

Core Competencies of the Certified Pediatric Doctor
of Chiropractic: Results of a Delphi Consensus ProcessThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Evid Based Complementary Altern Med. 2016 (Apr); 21 (2): 110–114 ~ FULL TEXT
OPEN ACCESS Elise Hewitt, DC, DICCP, FICC, Lise Hestbaek, DC, PhD,
Katherine A. Pohlman, DC, MS, DICCP, PhD(c)
Portland Chiropractic Group and University of Western States,
Portland, OR, USA
drelise@portlandchiropracticgroup.comAn outline of the minimum core competencies expected from a certified pediatric doctor of chiropractic was developed using a Delphi consensus process. The initial set of seed statements and substatements was modeled on competency documents used by organizations that oversee chiropractic and medical education. These statements were distributed to the Delphi panel, reaching consensus when 80% of the panelists approved each segment. The panel consisted of 23 specialists in chiropractic pediatrics (14 females) from across the broad spectrum of the chiropractic profession. Sixty-one percent of panelists had postgraduate pediatric certifications or degrees, 39% had additional graduate degrees, and 74% were faculty at a chiropractic institution and/or in a postgraduate pediatrics program. The panel were initially given 10 statements with related substatements formulated by the study's steering committee. On all 3 rounds of the Delphi process the panelists reached consensus; however, multiple rounds occurred to incorporate the valuable qualitative feedback received.
Key Indexing Terms: children, chiropractic, education
From the Full-Text Article:
Introduction

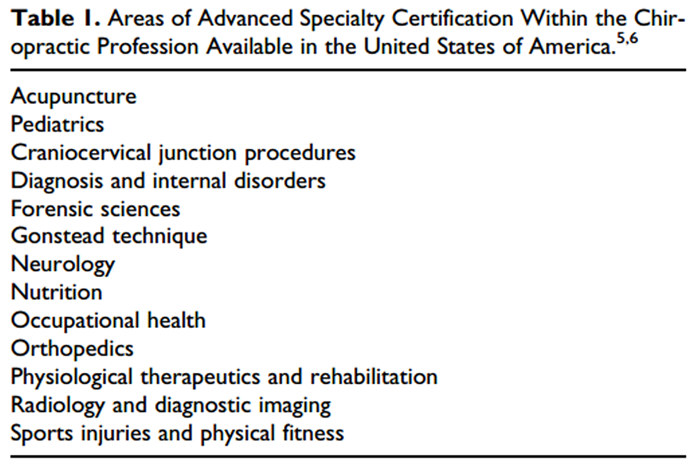
Table 1 With doctors of chiropractic playing an increasing role in the integrative team of health care providers, [1–4] it is important to delineate the skills of those doctors of chiropractic who present themselves as certified specialists. Chiropractic undergraduate educational curriculum includes training in many specialty areas, including sports, neurology, nutrition, radiology, and pediatrics, to name a few. This training supplies the necessary skills for all doctors of chiropractic to provide basic care within each specialty. As the chiropractic profession has grown and matured, specialty certifications have developed for those doctors of chiropractic wishing to further their education and skills in specific areas of practice. Currently, there are several certification programs covering 13 areas of advanced specialty within the chiropractic profession (see Table 1). [5, 6] Becoming a certified specialist requires advanced training and passage of a specialty-specific certification examination.
One such specialty is the field of chiropractic pediatrics. Usage of the services of a doctor of chiropractic by the pediatric population has increased over time. In 2008, the Centers for Disease Control and Prevention reported chiropractic/osteopathic was the most common form of provider-administered complementary or alternative medicine used by children in the United States. [7] A recent update to this survey found the percentage of children receiving chiropractic/osteopathic manipulation has increased from 2.8% in 2007 to 3.3% in 2012. [8] The most recent practice analysis by the National Board of Chiropractic Examiners found the percentage of pediatric patients in US practices has increased from 9.7% in 1991 to 17.4% in 2014. [9] A recent study of 20 European countries found children represented 8.1% of European chiropractic practices. [10] A job analysis of certified pediatric doctors of chiropractic was conducted in 2009, but core competencies were not evaluated. [11]
Two postgraduate pediatric diplomate programs have been developed within the chiropractic profession in the United States, with additional programs in the United Kingdom and Australia. In 1993, the first program was developed by the International Chiropractors Association’s (ICA) Council on Chiropractic Pediatrics. This program offers a Diplomate in Clinical Chiropractic Pediatrics (DICCP). [12] In 2002, a second program, the Diplomate in Pediatrics from the Academy Council of Chiropractic Pediatrics (DACCP), was organized by the International Chiropractic Pediatric Association (ICPA). [13] A doctor of chiropractic who completes one of these programs and passes a board examination is referred to in this report as a “Certified Pediatric Doctor of Chiropractic” (CPDC).
These postgraduate programs entail between 280 and 400 hours of training taken over 2 to 3 years. As the purpose of these postgraduate training programs is to expand on and deepen the knowledge base obtained during the undergraduate chiropractic curriculum, the resulting competencies will be a combination of both the basic chiropractic training and the additional acquired skills.
The Council on Chiropractic Education defines the required competencies for the general doctor of chiropractic. Although individual pediatric specialty programs have their own requirements, no profession-wide consensus of standards exists for the CPDC. [14] Thus, institutions wishing to develop postgraduate educational programs in chiropractic pediatrics have no standards to guide the development of their programs. Similarly, testing bodies lack profession-wide guidelines on which to structure certification examinations. Finally, without outlined competencies patients as well as other health care practitioners cannot be informed about the competencies of a CPDC. Therefore, the purpose of this study was to utilize an expert Delphi panel to develop consensus-based core competencies for the CPDC. This panel was composed of a diverse group of chiropractic pediatric specialists from across the broad spectrum of the chiropractic profession to ensure all viewpoints were represented.
Methods
This project was approved by Logan University Institutional Review Board, which ensured all issues related to the rights and confidentiality of the participating panelists were addressed. Panelists gave written consent to use their names in relation to all aspects of this project, including any publications. The steering committee provided oversight for the development of the competencies.
Establishment of a Steering Committee (SC)
The purpose of the Steering Committee (SC) was to provide oversight in the development of the competencies and to ensure that all stakeholders were represented on the panel. The SC evaluated all panelists’ comments received after each round, revised the seed statements as appropriate, then returned the revised statements to the panel for further evaluation. The SC was made up of the 3 authors who are all doctors of chiropractic with an average 20 years of experience within the chiropractic profession: 2 authors hold postgraduate pediatric certifications, 1 author is a PhD, 1 author a PhD candidate, and 2 authors are faculty/adjunct faculty at chiropractic institutions. The SC was multinational, with members living in the United States, Canada, and Denmark.
Seed Statement Development
The initial 10 seed statements and substatements were based on similar competencies used by other organizations, including (a) the Council on Chiropractic Education’s Metacompetencies for Undergraduate Doctor of Chiropractic Degree Programs [14] and (b) Paediatric Undergraduate Program Directors of Canada Shared Canadian Curriculum for Undergraduate Paediatrics: Outcomes for the Graduating Medical Student. [15] An initial draft of the seed statements was developed by a committee of experts in pediatrics and education convened by the American Chiropractic Association’s (ACA) Council on Chiropractic Pediatrics. The SC refined these into the initial set of seed statements and substatements provided to the Delphi panelists. The 10 seed competencies related to different aspects of the clinical encounter with pediatric patients, including a working knowledge of pediatric growth and developmental, childhood health conditions, age-appropriate evaluation, development of differential diagnoses and management plan, and delivery of appropriate therapeutic interventions. The statements also discussed collaboration with other health care providers, as well as the maintenance of high professional and ethical standards. Seed statements were further defined by substatements as appropriate.
Delphi Panel Invitees
The SC developed a list of 35 doctors of chiropractic with a special interest in pediatrics (22 females), which included instructors in current postgraduate pediatric chiropractic courses, scientists with clinical pediatric expertise, holders of pediatric chiropractic board certification, and undergraduate pediatric chiropractic instructors. Panelists were invited from an array of perspectives within the chiropractic profession to ensure broad representation. Thirty-three of the invited panelists held chiropractic degrees with 14 holding additional degrees/certifications in multidisciplinary professions, including nursing, physical therapy, medicine, academic degrees, and lactation consulting. Twenty of the invitees were CPDCs; 4 others held certifications in the chiropractic specialties of radiology, neurology, or orthopedics.
Delphi Consensus Process
The goal of the Delphi process was to gather judgment and potential additional information from experts. All communication with the Delphi panel occurred through email, and all panelists were kept anonymous throughout the process. This method limited bias and reduced the chances that panelists could influence each other’s opinions. We utilized the RAND Corp/University of California, Los Angeles Delphi methodology. [16]
Panelists were asked to indicate the appropriateness of each competency described in the seed statement and any related substatements according to a 9-point scale (highly inappropriate to highly appropriate). The RAND methodology was used to define appropriateness as“the expected health benefit to the patient exceeds the expected negative consequences by a sufficiently wide margin that it is worth doing, exclusive of cost.” [16]
A comment box was provided following each seed statement that allowed any length of comment desired. If an inappropriate score was assigned (less than 5), panelists were required to provide the specific reason.
Agreement on appropriateness for each competency was considered to be present if at least 80% of the panelists gave an “appropriate” rating, defined as 7 or more points and the median rating was at least 7. Additional Delphi rounds were to be repeated until at least 80% consensus was reached for all seed statements and substatements.
Results
Of the 35 panelists invited to participate, 23 agreed to participate (66%).
Panelists represented 4 countries14 United States,
4 Australia,
3 Canada, and
2 Englandand 61% were female (n = 14). All but one member of the Delphi panel were doctors of chiropractic, and 74% (n = 17) were faculty at a chiropractic institution and/or in a postgraduate pediatrics program. Additional graduate degrees (MD, PhD, MS) were held by 39% (n = 9), and 61% (n = 14) had a postgraduate certification or degree in pediatrics. Regarding pediatric chiropractic association membership, 52% had no association with a specific US pediatric organization (n = 12), 30% were members of the ICA Pediatrics Council (n = 7), 26% ACA Pediatrics Council (n = 6), and 17% ICPA (n = 4).
Delphi Rounds
The Delphi panel participated in 3 rounds from January to May 2015. The rounds had a response rate of 91%, 54%, and 91%, respectively. In each round, all statements reached consensus, that is, more than 80% of the panelists gave an “appropriate” rating; however, the panelists provided a large body of quality feedback on the first 2 rounds. As a result, the Steering Committee (SC) felt additional rounds were necessary to incorporate the panel’s feedback. The third round had no substantive changes required from panelists’ feedback, so competencies were considered complete by the SC. Throughout the project, agreement was reached among the SC members and no requests for minority opinions were received from the panelists.
Competencies Description
Following are the introduction and final competencies expected of the CPDC as decided on by the Delphi panel of chiropractic pediatric experts.
Core Competencies of the Certified Pediatric Doctor of Chiropractic
Introduction
All doctors of chiropractic are adequately trained in basic pediatrics skills and are licensed to examine, treat, and manage pediatric patients. The following core competencies describe the minimum skills of doctors of chiropractic who have received additional postgraduate certification in the specialty of chiropractic pediatrics. Many of these skills naturally overlap with those of the general doctor of chiropractic. Formalizing these competencies does not imply that only certified pediatric doctors of chiropractic may treat children; rather, the certified pediatric doctor of chiropractic has obtained a deeper knowledge and skillset compared to the general doctor of chiropractic. This document applies to patients under the age of 18 years and assumes that certified pediatric doctors of chiropractic use the principles of evidence informed clinical practice.
The Certified Pediatric Doctor of Chiropractic will...

Possess a working knowledge and understanding of the anatomy,
physiology, neurology, psychology, and developmental stages of a child.
Recognize known effects of the prenatal environment, length of the pregnancy,
and birth process on the child’s health.Identify and evaluate the stages of growth and evolution of systems from birth
to adulthood.Appraise the clinical implications of developmental stages in health and disease,
including gross and fine motor, language/communication, and cognitive, social,
and emotional skills.Recognize normal from abnormal in these areas.
Possess an understanding of the nutritional needs of various stages of childhood.
Recognize common and unusual health conditions of childhood.
Identify and differentiate clinical features of common physical
and mental pediatric conditions.Identify and differentiate evidence-based health care options
for these conditions.Identify and differentiate clinical features and evidence-based health care options
for the pediatric special needs population.
Be able to perform an age-appropriate evaluation of the pediatric patient.
Take a comprehensive history, using appropriate communication skills to address
both child and parent/guardian.Perform age-appropriate and case-specific physical, orthopedic, neurological,
and developmental examination protocols.When indicated, utilize age-appropriate laboratory, imaging, and other diagnostic
studies and consultations, according to best practice guidelines.Appropriately apply and adapt these skills to the pediatric special needs population.
Be able to obtain and comprehend all relevant external health records.
Formulate differential diagnoses based on the history, examination, and
diagnostic studies.
Establish a plan of management for each child, including treatment,
referral to, and/or co-management with other health care professionals.
Use the scientific literature to inform the management plan.
Adequately document the patient encounter and management plan.
Communicate management plan clearly (written, oral, and nonverbal cues)
with both the child and the child’s parent/guardian.Communicate appropriately and clearly with other professionals in the referral and
co-management of patients.
Deliver skillful, competent, and safe chiropractic care, modified for the
pediatric population, including but not limited to:
Manual therapy and instrument-assisted techniques including manipulation/
adjustment, mobilization, and soft tissue therapies to address articulations and/
or soft tissues.Physical therapy modalities.
Postural and rehabilitative exercises.
Nutrition advice and supplementation.
Lifestyle and public health advice.
Adapt the delivery of chiropractic care for the pediatric special needs population.
Integrate and collaborate with other health care providers in the care
of the pediatric patient.
Recognize the role of various health care providers in pediatric care.
Utilize professional inter-referral protocols.
Interact clearly and professionally as needed with health care professionals and
others involved in the care of each patient.Clearly explain the role of chiropractic care to professionals, parents,
and children.
Function as a primary contact, portal of entry practitioner who will.
Be proficient in pediatric first aid and basic emergency procedures.
Identify and report suspected child abuse.
Demonstrate and utilize high professional and ethical standards in all
aspects of the care of pediatric patients and professional practice.
Monitor and properly report side effects/adverse events.
Recognize cultural individuality and respect the child’s and family’s wishes regarding
health care decisions.Engage in lifelong learning to maintain and improve professional knowledge and skills.
Contribute when possible to the knowledge base of the profession by participating
in research.Represent and support the specialty of pediatrics within the profession and to
the broader healthcare and lay communities.
Discussion
This Delphi process was successful in assembling a panel of experts in chiropractic pediatrics from across the broad spectrum of stakeholders within the chiropractic profession, making the resulting comprehensive set of minimum competencies for a Certified Pediatric Doctor of Chiropractic (CPDC) generalizable throughout the chiropractic profession. The panel had a surprisingly high degree of consensus throughout the project, achieving over 80% agreement on all 3 rounds of this consensus process.
The results of this Delphi process meet several needs. First, because of the significant anatomical, physiological, developmental, and psychological differences between children and adults, those who specialize in pediatrics must make many adaptations to both the health care encounter and the delivery of therapeutic interventions. This document contributes to standardization of knowledge and skills in these areas. In addition, these competencies provide a transparent description of the CPDC to be used by other health care providers and the general public to clearly identify the skills of members of this specialty.
The resulting competencies contribute to the maturation of the chiropractic profession by developing standards for postgraduate specialty certification programs. These competencies can be used to guide institutions as they implement postgraduate educational programs in chiropractic pediatrics, as well as specialty pediatric boards in their certification processes. Additionally, if such competencies become standard for all CPDCs, then those outside of the profession will know what to expect of these specialists in terms of their diagnostic skills, range of therapeutic modalities, and co-management of pediatric patients.
There are limitations to this study. The low response rate in the second round could be a cause of concern, but this is compensated by the high response rate in the third and final round (91%). More important, since the Delphi panel did not create the initial set of seed statements and substatements, panelists may have been unduly guided by the predefined seed statements provided to them by the Steering Committee (SC). Modeling the seed statements on previous guidelines and providing room for qualitative feedback was thought to reduce this problem, but nevertheless there might still be issues which were ignored. Therefore, the competencies should be revised after several years of practical application to identify potential shortcomings. Finally, setting competencies, while an important first step, is not enough. Future projects should focus on the development of assessment tools to be used to determine whether competencies have been met.
Conclusion
This Delphi project assembled a panel of experts in the specialty of chiropractic pediatrics for the purpose of describing the minimum core competencies expected of a Certified Pediatric Doctor of Chiropractic (CPDC). The panel successfully reached a high level (80%) of consensus regarding the first profession-wide set of core competencies expected of the CPDC. As a result, these competencies may now be used to inform the creation of postgraduate educational programs in chiropractic pediatrics, to shape certification examinations in this specialty, as well as to inform both health care providers and the public about the skills of the CPDC.
Acknowledgements
The authors would like to acknowledge Cheryl Hawk, DC, PhD, for her guidance to start this project and ensure the Delphi process was done accurately. We thank Michelle Anderson, Project Coordinator, for her management of the complex communications and data collection required for this project to be completed. We would also like to thank the Delphi panelists who all served without compensation. Their leadership in this specialty and participation in this study have made it successful. Panelists granting permission to be acknowledged are Jennifer Brocker, DC, DICCP; Maria Browning, BSc (Chiro), MSc (Chiro Paeds); Neil Davies, DC, CCCP, FICC, FACC; Chantal Doucet, DC, DICCP MsC; Matthew Doyle, DC, MSc AP Paediatric Chiropractic, BAppSc(Clinical)/BChiroSc, BSc (Neurobiology); Randy Ferrance, DC, MD; Brian Gleberzon, MHSc, DC; Paul Greteman, DC, DICCP; Navine Haworth, DC, DICCP, GCTTL, PhD(c); Donna Hedgepeth, MT(ASCP), DC, DACCP; Anne Langford, DC, DICCP; Michael Master, DC, DACNB; Joyce Miller, DC, DABCO, PhD; Carol Phillips, DC; Anthony Rosner, PhD; Michael Schneider, DC, PhD; Angela Todd, BAppSci (Chiro), Dip. (Chiro Paed); Sharon Vallone, DC, FICCP; Mary Unger-Boyd, DC, DICS, CACCP; and Steve Zylich, DC.
Author Contributions
EH was involved in the conceptualization of the overall project and development of the first set of seed statements. EH, LH, and KAP, as members of the steering committee, participated in finalizing the initial set of statements, reviewed results from each round, and edited the statements until the final set was prepared. All authors wrote the article, critically edited all drafts, and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References:
The Institute for Alternative Futures
The Future of Chiropractic Revisited: 2005 to 2015
Alexandria, VA: (2005)Garner MJ, Birmingham M, Aker P, Moher D, Balon J, Keenan D, Manga P.
Developing Integrative Primary Healthcare Delivery: Adding a Chiropractor to the Team
Explore (NY). 2008 (Jan); 4 (1): 18–24Pfefer, M, Strunk, R, Hawk, C et al.
Integration of Chiropractic Services into a Multidisciplinary Safety-Net Clinic
Topics Integr Health Care. 2010 (Sep 1); 1: 1: 1005Lothe LR, Bolton JE.
Increasing research capacity in the chiropractic profession: a case study and evaluation of an innovative research program in Norway.
J Chiropr Educ. 2013;27:40–47Wikipedia.
List of chiropractic credentials.
https://en.wikipedia.org/wiki/List_of_chiropractic_credentials
Accessed October 2015.Shaw G.
Chiropractic specialties on the rise.
https://www.acatoday.org/content_css.cfm?CID=2323
Accessed October 2015.Barnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Black, LI, Clarke, TC, Barnes, PM, Stussman, BJ, and Nahin, RL.
Use of Complementary Health Approaches Among Children Aged
4–17 Years in the United States: National Health
Interview Survey, 2007–2012
National Health Statistics Report 2015 (Feb 10); (78): 1–19Christensen M, Hyland J, Goertz C, Kollasch M.
Practice Analysis of Chiropractic 2015:
A Project Report, Survey Analysis, and Summary of Chiropractic Practice in the United States.
Greeley, CO: National Board of Chiropractic Examiners; 2015Marchand AM.
Chiropractic Care of Children from Birth to Adolescence and Classification of
Reported Conditions: An Internet Cross-Sectional Survey of
956 European Chiropractors
J Manipulative Physiol Ther. 2012 (Jun); 35 (5): 372–380Pohlman, KA, Hondras, MA, Long, CR, and Haan, AG.
Practice Patterns of Doctors of Chiropractic With
a Pediatric Diplomate: A Cross-sectional Survey
BMC Complement Altern Med. 2010 (Jun 14); 10: 26Council on Chiropractic Pediatrics.
http://www.icapediatrics.com/
Accessed December 2014.International Chiropractic Pediatric Association.
About the ICPA.
http://icpa4kids.com/
Accessed December 2014.The Council on Chiropractic Education.
CCE Accreditation Standards: Principles, Processes, & Requirements for Accreditation.
Scottsdale, AZ: Council on Chiropractic Education; 2013The Paediatric Undergraduate Program Directors of Canada.
www.pupdoc.ca
Accessed October 2014.Fitch K, Bernstein SJ, Aquilar MS
The RAND UCLA Appropriateness Method User’s Manual.
Santa Monica, CA: RAND Corporation; 2003Return to PEDIATRICS
Return to PEDIATRICS GUIDELINES
Since 3–25–2017
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |