

Adverse Events Due to Chiropractic and Other
Manual Therapies for Infants and Children:
A Review of the LiteratureThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther. 2015 (Nov); 38 (9): 699–712 ~ FULL TEXT
Angela J. Todd, MS • Matthew T. Carroll, PhD • Anske Robinson, PhD,
Eleanor K.L. Mitchell, PhD
Department of Rural and Indigenous Health,
Faculty of Medicine, Nursing and Health Sciences,
School Of Rural Health,
Moe, Victoria, Australia.OBJECTIVE: The purpose of this study was to review the literature for cases of adverse events in infants and children treated by chiropractors or other manual therapists, identifying treatment type and if a preexisting pathology was present.
METHOD: English language, peer-reviewed journals and non-peer-reviewed case reports discussing adverse events (ranging from minor to serious) were systematically searched from inception of the relevant searchable bibliographic databases through March 2014. Articles not referring to infants or children were excluded.
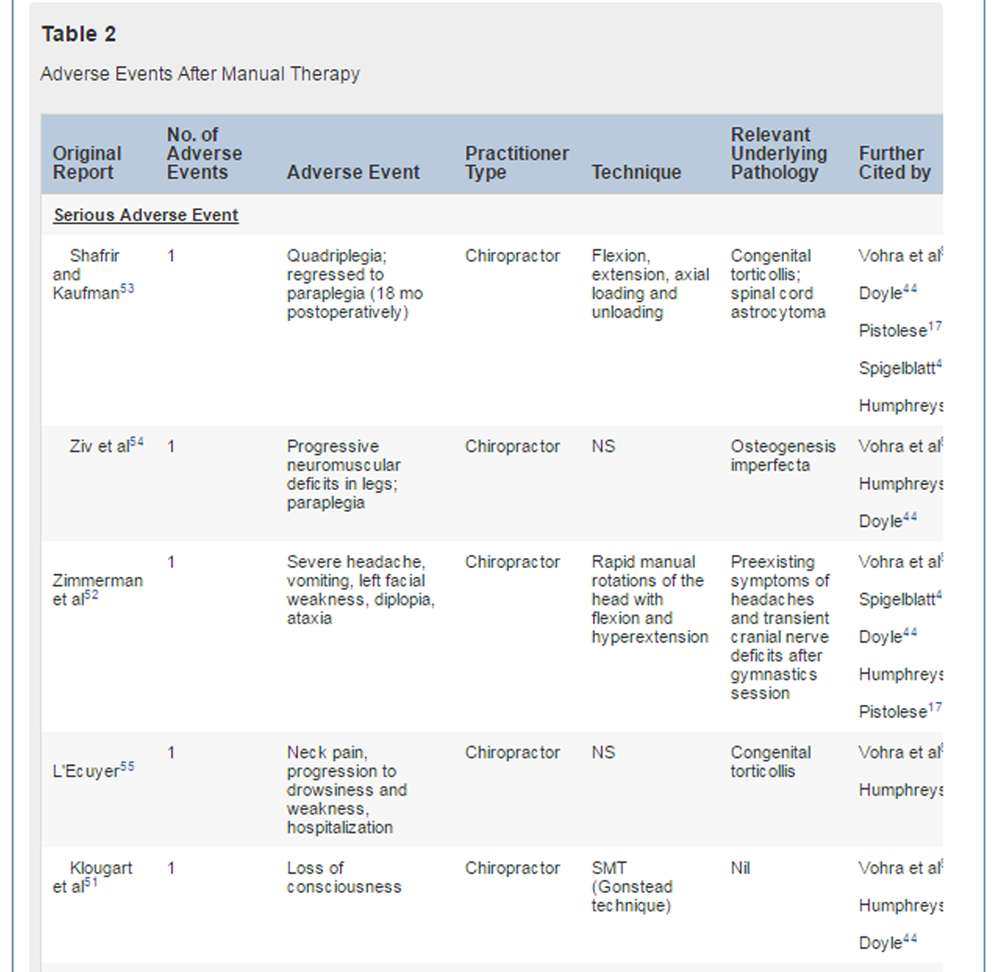
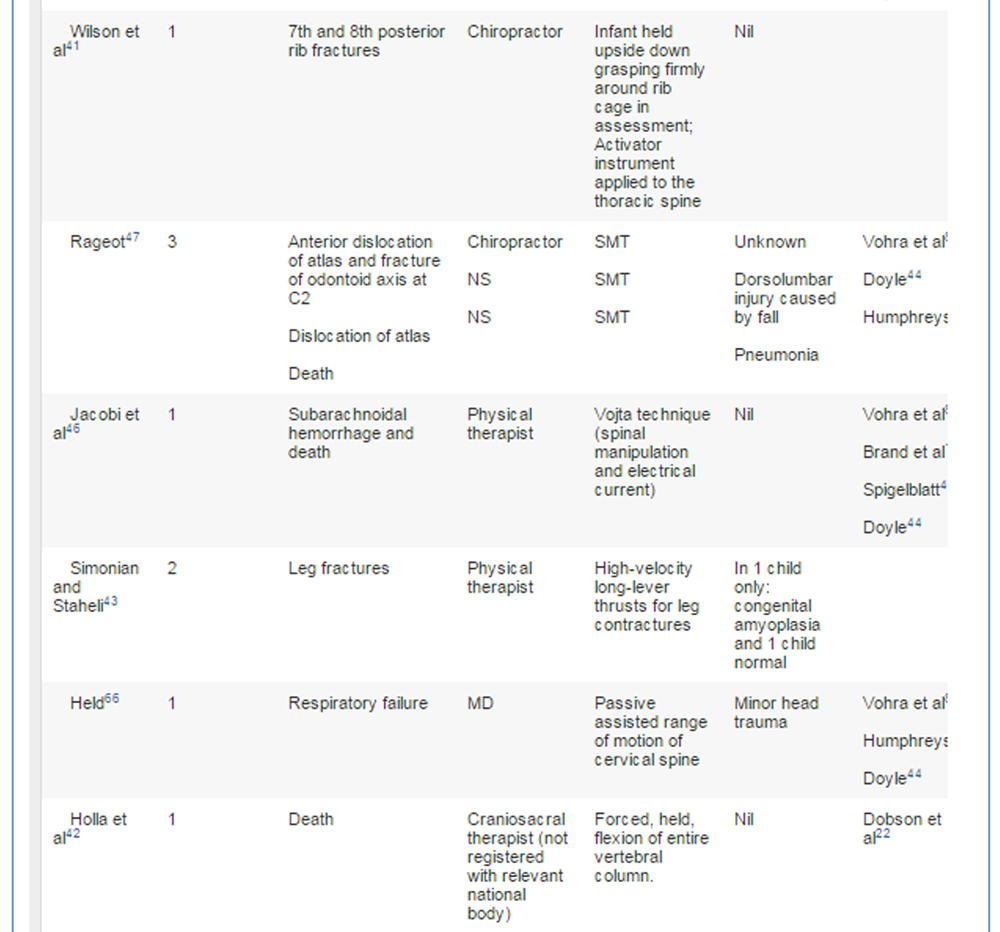
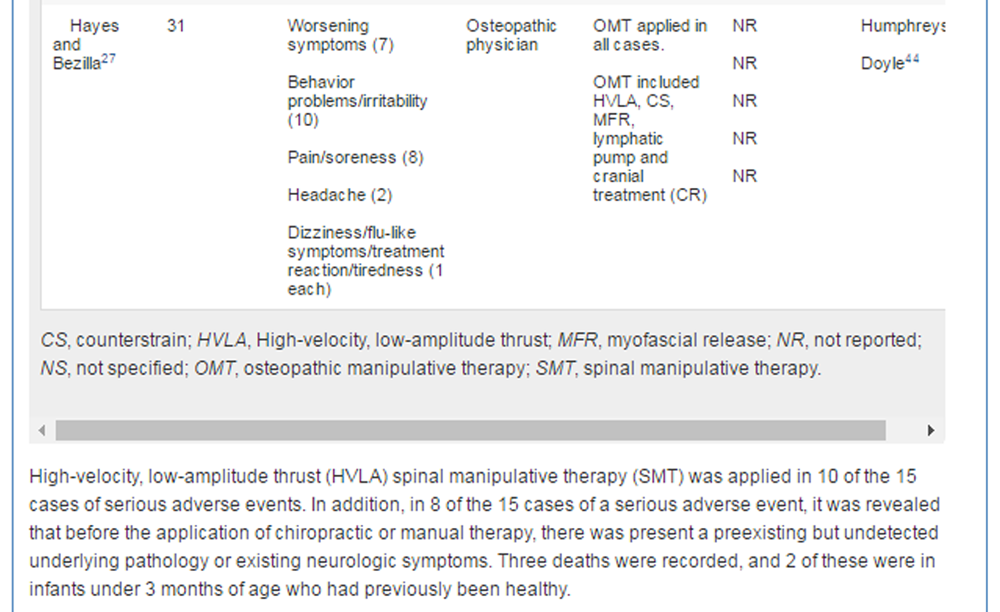
RESULTS: Thirty-one articles met the selection criteria. A total of 12 articles reporting 15 serious adverse events were found. Three deaths occurred under the care of various providers (1 physical therapist, 1 unknown practitioner, and 1 craniosacral therapist) and 12 serious injuries were reported (7 chiropractors/doctors of chiropractic, 1 medical practitioner, 1 osteopath, 2 physical therapists, and 1 unknown practitioner). High-velocity, extension, and rotational spinal manipulation was reported in most cases, with 1 case involving forcibly applied craniosacral dural tension and another involving use of an adjusting instrument. Underlying preexisting pathology was identified in a majority of the cases.
CONCLUSION: Published cases of serious adverse events in infants and children receiving chiropractic, osteopathic, physiotherapy, or manual medical therapy are rare. The 3 deaths that have been reported were associated with various manual therapists; however, no deaths associated with chiropractic care were found in the literature to date. Because underlying preexisting pathology was associated in a majority of reported cases, performing a thorough history and examination to exclude anatomical or neurologic anomalies before applying any manual therapy may further reduce adverse events across all manual therapy professions.
From the Full-Text Article:
Introduction
A 2010 survey of doctors of chiropractic across Europe and the United States [1] found that 5% to 11% of their client visits were pediatric patients, with an earlier worldwide study reporting in excess of 30 million chiropractic treatments are given to children annually. [2] The safety of chiropractic care for infants and children has been questioned by health practitioners and community members. [3–8] In Australia, the Friends of Science in Medicine has called for a ban on chiropractic care for children, claiming that heavy manipulation puts the lives of children at risk [9] based on the inaccurate reporting of a child having suffered a neck fracture after chiropractic therapy (dural tension technique and cranial therapy). A report by the Australian Health Practitioners Registration Authority (AHPRA) [10] cleared the chiropractor of any wrongdoing when expert radiological evidence showed the child had an undetected congenital cervical spondylolysis and there was no evidence of a fracture. Vohra et al [8] note that chiropractic management of infants and children safety data is virtually nonexistent, and others also express concern about the lack of beneficial evidence supporting chiropractic care for children. [11] This further highlights the stated need for more randomized controlled trials (RCTs). [1] However, in contrast to this reported lack of evidence, Rome [12] insists that there has been a considerable number of research articles and textbooks published in Europe espousing the benefits of manual therapy for children and infants, particularly the work of Biedermann. [13] A consensus document [14] supported the recommendation for standards of chiropractic care developed for children and clearly outlined best practice for the chiropractic care of infants, children, and adolescents, including when a therapeutic trial is reasonable, using evidence-based practice, as well as altering technique selection and application based upon the unique anatomy and physiology of infants, children, and adolescents.
It is not clear if the publicized concerns about the safety of chiropractic and other manual treatments for infants and young children are supported by published evidence. Therefore, the purpose of this review is to examine all reported cases of serious adverse events caused by practitioners who apply manual therapies (ie, chiropractors/doctors of chiropractic, physical therapists, medical physicians, doctors of osteopathy, and other manual therapists) when caring for infants and children, with particular focus on the types of treatment applied, the field of the treating practitioner, and whether a preexisting, undiagnosed pathology was present. [8, 15]
Methods

Figure 1

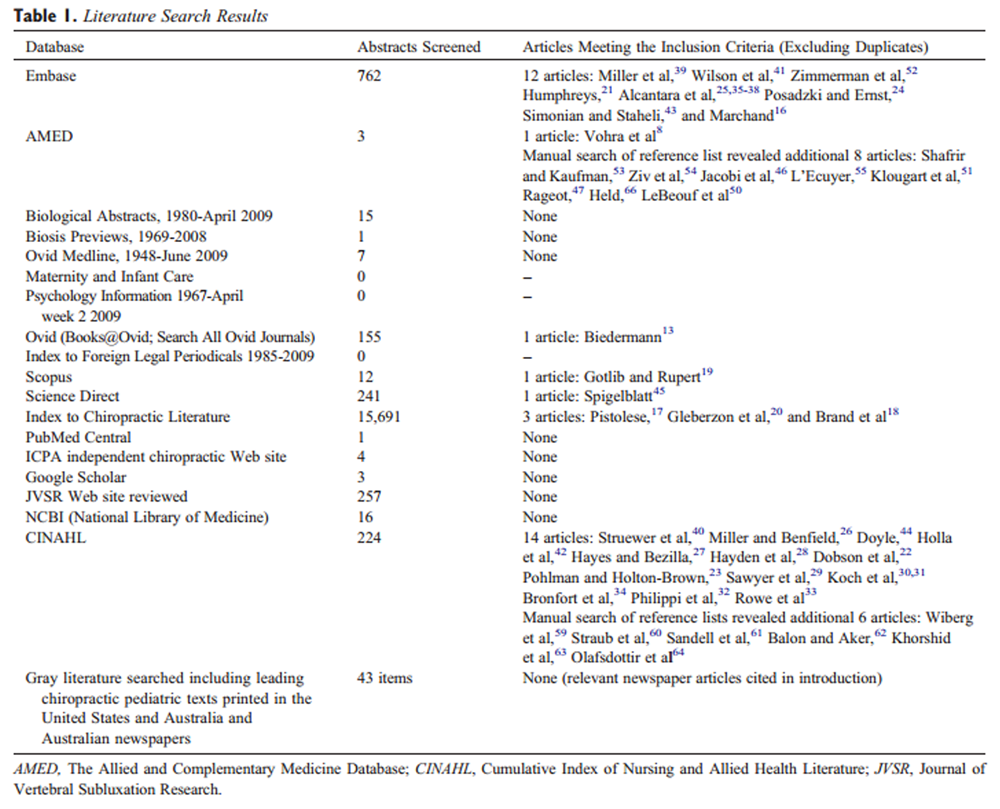
Table 1 The scientific literature was systematically searched using the terms summarized in Figure 1 in the locations listed in Table 1. The search of published peer-reviewed articles and gray literature included events documented by any manual therapy health provider (ie, chiropractors/doctors of chiropractic, physical therapists, medical physicians, doctors of osteopathy, and other manual therapists). Throughout this article, the term physical therapist (a term used in the United States) is used in preference to physiotherapists (used in other countries to refer to the same professional type).
Only articles published in the English language were searched. All available articles published from the inception of searchable bibliographic databases to March 2014 were included. EMBASE, AMED, BIOSIS previews, MEDLINE, Maternity and Infant Care, OVID, CINAHL, Psychinfo, PubMed, INDEX to Foreign and Legal Periodicals, SCOPUS, Science Direct, Index to Chiropractic Literature, and PubMed Central databases were searched.
Web sites, books, and gray literature were searched including Google Scholar and 2 chiropractic Web sites, the International Chiropractic Pediatric Association and Journal of Vertebral Subluxation Research. The bibliographies of seminal articles were screened to identify any additional articles.
Abstracts were screened for those discussing manual therapy of any kind on infants and children. After reading the relevant full texts, articles were included in this review if they clearly discussed adverse events (mild, moderate, or severe). Articles were excluded if they were commentaries not reporting case information, the details of adverse event data collection were not clear, there was no discussion of adverse events, or the articles did not discuss manual therapy with children.
The full text of each document was analyzed to identify the nature of the adverse event; the practitioner type; technique applied; and evidence of any undiagnosed, preexisting pathology. Adverse events were defined as mild (transient effects lasting <24 hours, eg, crying or discomfort), moderate (requiring medical/general practitioner treatment), or severe (requiring hospital treatment)16
Results
Table 2A
Table 2B
Table 2C
Table 2D
Table 2E
The search captured 17,435 potential articles, and of that, 48 published, peer-reviewed articles were reviewed (Table 1), 31 of which met the selection criteria (all 31 articles are summarized in Appendix A).
Included were5 systematic reviews of the literature, [8, 17, 18, 19, 20]
5 narrative reviews, [21, 22, 23, 24, 25]
4 cross-sectional surveys, [16, 26, 27, 28]
6 randomized controlled trials, [29, 30, 31, 32, 33, 34]
4 Practice Based Research Network (PBRN) survey studies, [35, 36, 37, 38]
4 case studies and 1 case series, [39, 40, 41, 42, 43] and
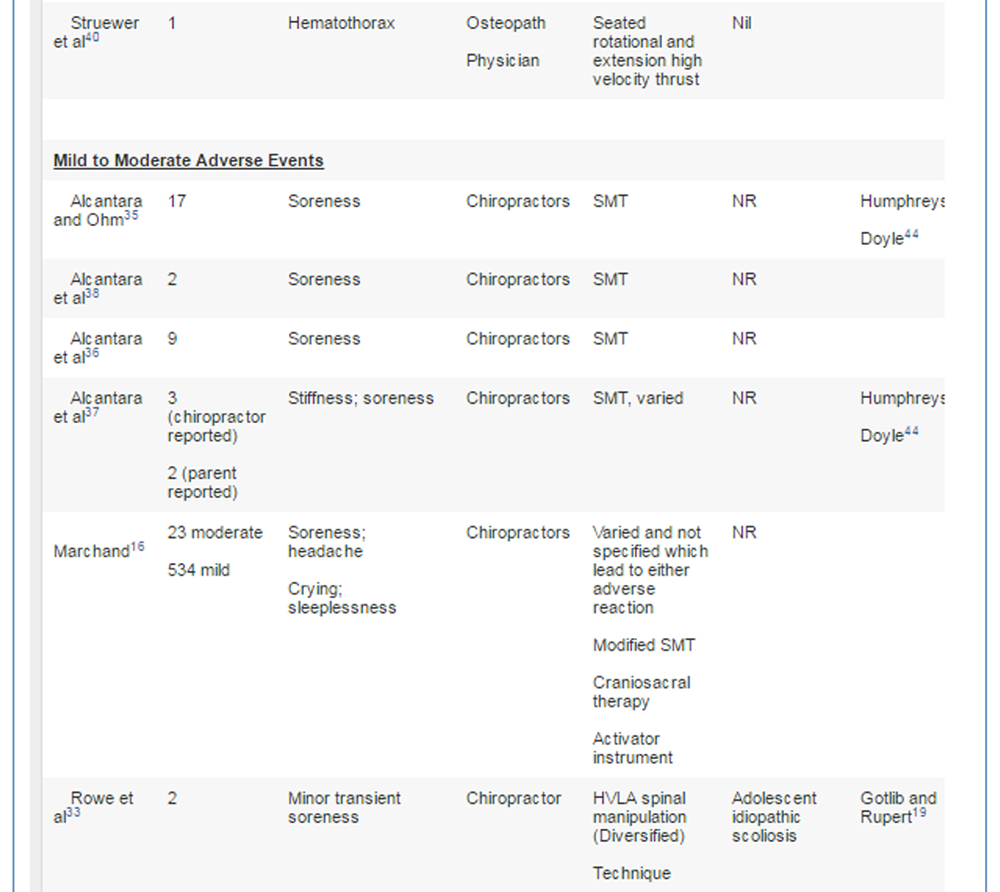
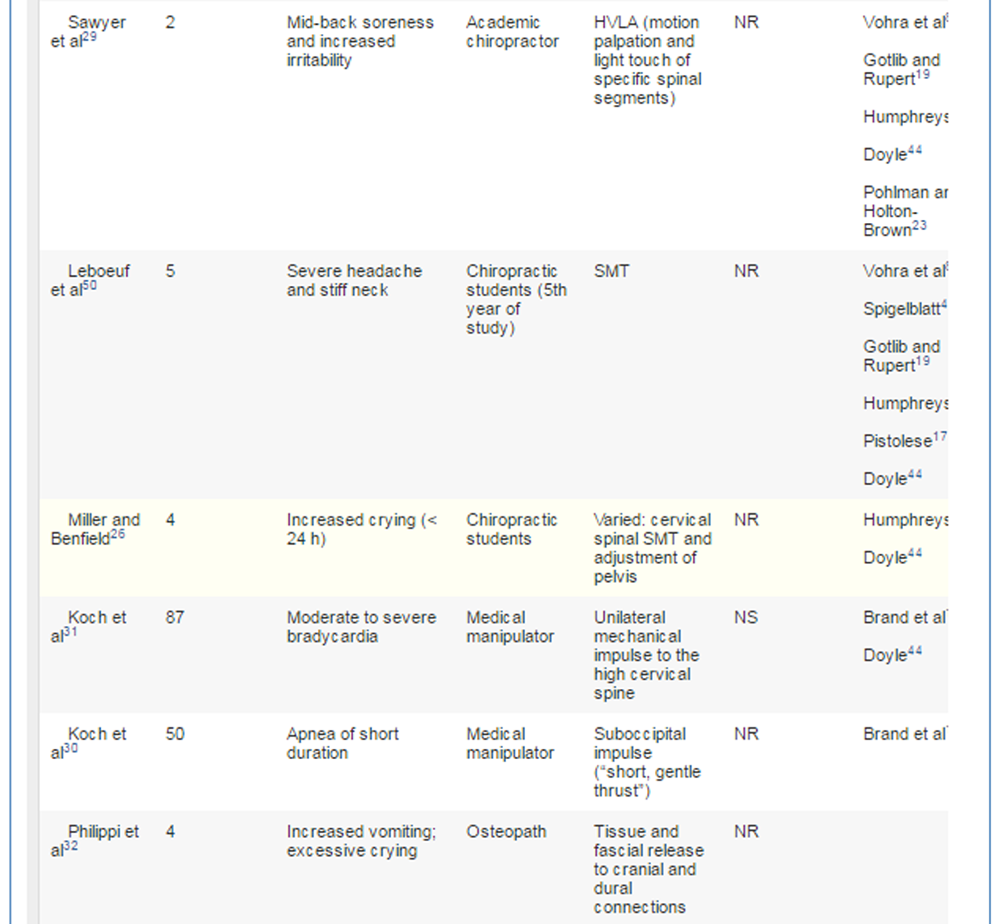
2 discussion papers. [44, 45]The details of all adverse events results are summarized in Table 2. This includes 15 instances of serious adverse events involving the application of some form of manual therapy on children younger 18 years. Moderate and mild adverse events are also described (Table 2).
Discussion
This review of the literature varies from previous reviews in that it looks into the adverse events for all types of manual therapists and not just chiropractors and combines this information with the type of technique that was used and also finally the presence of any preexisting pathology. This review of the literature identified that some authors suggest that adverse events can occur after manual therapies; however, the reported incidence appears to be rare and may be heightened by preexisting pathologies or the use of inappropriate techniques or inappropriately applied techniques.
Three deaths have been reported to be associated with any type of manual therapy:a 3–month-old infant treated by a physical therapist using both electrical current and spinal manipulation [46];
a craniosacral therapist incorrectly applying craniosacral therapy [42];
and a death reported in France in the 1960s with no details of the therapist type or technique used, although it is known that the child had underlying pneumonia. [47]All 3 of these deaths were associated with European-based practitioners in a region where regulation of chiropractic care is relatively recent. These 3 deaths reflect similar findings from previous reviews that misdiagnosis, failure to recognize the onset or progression of neurological symptoms, improper technique, SMT performed in the presence of clotting disorders, or poor spinal structural integrity increases the likelihood of an adverse event. [48]
This review found that HVLA thrust techniques were more often reported as the technique used in adverse events in infants and children and further research is required to determine if this is the result of the specific manipulations involved in HVLA, is an artifact of the greater frequency with which this treatment is used across all therapy types, or is the result of limitations in the experience and training of the manual therapist. It is also necessary to determine whether particular techniques or forces are more appropriate for different ages, perhaps in accordance with the known osteoligamentous tensile strength limits, the anatomical development of the spine and nervous system in the child, and the potential for subcatastrophic events, especially in infants less than 3 months of age. [49]
In addition to the 15 serious events that have been reported, there have been 775 mild to moderate adverse events. This includes 604 cases of crying, soreness, or transient headache, [16, 26, 33, 36, 37, 38, 50] and 1 case of syncope [51] recorded after chiropractic care. There were a further 35 cases of soreness or transient headache [27, 32] after osteopathic treatment. Finally, there were 50 cases of transient apnea (returned to normal in 4 breaths) with vegetative responses [30] and 87 cases of short lasting (seconds) marked bradycardia, in infants after SMT to the upper cervical spine in otherwise healthy children from medical manipulators. [31] These responses to manual medical therapy were recorded as part of an experiment in a hospital setting, and further investigation of this potentially serious physiological phenomenon in infants less than 3 months of age is warranted.
Manual medicine practitioners in Europe tend to use SMT for children from birth, [12, 13] and radiographs are almost always undertaken to exclude skeletal pathology before the application of SMT. The use of ultrasound, before full cervical spine ossification, pediatrician screening, and appropriate neurologic examination to screen out those children with an underlying pathology and to refer them appropriately, should be a consideration for all those using manual therapy in infants with congenital torticollis or unusual body posturing.
Although this review has looked at all types of manual therapies involving children, it should be noted that in terms of chiropractic treatments, the number of treatments for the population is extensive; however, there are no reported deaths and only 7 severe adverse events, [41, 47, 51–55] 4 of which were associated with an underlying preexisting pathology [52–55] and the health status of 1 other child unknown before care. [47] The HVLA spinal manipulation was the technique that was reported to be most common of these rare recorded adverse events associated with chiropractic care.
Chiropractors are trained to use techniques that best suit the age and condition of the patient. Undergraduates are taught to modify the level of force during manipulation such as when used on a child and a variety of techniques can be considered for neonates or infants. [56, 57] In a study of 956 European chiropractors, [16] more than 96% reported treating children, and they estimated that they reduced the magnitude of their thrusts with infants under 1 year of age by 90% of that used on adults, with the level being gradually increased in line with the age of the child. Chiropractors, osteopaths, physical therapists, and manual medicine practitioners all use very similar modified SMT and stretching techniques when treating very young infants and children. [12]
Limitations
This literature review may have missed relevant articles because the search was only conducted in English publications. A further limitation would be that the terms referring to manipulation vary considerably in the literature and so what is described as spinal manipulation can vary to be very light touch to the use of a mechanical instrument to that of a modified HVLA thrust. [58] Biedermann [13] is a European medical manual therapist with decades of experience and none of Biedermann's comments regarding medical manipulation of infants and its apparent safety were included in the results because this was merely commentary and there were no specific cases reported. The RCTs of Wiberg et al, [59] Klougart et al, [51] Straub et al, [60] Sandell et al, [61] Balon et al, [62] Khorshid et al, [63] and Olafsdottir et al [64] were reviewed but excluded from the matrix for this article because there was no mention of whether adverse event data were recorded.
Recommendations
Adverse Event Reporting
More comprehensive methods of adverse event recording across all manual therapy professions are recommended. For example, the Chiropractic Patient Incident Reporting and Learning System launched in the UK in 2005 [65] is now accessible to Australian chiropractors. This adverse event report monitoring service is available for chiropractors to report anonymously. The Chiropractic Patient Incident Reporting and Learning System reporting system is not currently available to all other users of manual therapy so reported events may be overrepresented by chiropractors. We should consider how to include all manual therapists in the collection of this type of data and ensure that practitioners use the service and make changes based on the reports.
Registration boards of all professions involved in this study have the primary role of reducing risk to the community at large from poor practitioner conduct and delivery of care. For example, in Australia, this is through the AHPRA.
A related issue canvassed by Vohra et al8 is that not all parents of children treated by a chiropractor will return to the chiropractor if they believe there has been an adverse event. Instead, parents may turn to their medical practitioners or other health care providers such as maternal and child health nurses or hospitals, leading to possible underreporting of adverse events. The regulatory body AHPRA has a role in providing an avenue for reporting of adverse events that is independent and available to everyone in the community.
Undergraduate Education
To enhance the safe application of manual therapy on children, regulatory bodies, and also universities could ensure that undergraduates are exposed to a broad case mix of patients including children and that a range of age appropriate techniques are taught. Further study in this area is required.
In terms of chiropractic training, undergraduate education prepares chiropractors for working with all ages of patients and is part of the worldwide requirements for chiropractic education and accreditation. Likewise, osteopaths, manual medicine practitioners, and physical therapists are trained in the assessment and application of therapy across all ages of people. A review of the rigor and quality of postgraduate courses available is also needed.
All Manual Therapists Need to Be Diligent in Clinical Practice and Application
Because some of the adverse events reported in the literature may have been avoided if a better history and examination were completed or if there had been a better technique selection or application, it might be appropriate to further investigate both undergraduate and postgraduate training of all types of manual therapy practitioners. Further research is recommended to investigate appropriate technique usage, especially of HVLA, and the range and number of case mix exposures that would deem someone competent to care for children.
Conclusion
Published cases of serious adverse events in infants and children receiving chiropractic, osteopathic, physiotherapy, or manual medical therapy are exceedingly rare. There have been no cases of deaths associated with chiropractic care reported in the academic literature to date. Three deaths were reported caused by other types of manual therapists. Performing a thorough history and examination to exclude anatomical or neurologic anomalies before the provision of care, appropriate technique selection and its application may further reduce adverse events across all manual therapy professions.
Appendix A. Studies included in review
References:
Hestbaek, L and Stochkendahl, MJ.
The Evidence Base for Chiropractic Treatment of Musculoskeletal
Conditions in Children and Adolescents: The Emperor's New Suit?
Chiropractic & Osteopathy 2010 (Jun 2); 18: 15Lee, AC, Li, DH, and Kemper, KJ.
Chiropractic Care for Children
Arch Pediatr Adolesc Med 2000 (Apr); 154 (4): 401–407Chapman-Smith, D.
The chiropractic profession: its education, practice, research, and future directions.
NCMIC Group, Des Moines; 2000Beck, RW.
Functional neurology for practitioners of manual therapy.
Churchill Livingstone Elsevier, Philadelphia; 2008Gotlib, A and Rupert, R.
Assessing the Evidence for the Use of Chiropractic Manipulation in Paediatric Health Conditions:
A Systematic Review
Paediatr Child Health. 2005 (Mar); 10 (3): 157–161Hamann, G, Felber, S, Haas, A et al.
Cervicocephalic artery dissections due to chiropractic manipulations.
Lancet. 1993; 341: 764–765Christensen, P.
Sceptics question alternative claim: more chiropractors are treating more Australians every year.
The Australian. ; 2011Vohra, S, Johnston, BC, Cramer, K, and Humphreys, K.
Adverse Events Associated with Pediatric Spinal Manipulation: A Systematic Review
Pediatrics. 2007 (Jan); 119 (1): e275–e283Corderoy, A.
Chiropractic funding called into question.
Sydney Morning Herald. ; 2013Fraser, A.
Chiropractor cleared over “break”.
The Australian. ; 2013Ernst, E.
Spinal manipulation for asthma: a systematic review of randomised clinical trials.
Respir Med. 2009; 103: 1791–1795Rome, PL.
Medical Management of Pediatric and Non-Musculoskeletal
Conditions by Spinal Manipulation
Chiropractic Journal of Australia 2013 (Dec); 43 (4): 131–136Biedermann, H.
Manual Therapy in Children: Proposals for an Etiologic Model
J Manipulative Physiol Ther 2005 (Mar); 28 (3): e1–e15Hawk, C, Schneider, M, Ferrance, RJ, Hewitt, E.
Best Practices Recommendations for Chiropractic Care for Infants, Children,
and Adolescents: Results of a Consensus Process
J Manipulative Physiol Ther. 2009 (Oct); 32 (8): 639–647Ernst, E.
Serious adverse effects of unconventional therapies for children and adolescents: a systematic review of recent evidence.
Eur J Pediatr. 2003; 162: 72–80Marchand, AM.
Chiropractic Care of Children from Birth to Adolescence and Classification
of Reported Conditions: An Internet Cross-Sectional Survey
of 956 European Chiropractors
J Manipulative Physiol Ther. 2012 (Jun); 35 (5): 372–380Pistolese, RA.
Risk Assessment of Neurological and/or Vertebrobasilar Complications
in the Pediatric Chiropractic Patient
J Vertebral Subluxation Research 1998; 2 (2): 73–78Brand, PL, Englebert, R, Paul, H, Helders, J.
Systematic review of effects of manual therapy in infants with kinematic imbalance due to suboccipital strain (kiss) syndrome.
J Manipulative Physiol Ther. 2005; 13: 209–214Gotlib, A and Rupert, R.
Chiropractic Manipulation in Pediatric Health Conditions - An Updated Systematic Review
Chiropractic & Osteopathy 2008 (Sep 12); 16: 11Gleberzon, BJ, Arts, J, Mei, A, and McManus, EL.
The Use of Spinal Manipulative Therapy For Pediatric Health Conditions:
A Systematic Review of the Literature
J Can Chiropr Assoc. 2012 (Jun); 56 (2): 128–141Humphreys, BK.
Possible adverse events in children treated by manual therapy: a review.
Chiropr Osteopat. 2010; 18Dobson D, Lucassen PLBJ, Miller JJ, Vlieger AM, Prescott P, Lewith G.
Manipulative Therapies for Infantile Colic
Cochrane Database Syst Rev. 2012 (Dec 12); 12: CD004796Pohlman KA, Holton-Brown MS.
Otitis Media and Spinal Manipulative Therapy: A Literature Review
Journal of Chiropractic Medicine 2012 (Sep); 11 (3): 160–169Posadzki, P and Ernst, E.
Is spinal manipulation effective for paediatric conditions? An overview of systematic reviews.
Focus Altern Complement Ther. 2012; 17: 22–26Alcantara, J, Alcantara, JD, and Alcantara, J.
An integrative review of the literature on the chiropractic care of infants with constipation.
Complement Ther Clin Pract. 2014; 20: 32–36Miller, JE and Benfield, K.
Adverse effects of spinal manipulative therapy in children younger than 3 years: a retrospective study in a chiropractic teaching clinic.
J Manipulative Physiol Ther. 2008; 31: 419–423Hayes, NM and Bezilla, TA.
Incidence of iatrogenesis associated with osteopathic manipulative treatment of pediatric patients.
J Am Osteopath Assoc. 2006; 106: 605–608Hayden, JA, Mior, SA, and Verhoef, MJ.
Evaluation of chiropractic management of pediatric patients with low back pain: a prospective cohort study.
J Manipulative Physiol Ther. 2003; 26: 1–8Sawyer C.E., Evans R.L., Boline P.D., Branson R., Spicer A.
A Feasibility Study of Chiropractic Spinal Manipulation Versus Sham Spinal Manipulation for
Chronic Otitis Media with Effusion in Children
J Manipulative Physiol Ther 1999 (Jun); 22 (5): 292–298Koch, LE, Biedermann, H, and Saternus, KS.
High cervical stress and apnoea.
Forensic Sci Int. 1998; 97: 1–9Koch, LE, Koch, H, Graumann-Brunt, S, Stolle, D.
Heart rate changes in response to mild mechanical irritation of the high cervical spinal cord region in infants.
Forensic Sci Int. 2002; 128: 168–176Philippi, H, Faldum, A, Schleupen, A et al.
Infantile postural asymmetry and osteopathic treatment: a randomized therapeutic trial.
Dev Med Child Neurol. 2006; 48: 5–9 ([discussion 4])Rowe D.E., Feise R.J., Crowther E.R., Grod J.P., Menke J.M., Goldsmith C.H.
Chiropractic Manipulation in Adolescent Idiopathic Scoliosis: A Pilot Study
Chiropractic & Osteopathy 2006 (Aug 21); 14: 15Bronfort G, Evans RL, Kubic P, Filkin P.
Chronic Pediatric Asthma and Chiropractic Spinal Manipulation:
A Prospective Clinical Series and Randomized Clinical Pilot Study
J Manipulative Physiol Ther 2001 (July); 24 (6): 369–377Alcantara, J and Ohm, J.
The safety and effectiveness of pediatric chiropractic: results from a practice-based research network.
ICPA, ; 2006Alcantara, J, Ohm, J, and Kunz, D.
The safety and effectiveness of pediatric chiropractic: a survey of chiropractors and parents in a practice-based research network.
Explore (NY). 2009; 5: 290–295Alcantara, J, Ohm, J, and Kunz, D.
Treatment-related aggravations, complications and improvements attributed to chiropractic spinal manipulative therapy of pediatric patients: a practice-based survey of practitioners.
Focus Altern Complement Ther. 2007; 12: 3Alcantara, J, Ohm, J, and Kunz, D.
Treatment related aggravations, complications and improvements with pediatric chiropractic SMT: a survey of parents.
ICPA, ; 2006Miller, J. E., Miller, L., Sulesund, A. K., & Yevtushenko, A.
Contribution of Chiropractic Therapy to Resolving Suboptimal Breastfeeding:
A Case Series of 114 Infants
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 670–674Struewer, J, Frangen, TM, Ziring, E, Hinterseher, U, and Kiriazidis, I.
Massive hematothorax after thoracic spinal manipulation for acute thoracolumbar pain.
Orthop Rev (Pavia). 2013; 5: 120–122Wilson, P, Greiner, M, and Duma, E.
Posterior rib fractures in a young infant who received chiropractic care.
Pediatrics. 2012; 130: 1359–1362 ([Internet])Holla, M, Ijland, MM, van der Vliet, AM, Edwards, M.
Death of an infant following “craniosacral” manipulation of the neck and spine.
Ned Tijdschr Geneeskd. 2009; 153: 828–831Simonian, PT and Staheli, LT.
Periarticular fractures after manipulation for knee contractures in children.
J Pediatr Orthop. 1995; 15: 288–291Doyle, MF.
Is chiropractic paediatric care safe? A best evidence topic.
Clin Chiropr. 2011; 14: 97–105Spigelblatt, L.
Chiropractic care for children: controversies and issues, position statement.
Paediatr Child Health (Oxford). 2002; 7: 85–89Jacobi, G, Riepert, T, Kieslich, M, and Bohl, J.
Fatal outcome during physiotherapy (vojta's method) in a 3-month old infant. Case report and comments on manual therapy in children.
Klin Padiatr. 2001; 213: 76–85Rageot, E.
Complications and accidents in vertebral manipulation.
Cah Coll Med Hop Paris. 1968; 9: 1149–1154Powell, FC, Hanigan, WC, and Olivero, WC.
A risk/benefit analysis of spinal manipulation therapy for relief of lumbar or cervical pain.
Neurosurgery. 1993; 33: 73–78 ([discussion 8–9])Marchand AM.
A Proposed Model With Possible Implications for Safety and Technique Adaptations
for Chiropractic Spinal Manipulative Therapy for Infants and Children
J Manipulative Physiol Ther 2015 (Nov); 38 (9): 713–726Leboeuf, C, Brown, P, Herman, A, Leembruggen, K, Walton, D, and Crisp, TC.
Chiropractic care of children with nocturnal enuresis: a prospective outcome study.
J Manipulative Physiol Ther. 1991; 14: 110–115Klougart, N, Leboeuf-Yde, C, and Rasmussen, LR.
Safety in chiropractic practice. Part II: treatment to the upper neck and the rate of cerebrovascular incidents.
J Manipulative Physiol Ther. 1996; 19: 563–569Zimmerman, AW, Kumar, AJ, Gadoth, N, and Hodges, FJ.
Traumatic vertebrobasilar occlusive disease in childhood.
Neurology. 1978; 28: 185–188Shafrir, Y and Kaufman, BA.
Quadriplegia after chiropractic manipulation in an infant with congenital torticollis caused by a spinal cord astrocytoma.
J Pediatr. 1992; 120: 266–269Ziv, I, Rang, M, and Hoffman, HJ.
Paraplegia in osteogenesis imperfecta. A case report.
J Bone Joint Surg (Br). 1983; 65: 184–185L'Ecuyer, JL.
Congenital occipitalization of the atlas with chiropractic manipulations: a case report.
Nebr State Med J. 1959; 44: 546–550Gleberzon, BJ.
Chiropractic name techniques in Canada: a continued look at demographic trends and their impact on issues of jurisprudence.
J Can Chiropr Assoc. 2002; 46: 241–256Mykietiuk, C, Wambolt, M, Pillipow, T, Mallay, C.
Technique systems used by post-1980 graduates of the Canadian Memorial Chiropractic College practicing in five Canadian provinces: a preliminary survey.
J Can Chiropr Assoc. 2009; 53: 32–39Wenban, AB.
Inappropriate use of the title “chiropractor” and term “chiropractic manipulation” in the peer-reviewed biomedical literature.
Chiropr Osteopat. 2006; 14: 16Wiberg, JM, Nordsteen, J, and Nilsson, N.
The Short-term Effect of Spinal Manipulation in the Treatment of Infantile Colic:
A Randomized Controlled Clinical Trial with a Blinded Observer
J Manipulative Physiol Ther 1999 (Oct); 22 (8): 517–522Straub, WF, Spino, MP, Alattar, MM et al.
The effect of chiropractic care on jet lag of Finnish junior elite athletes.
J Manipulative Physiol Ther. 2001; 24: 191–198Sandell, J, Palmgren, PJ, and Bjorndahl, L.
Effect of chiropractic treatment on hip extension ability and running velocity among young male running athletes.
J Chiropr Med. 2008; 7: 39–47Balon J, et al.
A Comparison of Active and Simulated Chiropractic Manipulation as Adjunctive Treatment
for Childhood Asthma
New England Journal of Medicine 1998; 339(15): 1013-1020Khorshid, K, Sweat, RW, Zemba, D, and Zemba, BN.
Clinical efficacy of upper cervical versus full spine chiropractic care on children with autism: a randomized clinical trial.
J Vertebral Subluxation Res. 2006; : 1–7Olafsdottir E, Forshei S, Fluge G, Markestad T:
Randomised Controlled Trial of Infantile Colic Treated With Chiropractic Spinal Manipulation
Archives of Disease in Childhood 2001 (Feb); 84 (2): 138–141Thiel, H and Bolton, J.
The reporting of patient safety incidents—first experiences with the chiropractic reporting and learning system (CRLS): a pilot study.
Clin Chiropr. 2006; 9: 139–149Held, JP.
Dangers of cervical manipulation in neurology.
Ann Med Phys (Lille). 1966; : 251–259
Return to PEDIATRICS
Return to ADVERSE EVENTS
Since 1–30–2015
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |