take advantage of intestinal sodium–glucose co-transport, have grown in popularity and availability.
In fact, in recent years sales of soda in the United States have fallen for the first time while sports drinks and energy drinks continue to grow more than 10% per year. [6] Previous epidemiologic surveys of associations of specific beverages with stone prevalence predated the popularity of sports drinks and did not include them as a distinct category. [7] We sought to determine if sports drinks would decrease urinary lithogenicity for calcium and uric acid stones due to their citrate content, or worsen it given their sodium and carbohydrate content.
Materials and methods
Subjects and study design
Sixteen healthy volunteers between 25 and 55 years of age with no history of kidney stones participated in a protocol to compare the effect of two sports drinks on urinary lithogenicity with that of water. Four participants were in both arms, six were only in the Gatorade arm and six were only in the Performance arm. We specifically excluded patients with a history of metabolic bone disease, hyperparathyroidism, chronic kidney disease, or diabetes.
The subjects provided informed consent regarding study participation. The study was reviewed and approved by the local institutional review board. Subjects were receiving no medications and were specifically asked not to ingest any multivitamins or calcium supplements during the study period.
During the control period each subject drank 946 mL (1 quart) of tap water daily for 3 days in addition to their usual fluid intake. Other than the water ingestion the subjects ate their regular unrestricted ad lib diets and ingested fluids freely, keeping a diary of all foods and beverages. Urine was collected for 24 h during the second and third days of the 3-day control period. During urine collections the urine was maintained at room temperature. An antimicrobial preservative and a volume marker were added to each urine container. At the end of the 24 h collection, the urine collection container was shaken and a 50 mL aliquot was obtained and sent by overnight mail to Litholink Corp. (Chicago, IL) for analysis.
After a 1 week washout period the subjects began the 3- day experimental period during which they drank 946 mL (1 quart) of sports drink daily. Other than the sports drink ingestion the subjects ate the same regular diet and ingested the same fluids as during the control period, duplicating the previously made diary entries. Urine was again collected for 24 h for the second and third days of the 3-day experimental period.
We used two sports drinks easily available: Performance (Shaklee Corporation, Pleasanton, CA) and Gatorade Thirst Quencher Original (Gatorade, Chicago, IL). Either lemon-lime flavor or orange flavor Performance and Gatorade was used based on the personal preference of the participants. Performance is sold by local, individual distributors who can be found and contacted via the internet. It is supplied as a powdered concentrate and was weighed out by the investigators and mixed with tap water to constitute 1 L according to the manufacturer’s instructions by the participants. Gatorade was purchased in local grocery stores. Some participants completed both protocols with at least one week between sports drinks. The study was not and could not be blinded. Results of individuals in whom 24 h excretion of creatinine varied between collections by 30% or more were judged to have been inaccurately collected and were excluded. Neither manufacturer was involved in the funding, design, conduct or reporting of the study.
Urine chemistry studies
In each 24 h urine sample we measured calcium, chloride, creatinine, magnesium, sodium, potassium, phosphate, ammonium and uric acid concentrations by standard laboratory technique using a Beckman Synchron CX5 (Beckman Instruments, Brea, CA, USA). [8] pH was measured by glass electrode. Oxalate was measured by enzyme assay using oxalate oxidase (Trinity Biotech, Bray, Ireland). Citrate was measured by enzyme assay using citrate lyase (Mannheim Bohringer, Mannheim, Germany). From these analyses we calculated supersaturation (SS) with respect to calcium oxalate, calcium phosphate and uric acid using the iterative computer program EQUIL 2. [9] For each of the 3-day experimental phases the mean values of the two 24 h collections were reported.
Statistics
Urine values obtained during the experimental and control periods were compared by paired Student t test and considered statistically different at P < 0.05. Statistical data were generated and analyzed with a commercially available software package, Systat (Point Richmond, CA, USA). Results were expressed as mean ± SD.
Results

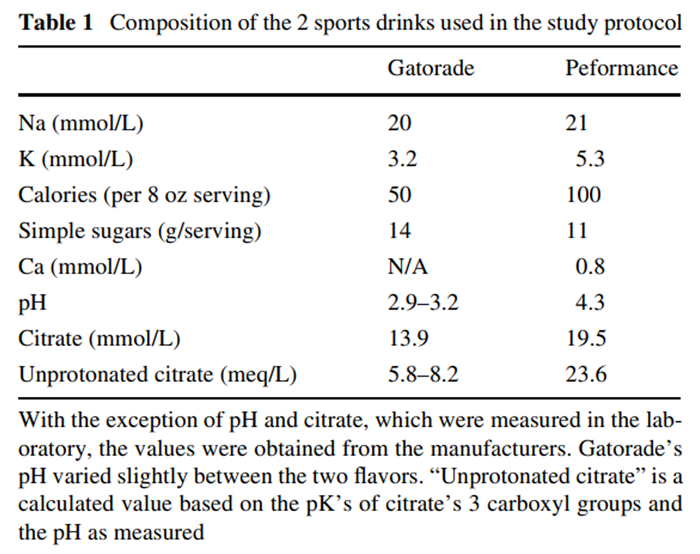
Table 1 The composition of the two sports drinks is given in Table 1. With the exception of pH and citrate which were measured in the laboratory, the values were obtained from the manufacturers. “Unprotonated citrate” is a calculated value based on the pKs of citrate’s 3 carboxyl groups and the pH as measured. It is a measure of the content of carboxyls associated with cations other than protons (e.g. sodium, potassium) and therefore represents potential base. Performance contained more citrate and had a significantly higher pH than Gatorade. Performance, which contains maltodextrin, had more calories per serving, though fewer grams of simple sugars. Neither had a significant calcium content. The contents of the two drinks for sodium and potassium were similar.
One subject did not successfully adhere to the study protocol as judged by a difference in creatinine excretion of more than 30% in consecutive periods, and that individual’s results were not included in the analysis. Of the fifteen remaining subjects, nine completed the protocol using Performance, and ten completed the protocol using Gatorade. There were no adverse events during the study periods.

Figure 1
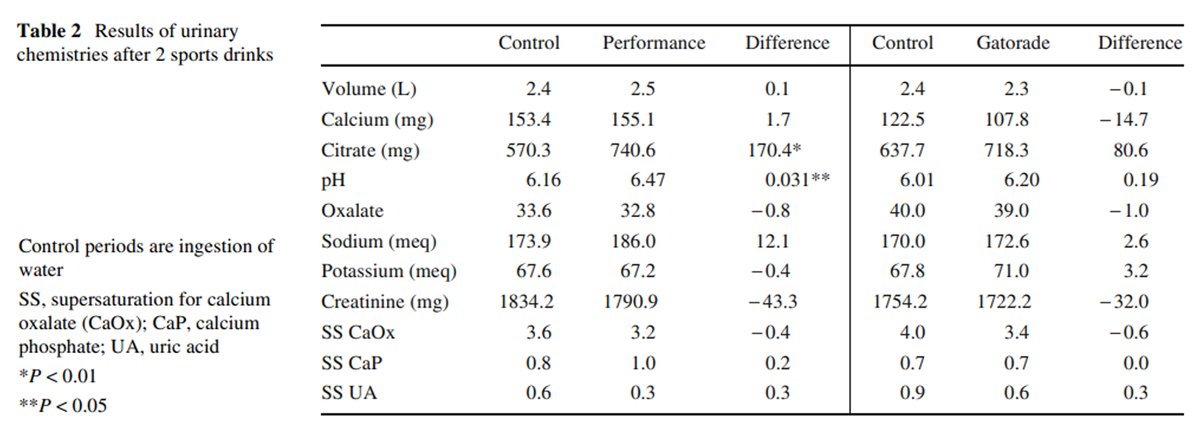
Table 2 There were two significant differences in urinary chemistry caused by Performance but not by Gatorade. Performance increased mean 24 h pH from 6.16 in the control period to 6.47 (P < 0.05) in the sports drink period, while Gatorade increased pH from 6.01 to 6.20 (P = NS). Performance also caused a significant increase in urinary citrate excretion from 570 to 741 mg/day (95% CI 57–284 mg/day; P = 0.003) while Gatorade caused an increase in citrate from 634 to 718 mg/day, which was not statistically significant. Figure 1 demonstrates that 8 of 9 individuals in the Performance arm had an increase in urinary citrate excretion, while only 5 of 10 had an increase with Gatorade.
There were no associated significant changes in sodium excretion with either drink. Performance was associated with a non-significant increase in Na excretion of 12.1 ± 49.4 meq/day while Gatorade also caused a non-significant change of 2.6 ± 44.3 meq/day. Similarly, urinary calcium excretion did not significantly increase with either beverage, rising 1.7 ± 44.4 mg/day with Performance and 14.7 ± 32.7 mg/day with Gatorade (both P = NS). Neither drink caused changes in urinary oxalate or potassium excretion (Table 2) or in magnesium or phosphate excretion (data not shown).
The net result was that neither drink was associated with a statistically significant decrease in urinary supersaturation for calcium oxalate, which was 3.6 in the control period and 3.2 with Performance and 4.0 in the control period and 3.4 with Gatorade. There were no changes in uric acid excretion with either sports drink. Despite the changes in urine pH, neither drink significantly lowered supersaturation for uric acid.
The protocol, using a diet diary to replicate the patients’ ad lib diets during collection periods was successful in controlling for other variables, as urine volumes, and excretion of potassium and oxalate were nearly identical with water versus Performance and Gatorade. The patients also performed the collections accurately, as evidenced by very similar 24 h excretion rates of creatinine (1,834.2 mg/day in the control period vs. 1,790.9 mg/day during the Performance period; 1,754.2 mg/day in the control period vs. 1,722.2 mg/day during the Gatorade period).
Discussion
Ingestion of sports drinks has been increasing in recent years, gaining a larger share of the beverage market. Their contribution to stone formation, whether to increase or decrease incidence, has not been assessed either by investigating their effects on urine chemistry or by assessing their epidemiologic association with stone formation. Based on their composition, effects to both increase and to decrease urine lithogenicity could be expected. The content of citrate would be expected to increase urine citrate excretion and urine pH, providing protection against both calcium and uric acid stones. However, the sodium content of sports drinks, promoted as useful for “rehydration” in athletes, might be associated with increases in urine calcium excretion. In addition, ingestion of significant amounts of simple carbohydrates such as sucrose in these drinks could also be associated with increases in calcium excretion. [10]
Finally, fructose content of sodas and juices has been implicated in increasing risk for stones. [11] While an explanation of this association is not yet available, fructose may cause hyperuricemia (and metabolic syndrome) [12] and nephrocalcinosis. [13] Effects on urine calcium and oxalate excretion may also occur. [11] While some of these effects would not be observed immediately, we thought it worthwhile to examine the acute effects of sports drinks on urine chemistry.
We found that both sports drinks studied led to increases in urine citrate and pH though these effects were statistically significant only for Performance and not for Gatorade. The effect of beverage ingestion on urine citrate excretion and pH depends on the amount of potential base contained in the drink, which in turn is dependent on the beverage’s pH and organic anion concentration. Citric acid, i.e. protonated citrate, will have no net effect on urine pH or citrate excretion. The citrate may be metabolized to bicarbonate by the liver and kidney, but the accompanying proton will neutralize the resultant bicarbonate. Only minimal changes in urine pH or citrate excretion would be expected, the result of intestinal citrate absorption leading to a higher filtered load.
At a higher beverage pH, more citrate has its negative charge balanced by potassium or sodium, in which case there will not be a proton to neutralize the effect of ingested citrate to either increase urine pH and, indirectly, citrate excretion (due to its hepatic and renal metabolism to bicarbonate). Measurement of citrate content without reference to beverage pH is therefore not sufficient to explain effects on urine pH and citrate excretion. The higher pH of orange juice compared to lemonade was thought responsible for the effect of the former to increase urine citrate and pH while lemonade had no effect. [14] Since the pH of Performance was about 1 unit greater than that of Gatorade, its effect is attributable not only to greater citrate content but to its greater content of potential base as well.
Despite the possible superiority of orange juice, lemon juice has been a popular liquid widely recommended for stone prevention due to its effect to increase urinary citrate excretion. [15] Other studies have suggested possible efficacy of lemon juice in stone prevention as well. [16, 17] The original protocol by Seltzer et al. entailed daily ingestion, by calcium stone formers with hypocitraturia, of 120 mL of lemon juice concentrate with water added to total 2 L. The increase in urinary citrate excretion seen here with 1 L/day of Performance was only 34 mg less than the increase seen in Seltzer’s study.
The change in urine pH, greater for Performance than for Gatorade, might have been associated with a clinically important decrease in supersaturation for uric acid if pH had been low, as it typically is in uric acid stone formers. [18] Instead, in these non-stone forming participants, pH started at about 6.1, and uric acid supersaturation was significantly below 1 at 0.58 so that the increase in pH caused a non-statistically significant decrease in supersaturation to 0.31. If uric acid stone formers had been studied, one might expect a clinically important effect of increased pH to decrease uric acid supersaturation.
Although the sports drink periods would have been associated with an increase in oral intake of sodium of 20 or 21 meq/day, there was enough urinary sodium in these study participants following their ad lib diets so that the effect of the sports drinks to change urine sodium excretion was not detected. Although increases in dietary sodium are associated with increases in urinary calcium excretion [19], this effect was also not detected. The small increase in sodium ingested might also not be sufficient to measurably increase urinary calcium excretion in hypercalciuric stone formers. Gatorade has recently marketed a formulation called Endurance which doubles the usual sodium content to 40 meq/L, which might have a measurable effect on urine calcium excretion.
The cost of using sports drinks to increase urinary citrate excretion is not less than that for prescription of potassium citrate tablets. The cost of 20 meq of citrate is as little as $0.31 to the Department of Veterans Affairs (New York, NY) for generic tablets; $0.40 for crystals; or as high as $2.20 for generic tabs; $2.32 for brand Urocit K (Mission Pharmacal, San Antonio, TX) at a Duane Reade (private) pharmacy in Manhattan (costs as of April, 2008). Performance costs $12.95 for a canister from an independent vendor so that 20 meq of citrate costs $2.72. The advantage of Performance is that unlike oral tablets, the sports drink will also increase urine volume and, due to the popularity of these drinks, possibly improve compliance.
Performance is not a perfect citrate supplement since as constituted it contains 400 calories/L. Its use as a preventive regimen for recurrent stones therefore cannot be considered the ideal choice for most patients. Given recent well demonstrated links between obesity, diabetes and stone formation, the prescription of this relatively caloric liquid may not be desirable for many stone formers. [20-22] Although the increase in urine pH could prevent uric acid stones, patients with uric acid stones too have an increased rate of diabetes and features of metabolic syndrome. [23] Fructose, a component of corn syrup, a frequent sweetener added to sports drinks and sodas, would also be an undesirable way for most stone formers to increase urine volume given its recent links to hyperuricemia, metabolic syndrome and stones. [11, 12] If the carbohydrate content of sports drinks could be addressed, their relative palatability and popularity of late may make them preferable to water for some patients.
Acknowledgments
This work was supported in part by NIH grant 2R44DK59086-02 and by the Dept. of Veterans Affairs. We appreciate the administrative support of Frank Modersitzki.
References:
Siener R, Hesse A (2003)
Fluid intake and epidemiology of urolithiasis.
Eur J Clin Nutr 57(suppl 2):S47–S51Borghi L, Meschi T, Schianchi T et al (1999)
Urine volume: stone risk factor and preventive measure.
Nephron 81(suppl 1):31–37.Borghi L, Meschi T, Amato F et al (1996)
Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study.
J Urol 155:839–843.Goldfarb DS, Coe FL (1999)
Prevention of recurrent nephrolithiasis.
Am Fam Physician 60:2269–2276Parks JH, GoldWscher ER, Coe FL (2003)
Changes in urine volume accomplished by physicians treating nephrolithiasis.
J Urol 169:863–866.Warner M (2006)
Soda sales fall for Wrst time in 20 years.
New York TimesCurhan GC, Willett WC, Rimm EB et al (1996)
Prospective study of beverage use and the risk of kidney stones.
Am J Epidemiol 143:240–247Asplin J, Parks J, Lingeman J et al (1998)
Supersaturation and stone composition in a network of dispersed treatment sites.
J Urol 159:1821–1825.Finlayson B (1977)
Calcium stones: some physical and clinical aspects.
In: David DS (ed) Calcium metabolism in renal failure and nephrolithiasis.
Wiley, New York, pp 337–382Lemann J Jr, Piering WF, Lennon EJ (1969)
Possible role of carbohydrate-induced calciuria in calcium oxalate kidney-stone formation.
N Engl J Med 280:232–237Taylor EN, Curhan GC (2008)
Fructose consumption and the risk of kidney stones.
Kidney Int 73:207–212.Nakagawa T, Hu H, Zharikov S et al (2006)
A causal role for uric acid in fructose-induced metabolic syndrome.
Am J Physiol Renal Physiol 290:F625–F631.Asselman M, Verkoelen CF (2008)
Fructose intake as a risk factor for kidney stone disease.
Kidney Int 73:139–140.Odvina CV (2006)
Comparative value of orange juice versus lemonade in reducing stone-forming risk.
Clin J Am Soc Nephrol 1:1269–1274.Seltzer MA, Low RK, McDonald M et al (1996)
Dietary manipulation with lemonade to treat hypocitraturic calcium nephrolithiasis.
J Urol 156:907–909Kang DE, Sur RL, Haleblian GE et al (2007)
Long-term lemonade based dietary manipulation in patients with hypocitraturic nephrolithiasis.
J Urol 177:1358–1362Penniston KL, Steele TH, Nakada SY (2007)
Lemonade therapy increases urinary citrate and urine volumes in
patients with recurrent calcium oxalate stone formation.
Urology 70:856–860.Asplin JR (1996)
Uric acid stones.
Semin Nephrol 16:412–424Phillips MJ, Cooke JN (1967)
Relation between urinary calcium and sodium in patients with idiopathic hypercalciuria.
Lancet 1:1354–1357.Abate N, Chandalia M, Cabo-Chan AV Jr et al (2004)
The metabolic syndrome and uric acid nephrolithiasis:
novel features of renal manifestation of insulin resistance.
Kidney Int 65:386–392.Taylor EN, Stampfer MJ, Curhan GC (2005)
Obesity, weight gain,and the risk of kidney stones.
JAMA 293:455–462.Taylor EN, Stampfer MJ, Curhan GC (2005)
Diabetes mellitus and the risk of nephrolithiasis.
Kidney Int 68:1230–1235Cameron MA, Maalouf NM, Adams-Huet B et al (2006)
Urine composition in type 2 diabetes: predisposition to uric acid nephrolithiasis.
J Am Soc Nephrol 17:1422–1428.
Return to SHAKLEE STUDIES
Since 11-06-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |